Article Text

Abstract
Anaplastic thyroid cancer represents a rare, highly aggressive form of thyroid cancer with a poor prognosis and an overall survival ranging from 5 to 12 months. Unfortunately, treatment options remain limited, even for patients with a targetable driver mutation. Here, we present a case of a patient with a BRAF V600E-mutated, PD-L1 positive (tumor proportion score of 95%) anaplastic thyroid cancer refractory to standard therapies, including debulking surgery, followed by chemoradiation, who had further progressed on PD-1 monotherapy, and was unable to tolerate BRAF/MEK inhibition. Ongoing treatment with FS118, a bispecific LAG-3/PD-L1 antagonist, has afforded 3 years of disease control, including a late confirmed partial response, with excellent tolerability. Given this response, further investigation is required to delineate the mechanism by which dual PD-L1/LAG-3 blockade by FS118 overcomes initial PD-1 pathway resistance, and therefore, identify which patients are most likely to benefit. Simultaneously, expanded use should be considered for those with refractory disease, especially if PD-L1 positive.
Insights
Dual PD-L1/LAG-3 blockade may be an effective treatment strategy for refractory metastatic tumors, including anaplastic thyroid cancer.
- Immunotherapy
- Head and Neck Neoplasms
- Therapies, Investigational
- Translational Medical Research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
In contrast to differentiated thyroid cancer, anaplastic thyroid cancer (ATC) is rare and extremely aggressive. While it accounts for less than 2% of all thyroid cancers, it leads to greater than 50% of annual thyroid cancer-related mortality.1 Recently, there has been rapid acceleration in the development and implementation of novel therapies, including targeted therapies and immunotherapy. Most notably, up to 50% of ATCs harbor BRAF V600E mutations and a recent phase II study demonstrated that dual BRAF/MEK inhibition with dabrafenib and trametinib led to an overall response rate of nearly 70%.2 However, even in the era of target therapy, the median overall survival (OS) of ATC is 5–12 months.1
Given the dismal prognosis, novel therapies are needed. Immunotherapy represents a promising approach in ATC: approximately 22% are PD-L1 positive, a proportion substantially higher than in differentiated thyroid carcinoma.3 Case reports combining immunotherapy with targeted therapies (eg, BRAF inhibitors, multitarget kinase inhibitors) have demonstrated some success, but durability of responses remains limited.4
The addition of LAG-3 blockade to anti-PD-1 in vitro enhances proliferation and cytokine secretion of T-cells compared with PD-1 blockade alone,5 providing a preclinical rationale for combination PD-1 and LAG-3 blockade for ATC refractory to standard therapies, including prior PD-1 inhibitors. Here, we present a case of a patient with ATC with progression on multiple lines of therapy, including BRAF/MEK inhibitors and a PD-1 inhibitor, with an ongoing and durable response to FS118, a tetravalent bispecific anti-PD-L1 and anti-LAG-3 molecule.6 7
Case presentation
A woman in her 60s presented in May 2017 with enlarging right thyroid nodules. Thyroid ultrasound demonstrated a 1.2 cm mass in the right thyroid. Pathology from her thyroidectomy June 13, 2017 demonstrated a 6.5 cm ATC with extensive extrathyroidal extension, positive for BRAF V600E and TERT mutations and negative for NTRK and RET rearrangements. Postoperative PET/CT revealed intense FDG-avidity of the residual mass in addition to multiple right cervical and paratracheal nodes suggestive of lymph node metastases, but no distant visceral metastases.
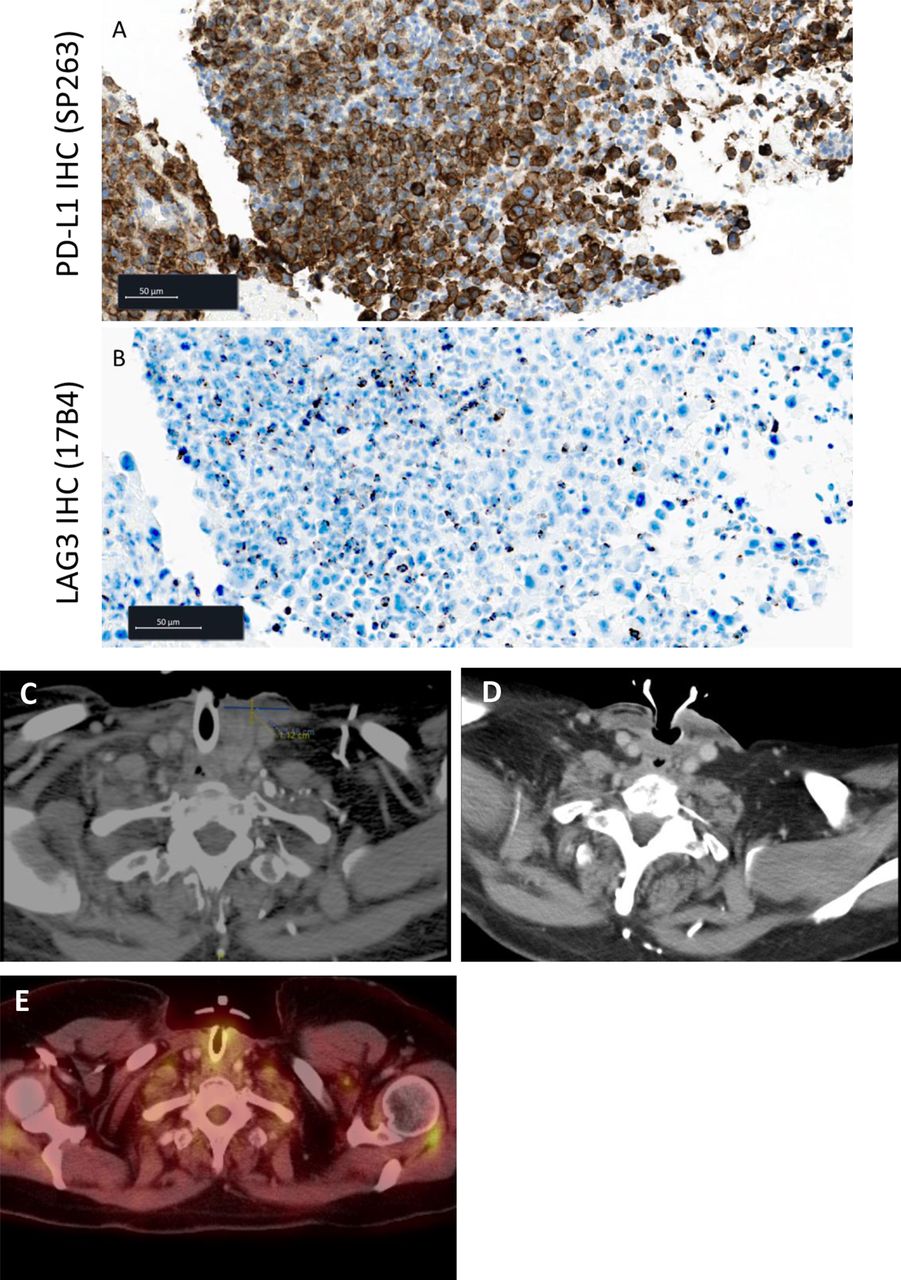
Postoperatively, the patient completed concurrent carboplatin and paclitaxel with daily radiotherapy. Despite initial surgery followed by chemoradiation, CT of her neck and chest on December 14, 2017 demonstrated an enlarging mass in the left thyroidectomy bed. Biopsy confirmed residual ATC with a PD-L1 tumor proportion score (TPS) of 95%. Additional retrospective analysis of this tissue for PD-L1 IHC (clone SP263) and LAG-3 confirmed high PD-L1 expression with a TPS of 80% (calculated as percent viable tumor cells with positive PD-L1 staining) (figure 1A). Furthermore, LAG-3 was quantified in selected five high power fields (HPF) within the interepithelial tumor component and five HPF within the intratumoral stroma. All selected HPF were positive for LAG-3 with an average of five cells/HPF within the tumor and 2.2 cells/HPF within the stroma (figure 1B).
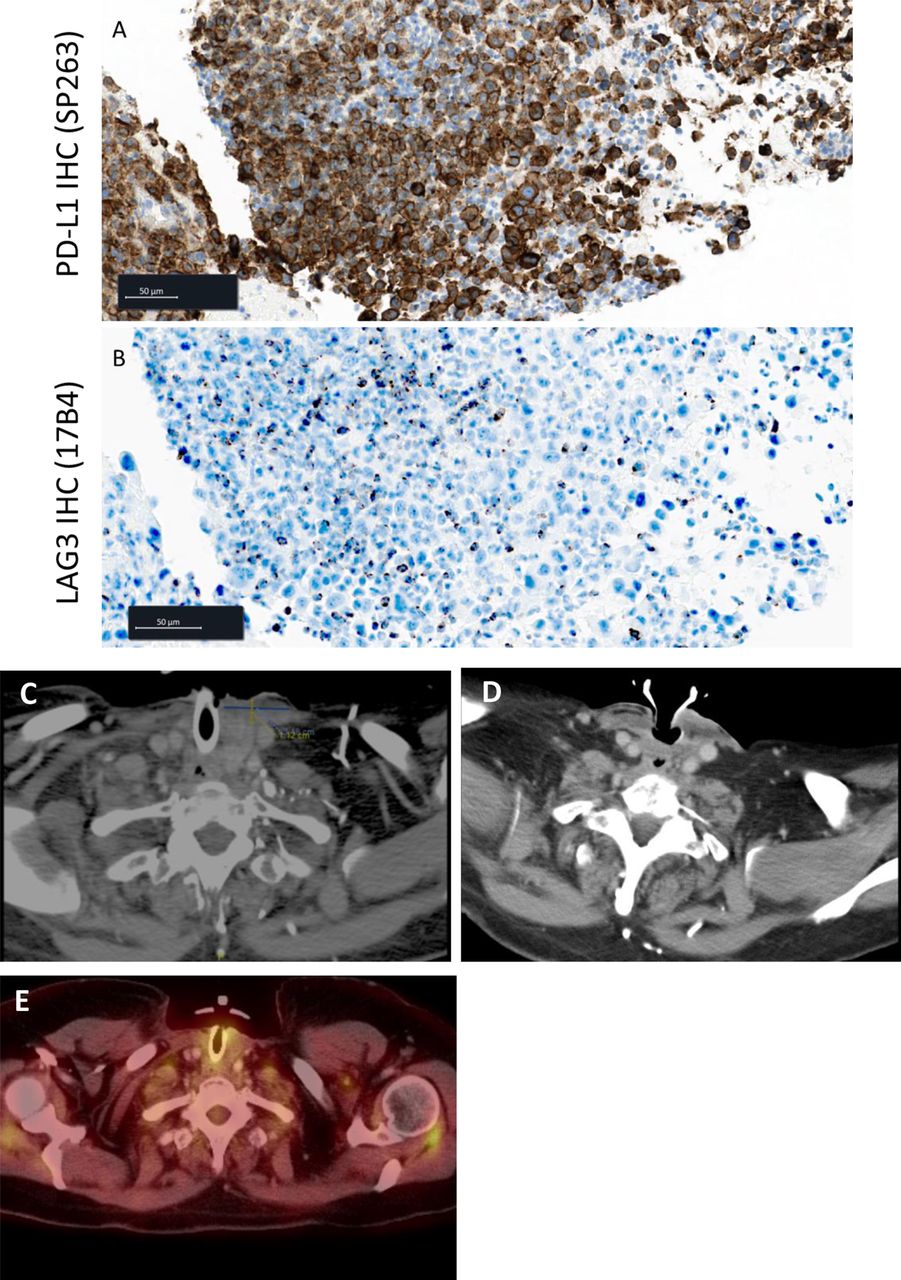
Treatment with FS118 results in radiographically stable perithyroidal metastasis from anaplastic thyroid carcinoma. Baseline tumor expression of target lesion for (A) PD-L1 (anti-PD-L1 IHC antibody SP263, Ventana/Roche) and (B) LAG-3 (anti-LAG-3 IHC antibody, clone 17B4, Abcam). Target lesion (C) prior to initiation of FS118 measuring 32 mm × 11 mm (February 24, 2019), (D) during cycle 57 treatment with FS118 measuring 18 mm × 11 mm (June 9, 2022), and (E) Positron Emission Tomography/Computed Tomography (PET/CT) without fluorodeoxyglucose (FDG) uptake after cycle 38 treatment with FS118 (March 15, 2021).
The patient began an open-label, phase 2 clinical trial of the PD-1 inhibitor nivolumab, on January 24, 2018. Baseline imaging January 16, 2018 demonstrated a 58×39 mm primary left thyroid mass and an adjacent, new parastomal mass measuring 46 mm × 28 mm. She achieved a partial response to treatment with decreases in both lesions to 42 mm × 29 mm and 33 mm × 21 mm, respectively, on May 17, 2018. However, imaging October 8, 2018 showed progression of the necrotic parastomal mass in the left strap muscles to 48 mm × 46 mm. The left thyroid gland lesion remained improved (34 mm × 26 mm). The patient was taken off study and began combined therapy with dabrafenib, trametinib, and nivolumab on October 10, 2018. This was interrupted within 1 month for high-grade fevers as high as 43°C. On restarting the dabrafenib and trametinib, she suffered grade III drug-induced liver injury, preventing further treatment. The final dose of nivolumab was administered on November 26, 2018. Dabrafenib and trametinib were held after December 10, 2018.
On March 1, 2019, the patient enrolled in FS118-17101 (NCT03440437), a first-in-human study of FS118 in patients with advanced malignancies.6 Of the 43 subjects enrolled, she represented the sole case of ATC.6 Within 1 month of treatment with FS118 20 mg/kg weekly, the patient had rapid, subjective improvement in the neck mass along with improvement in swallowing. Recent restaging CT of the neck, chest, abdomen and pelvis demonstrates a sustained partial response by Response Evaluation Criteria in Solid Tumors (RECIST) criteria (18 mm × 11 mm on June 9, 2022, previously 32 mm × 11 mm at enrolment) without development of any new nodal or visceral metastases (figure 1C,D). Furthermore, a Positron Emission Tomography/Computed Tomography (PET/CT) performed after cycle 38 demonstrated no fluorodeoxyglucose (FDG) uptake (figure 1E).
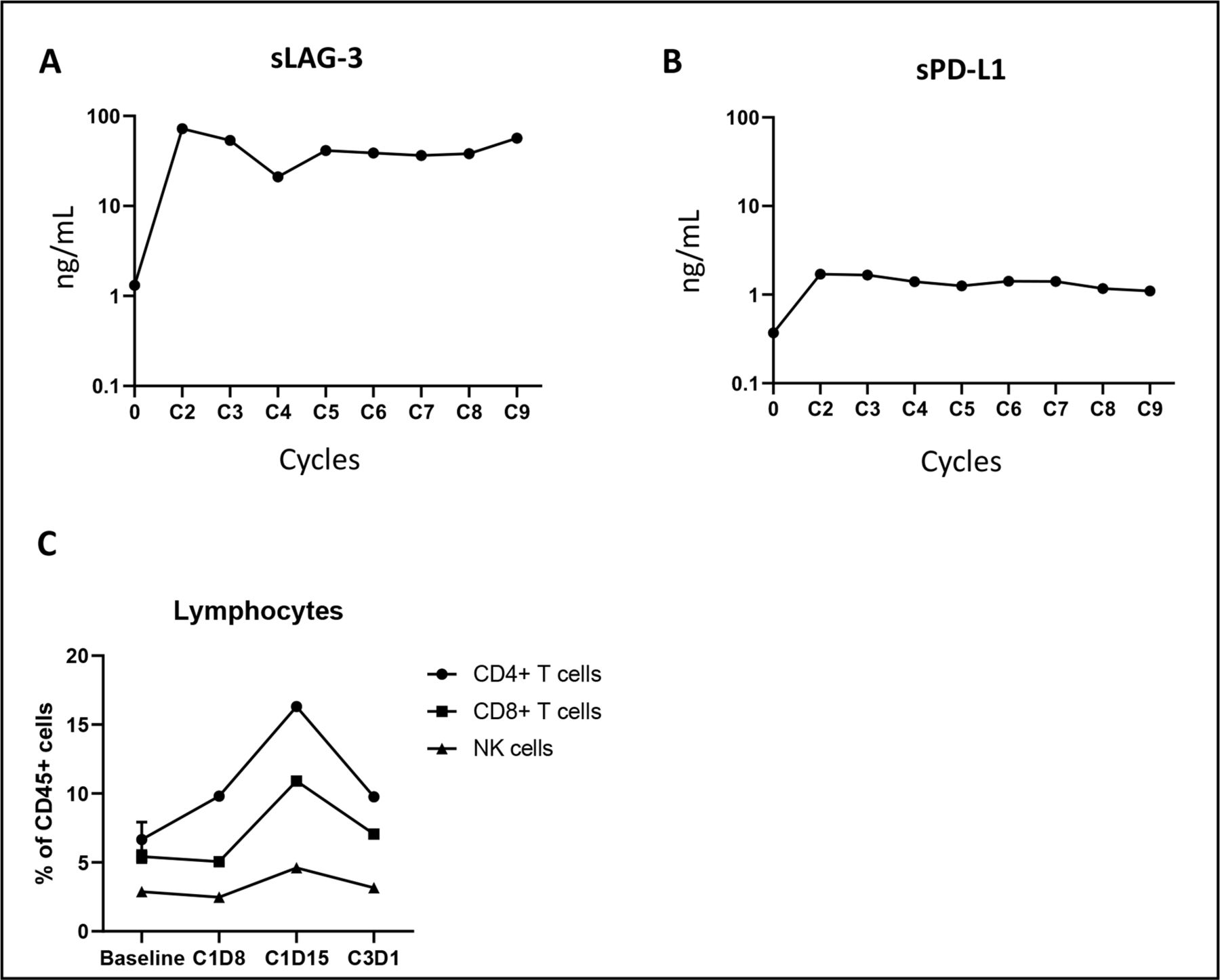
Measurement of soluble LAG-3 and PD-L1 concentrations in the serum revealed a substantial increase in sLAG-3 levels and more moderate increase in sPD-L1 (figure 2A,B). Elevated serum receptor levels were observed continuously throughout nine cycles (data not available for further cycles), indicative of continuous target engagement and enhanced shedding of receptors. In addition, measurement of circulating immune cells demonstrated an increase in the proportions of CD4+, CD8+ and NK cells 2 weeks following the first dose of FS118, suggesting lymphocyte expansion in response to FS118 (figure 2C).
{kind=link}
{kind=link}
Enhanced LAG-3 shedding and expansion of circulating lymphocytes following FS118 treatment. Total serum concentration of soluble LAG-3 was measured using an ELISA. Samples for soluble receptors were taken prior to dosing on each cycle. (A) total serum concentration of sLAG-3 as measured by ELISA. Serum sLAG-3 was complexed with a saturating concentration of FS118, and the complex was captured with a non-competing anti-LAG-3 antibody clone 17B4 (Enzo life sciences) and detected with a non-competing anti-FS118 anti-idiotype antibody (Maine biotechnology services). (B). Total serum concentration of soluble PD-L1 was measured using electrochemiluminescence immunoassay (ECLIA). (B) soluble receptors were complexed with saturating amount of FS118, captured with a non-competing anti-PD-L1 antibody clone 130 021 (BioTechne) and detected with anti-FS118 anti-idiotype antibody (Maine biotechnology services). Max increase from baseline: 55 x (sLAG-3), 4.6 x (sPD-L1). (C) circulating T cells and NK cells 8 and 15 days post first dose, and on predose of cycle 3 day 1. Immunophenotyping was performed using flow cytometry on live fresh blood cells. The panel included antibodies to CD45 (HI30, BD biosciences, 563204), CD3 (SK7, BD biosciences, 564001), CD19 (HIB19, BioLegend, 302240), CD4 (SK3, BD biosciences, 563028), CD8 (SK1, BD biosciences, 564629), CD56 (HCD56, BioLegend, 318334) and Ki67 (20Raj1, eBioscience, 46-5699-42). Immune cell populations were defined as: CD4 T- cells (CD45+/CD3+/CD4+/CD8-/CD19-), CD8 T- cells (CD45+/CD3+/CD8+/CD4-/CD19-) and NK cells (CD45+/CD3-/CD19-/CD56+/CD16+/-). All values were reported as a percentage of total CD45+leucocytes, and only cell subsets with more than 50 cells were considered.
Consistent with reported results, treatment with FS118 continues to be well tolerated overall with minor grades 1 and 2 adverse events such as occasional nausea, fatigue, and arthralgias without need for corticosteroids. The patient continues on treatment, recently having completed 57th cycles without any related toxicity of Common Terminology Criteria for Adverse Events (CTCAE) grade 2 or more and with ongoing disease and clinical benefit, over 3 years from the start of FS118 treatment.
Discussion
Here, we present a case of a patient with a BRAF V600E and PD-L1 positive ATC who received maximal local, combined modality treatment. She progressed after a relatively brief response to single agent checkpoint inhibition with nivolumab, but subsequent treatment with FS118, a LAG-3/PD-L1 tetravalent bispecific antibody, has afforded her a sustained partial response with excellent tolerability for over 3 years.
Widespread use of molecular profiling has changed the diagnostic and therapeutic landscape of ATC. Targeting BRAF and MEK is one of the most notable novel therapeutic interventions in ATC thus far, given the relative frequency of BRAF V600 mutations and response rates of nearly 70% in a traditionally treatment-refractory disease.2 Yet, BRAF and MEK inhibition also has its limitation, as evidenced by limited tolerability in the patient presented in our case.
Beyond targeted therapies, the case highlights the increasing relevance of immunotherapy for ATC. A phase 1/2 study of spartalizumab demonstrated the most promising results of checkpoint inhibitor monotherapy in ATC with an overall response rate of 19% across 42 patients.8 Similarly, a phase 2 study evaluating pembrolizumab in progressive radioactive iodine refractory thyroid cancer, revealed an overall response rate of 18.8% in the ATC cohort with a median OS of 3.6 months.9 Therefore, while response rates to various single agent PD-1/PD-L1 in ATC are not insignificant, especially in a notoriously treatment-refractory disease, they do result in temporally limited responses. As in this case, despite the markedly elevated PDL-L1 TPS and an excellent initial radiographic partial response to nivolumab, acquired resistance developed within 9 months.
Combined immune checkpoint inhibition with a tyrosine kinase inhibitor (TKI) has also been pursued in ATC, with some success, particularly with pembrolizumab.4 Yet median PFS after the addition of pembrolizumab to TKI remained under 7 months in a single center review.4 Given the limited treatment options in progressive ATC and the patient’s prior excellent tolerability of single agent nivolumab, such a strategy was pursued in this patient. It remains unknown whether this patient would have achieved a more durable response, as she was unable to tolerate further therapy secondary to progressive side effects including grade 3 transaminitis and high-grade fevers. Nonetheless, dual PD-L1/LAG-3 inhibition with FS118 has afforded her both durable and tolerable treatment for over 3 years in a disease with a median OS of under 1 year.
Clinical trials in ATC are limited given its low incidence and aggressive nature, but additional novel therapies are needed. This case highlights one such approach, using FS118, which is well tolerated at the dose level of 20 mg/kg.10 In addition to high PD-L1 TPS (figure 1A), retrospective assessment of tissue biopsied prior to nivolumab therapy detected LAG-3 positive cells both within the tumor and in the intratumoral stroma (figure 1B), indicating a tumor microenvironment with the potential for benefit from a PD-L1/LAG-3 bispecific blockade. Pharmacokinetics confirm exposure broadly consistent with preclinical data with low immunogenicity, and pharmacodynamic activity was prolonged, demonstrated by sustained increased levels of soluble LAG-3 throughout the dosing period and an increase in immune cell numbers. Early data demonstrate durable clinical benefit in some patients, particularly in patients with acquired resistance to PD-1/PD-L1 pathway blockade as in this subject.
Given this success, further investigation is required to further delineate the mechanism by which dual PD-L1/LAG-3 blockade overcomes initial PD-1/PD-L1 resistance in ATC, and therefore, which patients are most likely to benefit. Furthermore, given this patient’s remarkable and prolonged response to FS118, a dual inhibitor of LAG-3 and PD-L1 inhibition, additional investigation of FS118 for ATC should be pursued.
Ethics statements
Patient consent for publication
Ethics approval
This is a case report that does not contain any identifiable patient information. The subject of this case report is enrolled in a clinical trial that is approved by the UCLA institutional Review Board and the patient provided informed consent for participation in the clinical trial.
Footnotes
Contributors J-BH contributed to study conception and design; J-BH and LK contributed to study monitoring. J-BHH and DJW collected the data. J-BH, MJK, LK, MM, OS, CJS and DJW analyzed and interpreted the data; MJK, CJS, OS and DJW contributed to writing the manuscript; LK, MJK, MM, CJS and DJW edited the manuscript. All authors reviewed and approved the final version of the manuscript.
Funding F-Star Therapeutics provided funding to the institution for the clinical trial the subject is enrolled in (IRB# 18-000365).
Competing interests MJK, J-BH and OS have no relevant competing interests. LK, MM, and CJS are employees of F-star Therapeutics and hold stock options in F-STAR Therapeutics. DJW has received research funding paid directly to the institution from FSTAR Therapeutics.
Provenance and peer review Not commissioned; externally peer reviewed.