Article Text

Abstract
Patients with ROS1-rearranged non-small cell lung cancer (NSCLC) inevitably relapse after first-line targeted therapy with tyrosine kinase inhibitors. Efficacy of checkpoint inhibitor-based therapy on ROS1-positive NSCLC in second-line setting and change of immune factors during treatment are rarely studied. We report a ROS1-rearranged stage ⅢB lung adenocarcinoma patient who was resistant to ceritinib after developing a secondary ROS1 F2004L mutation. He received eight cycles of nivolumab plus chemotherapy and had an initial partial response, but brain metastases appeared in the seventh cycle. Lorlatinib was confirmed to have activity against CD74–ROS1 with F2004L in vitro, and was administered to this patient as the third-line therapy. The patient responded well to lorlatinib and had no relapse. We explored the tumor immune microenvironment (TIME) during immune-chemotherapy by multiplex immunohistochemistry, RNA sequencing, and multiplex plasma protein immunoassay. The results show that the TIME was active and plasma inflammatory factors were increased when the patient responded to immune-chemotherapy, while the plasma inhibitory checkpoint proteins, lymphocyte-activation gene 3, B and T lymphocyte attenuator, programmed cell death ligand 1 (PD-L1), and PD-1, were increased when the disease progressed. Moreover, the PD-L1 expression on tumor tissue was upregulated during treatment, predicting the limited benefit from immune-chemotherapy. This case report suggests that lorlatinib is a better choice than immune-chemotherapy in second-line setting for patients with similar genomic characteristics, and that monitoring the immune components during immunotherapy may help to predict disease response.
- biomarkers
- tumor
- case reports
- immunotherapy
- lung neoplasms
- tumor microenvironment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Oncogenic rearrangements of the ROS1 gene occur in 1%–2% of non-small cell lung cancer (NSCLC) patients.1 Oral ROS1 inhibitors, including crizotinib, ceritinib, and entrectinib, are the first-line therapy for patients with ROS1-positive advanced NSCLC according to the latest NCCN guidelines. However, relapse inevitably occurs and lorlatinib is the recommended choice for treating resistant tumors.2 Immune checkpoint inhibitors (ICIs) is considered for patients with targetable driver alterations after exhaustion of targeted therapy or chemotherapy, as these patients may not respond to ICIs.3 Nonetheless, studies have demonstrated the correlation between ROS1 rearrangement and high programmed cell death ligand 1 (PD-L1) expression.4 5 Whether ICI-based therapy is effective in patients following first-line targeted agents still needs more investigation.
Immunohistochemistry testing for PD-L1 expression is recommended for all patients with metastatic NSCLC before first-line treatment to assess whether ICI is an option according to the NCCN guidelines. High PD-L1 expression may suggest that PD-1/PD-L1 axis is the main strategy that tumor adopted to escape immune elimination. However, as a biomarker for predicting immunotherapy response, PD-L1 expression is imperfect because of the diversity of detection methods, threshold, and temporal and spatial heterogeneity.6 7 And as a prognostic biomarker, it may associate with poor outcome in NSCLC.8 Therefore, we propose that the dynamic changes of PD-L1 during immunotherapy may be more likely to predict disease response. In clinical practice, tumor biopsies may not be appropriate during treatment, but if such specimens are available, changes in PD-L1 expression may indicate the response status.
Here, we report an ROS1-rearranged NSCLC patient who showed a short-term response to nivolumab plus chemotherapy after acquiring a rare ceritinib-resistant ROS1 mutation. We investigated the tumor immune microenvironment (TIME), including PD-L1 expression, and peripheral plasma immune-related proteins during treatment, to find the correlation between immune characteristics and disease response to the immune-chemotherapy (ICT).
Case presentation
A 34-year-old male non-smoker with cervical lymph node enlargement for 2 weeks was admitted to our hospital in March 2019. Positron emission tomography CT (PET-CT) revealed a mass of 1.8×1.6 cm in the right lower lobe (figure 1A) and multiple enlarged right hilar, mediastinal, supraclavicular, and subclavian lymph nodes. The patient was diagnosed with lung adenocarcinoma (T1N3M0) by a needle biopsy on the supraclavicular lymph node. Next-generation sequencing (NGS) analysis of 543 cancer-related genes (Genecast Biotechnology Co) on the biopsy tissue sample revealed a CD74–ROS1 gene fusion, which was then confirmed by targeted RNA sequencing and Sanger sequencing (figure 1B). Concurrent chemoradiation followed by durvalumab is the recommended initial treatment for patients with stage ⅢB NSCLC according to NCCN guidelines. However, durvalumab was not available in China at that time. Based on the patient’s choice and the actionable oncogenic variant, the ROS1-positive NSCLC patient started the first-line therapy with ceritinib (450 mg orally once a day). Two months later, he achieved a partial response based on Response Evaluation Criteria in Solid Tumors version 1.1 (figure 1A).

Typical images of disease response during three lines of therapy and corresponding testing for treatment decision-making. (A) CT images of the lung primary tumor at baseline and 2.6 months during the first-line therapy with ceritinib. The primary tumor continued to shrink during subsequent treatment (the data not shown). (B) A diagram of CD74–ROS1 rearrangement with the acquired ROS1 F2004L mutation. CD74–ROS1 (C6; R34) fusion in the tumor tissue was confirmed by Sanger sequencing (left). (C) CT images of the largest lymph node lesion at right armpit at 4.5 months and 7.5 months during the second-line therapy with nivolumab plus chemotherapy. (D) PD-L1 expression in the metastatic supraclavicular lymph node tissue after ceritinib treatment by immunohistochemistry (PD-L1 clone SP142). Magnification: ×100. (E) MRI images of the brain at 8.9 months and 11.3 months during the third-line therapy with lorlatinib. (F) CD74–ROS1 and CD74–ROS1 F2004L overexpression in Ba/F3 cells (with flag tag). (G) Proliferation of CD74–ROS1 fusion and CD74–ROS1 F2004L overexpressed Ba/F3 cells treated with ceritinib (100 nM) or lorlatinib (100 nM). Red arrow, tumor area. ICT, immune-chemotherapy; PD-L1, programmed cell death ligand 1.
However, the disease progressed at the end of July as PET-CT revealed multiple lymph nodes metastases and bone destruction. The largest newly metastatic lymph node was in the right armpit with a short diameter of about 2.1 cm (figure 1C), while the primary lung lesion has regressed (not shown). A second NGS assay found a possible resistance mutation of c.6012T>G (p.F2004L) (MAF 1.65%) in ROS1 kinase domain in the plasma circulating tumor DNA in addition to the ROS1 fusion. And a PD-L1 assay (SP142 staining) of a repeat biopsy tissue sample from the supraclavicular lymph node showed that the expression of PD-L1 in both tumor cells and immune cells was 10% (figure 1D). For the high expression of PD-L1 and the unavailability of lorlatinib at that time, eight cycles of immunotherapy plus chemotherapy with nivolumab (200 mg, d1), nedaplatin (120 mg, d1), and pemetrexed (800 mg, d1) every 3 weeks were started to administered to the patient. After four cycles of ICT, PET-CT scans showed that the primary tumor disappeared, all metastatic lymph nodes were regressed, and bone destruction was well controlled. And the largest metastatic lymph node in the right armpit also disappeared (figure 1C). The patient achieved a partial response to ICT.
Unfortunately, it was not long before the disease progressed again. After six cycles of ICT on December 4, 2019, PET-CT showed suspected brain metastases, which were confirmed by MRI of the brain 2 weeks later (figure 1E). Then the patient received 10 brain radiation treatments and completed the remaining cycle of ICT. At the same time, we confirmed the transforming ability and the sensitivity to lorlatinib of the F2004L mutant CD74–ROS1 fusion in Ba/F3 cells (figure 1F,G). On the other hand, ultrasonography showed multiple enlarged lymph nodes after radiotherapy. Therefore, the third-generation tyrosine kinase inhibitor (TKI) lorlatinib, which is potent for brain metastases, was administered to the patient (100 mg orally once a day). Fortunately, brain metastases responded quickly to lorlatinib (figure 1E), and the previously enlarged lymph nodes also shrank to normal size. The patient continued to take lorlatinib and has not experienced disease progression so far.
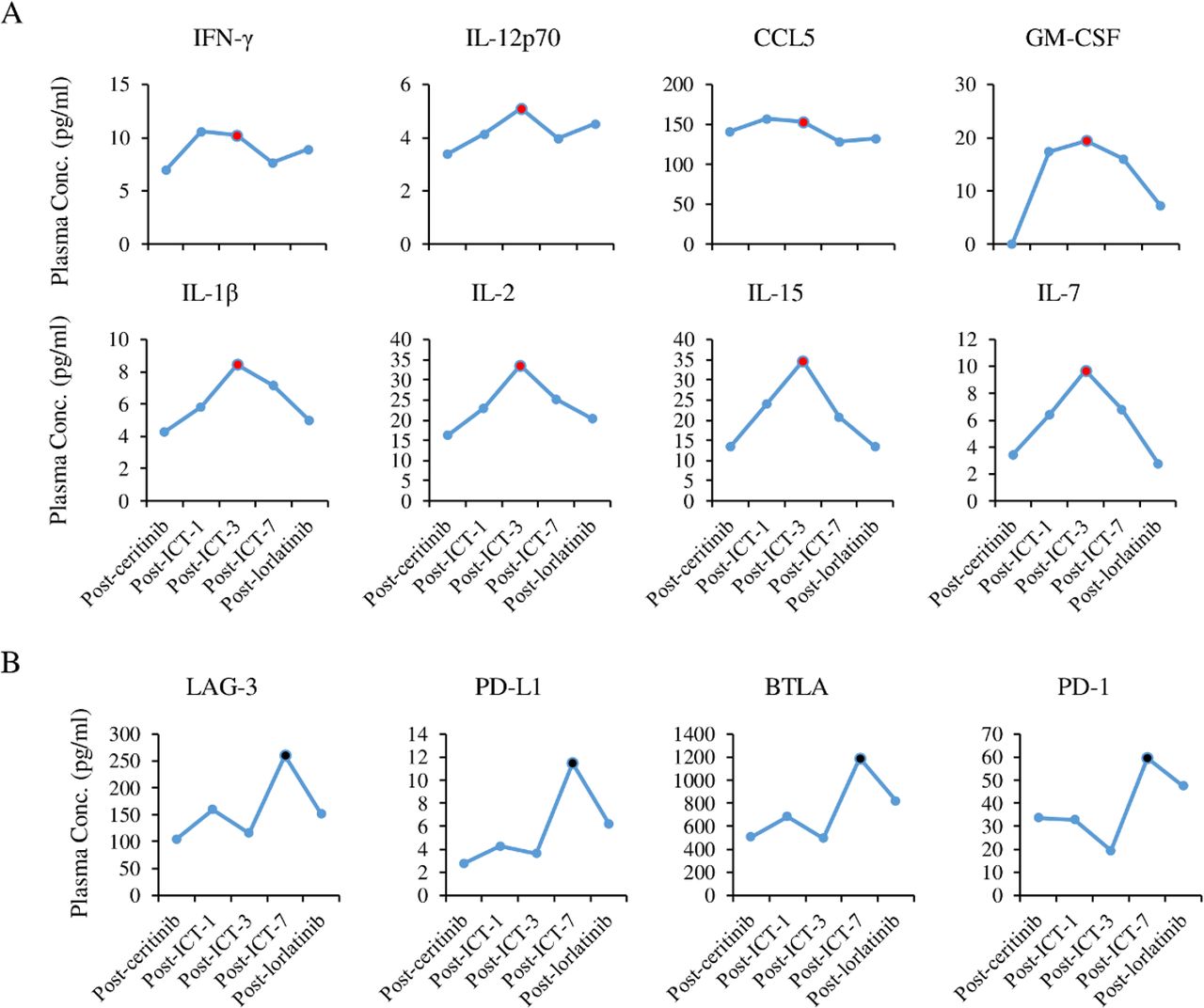
The rapid response and resistance of the disease to nivolumab-based therapy was so expressive that we further investigated the TIME and peripheral plasma immune-related proteins on samples at time points as shown in figure 2A. TIME was examined by multiplex immunohistochemistry (mIHC) and RNA sequencing. The mIHC assay was designed for simultaneous detection of CD8 (clone SP16), CD68 (clone KP1), CD57 (clone NK-1), PD-1 (clone UMAB199), and PD-L1 (clone E1L3N) using the Opal seven-color IHC Kit (PerkinElmer, USA), and RNA sequencing targeting 396 immune-related genes is based on the Oncomine Immune Response Research Assay (Thermo Fisher Scientific, USA). The results show that the infiltration of CD8+ cytotoxic T cells and CD68 macrophages and expression of T cell response-related genes increased after three cycles of ICT, demonstrating an impetus of ICT to antitumor immune response (figure 2B,C). However, it is noteworthy that PD-L1 positive cells mounted up since the first-line ceritinib treatment (figure 2D,E). Conceptually, if the immunotherapy worked very well, the expression of PD-L1 would decrease with the reduction of tumor cells. It is rational to assume that upregulation of PD-L1 expression during immunotherapy might hint an imminent relapse. Plasma immune-related proteins were investigated by ELISA-based multiplex immunoassay (ThermoFisher, USA). The results show that pro-inflammatory factors such as interferon gamma (IFN-γ), interleukin 12 (IL-12), interleukin 2 (IL-2), and interleukin 15 (IL-15) were increased during the first three cycles of ICT (figure 3A), while inhibitory checkpoint proteins, B and T lymphocyte attenuator (BTLA), PD-L1, lymphocyte-activation gene 3 (LAG-3), and PD-1, were increased after seven cycles of ICT (figure 3B). Coincidentally, the disease responded to ICT at the third cycle of treatment and progressed with the brain metastases at the seventh cycle. The immune system seemed to be activated and contributed to the initial partial tumor response to immune-chemotherapy, which was consistent with results of the active TIME indicated by mIHC and RNA sequencing, and was inhibited and defeated by cancer during the later stage of treatment. Taken together, it is suggested that immune features of tumor microenvironment and signatures of peripheral plasma immune proteins could predict the response to ICT.

Immune features of tumor microenvironment during the early stage of ICT treatment. (A) Timeline of the patient’s therapeutic course, sample collection, and corresponding studies. (B) Percentages of CD8+, CD68+, and CD57+ cells in all nucleated cells in metastatic lymph node tissue before and after ceritinib treatment, and after three cycles of ICT by mIHC assay. (C) Heatmap of T cell response-related gene expression. (D) Percentages of PD-1 and PD-L1 positive cells in all nucleated cells in metastatic lymph node tissue by mIHC assay. (E) Representative images of PD-L1 expression in (D) (PD-L1 clone E1L3N). Magnification: ×200. Tumor response was evaluated according to RECIST version 1.1 criteria. ICT, immune-chemotherapy; mIHC, multiplex immunohistochemistry; Nivo, nivolumab; NGS, next-generation sequencing; PD, progressive disease; PD-L1, programmed cell death ligand 1; PR, partial response; RECIST, Response Evaluation Criteria in Solid Tumors; RNAseq, RNA sequencing.
{kind=link}
{kind=link}
{kind=link}
Dynamic changes of immune-related proteins in plasma. Plasma concentration of pro-inflammatory factors (A) and immune checkpoint proteins (B) before ceritinib treatment, and after one, three, and seven cycles of ICT, and one month after lorlatinib treatment. Black dot, the time point of disease progression during ICT; red dot, the time point of partial response to ICT. BTLA, B and T lymphocyte attenuator; CCL5, C-C motif chemokine ligand 5; GM-CSF, granulocyte-macrophage colony-stimulating factor; ICT, immune-chemotherapy; IFN-γ, interferon gamma; IL, interleukin; LAG-3, lymphocyte-activation gene 3; PD-L1, programmed cell death ligand 1.
Discussion
This ROS1-positive NSCLC patient experienced a short-term response to ceritinib treatment and second-line nivolumab-based therapy, and a long-term benefit from lorlatinib. We identified a ceritinib-resistant lorlatinib-sensitive mutation ROS1 F2004L in this patient, and found features of tumor microenvironment and plasma immune-related factors reflecting the immune function that might predict the response to ICT.
As the common intrinsic mechanisms of resistance to ROS1 TKIs, many secondary ROS1 mutations have been reported in preclinical or clinical studies, such as substitutions at solvent front residues (G2032, D2033, and L1951) or the ‘gatekeeper’ residue (L2026).9 Although F2004L has not been reported in either clinical patients or in vitro experiments, ROS1 F2004C/I/V mutations were identified in several ROS1-positive NSCLC patients.10 11 Particularly, one patient with CD74–ROS1 positive lung adenocarcinoma had a dramatic response to lorlatinib after treated with crizotinib and entrectinib and developing a ROS1 F2004V secondary mutation.11 Hence, our case is the second reported patient with resistance mutation at F2004 residue that responds well to lorlatinib, adding evidence for the use of this agent in patients with similar molecular characteristics.
Identifying effective predictive biomarker for ICIs is still an urgent need in this era of cancer immunotherapy. Current focuses have been on PD-L1 expression, tumor mutational burden, immune gene signatures, and tumor infiltrating cytotoxic T lymphocytes. However, immune-related proteins in circulating blood could also be potential biomarkers. High levels of soluble LAG-3 or PD-1 in pretreatment serum samples were associated with resistance to ICI treatment in melanoma, and PD-1 serum levels were found increased with treatment in resistance patients.12 In addition, circulating immune checkpoint proteins have prognostic value in patients with clear cell renal cell cancer,13 pancreatic adenocarcinoma,14 and nasopharyngeal carcinoma,15 with high levels predicting poor survival outcomes. In this case, plasma PD-1, PD-L1, BTLA, and LAG-3 were all increased in the late period of immunotherapy treatment, likely predicting the disease progression.
A recent study suggests that PD-L1/PD-1 blockade could be the second-line treatment option based on the correlation of ROS1 fusion with PD-L1 expression.4 Two patients with ROS1 fusion have been reported to respond well to immunotherapy.16 However, PD-L1 expression was upregulated in this ROS1-rearranged NSCLC patient after ceritinib treatment but did not bring about a long-term benefit from ICT. One of the reasons may be the biopsy site, as recently Hong and colleagues reported that PD-L1 in lymph node biopsies could not predict benefit from ICIs.17 In brief, the efficacy of checkpoint inhibitor-based immunotherapy in ROS1-positive NSCLC need more studies.
In summary, this case report provides a valuable reference for ICI-based therapy in patients with PD-L1-positive ROS1-rearrangement NSCLC, and suggests that ICT might not be a better option than lorlatinib regimen in the second-line setting. Moreover, the study of immune features during treatment brought new insights to plasma immune-related proteins and PD-L1 expression, changes of which might predict the response to immunotherapy.
Acknowledgments
The authors wish to gratefully acknowledge the patient and his family for allowing us to publish his clinical case.
Footnotes
DY, JQ and ZC contributed equally.
Contributors DY, JQ, and ZC contributed equally to this work and are co-first authors. DY was the main treating physician and designed the study. ZC, BZ, PC, and JL performed the experiments and collected the data. JQ, ZC, and DY analyzed the data. The manuscript was drafted by JQ and edited by LZ. HZ and CW are the study guarantors. All authors have read and approved the final manuscript.
Funding This study was supported by the National Key Sci-Tech Special Project of China (NO. 2018ZX10302207).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Ethics Committee of Tianjin Medical University Cancer Institute and Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.