Article Text

Abstract
Background Gastrointestinal (GI) cancer is the second most common cancer type with mismatch repair-deficient (dMMR)/microsatellite instability-high (MSI-H) phenotype that is expected to respond to immune-checkpoint inhibitors (ICIs). However, approximately half of the patients with dMMR/MSI-H GI cancer derive no benefit from ICIs. We sought to identify the predictors of primary resistance to ICIs in dMMR/MSI-H GI cancer.
Methods Three independent cohorts were included: (1) the discovery cohort (65 patients with dMMR/MSI-H GI cancer) with ICI efficacy data and pre-ICIs tissue samples for genomic profile and tumor immune infiltration; (2) the validation cohort (22 patients with dMMR/MSI-H GI cancer) with ICI efficacy data and pre-ICIs plasma samples for genomic profile; and (3) the TCGA (The Cancer Genome Atlas) cohort not receiving ICIs (152 patients with MSI-H GI cancer) with genomic profile and survival data.
Results AKT1 and CDH1 mutations were identified as independent predictors of poor progression-free survival (PFS) and primary resistance to ICIs in dMMR/MSI-H GI cancer. We combined these two genes as an immuno-oncology therapy predictor (IOpred), which could recognize 52.4% (11/21) of dMMR/MSI-H patients with primary resistance to ICIs with a positive predictive value (PPV) of 91.7% (11/12). Receiver operating characteristic analysis demonstrated IOpred with a good performance in predicting primary resistance (area under the curve 0.751). Patients with IOpred-Mut (mutant AKT1 or CDH1) GI cancer had significantly shorter PFS (HR=8.36, p<0.001) and overall survival (OS, HR=5.17, p<0.001) than IOpred-WT (wild-type for both AKT1 and CDH1) cases upon ICI treatment. The validation cohort also confirmed the correlation between IOpred-mutation and poorer prognosis (PFS, HR=4.68, p=0.004; OS, HR=15.98, p<0.001) in dMMR/MSI-H patients after ICIs. The PPV of IOpred in identifying primary resistance to ICIs was 80% (4/5) in the validation cohort. Additionally, IOpred-WT patients could be further stratified by tumor mutational burden (TMB), wherein TMB-low patients (TMB ≤26.19 mutations per megabase (Mb)) had a significantly higher primary resistance rate to ICIs (34.8% vs 6.7%, p=0.014) and poorer PFS (HR=3.46, p=0.008) and OS (HR=4.42, p=0.047) than TMB-high patients (TMB >26.19 mutations/Mb).
Conclusions IOpred was identified as a powerful predictor of primary resistance to ICIs in dMMR/MSI-H GI cancer, which might serve as a promising biomarker to help guide immunotherapy decision-making.
- immunotherapy
- immunohistochemistry
- biomarkers, tumor
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Although Food and Drug Administration has approved immune checkpoint inhibitors (ICIs) for mismatch repair-deficient (dMMR)/microsatellite instability-high (MSI-H) gastrointestinal (GI) cancer treatment, approximately half of patients with dMMR/MSI-H GI cancer exhibit primary resistance to ICIs, suggesting that identifying an effective biomarker for predicting ICI therapy is an urgent unmet clinical need.
What this study adds
AKT1 and CDH1 mutations are identified as independent predictors of poor progression-free survival and primary resistance to ICIs in dMMR/MSI-H GI cancer.
The combination of AKT1 and CDH1 mutations as an immuno-oncology therapy predictor (IOpred) has a good performance in predicting primary resistance (area under the curve 0.751), which could recognize 52.4% (11/21) of dMMR/MSI-H patients with primary resistance to ICIs with a positive predictive value of 91.7% (11/12).
How this study might affect research, practice or policy?
In view of the predictive role of IOpred for primary resistance to ICIs, IOpred might guide clinical decision-making that the dMMR/MSI-H patients with IOpred-mutation should not be recommended for ICI therapy.
IOpred can be easily translated into an easy-to-use clinical assay due to only detection of two decisive common genes, and could be recommended for routine clinical care in dMMR/MSI GI cancer.
Background
Gastrointestinal (GI) cancer, one of the most common causes of cancer-related death worldwide, has the second-highest prevalence of DNA mismatch repair-deficient (dMMR)/microsatellite instability-high (MSI-H) after endometrial cancer.1 dMMR/MSI-H is observed in 3%–14% of advanced gastric cancer (GC) cases and approximately 5% of metastatic intestinal cancer (IC) cases.2–5 The clinical efficacy of immune-checkpoint inhibitors (ICIs) in advanced or metastatic dMMR/MSI-H GI cancer has been well validated in several phase II and III studies with an objective response rate (ORR) ranging from 33.0% to 57.1%.5–8 Although these promising results have led to Food and Drug Administration approval and National Comprehensive Cancer Network recommendation of ICIs for dMMR/MSI-H GI cancer treatment, approximately half of the patients in these pivotal trials do not respond to ICIs.
To date, the reasons why these patients could not benefit from ICIs mainly fall into two categories: the misdiagnosis of dMMR/MSI-H status and intrinsic resistance to ICI therapy.9–11 Therefore, correct identification of dMMR/MSI-H status and uncovering the molecular mechanisms of resistance are critical for screening patients who could benefit from ICI treatment. Indeed, this might have fuelled a wave of research into the molecular mechanisms of tumor-intrinsic resistance to ICIs.9 10 12 13 Although the molecular mechanisms of resistance remain to be clarified, an effective biomarker predictive of response to ICIs has been an urgent unmet clinical need to inform immunotherapy of dMMR/MSI-H GI cancer. Several potential biomarkers have been proposed, including cytosolic DNA, PTEN mutations, and tumor mutational burden (TMB). Lu et al12 demonstrated that cytosolic DNA induces the release of interferon-β in a cGAS-STING-dependent manner and cascade activation of antigen-presenting cells and T cells, and thus increases the sensitivity to ICIs, but the clinical evidence was obtained from only seven patients with MSI-H colorectal cancer (CRC). PTEN mutations, especially mutations in the phosphatase domain, were reported by one recent retrospective study with a small sample size (N=38) related to response to programmed cell death protein-1 (PD-1) blockade in dMMR/MSI-H GI tumors, but the necessary validation was lacking.14 Three studies with small sample sizes (N=19, 38, and 22, respectively) indicated low TMB level to be a negative predictor of response to ICIs in dMMR/MSI-H GI cancer,4 14 15 whereas Bortolomeazzi et al16 demonstrated no correlation between TMB and ICI response in hypermutated CRC with TMB >12 mutations per megabase (Mb) by analysis of the KEYNOTE 177 trial and validation cohorts (N=29). Besides, TMB also encounters several challenges, the biggest of which is no clear consensus on the TMB cut-off threshold, limiting TMB as a universal biomarker.
In this study, through next-generation sequencing (NGS)-based genome sequencing of pre-immunotherapy tissue samples from 65 patients with at least dual-tech proven dMMR/MSI-H GI tumor who received ICI therapy, we explored the correlations of ICI efficacy with gene mutation, TMB, insertion and deletion (indel) burden, intratumor genetic heterogeneity (ITH), chromosome instability, and clinical features. Then we developed an immuno-oncology therapy predictor (IOpred) by combing the independent candidate genes together and validated the IOpred in an independent cohort with 22 patients with dMMR/MSI-H GI cancer. We also investigated the IOpred’s potential mechanisms related to ICI efficacy by immune microenvironment analysis through multiplex immunofluorescence (mIF).
Methods
Study design and population
The study consisted of three major phases: (1) biomarker discovery in an ICI cohort using the genetic profile through tissue-based NGS; (2) biomarker validation in an ICI cohort characterized by a plasma-based NGS panel; and (3) mechanism exploration in the biomarker discovery cohort. The study design and consort patient flow diagram were illustrated in online supplemental figure 1.
Supplemental material
The discovery cohort included 65 patients with advanced or metastatic dMMR/MSI-H GI cancer consisting of 50 patients with IC and 15 patients with GC, who had received ICI therapy at Peking University Cancer Hospital and Institute from February 14, 2016, to December 10, 2020. Their tumor tissues were collected along with matched white blood cell samples prior to immunotherapy and had concordant-dMMR/MSI-H status by NGS (100 microsatellite loci) and immunohistochemistry (IHC)/polymerase chain reaction (PCR, five microsatellite loci) testing. In this cohort, biomarkers were screened via a sequential two-step process involving a significant association with progression-free survival (PFS and primary resistance. The selected gene mutations as biomarkers also needed to meet the criteria with a mutation frequency of ≥5%.
The validation cohort consisted of 22 cases with advanced or metastatic dMMR/MSI-H GI cancer with 16 cases with IC and 6 cases with GC receiving ICI therapy at Peking University Cancer Hospital and Institute from July 22, 2016, to October 11, 2019. The blood samples were collected before immunotherapy initiation. In the discovery and validation cohort, the data of dMMR determined by IHC and MSI-H identified by PCR were collected from medical records. Other information regarding age, sex, prior therapy, personal/family cancer history, TNM (tumor, node, metastases) stage, location of metastases, the number of metastatic sites, and human epidermal growth factor receptor 2 (HER2) and programmed death-ligand 1 (PD-L1) expression was also collected from medical records.
The Cancer Genome Atlas (TCGA) cohort (n=152) was obtained from the TCGA PanCancer Atlas, wherein the patients meeting the following criteria were included: (1) MSI-H phenotype diagnosed by PCR; (2) no experience of ICI therapy; and (3) available clinical and genetic data.17–19 We utilized this cohort to investigate the prognostic value of the identified biomarkers.
Written informed consents were obtained from all the participants involved in this study. This report followed the Standards for Reporting of Diagnostic Accuracy (STARD) statement.
Outcome
The tumor response was assessed as per the Response Evaluation Criteria in Solid Tumors (RECIST), V.1.1, and categorized as complete response (CR), partial response (PR), stable disease (SD), disease progression (PD), or not evaluable (NE). ORR was defined as the proportion of patients whose best overall response was CR or PR. PFS was defined as the time from ICI treatment initiation to PD or death, whichever occurred first. Overall survival (OS) was defined as the time from the initiation of ICI treatment to death from any cause. Primary resistance was defined as PD at the time of the first tumor assessment, NE caused by death within 3 months, or SD with PFS <6 months after starting immunotherapy, according to recommendations from the first meeting of the Society for Immunotherapy of Cancer (SITC) Immunotherapy Resistance Taskforce.20 21 The patients with primary resistance to ICIs were called ICI-resistant patients, and the rest were ICI-sensitive patients.
NGS, PCR, IHC, mIF, copy number alteration (CNA) by CNApp, and ITH by mutant-allele tumor heterogeneity (MATH) were described in online supplemental methods. The gene lists of the panels for tissue and plasma DNA testing were attached in online supplemental tables 1–3.
Statistical analysis
The difference between the two groups was tested using the Mann-Whitney U test for continuous variables, Fisher’s exact test for binary variables, and Χ2 test for multi-categorical variables. Survival analysis was realized by both Kaplan-Meier product-limit method and Cox proportional hazards method, and the latter was utilized to screen candidate biomarkers correlated with ICI efficacy. Multivariate exact logistic and Cox proportional hazards regression analyses were performed to analyze the independence of the candidate biomarkers for predicting primary resistance and PFS, respectively. The receiver operating characteristic (ROC) curve and the corresponding area under the curve (AUC) calculation were realized by the R package pROC to evaluate the predictive accuracy of IOpred and to determine the optimal cut-off value of TMB for the discrimination between ICI-resistant and ICI-sensitive patients.22 All reported p values were two-tailed, and a p value of <0.05 was considered statistically significant unless otherwise stipulated. Statistical analyses were performed using R software, V.3.6.1 (R Foundation for Statistical Computing), and Python software, V.3.9.5.
Results
Patient characteristics
We performed biomarker screening in the discovery cohort, including 65 patients with GI cancer receiving ICI therapy. In this cohort of 50 patients with IC and 15 patients with GC, all patients were NGS-MSI-H, wherein 38 patients had consistent dMMR and MSI-H phenotype previously identified by IHC and PCR, 26 patients were IHC-identified dMMR without available PCR data, and 1 patients was PCR-MSI-H without available IHC data. The baseline characteristics of the patients were summarized in table 1. Fifty-seven (57/65, 87.7%) patients received anti-PD-1/PD-L1 monotherapy, and eight (8/65, 12.3%) patients were administered combination therapy of anti-PD-1/PD-L1 plus anti-cytotoxic T‐lymphocyte antigen‐4. With a median follow-up time of 27.3 months, the ORR to ICIs was 53.9%, including 29 PR and 6 CR. Median PFS (mPFS) and median OS (mOS) were 10.4 and 20.2 months, respectively. According to the definition of primary resistance, 65 patients were assigned into ICI-resistant (21, 32.3%) and ICI-sensitive (44, 67.7%) subgroups. Demographic and baseline characteristics were generally well balanced between the two subgroups.
Basic characteristics of the patients with dMMR/MSI-H GI cancer in the discovery cohort
Identification of gene mutations associated with primary resistance to ICIs
To investigate what factors may affect the benefits of immunotherapy in patients with dMMR/MSI-H GI cancer, we assessed the correlation of genomic features with PFS in the discovery cohort. We first examined whether particular gene mutations were associated with PFS by the univariate Cox proportional hazards regression model. The frequently mutated genes were summarized in online supplemental figure 2. Mutations in three genes, AKT1, CUL3, and CDH1, were all identified significantly correlated with PFS (adjusted p=0.013 for AKT1; adjusted p=0.046 for CUL3; and adjusted p=0.046 for CDH1) (figure 1A). Then we further investigated the association of mutations in three candidate genes with primary resistance to ICIs. There were significant differences in the frequency of AKT1 (p=0.002) and CDH1 (p=0.005) mutations but not CUL3 (p=0.080) mutations between ICI-sensitive and ICI-resistant subgroups. AKT1 and CDH1 mutations were significantly enriched in the ICI-resistant subgroup compared with the ICI-sensitive subgroup (figure 1B). Besides, the frequency of AKT1 (6/65, 9.2%) and CDH1 (7/65, 10.8%) mutations was both more than 5% in this cohort, guaranteeing that the proportion difference between subgroups was not caused by mutations randomly occurred. Lollipop plot visualized the entire mutation spots of AKT1 and CDH1 genes, including a range of mutation types (online supplemental figure 3A,B). Kaplan-Meier survival curves showed that patients with AKT1-mutant (AKT1-Mut) tumors obtained significantly adverse PFS (mPFS 2.4 months vs not reached (NR), HR (HR)=7.80, 95% CI 2.90 to 20.95, p<0.001) and OS (mOS 8.2 months vs NR, HR=6.21, 95% CI 1.89 to 20.44, p<0.001) compared with those with AKT1-wild-type (AKT1-WT) tumors (figure 1C, online supplemental figure 4A). Likewise, the patients with CDH1-Mut tumors exhibited significantly shorter PFS (mPFS 1.5 months vs NR, HR=5.37, 95% CI 2.10 to 13.76, p<0.001) than those with CDH1-WT tumors, but no significant difference for OS (mOS NR vs NR, HR=1.81, 95% CI 0.41 to 8.12, p=0.430) was observed between patients with CDH1-Mut and CDH1-WT (figure 1D, online supplemental figure 4B).

Identification of gene mutations associated with primary resistance to ICIs in dMMR/MSI-H GI cancer. (A) The univariate Cox proportional hazards regression model identifies particular gene mutations associated with PFS following ICIs. (B) The proportion of particular gene-Mut patients in ICI-sensitive and ICI-resistant patients. (C and D) Kaplan-Meier curves comparing PFS between the patients with or without AKT1 (C) or CDH1 mutations (D). dMMR, mismatch repair-deficient; GI, gastrointestinal; ICIs, immune-checkpoint inhibitors; MSI-H, microsatellite instability-high; Mut, mutant; PFS, progression-free survival; WT, wild-type.
Given the well-documented correlations of ICI efficacy with TMB, indel burden, CNA load, and MATH in multiple cancer types, including GI cancer,23–27 we also studied whether these associations exist in dMMR/MSI-H GI cancer. All variables, including TMB, clonal TMB, non-clonal TMB, indel burden, broad CNA score, focal CNA score, global CNA score, and MATH score, were individually subjected to univariate Cox proportional hazards analysis revealing that no parameters were significantly associated with PFS (online supplemental figure 5A). Additionally, there were no significant differences in the values of these parameters between ICI-resistant and ICI-sensitive patients with dMMR/MSI-H GI cancer (online supplemental figure 5B). These results suggested no association of ICI efficacy with TMB, indel burden, CNA load, and MATH in dMMR/MSI-H GI cancer.
Model construction and performance evaluation of IOpred
In the discovery cohort, there were six AKT1-Mut patients, seven CDH1-Mut patients, and one patient with AKT1 and CDH1 co-mutation. A multivariable exact logistic regression analysis demonstrated that AKT1 and CDH1 were independently correlated with primary resistance to ICIs (p=0.001 for AKT1 and p=0.006 for CDH1) (figure 2A). Meanwhile, a multivariable Cox regression analysis showed that AKT1 and CDH1 were independent predictors of PFS (figure 2B). Based on these findings, we combined AKT1 with CDH1 as an IOpred to identify the patients who could not benefit from ICIs. The patients with GI cancer with IOpred-Mut (mutant AKT1 or CDH1) tumors had significantly inferior PFS (mPFS 2.1 months vs NR, HR=8.36, 95% CI 3.58 to 19.55, p<0.001; GC: mPFS 1.4 vs 28.7 months, HR=13.01, 95% CI 2.39 to 70.89, p<0.001; and IC: mPFS 3.6 months vs NR, HR=6.33, 95% CI 2.23 to 17.94, p<0.001) and OS (mOS 16.9 months vs NR, HR=5.17, 95% CI 1.77 to 15.12, p<0.001; GC: mOS 5.6 months vs NR, HR=7.35, 95% CI 1.12 to 48.00, p=0.018; and IC: mOS 16.9 months vs NR, HR=3.62, 95% CI 0.90 to 14.58, p=0.053) as compared with those with IOpred-WT (wild-type for both AKT1 and CDH1) tumors regardless of IC or GC (figure 2C–E, online supplemental figure 6A–C).
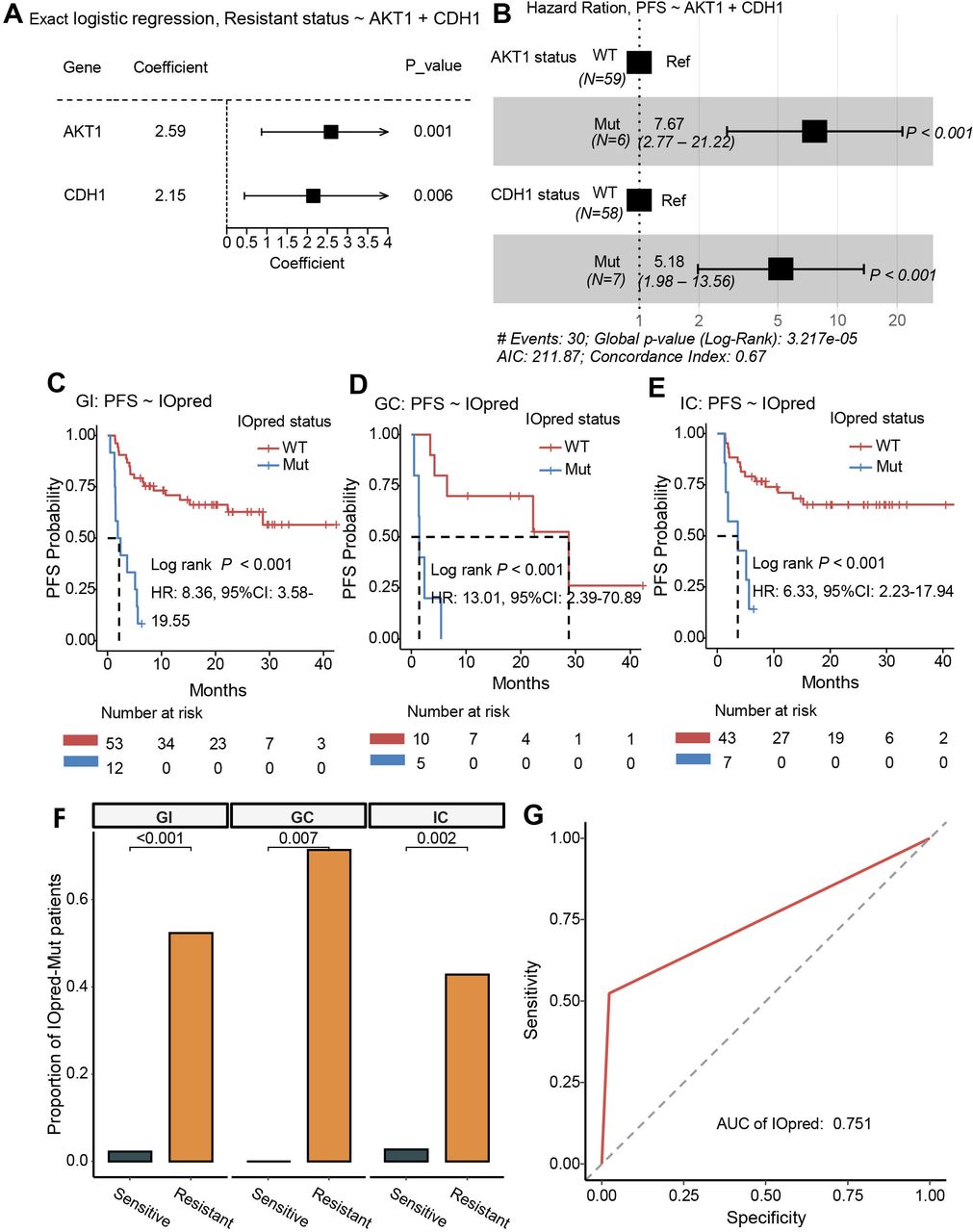
Model construction and performance evaluation of IOpred in dMMR/MSI-H GI cancer. (A) A multivariable exact logistic regression analysis shows that AKT1 and CDH1 are independently correlated with primary resistance to ICIs. (B) A multivariable Cox regression analysis demonstrates the independence of AKT1 and CDH1 for predicting PFS in patients with dMMR/MSI-H GI cancer receiving ICIs. AKT1 and CDH1 are integrated as an immuno-oncology therapy predictor (IOpred) to identify patients with dMMR/MSI-H GI cancer who could not benefit from ICIs. (C–E) Kaplan-Meier curves comparing PFS between IOpred-Mut and WT patients with dMMR/MSI-H GI cancer (C), GC (D), or IC cancer (E). (F) The proportion of IOpred-Mut patients in ICI-sensitive and ICI-resistant patients with dMMR/MSI-H GI cancer, GC or IC. (G) ROC curve and AUC calculation are adopted to evaluate the predictive accuracy of IOpred for primary resistance to ICIs in dMMR/MSI-H GI cancer. The AUC value is 0.751 (95% CI 0.639 to 0.862) with 98% of specificity and 52% of sensitivity for the GI cancer data set. AUC, area under the curve; dMMR, mismatch repair-deficient; GC, gastric cancer; GI, gastrointestinal; IC, intestinal cancer; ICIs, immune-checkpoint inhibitors; MSI-H, microsatellite instability-high; Mut, mutant; PFS, progression-free survival; ROC, receiver operating characteristic; WT, wild-type.
To further evaluate the predictive value of IOpred for immunotherapy efficacy, the univariate and multivariate Cox regression analyses were performed on IOpred and clinicopathological parameters and demonstrated that IOpred was an independent predictor of PFS in dMMR/MSI-H patients receiving ICIs (table 2). IOpred-mutation was highly enriched in the ICI-resistant subgroup compared with the ICI-sensitive subgroup across tumor types (p<0.001 in GI; p=0.007 in GC; and p=0.002 in IC) (figure 2F). Additionally, the ROC curve and the corresponding AUC were adopted to evaluate the accuracy of IOpred predictive of primary resistance to ICIs. AUC values were 0.751 (95% CI 0.64 to 0.86) with 98% (95% CI 0.88 to 1.00) of specificity and 52% (95% CI 0.32 to 0.72) of sensitivity for GI cancer, 0.857 (95% CI 0.68 to 1.00) with 100% (95% CI 0.66 to 1.00) of specificity and 71% (95% CI 0.36 to 0.92) of sensitivity for GC, and 0.7 (95% CI 0.56 to 0.84) with 97% (95% CI 0.86 to 1.00) of specificity and 43% (95% CI 0.21 to 0.67) of sensitivity for IC (figure 2G, online supplemental figure 6D,E). The positive predictive value (PPV) was 91.7% (11/12, 95% CI 0.65 to 0.99) for the overall data set, 100% (5/5, 95% CI 0.56 to 1.00) for the GC data set, and 85.7% (6/7, 95% CI 0.49 to 0.97) for the IC data set. Collectively, IOpred demonstrated a good performance at primary resistance prediction in the discovery cohort.
Univariate and multivariate Cox regression against PFS of clinical and genetic relevant variables in patients with dMMR/MSI-H GI cancer receiving ICIs
Furthermore, the prognostic values of single gene AKT1 or CDH1 and their combination IOpred were investigated in MSI-H TCGA-STAD (stomach adenocarcinoma) and TCGA-CRC cohort without experiences of ICI therapy. In this 152-case cohort, 30 patients were IOpred-Mut, including 18 CRC and 12 GC. Single AKT1 or CDH1 mutations and IOpred-Mut were associated with neither PFS nor OS in these cases (online supplemental figure 7). Taken together, AKT1, CDH1, and IOpred were not prognostic biomarkers but might function as predictive biomarkers, whose mutations were significantly associated with primary resistance to ICIs and poor PFS in dMMR/MSI-H GI cancer.
Validation of the predictive value of IOpred for primary resistance to ICIs
To validate the predictive value of IOpred for primary resistance to ICIs, we analyzed one independent ICI-treated cohort comprizing 22 cases with dMMR/MSI-H GI cancer with adequate data regarding survival and genomic alterations obtained from blood-based NGS. In this cohort, all cases were diagnosed with dMMR by IHC, wherein 15 of them were identified as MSI-H by tumor tissue PCR, and the remaining 7 patients had no available PCR data. The basic characteristics of patients were summarized in table 3. This cohort consisted of 5 IOpred-Mut cases and 17 IOpred-WT cases. The frequency of AKT1 and CDH1 mutations was 13.6% (3/22) and 9.1% (2/22), respectively. All mutations of AKT1 and CDH1 were displayed in lollipop plots (online supplemental figure 3C,D). The IOpred-Mut cases had significantly adverse PFS (mPFS 1.6 vs 21.7 months, HR=4.68, 95% CI 1.47 to 14.97, p=0.004) and OS (mOS 2.8 vs 20.0 months, HR=15.98, 95% CI 2.98 to 85.64, p<0.001) as compared with IOpred-WT cases (figure 3A,B). The univariate and multivariate Cox regression analyses were performed, revealing that IOpred-mutation was an independent predictor of a shorter PFS (HR=11.80, 95% CI 2.59 to 53.75, p<0.001) (figure 3C,D). Among 5 IOpred-Mut cases, 4 cases (80%) were ICI-resistant, while among 17 IOpred-WT cases, only 6 cases (35.3%) were ICI-resistant, yielding a PPV of 80% (4/5, 95% CI 0.38 to 0.96). The AUC value of the IOpred for primary resistance prediction was 0.658 (95% CI 0.48 to 0.84) with the specificity of 91.67% (95% CI 0.65 to 0.99) and sensitivity of 40% (95% CI 0.17 to 0.69) in the validation cohort. Collectively, these results validated that IOpred was a convenient and powerful predictor of primary resistance to ICIs.
Basic characteristics of the patients with dMMR/MSI-H GI cancer in the validation cohort
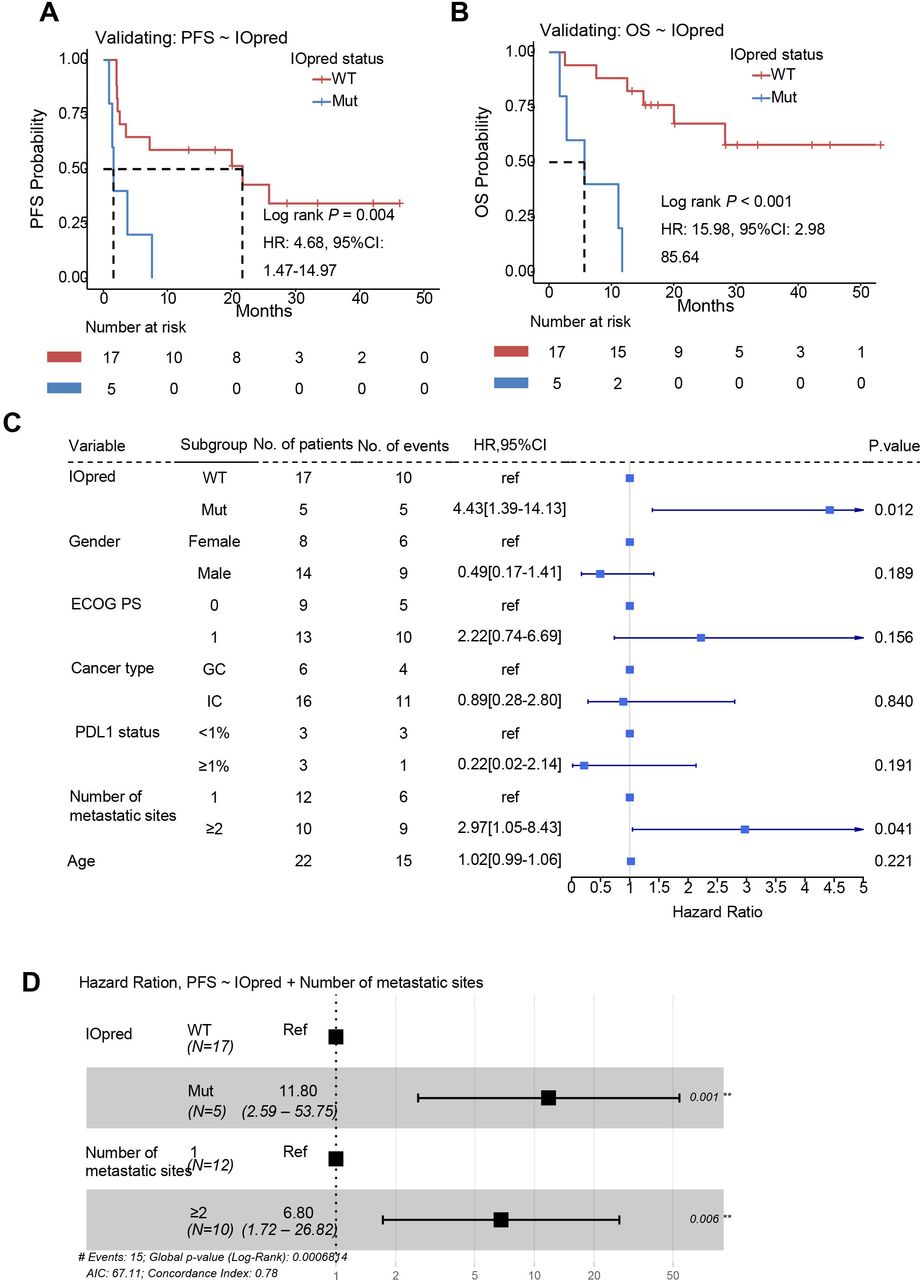
Validation of the predictive value of IOpred for primary resistance to ICIs in dMMR/MSI-H GI cancer. (A and B) Kaplan-Meier curves comparing PFS (A) and OS (B) between IOpred-Mut and WT patients in the validation cohort consisting of 22 patients with dMMR/MSI-H GI cancer treated with ICIs. (C and D) The univariate and multivariate Cox regression analyses reveal that IOpred-mutation is an independent predictor of a shorter PFS. dMMR, mismatch repair-deficient; ECOG PS, Eastern Cooperative Oncology Group Performance Status; GC, gastric cancer; GI, gastrointestinal; IC, intestinal cancer; ICIs, immune-checkpoint inhibitors; IOpred, immuno-oncology therapy predictor; MSI-H, microsatellite instability-high; Mut, mutant; OS, overall survival; PD-L1, programmed death-ligand 1; PFS, progression-free survival; WT, wild-type.
The predictive value of TMB in patients with IOpred-WT GI cancer
It was obvious from the above results that the specificity of IOpred is very high, but its sensitivity is moderate. There are still approximately 20% of IOpred-WT patients (18.9% for the discovery cohort and 35.3% for the validation cohort) with primary resistance to ICI. To recognize more ICI-resistant patients, we performed biomarker analyses in IOpred-WT patients as an exploratory. We tested the differences in gene mutation, CNA score, MATH score, TMB, and indel burden between ICI-resistant and ICI-sensitive patients. TMB level was lower in ICI-resistant patients than in ICI-sensitive patients with a trend close to significance (median TMB 20.8 vs 29.3 mutations/Mb, p=0.051) (figure 4A), while no significant difference was found in the rest parameters (online supplemental figure 8). The optimal cut-off value of TMB for the discrimination between ICI-resistant and ICI-sensitive patients was determined at 26.19 mutations/Mb using an ROC curve, with an AUC value of 0.701 (figure 4B). When the IOpred-WT patients were stratified by this cut-off point, TMB-low (TMB-L, TMB ≤26.19 mutations/Mb) patients had a significantly higher primary resistance rate of 34.8% (8/23) than TMB-high (TMB-H, TMB >26.19 mutations/Mb) patients with a primary resistance rate of 6.7% (2/30) (p=0.014, figure 4C). Survival analysis showed that TMB-L patients had significantly poorer PFS (mPFS 15.2 months vs NR, HR=3.46, 95% CI 1.31 to 9.12, p=0.008, figure 4D) and OS (mOS NR vs NR, HR=4.42, 95% CI 0.89 to 21.91, p=0.047, online supplemental figure 9A) than TMB-H patients. After adjustment by cancer type, TMB remained a significant predictive factor of primary resistance to ICIs (p=0.015) and PFS (p=0.015) in patients with IOpred-WT GI cancer receiving ICI (online supplemental figure 9B,C). Therefore, through adopting the two-step classification strategy, patients could be stratified into three subgroups: IOpred-Mut, IOpred-WT +TMB-L, and IOpred-WT +TMB-H. The IOpred-Mut subgroup presented the strongest primary resistance to ICI, followed by the IOpred-WT +TMB-L subgroup and the IOpred-WT +TMB-H subgroup (91.7% vs 34.8% vs 6.7%, p<0.001) (figure 4E). Accordingly, the IOpred-Mut subgroup was associated with the worst prognosis for both PFS and OS, the IOpred-WT +TMB-L subgroup with moderate prognosis, and the IOpred-WT +TMB-H subgroup with the best prognosis (mPFS: 2.1 months vs 15.2 months vs NR, p<0.001; mOS: 16.9 months vs NR vs NR, p=0.001) (online supplemental figure 10).

The predictive value of TMB in dMMR/MSI-H GI cancer with IOpred-WT. (A) TMB level of ICI-sensitive and ICI-resistant patients in dMMR/MSI-H GI cancer with IOpred-WT. (B) The optimal cut-off value of TMB is determined at 26.19 mutations/Mb using the ROC curves, with an AUC of 0.701. (C) The percentage of ICI-resistant patients in TMB-H and TMB-L patients. (D) Kaplan-Meier curves comparing PFS between TMB-H and TMB-L patients. (E) Through a step-by-step filtering using IOpred and TMB, patients with dMMR/MSI-H GI cancer are stratified into three subgroups, IOpred-Mut, IOpred-WT+TMB-L, and IOpred-WT+TMB-H, with significantly different rates of primary resistance to ICIs. AUC, area under the curve; dMMR, mismatch repair-deficient; GI, gastrointestinal; ICIs, immune-checkpoint inhibitors; IOpred, immuno-oncology therapy predictor; MSI-H, microsatellite instability-high; Mb, megabase; Mut, mutant; PFS, progression-free survival; ROC, receiver operating characteristic; TMB, tumor mutational burden; TMB-H, high tumor mutational burden; TMB-L, low tumor mutational burden; WT, wild-type.
Correlations between AKT1/CDH1 mutations and immunosuppressive tumor environment
Next, we further explored the tumor microenvironment difference between ICI-resistant and ICI-sensitive patients and whether the IOpred-Mut status was associated with immune cell infiltration in the tumor. The density of multiple lymphocyte subgroups in the tumor was determined using mIF. Only the density of CD56bright natural killer (NK) cells was significantly higher in the ICI-resistant subgroup than in the ICI-sensitive subgroup (median 6 vs 1 cell/mm2, p=0.047) (figure 5A). Other lymphocyte subgroups, including CD3+ (T-cells), CD4+ (T-helper-cells), CD8+ (cytotoxic T-cells), CD20+ (B-cells), CD68+ (macrophages), CD68+/CD163− (M1 macrophages), CD68+/CD163+ (M2 macrophage), CD56dim NK cells, and tertiary lymphoid structure were not significantly differed between two subgroups (online supplemental figure 11A). Likewise, AKT1-Mut tumors were more infiltrated by CD56bright NK cells than AKT1-WT tumors (median 9 vs 2 cells/mm2, p=0.023) (figure 5B). In addition, compared with AKT1-WT tumors, the M1/M2 ratio of tumor-associated macrophages was significantly decreased in AKT1-Mut tumors (median ratio 23.50 vs 3.29, p=0.021) (figure 5C, online supplemental figure 11B). CDH1 mutation elicited a numerically high density of CD56bright NK cells compared with wild-type CDH1, although the difference was insignificant (median 5.5 vs 2.5 cells/mm2, p=0.190) (online supplemental figure 11C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlations between AKT1/CDH1 mutations and immunosuppressive tumor environment. (A) Multiplex immunofluorescence staining shows the density of CD56bright NK cells in pre-ICI tissues from ICI-resistant and ICI-sensitive patients with dMMR/MSI-H GI cancer. (B and C) Multiplex immunofluorescence staining shows the density of CD56bright NK cells (B) and M1/M2 ratio of tumor-associated macrophages (C) in pre-ICI tissues from AKT1-Mut and WT patients with dMMR/MSI-H GI cancer. dMMR, mismatch repair-deficient; GI, gastrointestinal; ICIs, immune-checkpoint inhibitors; MSI-H, microsatellite instability-high; Mut, mutant; NK, natural killer; WT, wild-type.
Discussion
In the present study, we analyzed multiple parameters that may be related to clinical benefits from ICIs through panel-based NGS and finally found that only AKT1 and CDH1 mutations were significantly associated with ICI efficacy. On this basis, we developed a genomic classifier, IOpred, consisting of AKT1 and CDH1, which could independently predict PFS and primary resistance to ICIs, and recognize 52.4% of patients with dMMR/MSI-H GI cancer with primary resistance to ICIs with a PPV of 91.7%. As the biomarker developed from dMMR/MSI-H GI cancer cohort with the largest sample size to date, IOpred’s predictive value for ICI efficacy was also validated in an independent cohort. These results suggested that IOpred is a promising biomarker of ICI efficacy in dMMR/MSI-H GI cancer and can be easily translated into an easy-to-use clinical assay due to only detection of two decisive common genes.
Since dMMR/MSI-H misdiagnosis may partly account for primary resistance to ICIs among patients with metastatic CRC,11 we only included the samples with IHC-dMMR or PCR-MSI-H and NGS-MSI-H in the discovery cohort. The clinical activity with an ORR of 46.7% (7/15) for GC and an ORR of 56% (28/50) for IC in our 65-case cohort was comparable or superior to previously published MSI-H GI data.6 8 28–31 In addition, there were four patients with GI cancer with dMMR by IHC, but microsatellite stable (MSS) by both PCR and NGS, who were not included in the discovery cohort. All four patients experienced PD at the first tumor assessment, with comparable PFS and OS with MSS patients. These findings were in accordance with those of the previous studies showing that the misdiagnosis of dMMR/MSI-H status is one leading cause of the resistance to ICIs in mCRC shown as dMMR/MSI-H.11 Therefore, excluding misdiagnosed dMMR/MSI-H patients via the strict criteria is the premise of identifying the real biomarkers predictive of resistance to ICIs in dMMR/MSI-H patients.
After ruling out the interference of misdiagnosis, AKT1 and CDH1 mutations were identified to be both independent predictors of PFS and primary resistance in patients with dMMR/MSI-H GI cancer through a sequential two-step screening method. AKT1 is the most commonly mutated AKT isoform in most solid tumors. As a central nod of possibly the most frequently activated pathways of cell survival and proliferation in cancer, AKT1 aberrant activation elicits the pathogenesis of cancer. Interestingly, mounting evidence suggests that AKT plays a pivotal role in regulating immune cell development, including T cells, B cells, dendritic cells, and macrophages, whose mutations inhibit tumor immune surveillance and antitumor immune-intrinsic properties by the creation of immunosuppressive conditions and escaping of immune recognition.32–37 Consistently, immunosuppressive tumor microenvironments with a low M1/M2 ratio were observed in dMMR/MSI-H GI tumors with AKT1 mutations. Of note, AKT1-Mut tumors also had a significantly higher density of CD56bright NK cells compared with AKT1-WT tumors. Likewise, ICI-resistant tumors were more infiltrated by CD56bright NK cells than ICI-sensitive tumors. CD56bright cells are a kind of immature, poorly cytotoxic but cytokine-producing NK cells. Existing evidence suggests that the role of CD56bright cells in the antitumor immune response is controversial, which might be due to different cancer types and tumor staging.38–40 Our results supported the notion that CD56bright cells play a negative regulatory role in antitumor immune response in dMMR/MSI-H GI cancer, in line with a recently published clinical study in melanoma.40 Whether a high density of CD56bright NK cells at baseline predicts the poor efficacy of ICIs in dMMR/MSI-H GI cancer and its underlying mechanisms warrant further exploration.
CDH1 is a well-known tumor suppressor gene encoding E-cadherin, a marker of differentiated epithelia, and loss of function mutations in CDH1 correlate with increased invasiveness and metastasis of tumors.41 Using RNA-sequencing data, Hugo et al42 reported that innate anti-PD-1 resistance melanomas display a transcriptional signature, including CDH1, and non-responder tumors express less CDH1 than responder tumors. Moreover, in a phase II trial of pembrolizumab in patients with advanced MSI-H GC conducted by Kwon et al4 5 out of 19 patients have CDH1 mutations, and all do not respond to PD-1 blockade. In line with these findings, we identified CDH1 mutations as an independent predictor of primary resistance to ICIs. The mechanism of CDH1 mutations related to primary resistance to ICIs might differ from that of AKT1 mutations, which is worthy of further study.
Given that AKT1 and CDH1 were both independent predictors of ICI therapy, we went on to combine AKT1 with CDH1 as a genomic classifier, IOpred. IOpred demonstrated a good performance at primary resistance prediction with a high PPV. In the discovery cohort, 11 (91.7%) of 12 IOpred-Mut patients were ICI-resistant, and 4 (80%) of five IOpred-Mut patients in the validation cohort were ICI-resistant. In addition, IOpred could be detected by NGS testing of plasma circulating tumor DNA (ctDNA), a technique providing mutational data with high credibility and validity. The use of ctDNA-based NGS testing will greatly expand the applicability of IOpred from the patients with available tumor tissues to the patients with advanced diseases where tissue procurement can be extremely challenging. Thus IOpred might widely guide clinical decision-making that the dMMR/MSI-H patients with IOpred-mutation should not be recommended for ICI therapy and may require more aggressive clinical management and a better understanding of underlying pathogenesis.
In fact, preclinical data have suggested that AKT inhibitors could work synergistically with immunotherapies and targeted therapies.43–45 Several pan-AKT inhibitors have already been developed and are in ongoing clinical trials for different malignant tumors combined with immunotherapies and targeted therapies, including GC (NCT02240212).46 Interestingly, Bougen-Zhukov et al47 observed that mouse-derived gastric organoids lacking CDH1 were sensitive to the apoptotic effects of AKT1 E17K inhibitor, miransertib. These findings suggest that despite the poor benefit from ICIs in IOpred-Mut patients, the combination of AKT inhibitors and immunotherapies might be a feasible choice in this subgroup, particularly in AKT1-Mut dMMR/MSI-H GI cancer.
However, there were still half of ICI-resistant patients belonging to the IOpred-WT subgroup. We thus tried to further stratify IOpred-WT patients for identification of ICI-resistant patients. About 34.8% (8/23) of TMB-L patients showed primary resistance to ICIs, while only 6.7% (2/30) of TMB-H patients exhibited primary resistance to ICIs. Thus when IOpred-WT patients received ICI therapy, the TMB-L patients should be closely followed up and paid much attention to the resistance to ICIs. Collectively, the classification established through a step-by-step filtering using IOpred and TMB could readily be applied to clinical care and contribute to dMMR/MSI-H GI cancer management as treatment and follow-up strategies can be chosen based on the specific IOpred and TMB status, respectively.
There are several limitations to the current study. On the one hand, this was a retrospective study, and the underlying mechanism of the prediction role of IOpred in dMMR/MSI-H GI cancer population is not explored deeply. Future investigations based on in vitro and in vivo experiments and prospective trials with larger sample sizes are warranted to assess the predictive value of IOpred and dig deep into its mechanisms. On the other hand, due to the lack of consensus regarding the TMB cut-off point, the cut-off value of TMB used in our study was determined by ROC, which warrants further validation in a larger cohort.
Conclusions
In conclusion, we developed and validated IOpred that could effectively predict primary resistance to ICIs in dMMR/MSI-H GI cancer. This classifier provides a cost-effective and feasible approach to identify patients who could not benefit from ICIs that can hopefully be further validated in a prospective trial.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the ethics committee of Peking University Cancer Hospital (approval ID: 2021YJZ34), and was conducted in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
The authors would like to acknowledge the technical support provided by Zhonghu He from Peking University Cancer Hospital & Institute and Hao Chen from 3D Medicines. Additionally, we would like to thank Yao Jiang and Jingjie Bian, the employees of 3D Medicines, for assistance with sample collection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
ZW, QZ and CQ contributed equally.
Contributors ZW, QZ, and CQ contributed equally to this study as co-first authors. LS and JL have full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. LS, JL, ZW, QZ, CQ, YB, FZ, HC, SC, and XZhao participated in the design and performance of the study. All authors participated in the data acquisition, analysis, and interpretation. The manuscript was drafted by JC, ZW, QZ, CQ, HC, and FZ, and reviewed by all authors. All authors read and approved the final manuscript.
Funding This study was supported by Beijing Municipal Natural Science Foundation (No. 7224323) and the Major Research Program of National Natural Science Foundation of China (No. 91959130).
Competing interests FZ, HC, JC, SC, and XZhao are employees of 3D Medicines. No other disclosures are reported.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.