Article Text

Abstract
Background Besides the interest of an early detection of ovarian cancer, there is an urgent need for new predictive and prognostic biomarkers of tumor development and cancer treatment. In healthy patients, circulating blood monocytes are typically subdivided into classical (85%), intermediate (5%) and non-classical (10%) populations. Although these circulating monocyte subsets have been suggested as biomarkers in several diseases, few studies have investigate their potential as a predictive signature for tumor immune status,tumor growth and treatment adaptation.
Methods In this study, we used a homogeneous cohort of 28 chemotherapy-naïve patients with ovarian cancer to evaluate monocyte subsets as biomarkers of the ascites immunological status. We evaluated the correlations between circulating monocyte subsets and immune cells and tumor burden in peritoneal ascites. Moreover, to validate the use of circulating monocyte subsets tofollow tumor progression and treatment response, we characterized blood monocytes from ovarian cancer patients included in a phase 1 clinical trial at baseline and following murlentamab treatment.
Results We demonstrate here a robust expansion of the intermediate blood monocytes (IBMs) in ovarian cancer patients. We establish a significant positive correlation between IBM percentage and tumor–associate macrophages with a CCR2high/CD163high/CD206high/CD86lowprofile. Moreover, IBM expansion is associated with a decreased effector/regulatory T-cell ratio in ascites and with the presence of soluble immunosuppressive mediators. We also establish that IBM proportion positively correlates with the peritoneum tumor burden. Finally, the study of IBMs in patients with ovarian cancer under immunotherapy during the phase clinical trial supports IBMs to follow the evolution of tumor development and the treatment adaptation.
Conclusions This study, which links IBM level with immunosuppression and tumor burden in peritoneum, identifies IBMs as apotential predictive signature of ascites immune status and as a biomarker ofovarian cancer development and treatment response.
Trial registration number EudraCT: 2015-004252-22 NCT02978755.
- immunity
- tumor microenvironment
- macrophages
- biomarkers, tumor
- immunotherapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Ovarian cancer is the second most common gynecological malignancy and the fourth leading cause of cancer deaths in women.1 For the past 20 years, the standard treatment has been surgical debulking of tumors followed by chemotherapy with platinum salts and taxanes in combination. Despite an initial clinical response in most patients (70%–80%), recurrence and acquired resistance to platinum salts frequently occur.2 The 5-year survival rate for patients with ovarian cancer is still only 30%, even with the application of promising new therapeutic agents, such as between other angiogenesis inhibitors, poly-ADP-ribose polymerase inhibitors3 or inductors of apoptosis like second mitochondria-derived activator of caspase mimetics.4 The poor prognosis of ovarian cancers can be explained by the fact that it is still difficult (1) to detect ovarian cancer at an early stage, (2) to monitor patients’ response to cancer treatment and adapt therapeutics, and (3) to predict and detect resistance to drugs. In this context, there is an urgent need of new predictive and prognostic biomarkers. However, to date, there is no effective screening tool for this peritoneal cancer, and one of the best few available tumor biomarker, the serum cancer antigen 125 (CA125), has a sensitivity of only 50%.5 Recently, the risk of ovarian malignancy algorithm, which combines the serum levels of CA125, human epididymis-specific protein 4 and the patients’ menopausal status, has been proposed to evaluate the risk of malignancy.6 However, this algorithm has not been evaluated as predictive biomarker of ovarian cancer in large cohorts.
Several authors have suggested that monocyte subsets in the peripheral blood should be evaluated as biomarkers in several diseases.7 Monocytes can be classified into three subsets according to CD14 and CD16 surface marker expression.7 In healthy donors, the predominant subset, classical monocytes (CD14high CD16neg), accounts for approximately 85% of the total monocyte population. Of the remaining 15%, 10% are non-classical monocytes (CD14low CD16high) and 5% are intermediate monocytes (CD14high CD16low). An expansion of the CD16-positive monocytes has been well described in different types of diseases, mostly in infectious or inflammatory conditions.7 This expansion has also been described in some malignancies, and the frequency of CD16-positive monocytes has been related to tumor size and stage in breast cancer,8 to the invasive character of cholangiocarcinoma9 or to poor patients’ response to immunotherapy in melanoma.10
Sixty percent of women who are diagnosed with ovarian cancer present an extensive peritoneal carcinomatosis associated with the development of tumor ascites. This peritoneal fluid is a reservoir of a complex mixture of soluble factors and cellular components which provide an immunosuppressive and tumor-promoting microenvironment.11–13 Thus, the identification of specific subsets of circulating blood monocytes, which are induced by disease progression and whose expansion can be correlated with the immunological status of peritoneal ascites, may be an interesting approach to predict the disease course. Here, we established a homogeneous cohort of 28 patients diagnosed with ovarian cancer and characterized circulating blood monocytes and immune cells from peritoneal ascites at diagnosis. Moreover, to determine the potential of circulating monocyte subsets as a biomarker to follow tumor progression and to assess treatment efficiency, particularly immunotherapies, we also analyzed circulating blood monocytes from patients with ovarian cancer included in a phase I clinical trial with GM102, also named murlentamab (a low-fucose humanized IgG subclass 1 (IgG1) anti-Müllerian hormone receptor type 2 (AMHRII) antibody) at baseline and following treatment. GM102 targets AMHRII, which is expressed in 96% of human primary granulosa cell tumors14 and in around 70% of ovarian cancer cells.15
We demonstrate here an increase in the intermediate blood monocyte (IBM) subset in patients with ovarian cancer. This increase is positively correlated with the protumoral and immunosuppressive microenvironment of peritoneal ascites and with the peritoneum tumor burden. This study demonstrates that the frequency of blood monocyte populations reflects the situation in the peritoneum and identifies circulating monocyte subsets as a potential predictive signature for ovarian cancer progression at diagnosis and following treatments.
Finally, the results obtained from patients included in a phase I clinical trial under GM102 reinforce the use of blood monocyte profiling as a new strategy to follow up tumor growth and treatment response.
Materials and methods
Ascites fluid and blood sample collection
Ascitic fluids and blood samples from individuals with ovarian cancer were collected from chemotherapy-naïve patients who underwent a tumor surgical resection at the Claudius Regaud Institute (IUCT Oncopole, Toulouse, France). We also analyzed blood samples of patients included in a phase I multicentric clinical trial who underwent an immunotherapy treatment with murlentamab (GM102, a low-fucose IgG1 anti-AMHRII antibody). Only blood samples from the six patients managed by IUCT were analyzed. The progression of the disease was established by the analysis of tumor markers (CA125 or inhibin B) and of tumor lesions evaluated by Response Evaluation Criteria In Solid Tumors (RECIST V.1.1). Blood samples from healthy volunteers were provided by the French Blood Establishment (EFS).
Isolation of mononuclear cells from blood and ascites
Blood samples and ascitic fluids were obtained using an aseptic technique from 28 chemotherapy-naïve patients with ovarian cancer. Blood samples were also obtained from seven healthy subjects and from six patients with ovarian cancer who underwent a tumor-targeted immunotherapy treatment.
Mononuclear cells were isolated from patients’ blood and ascites with a Ficoll density gradient (Lymphoprep, Stemcell Technologies). The fractions containing peripheral blood mononuclear cells or ascitic mononuclear cells were then washed two times. Cell number was evaluated and 250 000 cells were stained for flow cytometry analysis.
Flow cytometry
All analyses were gated on viable cells after live/dead staining (Molecular Probes LIVE/DEAD Fixable Violet Dead Cell Stain Kit, Life Technologies).
To study blood monocyte populations, CD14 and CD16 were respectively detected after staining with CD14-PerCPVio700 and CD16-PE antibodies (Myltenyi Biotec). To study the phenotype of blood monocytes and macrophages from ascitic fluid, cells were labelled with the following antibodies: CD14-PerCPVio700, CCR2-PEVio770, CD163-PEVio770, CD86- Vioblue, TLR-2-APC, CD36-FITC, MHC2-APCVio700 (Myltenyi Biotec) and CD206-APC (BD Biosciences). In ascites, analysis of the percentage of cells expressing studied receptors and/or the level of expression of the receptors (measured as the mean fluorescence intensity) was conducted in a population of cells characterized by medium-sized granules (Side Scatter (SSC)med) and the expression of the monocyte/macrophage receptor CD14.
To study the ascitic lymphocyte population, cells were labelled with the following antibodies: CD45-Viogreen, CD3-Vioblue, CD4-APCVio770, CD8-PerCP, CD25-PE, CD56-APC, CD19-PEVio700 and CD183-FITC (Myltenyi Biotec). For intracellular staining, cells were fixed and permeabilized with the FoxP3 staining buffer set (Myltenyi Biotec) and stained with the FoxP3-APC antibody (Myltenyi Biotec).
Appropriate fluorochrome-matched isotype antibodies were used to determine non-specific background staining. All stainings were performed on 100 µL of phosphate-buffered saline (PBS) solution without calcium and magnesium (PBS−/−) and 1% heat-inactivated fetal calf serum. A population of 10,000 cells was analyzed for each data point. All analyses were carried out in a BD Fortessa flow cytometer with Diva software.
For ascitic fluid cytokine titration, a multiplex bead-based immunoassay was used according to the manufacturer’s instructions (LEGENDPlex Mix and Match System, Biolegend).
Statistical analysis
For blood monocyte comparison between healthy subjects and patients with ovarian cancer, the data were subjected to analysis of variance followed by the Bonferroni’s multiple comparisons test. Spearman rank correlation was used to investigate the relationships between IBMs and immune/clinical parameters of patients with ovarian cancer. Analysis was performed using GraphPad Prism V.7.0. A p value of <0.05 was considered statistically significant.
Results
CD14high CD16low IBM frequency is increased in patients with ovarian cancer
In our cohort of chemotherapy-naïve patients with tovarian cancer (see online supplementary table 1 for clinical parameters of subjects), complete blood count revealed a slight increase in leukocyte concentration compared with normal values established in healthy subjects (figure 1A). Moreover, although the blood counts of some patients with ovarian cancer deviate from healthy subject reference intervals, the average concentrations for leukocyte subtypes and other blood cells did not show any significant change in regard to normal values (figure 1A).
Supplemental material

Characterization of blood monocyte subsets at diagnosis from healthy subjects and patients with ovarian cancer. (A) Complete blood counts of 28 patients with ovarian cancer. (B–D) Blood monocyte subsets from healthy subjects and patients with ovarian cancer were characterized by flow cytometry after CD14 and CD16 staining. Blood monocyte subset analysis was conducted in a population of cells characterized by SSCmed and the expression of the monocyte/macrophage receptor CD14. (B) Gating strategy for the identification of the three monocyte subsets. (C) Dot blot of representative data for both analyzed groups. (D) Quantification of classical (CD14high CD16neg), intermediate (CD14high CD16low) and non-classical (CD14low CD16high) monocytes. Results correspond to mean±SEM. ***P<0.001 compared with the respective monocyte subset in healthy subjects. P values were determined using an analysis of variance followed by Bonferroni’s multiple comparisons test. FSC, Foward scatter; PBMC, peripheral blood mononuclear cell; SSC, Side scatter.
Human blood monocytes are heterogeneous and are classified into three subsets based on CD14 and CD16 expressions. Fluorescence-activated cell sorting analysis performed in the blood of patients with ovarian cancer demonstrated that the proportions of monocyte subsets were altered (figure 1B–D). As expected, in healthy subjects (n=7), classical monocytes (CD14high CD16neg) represented 85%–90% of total monocytes, whereas non-classical (CD14low CD16high) and intermediate (CD14high CD16low) populations, these represented only 5%–10% (figure 1C,D). Interestingly, in 28 chemotherapy-naïve patients with ovarian cancer, there was a significant increase in CD14high CD16low monocytes (on average, 34%±4% of total circulating monocytes) to the detriment of CD14high CD16neg monocytes (on average, 61%±4% of total monocytes). The proportion of CD14low CD16high monocytes was the same as in healthy subjects (on average, 3%±1% of total monocytes) (figure 1C,D). These data reveal a robust expansion of the IBM population in patients with ovarian cancer.
We then characterized the phenotype of the three monocyte subsets and analyzed whether it could change in patients with ovarian cancer (online supplementary figure 1). In healthy subjects, classical, intermediate and non-classical monocytes displayed different protein levels of markers, such as CCR2, CD206, CD163, CD86, CD36 and MHC2. However, the expression level of these markers remained unchanged in patients with ovarian cancer compared with those observed in healthy donors. Together, these results support that ovarian tumors impact the proportion of monocyte subsets without altering their phenotype.
Supplemental material
CD14high CD16low IBM frequency predicts the peritoneal ascites immune status in patients with ovarian cancer
To establish whether intermediate monocyte expansion in the blood of patients with ovarian cancer may reflect the immune microenvironment in the tumor site, we evaluated the correlation between the circulating IBM population and innate and adaptive immune cells in tumor ascites.
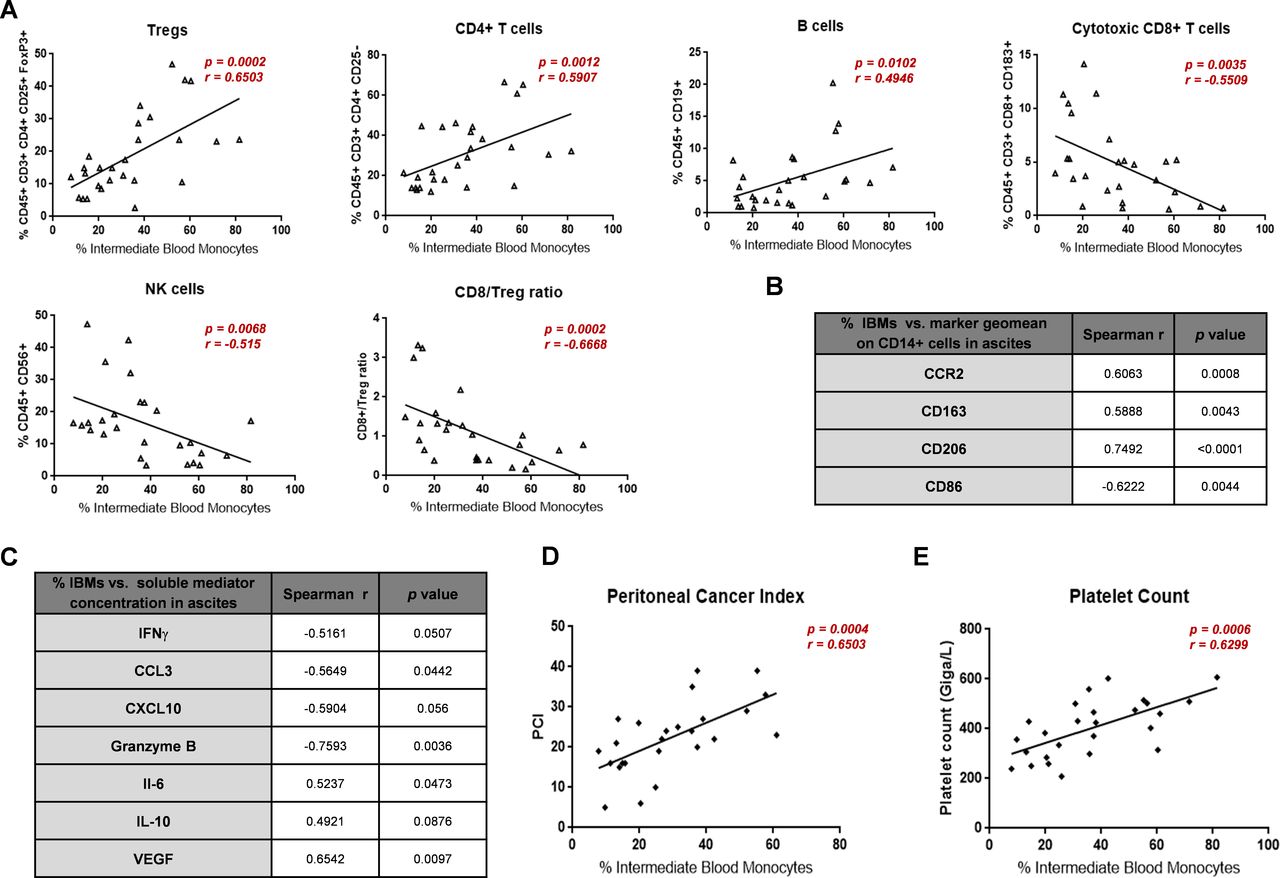
We found significant positive correlations between the percentage of IBMs and the percentage of regulatory T cells (Spearman rank correlation coefficient (r)=0.6503, p=0.0002), of CD4+ T cells (r=0.5907, p=0.0012) and of B cells (r=0.4946, p=0.0102) in the ascites (figure 2A). Conversely, we observed significant inverse correlations between the proportion of IBMs and cytotoxic CD8+ T cells (r=−0.5509, p=0.0035), natural killer (NK) cells (r=−0.515, p=0.0068) and the CD8+/regulatory T-cell ratio present in the ascites of patients with ovarian cancer (figure 2A). Together, these results clearly demonstrate that circulating IBM expansion is associated with a decrease in the effector/regulatory T-cell ratio in tumor ascites.

Correlation between CD14highCD16low IBMs and ascites immune status and cancer development in patients with ovarian cancer. (A–C) Analysis of immune cell population and soluble mediators of blood and ascitic fluid samples from 28 patients with ovarian cancer. (A) Correlation of circulating IBMs with the proportion in ascites of T-cell populations, B cells, NK cells and with the CD8/regulatory T-cell ratio. (B) Correlation of circulating IBMs with the geomean of several markers (CCR2, CD163, CD206 and CD86) at the surface of CD14+ cells of ascites. (C) Correlation of circulating IBMs with the concentration of several soluble mediators of ascites involved in immunity (IFN-γ, CCL3, CXCL10 and granzyme B), tolerance (IL-6 and IL-10) and tumor progression (VEGF). (D) Correlation of circulating IBMs with the PCI. (E) Correlation of circulating IBMs with the platelet count. P values were determined using the Spearman rank correlation. CCL3, C-C Motif Chemokine Ligand 3; CXCL10, C-X-C Motif Chemokine Ligand 10; IBM, intermediate blood monocyte; IFN-γ, interferon-γ; IL, interleukin; NK, natural killer; PCI, peritoneal cancer index; VEGF, vascular endothelial growth factor.
The phenotypical characterization of macrophages (CD45+ CD14+ cells) in tumor ascites of the 28 patients with ovarian cancer demonstrated that almost all of them express CCR2, CD163, CD206 and CD86 (online supplementary figure 2). However, considering the variation in the expression level (geomean) of these markers on CD14+ cells, we established significant positive correlations between the proportion of IBM subset and the expression on CD14+ cells from tumor ascites of CCR2, CD163 and CD206, markers associated with ovarian tumor progression and poor prognosis (figure 2B). Conversely, we established an inverse correlation between the percentage of IBMs and the expression of CD86, costimulatory molecule for the priming and activation of T cells, on macrophages from tumor ascites (figure 2B).
Supplemental material
The quantification of protein levels of ascites soluble mediators showed a significant negative correlation between the frequency of IBMs and interferon-γ (IFN-γ), CXCL10 and CCL3, factors that are involved in the Th1 response (figure 2C). Moreover, this inverse correlation was also observed with granzyme B, which is well described as a mediator of the cytotoxic response of T lymphocytes and NK cells. However, the frequency of IBMs was significantly correlated with the protein level in ascites of interleukin (IL)-10 and IL-6 immunosuppressive cytokines (figure 2C). Finally, the increase in IBM frequency significantly correlated with the augmentation of the proangiogenic vascular endothelial growth factor (VEGF) (figure 2C).
Together, these data link the expansion of the IBM population in patients with ovarian cancer to the peritoneal ascites protumor immunosuppressive status.
CD14high CD16low IBM population increase is associated with progression of ovarian cancer
To evaluate whether the higher frequency of circulating IBMs in patients with ovarian cancer might be related to tumor burden, and hence might reflect disease progression, we examined the correlation between the circulating IBM population and the peritoneal cancer index (PCI) used to assess the extent of peritoneal cancer throughout the peritoneal cavity.16 Interestingly, we established a correlation between the percentage of IBMs and the PCI (r=0.6503, p=0.0004) (figure 2D), highlighting the circulating IBM subset as a potential signature for the progression of ovarian cancer.
In line with the link between IBMs and ovarian tumor progression, we also established a positive correlation between IBM proportion and the platelet count (figure 2E), which has been previously described to be related to poor prognosis and unfavorable clinicopathological parameters for patients with ovarian cancer.17 Except for platelets, no other correlations could be established between IBM proportions and blood cell counts (online supplementary figure 3).
Supplemental material
CD14high CD16low IBMs as a biomarker to follow up the progression of ovarian cancer
We analyzed blood samples, at diagnosis and following treatment, from six patients with ovarian cancer who underwent a tumor targeted immunotherapy with murlentamab (GM102) (see online supplementary table 2 for clinical parameters of subjects). Preliminary data have demonstrated various responses under GM102 treatment from stabilization to partial response.18 Moreover, GM102 has been shown to activate the antitumor T-cell immune response.19
As observed in the first cohort of 28 chemotherapy-naïve patients with ovarian cancer (figure 1C,D), the 6 patients with ovarian cancer included in the GM102 phase I clinical trial presented a high proportion of CD14high CD16low IBMs and a low proportion of CD14high CD16neg classical blood monocytes prior to treatment (C1D1 SOI) (figure 3A).
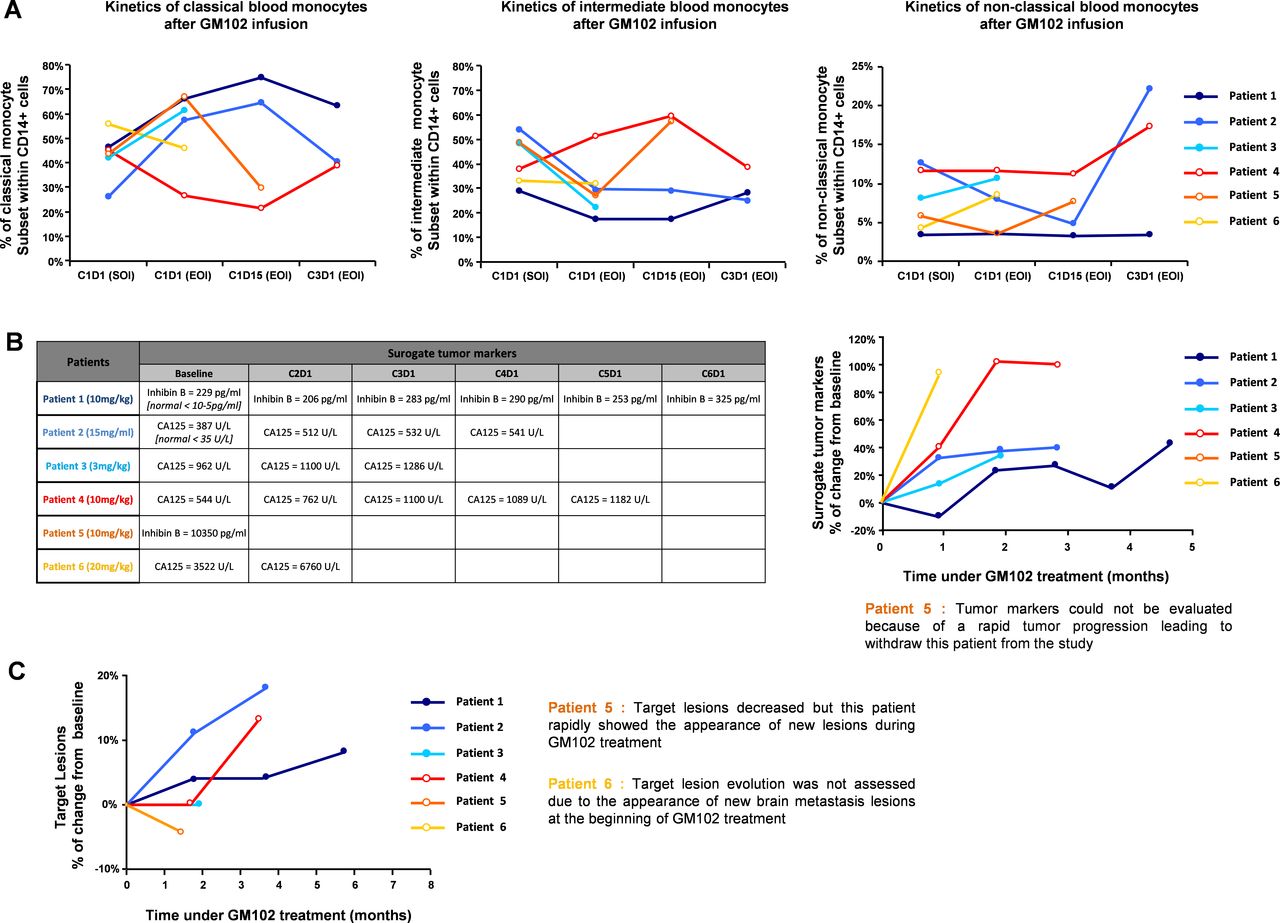
Effect of GM102 infusion on blood monocyte subsets and tumor progression in patients with gynecological cancer. (A–C) Proportion of blood monocyte subsets, evolution of surrogate tumor markers and tumor development were evaluated in six patients with ovarian cancer at diagnosis and after GM102 (an anti-anti-Müllerian hormone receptor type 2 low fucose IgG subclass 1 antibody) treatment. These six patients included in a phase I multicentric study were followed up on the site of Toulouse IUCT Oncopole. (A) Quantification of classical (CD14high CD16neg), intermediate (CD14high CD16low) and non-classical (CD14low CD16high) monocytes during GM102 treatment in six patients with ovarian cancer. (B) Evolution of tumor markers (CA125 and inhibin B) in these six patients during GM102 treatment. (C) Evolution of target lesions evaluated with RECIST V.1.1 in these six patients during GM102 treatment. C, cycle; D, day; EOI, end of infusion; SOI, start of infusion.
Interestingly, we observed a decrease of IBMs, which was mirrored by an increase of classical blood monocytes over time following GM102 infusion in three out of six patients with ovarian cancer (patients 1, 2, and 3) (figure 3A). These data support that GM102 treatment can orient monocyte subset proportions towards those found in healthy subjects. In patient 1, the orientation of classical and IBM subsets towards standard proportions was accompanied by a stabilization of both tumor markers (figure 3B) and tumor lesions evaluated by RECIST V.1.1 (figure 3C). During the first few hours after GM102 treatment, we observed in patient 3 a profile similar to patient 1, that is, a decrease in IBM proportion associated with a moderate increase in tumor marker, as well as a stabilization of tumor lesions (figure 3A–C). Surprisingly, in patient 2, although the orientation of classical and IBM subsets towards standard proportions was accompanied by a stabilization of tumor marker (figure 3B), the tumor lesions gradually increased after GM102 infusion (figure 3C). These mitigated results are further corroborated by the fact that, contrary to the first two patients (patients 1 and 3), the reduction of IBM proportions observed in patient 2 during GM102 treatment was accompanied by a strong increase in CD14low CD16high non-classical monocytes whose deleterious role has already been described in tumors.20
In patient 4, 5 and 6, GM102 infusion was not followed by reduced IBM proportions and simultaneous increased classical monocyte proportions (figure 3A). In patient 4, the continuous IBM elevation after GM102 infusion was associated with the progression of the disease, as indicated by the increase in tumor markers and lesion development (figure 3B,C). In patient 5, while the target lesion evaluated by RECIST V.1.1 appeared to decrease (figure 3C), the failure of GM102 treatment to orient IBM proportions towards those found in healthy subjects was accompanied by the appearance of new non-target lesions resulting from a rapid tumor progression that led to the withdrawal of this patient from the study (figure 3A–C). Similarly, in patient 6, the increase in IBMs during treatment was also accompanied by an increase in tumor markers and tumor progression, as evidenced by the appearance of non-target tumor lesions in the brain, resulting in the exclusion of this patient from the study (figure 3B,C).
In addition to the established positive correlation between IBM frequency and the PCI (figure 2D), these results suggest that the expansion of IBM is linked to tumor load and could therefore be used to follow up tumor growth and to monitor treatment adaptation in patients with ovarian cancer.
Discussion
Circulating monocytes have an essential role in cancer pathophysiology. Indeed, monocytes are recruited at the tumor site and differentiate into macrophages which support tumor growth. An increase in the proportion of CD16-positive monocytes has been described in various infectious and inflammatory diseases.7 Although the reasons for this expansion remain unclear, several studies suggest that these intermediate or non-classical populations are associated with the promotion of several pathologies and a poor prognosis.8 In the context of tumors, although several studies report that classical monocytes exert numerous potent antitumor effects,21 non-classical and intermediate monocytes perform protumor functions through their proangiogenic capacities.22 23 In this study, we demonstrate a change in the proportion of circulating monocyte subsets—a significant increase in CD14high CD16low IBMs and a decrease in CD14high CD16neg classical monocytes—in chemotherapy-naïve patients with ovarian cancer. Our findings are consistent with previous studies showing an increase in CD16-positive populations has been found in the peripheral blood of patients with breast cancer,8 gastric cancer,24 cholangiocarcinoma,9 multiple myeloma,25 melanoma10 and chronic lymphocytic leukemia.26 The expansion of the blood of CD16-positive populations is clearly associated with the presence of tumor tissue, since after resection of the tumor the CD16-positive population decreased close to the normal levels found in healthy subjects.9 Moreover, several cytokines, such as IL-10, macrophage colony-stimulating factor, P-selectin and CCL2, have been reported to induce the in vivo and in vitro expansion of the blood CD16-positive population.8 27 28 Given the high concentration of these mediators in ascites of patients with ovarian adenocarcinoma,11 29 these data support the idea that the modulation of peripheral blood monocyte subpopulations may be mediated by secreted factors produced by ovarian tumor cells and stromal cells of tumor microenvironment. This was also reinforced by our results showing a robust expression of CCR2, the CCL2 receptor, on macrophages from ascites of patients with a strong expansion of IBMs. Moreover, the ability of tumor cells to ‘re-educate’ immune cells towards a tolerogenic state suggests that these intermediate monocytes may have a role in tumor promotion.
In this context, we have shown here that the robust expansion of the IBM population in patients with ovarian cancer is associated with a protumor immunosuppressive microenvironment in ascites. Indeed, a high proportion of circulating IBMs is positively correlated with decreased effector/regulatory T-cell ratio in tumor ascites. In line with this, we have demonstrated that the expansion of IBMs is also associated with the decrease in ascites of IFN-γ, CCL3, CXCL10 and granzyme B, and the increase of IL-6, IL-10 and VEGF, thus linking the frequency of IBMs with a decrease in the balance between immunity and tolerance. Furthermore, we have established a positive correlation between this intermediate population and the expression level on tumor-associated macrophages (TAMs) of CCR2, CD206 and CD163, markers associated with ovarian tumor progression and poor prognosis. Given the well-established correlation between CCL2 overexpression, TAM infiltration and poor prognosis in many cancers,30 31 TAM CCR2 expression is associated with tumor development. Moreover, while absolute densities of CD206-positive cells are not prognostic, a high CD206/CD68 ratio is strongly associated with worse progression-free survival in patients with high-grade ovarian epithelial carcinoma.32 Similarly, the number of CD163- positive TAMs in borderline and malignant ovarian tumors is significantly higher than that in benign ovarian tumors.33 In ovarian adenocarcinoma, the density of CD163-positive TAMs and the CD163/CD68 ratio have been identified as negative predictors for progression-free survival and overall survival.34 In addition, several studies have suggested the role of CD163 in the induction of immune tolerance.35 Together, these data link the high proportion of circulating IBMs in patients with ovarian cancer with the presence in ascites of TAMs strongly expressing markers involved in immunosuppression and tumor development (figure 4). The presence of these protumor TAMs is consistent with the high concentrations in ascites of IL-6 and IL-10, which are soluble mediators that are involved in the generation of immunosuppressive TAMs.36 37 Thus, our data suggest that the expansion of the IBM subpopulation in patients with ovarian cancer may represent a new biomarker for the immunosuppressive status of the ascites microenvironment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic illustration of IBM population as a predictive signature of ascites immune status and as a biomarker of ovarian cancer development and treatment adaptation. We report a strong expansion of intermediate blood monocytes in patients with ovarian cancer. IBM proportion positively correlates with the pro-tumoral and immunosuppressive microenvironment in ascites and with the peritoneal tumor burden, therefore identifying IBMs as a predictive signature of ascites immune status and as a biomarker of ovarian cancer development.CCL3, C-C Motif Chemokine Ligand 3; CTL, Cytotoxic T Lymphocytes; CXCL10, C-X-C Motif Chemokine Ligand 10; IFN-γ, interferon-γ; IL, interleukin; NK, natural killer; TAM, tumor-associated macrophage; VEGF, vascular endothelial growth factor.
Given the evidence that a high CD8+/regulatory T-cell ratio is associated with a favorable prognosis in ovarian cancer,13 38 our results showing a significant inverse correlation between IBM proportions and cytotoxic CD8+ cells also strongly suggest that the expansion of IBMs may be correlated with poor prognosis. In line with this, we established a positive correlation between the percentage of IBMs and the tumor burden in the peritoneum of patients with ovarian cancer. Moreover, we demonstrated that IBM proportions are also positively correlated to platelet count. Since an elevated platelet count has been previously described to be related to poor prognosis and unfavorable clinicopathological parameters for patients with ovarian cancer,17 these results further support that IBMs, in addition to being a predictive signature of the immunosuppressive status in ascites, could also be used to predict patients’ prognosis. Finally, in our study, the orientation of the proportion of classical and IBM subsets towards normal in patients with ovarian cancer under murlentamab treatment and the associated stabilization of tumor markers and tumor burden strongly suggest that the monitoring of monocyte subsets could be used to follow up tumor growth and treatment response. This is consistent with the data showing that the frequency of classical monocytes and an increased abundance of intratumoral CD8+ T cells are positively correlated with better clinical outcomes in patients receiving pembrolizumab, an anti-PD-1 for metastatic melanoma.10
In conclusion, we have demonstrated a robust expansion of the IBM population in patients with ovarian cancer and have linked this high subpopulation frequency with the protumor immunosuppressive microenvironment in ascites. We have also established a positive correlation between the percentage of IBMs and the PCI (figure 4). Altogether, our results highlight the potential use of IBMs as biomarkers for ascites immune status and ovarian cancer progression.
Acknowledgments
We thank Alexia Zakaroff-Girard and Elodie Riant (TRI imaging platform, IFR150/I2MC) for flow cytometry technical assistance. We are grateful to the ‘Phil-Anthrope’ Association, which provided a special grant for this project.
References
Footnotes
BC and AC are joint senior authors.
MP and ALN contributed equally.
Contributors AC and BC designed the experiments (concept and design, collection and assembly of data, data analysis and interpretation); MP, ALN, KC and HL designed some experiments, performed experiments and analyzed the data (collection and assembly of data); GJ, MCR, LL, and HA provided help with the experiments; GF, AM, J-PD, MA and LG provided critical clinical feedbacks and patients’ samples. FL, J-MB, IT-F and J-FP provided patients’ samples from GM102 phase I clinical trial and intellectual support; AC, BC and MP wrote the manuscript.
Funding This work was funded by a grant from the French government (IDEX 2012) and the Groupe de Recherche de l’Institut Claudius Regaud.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. If you need information about data related to this manuscript, please contact the corresponding author.