Article Text

Abstract
Background Amplivant is a molecularly optimized Toll-like receptor 2 ligand that can be covalently conjugated to tumor peptide antigens. In preclinical models, amplivant-adjuvanted synthetic long peptides (SLPs) strongly enhanced antigen presentation by dendritic cells, T cell priming and induction of effective antitumor responses. The current study is a first-in-human trial to investigate safety and immunogenicity of amplivant conjugated to human papillomavirus (HPV) 16-SLP.
Methods A dose escalation phase I vaccination trial was performed in 25 patients treated for HPV16 positive (pre-)malignant lesions. Amplivant was conjugated to two SLPs derived from the two most immunodominant regions of the HPV16 E6 oncoprotein. The vaccine, containing a mix of these two conjugates in watery solution without any other formulation, was injected intradermally three times with a 3-week interval in four dose groups (1, 5, 20 or 50 µg per conjugated peptide). Safety data were collected during the study. Peptide-specific T cell immune responses were determined in blood samples taken before, during and after vaccination using complementary immunological assays.
Results Toxicity after three amplivant-conjugated HPV16-SLP vaccinations was limited to grade 1 or 2, observed as predominantly mild skin inflammation at the vaccination site and sometimes mild flu-like symptoms. Adverse events varied from none in the lowest dose group to mild/moderate vaccine-related inflammation in all patients and flu-like symptoms in three out of seven patients in the highest dose group, after at least one injection. In the lowest dose group, vaccine-induced T cell responses were observed in the blood of three out of six vaccinated persons. In the highest dose group, all patients displayed a strong HPV16-specific T cell response after vaccination. These HPV16-specific T cell responses lasted until the end of the trial.
Conclusions Amplivant-conjugated SLPs can safely be used as an intradermal therapeutic vaccine to induce robust HPV16-specific T cell immunity in patients previously treated for HPV16 positive (pre-) malignancies. Increased vaccine dose was associated with a higher number of mild adverse events and with stronger systemic T cell immunity.
Trial registration numbers NCT02821494 and 2014-000658-12.
- Immunotherapy
- Immunogenicity, Vaccine
- Adjuvants, Immunologic
- Vaccination
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Cancer vaccines are a promising strategy for cancer immunotherapy. They allow reinforcing of tumor-specific T cell responses against predefined tumor antigens.1 Synthetic long peptides (SLPs) based cancer vaccines are safe, able to induce functional tumor-specific T cells, and show clinical efficacy.2–6 Their use requires a combination with immune stimulating agents, as they possess no intrinsic adjuvant.7 Our preclinical studies revealed that chemically well-defined adjuvants like Toll-like receptor (TLR) ligands can be used to improve synthetic peptide based cancer vaccines,8 comparable with modern self-adjuvanting RNA and DNA vaccines.7 These synthetic compounds can be covalently attached to antigenic peptide sequences in a Good Manufacturing Practices (GMP) compliant manner allowing self-adjuvanting of synthetic peptide-based vaccines.
Amplivant is an optimized, synthetic TLR2 ligand that can be conjugated to SLP using defined chemistry.9 10 It is chemically adapted to optimally interact with the binding domain of the TLR2/TLR1 heterodimer receptor to induce improved immunological activity.9 Molecularly defined, self-adjuvanting peptide vaccines have the potency to cause local innate immune activation, antigen-targeting to dendritic cells (DCs) and DC activation, together leading to efficient T cell activation.11 12
To test the potency of amplivant-conjugated SLP vaccines, we made use of SLP derived from the human papilloma virus type 16 (HPV16) E6 oncoprotein amino acid (aa) sequence. Studies in patients with HPV16-associated tumors have revealed that spontaneous HPV16-specific T cell responses occur but are weak and fail to sufficiently control tumor outgrowth.13 The constitutively expressed HPV16 oncoprotein E6 is an excellent target for immunotherapeutic vaccine strategies and has been shown to improve effective HPV16-specific antitumor T cell activity.2 4 14–16 In addition, the quantity and quality of human T cell responses, of both HPV16-specific CD4+ and CD8+ T cells derived from patient’s blood and lymph nodes could be markedly enhanced by ex vivo stimulation with amplivant-conjugated SLPs.10 17 In preclinical murine studies, skin vaccination with amplivant-conjugated SLP showed significantly enhanced bioactivity compared with unconjugated SLP, in terms of the induced tumor-specific T cell responses and tumor growth control.10
The present study describes the results from the first in human phase I trial to establish safety and T cell immunogenicity of amplivant conjugated to HPV16 E6-SLP. The amplivant-conjugated HPV16 SLP vaccine was administered via the intradermal route. This mode of delivery takes advantage of the direct loading potency of skin-resident DCs with vaccine antigen as we have studied in human skin explants.17
The two most immunodominant SLP from the 13 overlapping long peptide HPV16-SLP vaccine containing both T helper (Th) and cytotoxic T lymphocyte epitopes were identified based on responses of previously vaccinated patients.3 17 These two SLP were both conjugated to amplivant under GMP synthesis conditions. This self-adjuvanted vaccine was injected three times intradermally in four dose cohorts of patients previously treated for a HPV16 positive (pre-) malignant lesion. Here, we report that our TLR ligand conjugated vaccine is safe and results in a dose-dependent detection of vaccine-specific T cell responses.
Material and methods
Study design and participants
This phase I dose escalation study was designed to determine the safety and immunogenicity of amplivant conjugated SLP vaccine in humans. The protocol was first approved to enroll only oropharyngeal squamous cell carcinoma (OPSCC) patients after treatment with curative intent. Because of slow accrual, the protocol was amended in May 2016 to include persons with an HPV16 positive (pre-)malignant lesion following standard treatment. From July 2015 to March 2020, 25 patients were enrolled. Patients were eligible for inclusion if they were at least 18 years of age, had previously documented evidence of an HPV16 positive (pre-)malignant lesion following standard curative treatment and were without residual disease based on physical examination between 4 and 16 weeks after therapy. Other inclusion criteria included that patients of childbearing potential should test negative using a serum pregnancy test and agree to use effective contraception during the entire treatment and follow-up period of the study, and patients were required to have a WHO performance score of 0–1. Additionally, the following laboratory results were required: an adequate bone marrow function as indicated by absolute neutrophil count >1.5 × 109/L, platelet count >100 × 109/L or hemoglobin >6 mmol/L; serum liver function (bilirubin ≤2 × upper limit of normal range, alanine transaminase (ALT) and/or aspartate transaminase (AST) ≤2.5 × UNL, alkaline phosphatase ≤2.5 × UNL) and renal function (calculated creatinine clearance ≥40 mL/min/1.73 m2). Patients were excluded from the study in the following cases: (1) a history of an autoimmune disease or other systemic intercurrent disease that might affect the immunocompetence of the patient, (2) receiving immunosuppressive therapy, except for topical application, (3) a history of a second malignancy except curatively treated low-stage tumors with a histology that can be differentiated from the current tumor or pre-malignant lesion, (4) receipt of another investigational product within the previous 4 weeks or at any time during the study period and (5) receipt of prior HPV directed immunotherapy, (6) HIV or chronic hepatitis B or C infection and (7) any condition that in the opinion of the investigator could interfere with the conduct of the study. The study was registered at clinicaltrials.gov and EudraCT.
Study treatment and schedule
The vaccine employed in this study consists of two HPV16 E6 SLP sequences (E6 71–95 and E6 127–158, indicated as peptide A and B, respectively), both of which were included in the previously reported thirteen HPV16 SLP vaccine3 and were conjugated to the TLR ligand amplivant. T cell responses against these two E6 peptides were found in 40%–60% of individuals, using T cells derived from these previously vaccinated patients or healthy donors who were not selected for HLA type.17 From the Immune Epitope Database (IEDB) and SYFPEITHI databases, it was predicted that 50%–75% of individuals would have HLA class I-binding and class II-binding epitopes for these two E6 peptides.17 These findings suggest that at least 50% of the injected patients with a mixture of these two antigens is likely to respond to amplivant-conjugated SLP vaccination with an HPV16-directed T cell response. The amplivant conjugated SLPs were manufactured and tested for clinical use at the GMP facility of the Department of Clinical Pharmacy and Toxicology at the Leiden University Medical Center, Leiden, The Netherlands.
At the day of injection, the vaccine was reconstituted in DMSO/water for injections 20/80 v/v in a total volume of 0.10 mL. Patients were vaccinated intradermally at alternating sites of the thigh or upper arm at a dose of 1 µg per conjugated peptide (first group), 5 µg per peptide (second group), 20 µg per peptide (third group) or 50 µg per peptide (fourth group). Each dose group contained six patients. The trial included 2 weeks of screening, 6 weeks of vaccination treatment and follow-up visits during 20 weeks after the last dose of the vaccine (figure 1). Patients were vaccinated three times with an interval of 3 weeks. Vaccination started with the intradermal injection of the lowest dose. The decision to start enrollment at the next dose level was made by the principal investigator after assessing the safety after four out of six patients at the previous dose level had completed the first follow-up visit after the third vaccination. The safety data were reviewed and commented by an Independent Data Monitoring Committee at each dose of the vaccine before dose escalation was allowed.
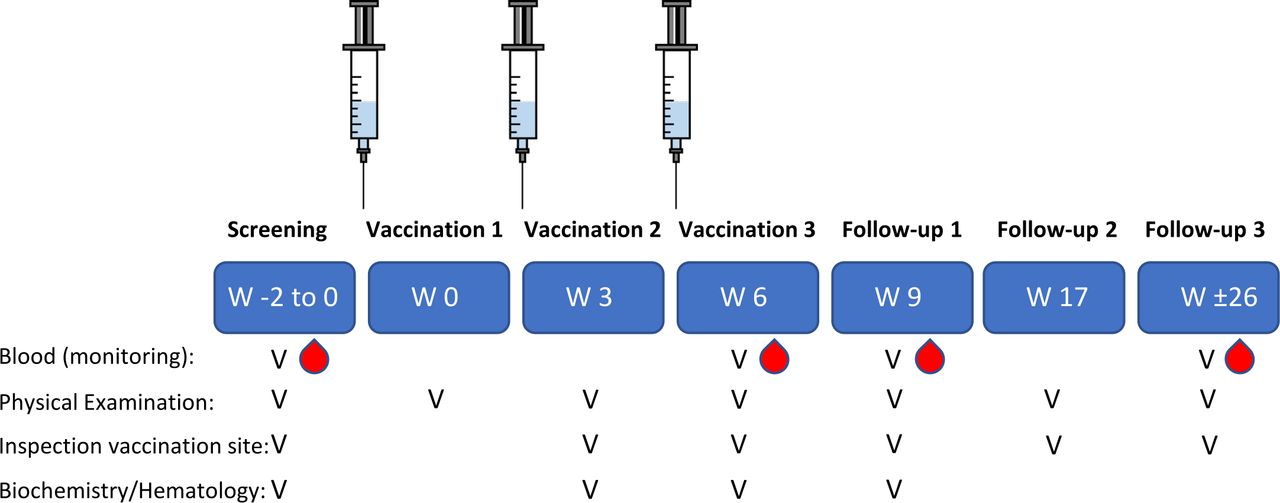
A schematic overview of the vaccination scheme. Individuals received the vaccine injections within a dose escalation of 1, 5, 20 or 50 µg/peptide – conjugate in patients with HPV16+ tumors or premalignant lesions at weeks 0, 3 and 6. Before, after two injections, three and 20 weeks after last injection, blood was drawn for immunomonitoring. Safety was assessed throughout the whole trial using the CTCAE. CTCAE, Common Terminology Criteria for Adverse Events; HPV, human papillomavirus.
Study objectives
The primary endpoint was to determine the biological activity of the amplivant-conjugated SLP vaccine by demonstrating its capacity to induce HPV16 E6-specific T cell immunity. Blood was drawn at screening, week 6, 9 and 26 (figure 1) to determine the induction of HPV16-specific T cells following treatment using an array of immunologic assays as described further (see: immunomonitoring). The secondary endpoint was to study safety of the vaccine. To assess the safety, the incidence and severity of all adverse events (AEs), vital parameters and changes in blood chemistry and hematology parameters were determined. Toxicity was measured using the Common Terminology Criteria for Adverse Events (CTCAE) V.4.0.18 Relationship to treatment was evaluated for all AEs. At each visit, patients were assessed by physical examination, vital signs, toxicity and complete blood count with differential and serum biochemistry.
Immunomonitoring
Immunomonitoring of patient samples was performed in the Laboratory of Medical Oncology at the LUMC, using standard operating procedures for all tests with predefined definitions of positive immune responses and by trained personnel.3 19 Peripheral blood mononuclear cells (PBMCs) were isolated from venous blood samples (72 mL) collected in sodium heparin blood collection tubes within 6 hours using Ficoll gradient centrifugation. Freshly isolated PBMCs were directly applied for the lymphocyte stimulation test (LST), using autologous serum obtained from a cloth activator blood tube (8 mL) as described earlier.4 19 20 In the LST, the PBMCs were stimulated in eightfold wells with four HPV16 E6 and two E7 peptide pools as described earlier (each pool consisting of four peptides of 22 aa long with 14 aa overlap; 10 µg/mL per peptide) covering the entire viral E6 and E7 oncoproteins.3 4 19 20 A positive proliferative response was defined as a stimulation index (SI) of at least three under the condition that six out of eight wells displayed values above the cut-off, of which the latter is the mean value of cells in medium only (negative control) plus three times the SD. Cytokine analysis (IFNγ, TNFα, IL10, IL5, IL4, IL2) in the LST supernatants obtained at day 6 was done by flow cytometric based cytometric bead array (CBA; human Th1/Th2 kit, BD Biosciences) according to the manufacturer’s instructions. Acquisition was done at the BD LSR Fortessa (BD Biosciences, Flow Cytometer Core Facility at LUMC) equipped with FCAP Array Software (BD Biosciences) following the staining. The detection limit was 20 µg/mL for each cytokine. A threefold increase over the baseline sample was defined as a vaccine-induced change. The remaining PBMCs were cryopreserved in Iscove’s Modified Dulbecco’s Medium (mLonza, Verviers, Belgium) with 10% human albumin (Albuman, Sanquin) and 10% DMSO (WAK chemie medical) and stored at the vapor phase of liquid nitrogen until use. In the validated 4-day IFNγ ELISpot assay,3 thawed PBMCs of all time points for all patients were screened for specificity against the SLP as used in the Amplivant-conjugated SLP vaccine. Cells in medium only and stimulated with memory response mixture (consisting of the common microbial recall antigens tetanus toxoid, PPD tuberculin and Candida albicans) served as negative and positive control, respectively. A positive response was defined as at least 10 spots per 1×105 PBMCs. For a selected number of patients, an intracellular cytokine staining (ICS) was performed measuring the T cell types (CD3, CD4, CD8), cytokines (IL-2, TNFα, IFNγ, IL-5, GM-CSF) and T cell activation markers (CD154, CD137). First, the PBMCs were stimulated once with peptides and cytokines and cultured for 10 days and for readout restimulated with peptide loaded autologous monocytes as described previously.3 4 20 As negative control cells in medium only were used, and staphylococcal enterotoxin B (Sigma, 2 µg/mL) stimulation as positive control. A positive ICS response was defined as at least twice the frequency of HPV-specific T cells observed in peptide stimulated wells over negative control wells and minimally 10 events in the gate. A vaccine-induced response was defined as at least a threefold increase in specific T cell frequency, both in ELISpot and ICS assay, compared with baseline sample.
Statistical analysis
To obtain one value of T cell response per patient, the median of the highest specific spot counts of the two SLPs in the ELISpot for each postvaccination blood sample was calculated (median of max; MoM).3 Differences in dose groups were determined by Mann-Whitney test, and a two-way analysis of variance test was performed to determine the differences between the cohorts using GraphPad Prism 8 (GraphPad Software, San Diego, California, USA), and a p value ≤0.05 was considered as statistically significant.
Results
Patient characteristics
Patient characteristics of 25 individuals enrolled between June 2015 and January 2020 are depicted in table 1. Patients received three injections of the amplivant-conjugated SLP vaccine with a 3-week interval and were followed for up to 26 weeks (figure 1). One patient (#23) refused the third vaccination out of fear for COVID-19, standard-of-care follow-up was performed for her. She was replaced by another person (#25). Sixteen patients with an HPV16 positive malignancy (12 × OPSCC; 3 × anal squamous cell carcinoma and 1 × cervical cancer were enrolled after treatment with curative intent of which 11 patients were male. Of these, only one person (#21) was diagnosed with a recurrence after vaccination and eventually died of it (table 1). Nine patients were treated for an HPV16-associated premalignant lesion either of the cervix, vagina or vulva. Two patients showed no clinical response as the lesion persisted during vaccination. In three of these nine patients, a recurrence of a premalignant lesion was found, and in four of nine patients, no atypical cells were found at latest clinical follow-up (table 1).
Patient characteristics and adverse events
Acceptable vaccination-related adverse events
Patients experienced a mild local burning sensation during injection and immediately afterwards a small weal at the injection site appeared. No skin toxicity was found directly after vaccination. Toxicity after three amplivant-conjugated HPV16-SLP vaccinations was limited to CTCAE grade 1 or 2 (table 1). Mild/moderate vaccine-related inflammation at the vaccination site after injection was not seen in the lowest dose group (1 µg/conjugated peptide), in three out of six patients in the second dose group (5 µg/conjugated peptide), in five of six patients in the third dose group (20 µg/conjugated peptide) and in all patients in the highest dose group (50 µg/conjugated peptide). These reactions appeared the first day after injection and generally disappeared within 48 hours. Flu-like symptoms were noticed in three patients in the highest dose group after at least one injection, while only once flu-like symptoms occurred in the other dose groups. These AEs generally resolved within 1 day.
Dose-dependent vaccine-specific T cell immune responses
In the LST, using freshly isolated PBMC of the different time points stimulated with a total of six peptides pools for HPV16 E6 and E7, the number of patients responding with proliferation increased at higher vaccine dose levels (figure 2A,B). The peptide pools E6.2 and E6.4 used to read-out T cell reactivity were expected to elicit specific proliferative LST responses as they contained the two vaccine peptides (peptide A: HPV16 E671-95 and peptide B: HPV16 E6127-158). The responses to peptides covering the whole HPV16 E6 and E7 were determined to check for spontaneous responses as this would include more peptide pools to be positive or for possible bystander responses in the other sequence areas of the oncoproteins that were not included in the vaccine (online supplemental table 1). Notably, in the LST the cells were stimulated only once during 7 days, and in general, no responses were detectable against the two control (E7) peptide pools, which indicates that this stimulation method is not inducing T cell responses. When the percentage of positive responses was calculated per dose level and time point of blood sample, a trend of a better T cell response on higher vaccine dose level was observed (figure 2C, online supplemental figure 1). Calculation of MoM response in the postvaccination time points for all patients per cohort revealed a significant difference (p=0.022) between the highest vaccine dose compared with the lowest one (figure 1D). Cytokine production in the pooled supernatants of eight replicate wells was analyzed by a CBA, showing only in the higher vaccine dose level patient cytokine concentrations exceeding the threshold (figure 2A,E; online supplemental table 2). Next to the proliferative response, stimulation with peptide pools E6.2 and E6.4 showed measurable cytokine concentrations in the higher dose level groups on treatment. Notably, in some patients, peptide pool E6.3 was also positive in the proliferation and/or cytokine production assay, which can be explained by 11 aa overlap of the E6 sequences from peptide A in this read-out peptide pool. In the 20 µg/conjugated peptide dose level, the cytokine production to the E6 peptide pools was more restricted to IL-5 production, while four out of seven patients in the highest dose level (50 µg/conjugated peptide) showed a combined IFNγ, IL-5 and often (although low) IL-10 response to one or more peptide pools, so a mixed type 1 and 2 cytokine response. Herein, in approximately half of the cytokine responses per time point the response consisted of only IL-5 production, while the other half showed the combination IFNγ and IL-5, in which either IFNγ (#23 and #24) or IL-5 (#19 and #25) concentration exceeded the other (online supplemental figure 1, online supplemental table 2).
Supplemental material
Supplemental material

Proliferative and cytokine response rate increases with dose of conjugated peptide vaccine. (A) An example (patient #25) of proliferative response indicated by stimulation index (SI) in the left graph as determined by LST of fresh PBMC. In the middle and right graph the IFNγ and IL-5 production, respectively, as measured by CBA in the LST of the same patient. Peptide pool E6.2 and E6.4 (and to a lesser extent E6.3) contain the conjugated peptides as present in the vaccine. The time points of tested PBMC samples were baseline, week 6 (postvaccination 2), week 9 (postvaccination 3) and week 26 (follow-up). The cut-off in the left graph indicates the counts per minutes in negative control (cells in medium only) plus 3 × SD SI above this cut-off are considered a positive response. In the middle and right graph, the cut-off indicates the threshold of the CBA. (B) A summary of the responses for all patients is presented in a heat map. (C) The percentage of positive proliferative (SI) responses (calculated as number of positive responses divided by the total tested peptide pools times 100) per time point and per vaccine dose level (cohort) is depicted in the upper graph. The numbers above the bars indicate the number of patients. A two-way analysis of variance test was performed to determine the differences between the cohorts. (D) The MoM of SI (LST) was determined per patients per vaccine dose level (cohort) and each dot represents a patient. The Mann-Whithney test was used to determine differences between the dose levels. (E) The cytokines produced on recognition of HPV16 peptide pools and measured by CBA are displayed in a heat map. No cytokine production was measurable on E6.1 or the E7 peptides stimulation and therefore not shown here. CBA, cytometric bead array; LST, lymphocyte stimulation test; MoM, median of maximal response; PBMC, peripheral blood mononuclear cell; SI, stimulation index.
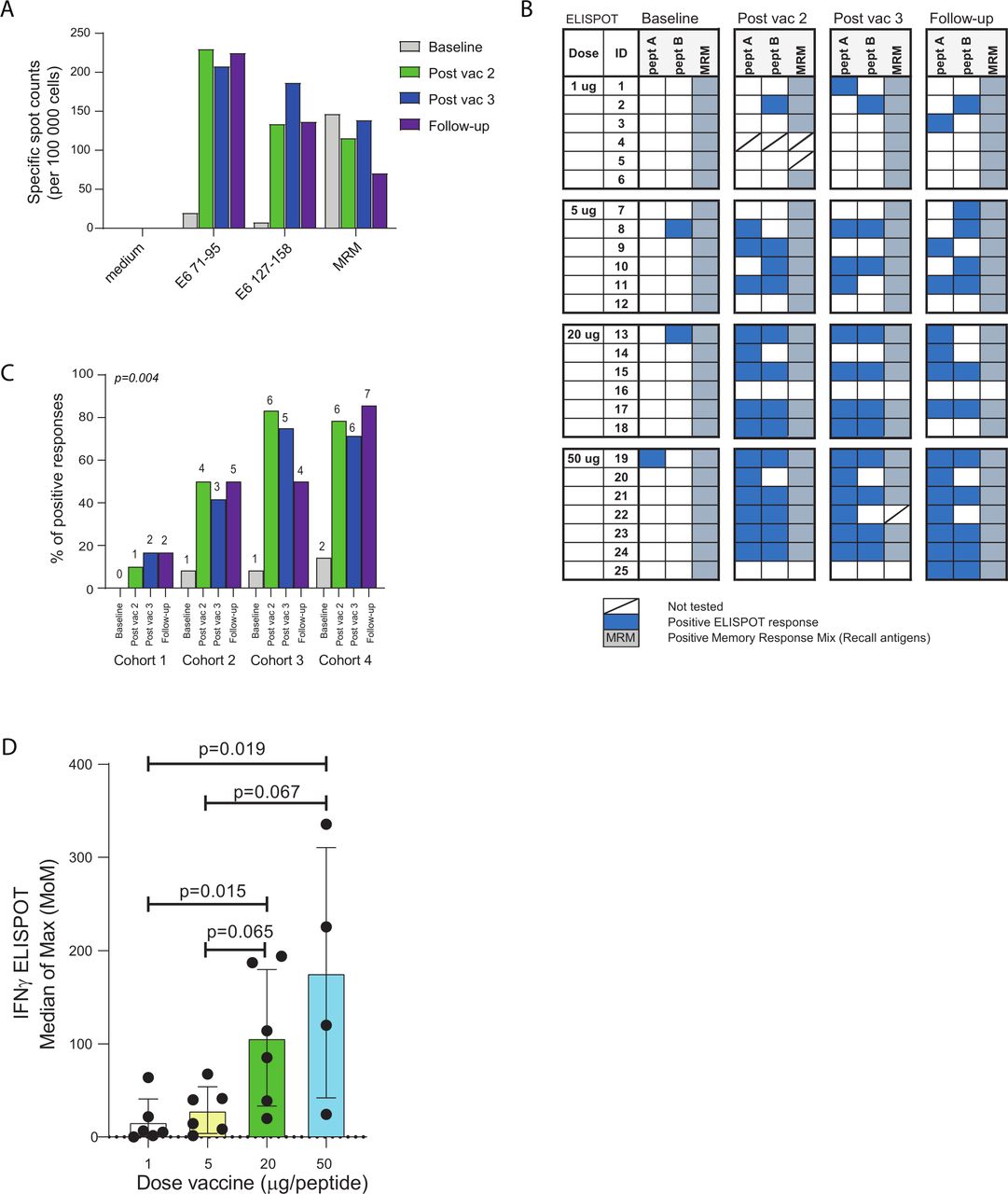
In the more sensitive and validated 4-day IFNγ ELISpot assay, T cell responses to the two vaccine peptides A (HPV16 E671-95) and B (HPV16 E6127-158) were measured. In this IFNy ELISpot assay, the baseline samples hardly showed any responses, which indicates that no in vitro induction occurred. In this IFNy ELISpot assay, the baseline samples hardly showed any responses, only in 4 out of 25 patients (#8, #13, #19 and #25) and only to one of the two vaccine peptides, which indicates that no in vitro induction occurred (online supplemental table 3). Figure 3A shows a time course of response induction in a representative patient (#19) indicating that two injections resulted in a significant increase in specific T cells to both vaccine peptides compared with baseline. The third and follow-up injection did not further enhance the response. In the lowest dose level (1 µg/conjugated peptide), two out of six patients showed a detectable response, while five out of the six patients in the second dose level (5 µg/conjugated peptide) were responsive to the vaccine. Similar results were found for dose level 3 (20 μg/conjugated peptide) and dose level 4 (50μg/conjugated peptide; online supplemental figure 2) in that all patients tested positive in the ELISpot assay to one or both vaccine peptides (figure 3B; online supplemental table 3). The percentage of positive responses per time point and dose level (cohort) is depicted in figure 3C, showing a significant (p=0.004) increase in response towards higher dose levels. Similarly, the MoM showed a correlation with the increased vaccine dose (figure 3D). To check whether the responses were higher in male or female, the MoM in the ELISpot and LST were depicted per gender in cohort 2 and 3, showing no statistical differences (online supplemental figure 3).
Supplemental material
Supplemental material

Frequency of IFNγ producing T cells increased with dose of vaccine. (A) An example of the 4-day IFNγ ELISpot results showing patient #19 against the two peptides in the vaccine (pept A: HPV16 E671-95 and pept B: HPV16 E6127-158). The specific spot counts are given per 105 cells. The cut-off defines a spot count of 10 above which a response is positive. (B) An overview of the ELISpot responses to the two vaccine peptides for all patients. (C) The percentage of positive ELISpot responses (calculated as number of positive responses divided by the total tested peptide pools times 100) per time point and per vaccine dose level (cohort) is shown. The numbers above the bars indicate the number of patients. A two-way analysis of variance test was performed to determine the differences between the cohorts. (D) Patients are grouped according to their dose of vaccine and the median of max (MoM, see Methods), is depicted for each patient by a dot. Statistical significant differences are indicated (Mann-Whitney test).
Furthermore, cytokine analysis at the single-cell level by flow cytometry revealed that both CD4+ and CD8+ T cells responded to the vaccine peptides (figure 4, online supplemental figure 4). In all six tested patients (#13, #15, #16, #17, #19 and #21; selected based on positive responses in the 4 day IFNγ ELISpot assay and availability of PBMCs), CD4+ T cell responses (multiple cytokines) were observed to one or both vaccine peptides. In one patient (#17), a CD8+ T cell response was observed which was directed to vaccine peptide B. Overall, the peptide conjugated vaccine showed potent immunogenicity and was able to induce functional T cell responses in almost all vaccinated patients when applied in a 20 µg or higher dose.
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Both CD4+ and CD8+ T cell responses are induced by the conjugated peptide vaccine. A selected (based on responses in the 4-day IFNγ ELISpot assay as well as availability of PBMCs) group of six patients were analyzed in the intracellular cytokine staining (ICS) after a 10-day prestimulation. The PBMCs were only tested for the two vaccine peptides (pept A: HPV16 E671-95 and pept B: HPV16 E6127-158) and SEB was taken along as a positive control. (A) The individual frequencies of the peptide responses (indicated cytokine) per patient as percentage of CD4+ (upper graphs) or CD8+ (lower graphs) T cells are given. (B) A heat map of the ICS responses for both CD4+ (upper) and CD8+ (lower) T cells is displayed. The dose of the vaccine and patient number (ID) is given. PBMCs, peripheral blood mononuclear cells; SEB, staphylococcal enterotoxin B.
Discussion
This phase I vaccination study shows that intradermal administration of amplivant-conjugated SLPs is safe with only minimal and mostly local side effects. Injection of the vaccine dissolved in watery solution was easy to administer, and none of the patients experienced direct problems or pain of the injection. Side effects were limited to inflammation at the site of injection and flu-like symptoms that occurred within 1 day and generally disappeared within 1 day. Increase in vaccine peptide dose resulted in a higher number of mild adverse events. In the highest dose group, all vaccinees experienced at least one adverse event. Therefore, we conclude that this self-adjuvanted peptide vaccine, which requires no further formulation, is a safe and easy-to-administer vaccination platform.
T cell responses after injection of the two amplivant conjugated HPV16-SLP were analyzed in all vaccinated patients. The response was positively associated with the dosage, that is, both in number of responding patients as well as in strength of the immune response. All patients in the highest dose cohort, even though six out of seven patients were patients with cancer, showed a vaccine-induced T cell response as determined by the validated 4-day IFNγ-ELISpot assay and except for one patient in the LST. Both antigen-specific CD8+ and CD4+ T cells were detected by ICS analysis after vaccination. HPV16-specific CD8+ T cells could be detected in one of the patients tested, while all patients displayed a HPV-specific CD4+ T cell response.
Interestingly in our study, CD4+ T cell responses to the vaccine were more frequently found compared with CD8+ T cell responses. This is consistent with results found in our previous conducted vaccination studies with HPV16-SLP.2–4 We have also observed in a majority of healthy individuals, who have successfully cleared HPV16, the presence of HPV-16 E6-specific memory Th responses.21 Also in other vaccination studies to tumor antigens, like melanoma neoantigens, dominating vaccine-induced CD4+ T cell responses were observed,5 22 which correlated with clinical responses. Therefore, it is assumed that these tumor-specific CD4+ T cells are clinically relevant and may be involved in other mechanisms than only help for tumor reactive CD8+ T cells.
The functionality of the T cells can also be characterized by the cytokines produced as determined by CBA in the supernatant of the LST. Both IFNγ and IL-5 were produced specifically on vaccine peptide stimulation, a cytokine combination already often observed in patients who were vaccinated with HPV16-SLP and showed regression of their premalignant lesions or in healthy individuals who had spontaneously cleared previous HPV16 infections.20 21 TNFα and IL-10 were found in much lower concentrations and often did not reach levels above the threshold. In three patients (patients 11, 13 and 23), the IL-10 (although at low levels) dominated the cytokine response to HPV16 peptide pool E6.2, which might be suggestive for vaccine-boosted E6-specific regulatory T cells (Tregs) as we described earlier.20 When the cytokine levels were compared with historical data from HPV16-SLP vaccinated HPV16+ VIN3 patients4 20 and HPV16+ cervical cancer patients, it appeared that the levels of both IFNγ and IL-5 in this study were in the same order of magnitude or lower. However, cytokine levels were much higher in the cervical cancer patients vaccinated with HPV16-SLP during chemotherapy,3 suggesting that combination therapy of the vaccine and chemotherapy, shown to reduce systemic and local immune suppression, might be a worthwhile future perspective. An encouraging finding is that the ELISpot responses in the highest dose cohort are comparable with clinically responding patients in the combined HPV16-SLP and chemotherapy trial.3 Due to the trial set up and patient availability, the male–female ratio in dose cohorts 1 and 4 is unfortunately unbalanced. Nevertheless, in case of dose cohorts 2 and 3, no significant difference in outcomes for the ELISpot and LST were observed when patients were grouped by gender. Therefore, it is likely that the unfortunate but unintentionally skewed male–female ratio in dose cohorts 1 and 4 did not influence the T cell response outcomes. Overall, these results demonstrate that these two selected and conjugated HPV16 E6 peptides can be processed and presented by almost all patients, independent of the HLA type of the patient, to elicit a functional T cell response. Whether the vaccine-induced response is sufficient to clear HPV virus or to eradicate premalignant lesions or tumors remains to be established.
The design of this first in human study with the molecularly optimized TLR2 ligand amplivant was based on a number of studies including the synthetic design, in vitro analysis and preclinical murine and ex vivo human experiments.10 17 The PBMC sampling in the current trial was focused on the T cell response measurement and too long after vaccination to determine the efficacy of the TLR2 ligand amplivant, which required a blood sample 2–3 days following vaccination. However, the fact that in the highest dose cohort all patients responded with redness on the vaccination site 2–3 days postvaccination is indicative for a response to the TLR2 agonist. Key reports using TLR-ligand conjugated antigenic peptides were reported already more than 30 years ago.23 We have optimized several defined TLR-ligands aside from TLR2, like TLR9, TLR4 and TLR7 to covalently link to adjuvant antigenic peptides in a defined way.8 12 24 25 The TLR-ligand is generally attached to the N-terminus of the peptide in a one-to-one stoichiometry, which turned out to be immunologically highly effective and outperformed free peptides mixed with equimolar amounts of free ligands in both in vitro and in vivo T cell activation in different tumor models.10–12 17 An important advantage of this self-adjuvanted vaccine platform is that it can be administered by a simple single injection and without any other formulation or additional adjuvant . The current study, validates the feasibility of this vaccine platform in patients.
The amplivant-conjugated HPV16 SLP vaccine was injected intradermally, and therefore, we expect efficient targeting to a dense network of dermal DCs. Intradermal vaccination strategies for vaccination have been tested in several cancers26–28 and have met with some clinical benefit.29 30 It was shown before that an intradermal injection with the non-conjugated HPV16 SLP injected at a dose of 10 µg per peptide in healthy subjects is safe and results in the induction of an HPV16-specific Tcell response.31 The change of routing (intradermal instead of subcutaneous vaccination) also allowed us to omit the Montanide oil-depot, which was thus far used for subcutaneous SLP administration for both therapeutic HPV16 vaccines as for neoantigen vaccines. Our current conjugate vaccine can therefore easily be administered in watery solution and is immunogenic without any other formulation.
In summary, this first in human study with amplivant conjugated SLPs shows that conjugation of an optimized TLR2-ligand to SLPs is safe and can potently induce vaccine-specific T cell immunity with acceptable side effects. The vaccination platform is flexible and can potentially be used to self-adjuvant any peptide sequence in GMP conditions, including shared cancer antigens and patient-specific neo-epitope sequences. Whether conjugation of amplivant to SLP induces effective tumor-reactive T cell responses is subject to future investigations.
Supplemental material
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Central Committee on Research Involving Human Subjects in the Netherlands, ID: NL48274.000.14. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank the patients and their families for participating in the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Study conception and design: FMS, MJPW, MS, MIEvP, PJdVvS, W-JK, CJMM, SHVdB, HG and FO. Provision of study material or patients: FMS, MJPW, MS, MIEP, PJdVvS, IR, SB, NML, ARPMV, HG and CAHJ. Collection and assembly of data: FMS, MJPW, IR, SB, NML, SHVdB, HG and CAHJ. Data analysis and interpretation: FMS, MJPW, SHVdB, HG and FO. Manuscript writing: all authors. Final approval of manuscript: all authors. Accountable for all aspects of the work: all authors. Guarantor: FO
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests FO, CJMM, DVF and GAvdM are inventors of a patent application related to the work in this article entitled 'Adjuvant compound', with publication number WO 2013/051936 and filing date October 4, 2012. CJMM and WJK receive a salary from ISA Pharmaceuticals BV and are in possession of ISA stock appreciation rights and are inventors on patents that are licensed to or owned by ISA Pharmaceuticals BV, dealing with synthetic long peptide vaccines. SHB is named as an inventor on the patent for the use of synthetic long peptides as vaccine. SHB serves as a paid member of the strategy board of ISA Pharmaceuticals and received honoraria as a consultant for PCI Biotech, IO Biotech and DC prime.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.