Article Text

Abstract
Assessment of programmed cell death-ligand 1 (PD-L1) expression by immunohistochemistry (IHC) is the definite diagnostic test to guide treatment for patients with advanced-stage non-small cell lung cancer. Intratumoral heterogeneity and discrepancy of PD-L1 expression between primary and metastatic lesions may increase the risk of tumor misclassification. We performed a retrospective study of the Foundation Medicine, Inc clinical database on lung cancer cases that were evaluated for PD-L1 expression by IHC in the context of routine care. All cases were assessed with the Food and Drug Administration-approved 22C3 pharmDx assay and scoring system. 15,028 lung cancer cases, including 8285 primary tumors and 6743 unmatched metastatic lesions were analyzed. Metastatic lesions (mets) were more frequently high positive (tumor proportion score (TPS) ≥50%) for PD-L1 expression than primary lesions (33.8% vs 28.4%; OR, 1.28; 95% CI, 1.19 to 1.37; p<0.001). Higher levels in mets than primaries were seen in samples from lymph nodes, pleural fluid, soft tissue and adrenal gland but not in those from liver, brain and bone. Metastatic lesions of patients with non-squamous histology were more likely to have TPS ≥50% in comparison with primary (OR, 1.37; 95% CI, 1.27 to 1.49; p<0.001), but this was not the case for patients with squamous histology (OR, 0.89; 95% CI, 0.74 to 1.06; p=0.197). PD-L1 expression varies with respect to histologic subtype, sampling site and gender, but is generally higher in metastatic sites. This observation may affect future patient management and trial design.
- biomarkers
- tumor
- immunohistochemistry
- immunotherapy
- lung neoplasms
- programmed cell death 1 receptor
Data availability statement
Data are available upon reasonable request. Data requests may be submitted to Dr Richard SP Huang (rhuang@foundationmedicine.com) at Foundation Medicine.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Many patients with non-small cell lung cancer (NSCLC) lack targetable driver mutations and so, immunotherapy has become integrated into their first-line therapeutic options. KEYNOTE-024 trial showed that patients with high programmed death-ligand 1 (PD-L1) expression and tumor proportion score (TPS) ≥50% have significantly improved clinical outcomes when treated with pembrolizumab monotherapy.1 Anti-programmed cell death protein 1 (PD-1) therapy has, therefore, established PD-L1 expression assessment by immunohistochemistry (IHC) as routine practice in lung cancer as well as other tumor types. Despite its promising applications, detection of PD-L1 expression varies among different sampling sites, complicating therapeutic decisions.2–5 Intratumoral heterogeneity and discrepancy of PD-L1 expression between primary and metastatic lesions have been reported in several studies.2 5 In the clinical setting, metastatic sites are often the only accessible source for PD-L1 evaluation. Hence, validation of the concordance in PD-L1 TPS between primary and metastatic sites is necessary to eliminate the risk of tumor misclassification.6 Here, we used the Foundation Medicine, Inc (FMI) PD-L1 IHC database to assess real-world potential differences in PD-L1 protein expression, as measured by PD-L1 TPS, between primary and metastatic lesions of patients with lung cancer. For our comparisons we used the ≥50% cut-off, as this has been previously shown to have the highest level of reproducibility between pathologists.7
Methods
Approval for this study, including a waiver of informed consent and a HIPAA waiver of authorization, was obtained from the Western Institutional Review Board (Protocol No. 20152817). A retrospective data analysis of the FMI clinical database was conducted on lung cancer cases that were assessed for PD-L1 expression in the context of routine care. All samples were stained with the PD-L1 IHC 22C3 pharmDx assay at FMI North Carolina laboratory. PD-L1 expression was evaluated and scored with the TPS scoring methodology: TPS=Number of PD-L1 positive tumor cells/(Total number of PD-L1 positive + PD-L1 negative tumor cells) × 100%. A tumor was considered PD-L1 high if TPS ≥50%. Multivariable logistic-regression models were used to examine the relationship between PD-L1 expression level and other variables including age, gender, sampling site and histologic subtype. Since this is a real-world dataset, outcome variables and some clinical variables like stage and grade were not collected by the FMI lab since that is not required to provide clinical testing.
From the eight different subtypes, we focused on two; lung squamous cell carcinoma (LUSC) and non-squamous NSCLC that includes lung adenocarcinoma, NSCLC not otherwise specified and lung large cell carcinoma. In all tests, two-sided p values of <0.05 were considered significant. Statistical analysis was conducted using Prism V.8 software and RStudio V.4.0.1.
Results
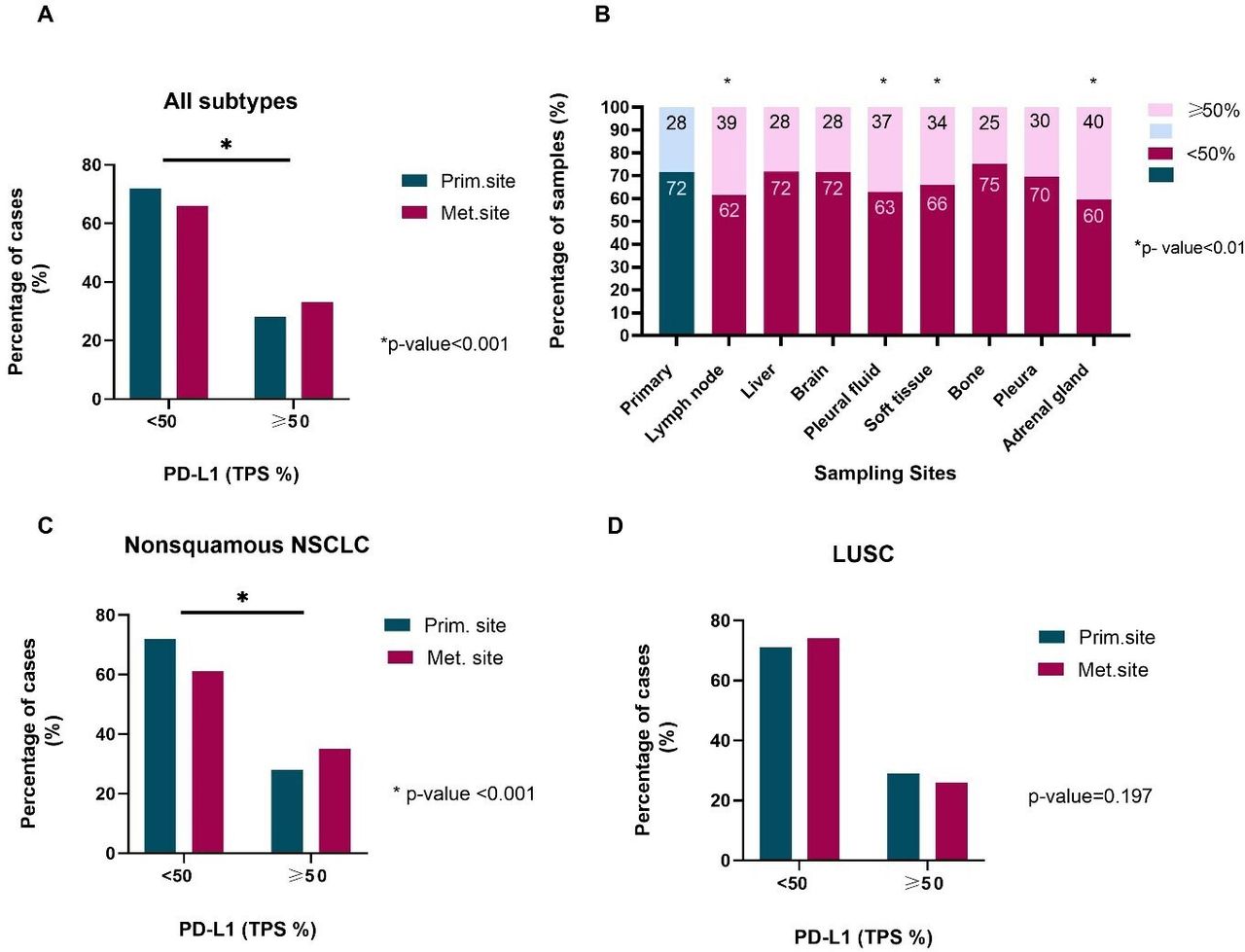
A total of 15,028 samples from 7599 male and 7429 female patients with lung cancer, with a median age of 68 years (range 19–90) were analyzed; 8285 samples were from primary and 6743 from metastatic lesions, representing 55 different metastatic sites (table 1). In general, samples obtained from metastatic lesions were more likely to be PD-L1 high compared with those from the primary site (33.8% vs 28.4%; OR, 1.28; 95% CI, 1.19 to 1.37; p<0.001; table 2, figure 1A). The absolute difference between the rate of PD-L1 high patients when PD-L1 TPS was measured at a metastatic site, and the average rate of PD-L1 high patients in the study population, when PD-L1 TPS was measured at both primary and metastatic sites, was 2.9% (33.8% vs 30.8%; 95% CI, 1.6% to 4.3%). Substantial heterogeneity was observed across different metastatic sites. Among the eight most common metastatic sites, high PD-L1 expression was, statistically significantly, more frequent in samples obtained from lymph nodes (OR, 1.58; 95% CI, 1.43 to 1.74; p<0.001), pleural fluid (OR, 1.48; 95% CI, 1.23 to 1.78; p<0.001), soft tissue (OR, 1.30; 95% CI, 1.08 to 1.58; p=0.007) and adrenal gland (OR, 1.70; 95% CI, 1.30 to 2.22; p<0.001) compared with primary site (table 2, figure 1B). This was not the case with metastatic lesions from pleura (OR, 1.12; 95% CI, 0.89 to 1.40; p=0.343), liver (OR, 0.98; 95% CI, 0.83 to 1.16; p=0.835), brain (OR, 1.00; 95% CI, 0.85 to 1.18; p=0.994) and bone (OR, 0.83; 95% CI, 0.67 to 1.04; p=0.101).
{kind=link}
(A) Comparison of PD-L1 TPS between primary and metastatic sites; all subtypes. (B) PD-L1 TPS stratified by sampling site. (C) Comparison of PD-L1 TPS between primary and metastatic sites; non-squamous NSCLC. (D) Comparison of PD-L1 TPS between primary and metastatic sites; LUSC. LUSC, lung squamous cell carcinoma; NSCLC, non-small cell lung cancer; PD-L1, programmed death-ligand 1; TPS, tumor proportion score.
Clinicopathologic characteristics
Multivariate analysis (dependent variable: TPS, independent variables: age, gender, primary, metastatic sites, subtypes)
In patients with non-squamous NSCLC, metastatic lesions were more likely to have high PD-L1 expression (OR, 1.37; 95% CI, 1.27 to 1.49; p<0.001) versus primary site lesions; the trend was reversed for LUSC patients (OR, 0.89; 95% CI, 0.74 to 1.06; p=0.197; table 2, figure 1C,D). Furthermore, age and gender are known to alter immune surveillance8 9; there was a higher probability of women having TPS ≥50% (OR, 1.08; 95% CI, 1.01 to 1.16; p=0.027) versus men; driven by the higher TPS of LUSC female patients (OR, 1.23; 95% CI, 1.04 to 1.44; p=0.015; table 2). Age was statistically significant only in the LUSC subtype (OR, 0.61; 95% CI, 0.37 to 0.99; p=0.046).
Discussion
In this study, we used a very large real-world lung cancer cohort, to comprehensively assess the intertumoral heterogeneity of PD-L1 expression in non-paired primary and metastatic specimens. We focused on negative or low versus high TPS values for PD-L1 expression (TPS <50% and TPS ≥50%, respectively), since this cut-off is the most reproducible among ‘real-world’ pathologists.1 7 We found high PD-L1 expression (TPS ≥50%) in 28.4% of the primary versus 33.8% of the metastatic lung cancer samples (OR, 1.28; 95% CI, 1.19 to 1.37; p<0.001; tables 1 and 2). This suggests that sampling of lung cancer at a metastatic site is more likely to result in high PD-L1 expression, consistent with previous studies.2 5 6
Subsequently, we compared TPS between various metastatic sites to the primary site. We saw that samples obtained from lymph nodes, pleural fluid, soft tissue and adrenal gland were more likely to be PD-L1 high than those obtained from the primary tumor site; samples from pleura, liver, brain and bone were not.3 10 A lower or negative TPS from these sites (pleura, liver, brain and bone) could preclude otherwise eligible patients from receiving immunotherapy when metastatic site is the preferred sampling site.
Site of metastasis seems to play an important role in PD-L1 expression. Immune surveillance differs among organs and consequently alters susceptibility to cancer dissemination. Through plasticity of clonal evolution of NSCLC over time, selective metastases may occur resulting in subclones of variable tumor grade and PD-L1 expression in metastatic sites.11 A recent study in patients with NSCLC showed that PD-L1 expression in metastatic lymph nodes was not correlated with clinical outcomes.10 Interestingly, data from the FMI database on triple negative breast cancer showed that PD-L1 positivity rates were significantly higher in primary tumors rather than metastatic lesions, indicating a reverse trend from our results in lung cancer.12 However, in that study PD-L1 expression was scored on immune cells and the cut-off for positivity was 1%, precluding direct comparisons.
In addition, we observed significant deviations in PD-L1 TPS according to histologic subtype. Patients with non-squamous histology were more likely to have high TPS in metastatic rather than primary lesions (OR, 1.37; 95% CI, 1.27 to 1.49; p<0.001). However, results were not significant for patients with squamous histology. Similar studies have reported subtype as an independent variable linked with PD-L1 expression but with conflicting results.10 13 14 Differences in PD-L1 protein expression between squamous and non-squamous NSCLC may extend beyond the distinct morphology of squamous tumor cells and their ability to produce keratin, that can affect IHC staining patterns. Tumor microenvironment also varies between the two subtypes, indicating differences in immunogenicity that can in part explain the observed discordances in PD-L1 expression.1 15 16 Importantly, younger (OR, 0.61; 95% CI, 0.37 to 0.99; p=0.046) and female (OR, 1.23; 95% CI, 1.04 to 1.44; p=0.015) patients with LUSC were more likely to have high PD-L1 TPS. A recent meta-analysis showed comparable efficacy of PD-1/PD-L1 axis inhibitors in adults younger and ≥65 years of age.17 Current literature suggests differences in antigenicity between tumors from male and female patients; overall survival data from a meta-analysis in patients with lung cancer indicated that men derive a statistically significantly larger benefit from PD-1 monotherapy than women, whereas women benefit more from the addition of chemotherapy to immunotherapy.18 19
The limitations of this work include the facts that the study is retrospective, and the samples are not matched since obtaining matched samples from both primary and metastatic sites is only rarely clinically indicated. As tissue accessibility drives routine patient care, real-world studies of matched specimens may never be done. Also, due to lack of that information, we were unable to control for factors that are known to be related with PD-L1 expression, such as smoking status, stage and mutation status.
In conclusion, this study demonstrates that PD-L1 TPS is significantly associated with the histologic type and with primary versus metastatic sampling sites. This work may raise awareness of this variable for future trial design and have impact on patient management.
Data availability statement
Data are available upon reasonable request. Data requests may be submitted to Dr Richard SP Huang (rhuang@foundationmedicine.com) at Foundation Medicine.
Ethics statements
Ethics approval
Approval for this study, including a waiver of informed consent and a HIPAA waiver of authorization, was obtained from the Western Institutional Review Board (Protocol No. 20152817).
Acknowledgments
Dr Moutafi and Dr Vathiotis were supported by a scholarship from the Hellenic Society of Medical Oncologists (HESMO).
References
Footnotes
Contributors MKM, WW and WT helped in data analysis and writing. RH, JH, BA, SR and JSR helped in writing the manuscript. LP and KS performed data interpretation. IAV helped in the data analysis, concept, design, data interpretation and writing. DLR was involved in concept, design, data interpretation and writing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests RH, JH, BA, SR and JSR are employees of Foundation Medicine. DLR has served as an advisor for AstraZeneca, Agendia, Amgen, BMS, Cell Signaling Technology, Cepheid, Daiichi Sankyo, Genoptix/Novartis, GSK, Konica Minolta, Merck, NanoString, PAIGE.AI, Perkin Elmer, Roche, Ventana and Ultivue, and received research funding from AstraZeneca, Cepheid, NavigateBP, NextCure, Nanostring, Lilly and Ultivue. LP has received consulting fees and honoraria from AstraZeneca, Merck, Novartis, Bristol-Myers Squibb Genentech, Eisai, Pieris, Immunomedics, Seattle Genetics, Clovis, Syndax, H3Bio and Daiichi.
Provenance and peer review Not commissioned; externally peer reviewed.