Article Text

Abstract
Merkel cell carcinoma is a rare, highly aggressive skin cancer with neuroendocrine differentiation. Immune checkpoint inhibition has significantly improved treatment outcomes in metastatic disease with response rates to programmed cell death protein 1/programmed cell death 1 ligand 1 (PD-1/PD-L1) inhibition of up to 62%. However, primary and secondary resistance to PD-1/PD-L1 inhibition remains a so far unsolved clinical challenge since effective and safe treatment options for these patients are lacking.
Fourteen patients with advanced (non-resectable stage III or stage IV, Union international contre le cancer 2017) Merkel cell carcinoma with primary resistance to the PD-L1 inhibitor avelumab receiving subsequent therapy (second or later line) with ipilimumab plus nivolumab (IPI/NIVO) were identified in the prospective multicenter skin cancer registry ADOREG. Five of these 14 patients were reported previously and were included in this analysis with additional follow-up. Overall response rate, progression-free survival (PFS), overall survival (OS) and adverse events were analyzed.
All 14 patients received avelumab as first-line treatment. Thereof, 12 patients had shown primary resistance with progressive disease in the first tumor assessment, while two patients had initially experienced a short-lived stabilization (stable disease). Six patients had at least one systemic treatment in between avelumab and IPI/NIVO. In total, 7 patients responded to IPI/NIVO (overall response rate 50%), and response was ongoing in 4 responders at last follow-up. After a median follow-up of 18.85 months, median PFS was 5.07 months (95% CI 2.43—not available (NA)), and median OS was not reached. PFS rates at 12 months and 24 months were 42.9% and 26.8 %, respectively. The OS rate at 36 months was 64.3%. Only 3 (21%) patients did not receive all 4 cycles of IPI/NIVO due to immune-related adverse events.
In this multicenter evaluation, we observed high response rates, a durable benefit and promising OS rates after treatment with later-line combined IPI/NIVO. In conclusion, our patient cohort supports our prior findings with an encouraging activity of second-line or later-line IPI/NIVO in patients with anti-PD-L1-refractory Merkel cell carcinoma.
- Skin Neoplasms
- CTLA-4 Antigen
- Programmed Cell Death 1 Receptor
- B7-H1 Antigen
- Drug Therapy, Combination
Data availability statement
Data are available upon reasonable request. Data will be provided by the corresponding author upon request for reasonable academic studies.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Merkel cell carcinoma (MCC) is a rare, highly aggressive skin cancer with neuroendocrine differentiation which occurs predominantly in chronically ultraviolet (UV)-exposed skin sites of elderly.1 2 Etiological factors promoting the development of this cutaneous neoplasia include the Merkel cell polyomavirus (MCPyV) and UV irradiation.1 For unresectable and metastatic disease immune checkpoint inhibition (ICI) has transformed treatment outcomes in a subset of patients. First-line programmed cell death protein 1 (PD-1) blockade with pembrolizumab and programmed cell death 1 ligand 1 (PD-L1) blockade with avelumab have shown high objective response rates (ORR) of 56% and 62%.3–5 Hence, the approval of PD-L1 inhibition with avelumab for advanced and metastatic MCC has replaced chemotherapy as first-line systemic therapy.5 However, a substantial number of patients show primary or acquired resistance to PD-L1 monotherapy. Unfortunately, homogenous data on subsequent treatment options for PD-L1/PD-1 refractory patients are still lacking. We recently reported a retrospective multicenter cohort of five patients with metastatic MCC showing primary resistance to avelumab being treated with subsequent ipilimumab plus nivolumab (IPI/NIVO).6 In our analysis, later-line treatment with combined immunotherapy resulted in a promising ORR of 60%. With approved systemic treatment options for these patients being limited to chemotherapy regimes showing mostly short-lived responses, we now conducted an extended analysis using the prospective multicenter skin cancer registry ADOREG.
Materials and methods
Patient cohort and data acquisition
The database of the prospective multicenter skin cancer registry ADOREG was queried for patients with unresectable stage III or stage IV MCC with primary resistance (best overall response (BOR) progressive disease (PD) or stable disease (SD) for less than 6 months according to Response Evaluation Criteria In Solid Tumors (RECIST) V.1.1) to first-line therapy with the PD-L1 inhibitor avelumab who received combined IPI/NIVO as any later treatment line. First-line treatment with avelumab for unresectable or metastatic disease was initiated between January 2017 and April 2021. Treatment with IPI/NIVO was initiated between January 2019 and September 2021 (data-cut off May 3, 2022). Tissue used for molecular analyses was collected during routine care for diagnostic or therapeutic reasons.
Exclusion criteria comprised prior adjuvant treatment with a PD-1 or PD-L1 inhibitor. Patients who had received adjuvant radiotherapy or had additive radiotherapy during ICI with avelumab or IPI/NIVO were eligible. Demographic and clinicopathological data including treatment specific outcomes were extracted from the ADOREG registry and hospital records by chart review.
ADOREG is a multicentric registry of the German Dermatologic Oncology Group (DeCOG) prospectively collecting real-world data of patients with skin cancer treated at skin cancer centers. On August 1, 2022, 67 centers were actively recruiting patients into ADOREG, and 794 patients with MCC had been enrolled. Details are provided at https://www.hautkrebsregister.de/en. The participating institutions were queried for endpoint data.
Five of the 14 patients were reported previously and included in this analysis with additional follow-up.6 For these patients, informed consent had been waived by the Ethics Committee of the University of Würzburg due to the retrospective nature of the study.
Definition of end-points and statistical analysis
Endpoints were ORR, progression-free survival (PFS), overall survival (OS) and safety (irAE). Radiological tumor assessment and response was performed according to the RECIST V.1.1.7 Radiological response to tumor therapy was defined as follows: complete response (CR), partial remission (PR) or stable disease (SD) for more than 6 months. Best changes in the sum of diameters were calculated with Microsoft Excel and depicted in a waterfall plot as % change from baseline. PFS and OS were calculated from the first cycle of IPI/NIVO to the last tumor assessment, respectively, the last consultation or date of death using the Kaplan-Meier method. The analyses were performed using R V.4.1.1 (R packages survival, swimplot). IrAE were documented and graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) V.5.0.
Results
Patient demographics
Fourteen patients, 64.3% (9/14) being male, with unresectable stage III (21.4%) or stage IV (78.6%) MCC according to UICC 2017 with a median follow-up of 18.85 months (IQR 17.63–22.40) were included in our analysis. Median age at first MCC diagnosis was 64 years (range 53–83). MCPyV status was determined in 10 patients. For the remaining patients, tissue for analysis was unavailable. Congruent to the literature, 80% were MCPyV positive. The PD-L1 status was determined in seven patients. Patient demographics are summarized in table 1.
Patient characteristics
First-line avelumab and subsequent therapies
All patients received first-line avelumab treatment for unresectable or metastatic disease. Median number of cycles was 5 (range 2–12). Twelve patients showed PD in the first tumor assessment and two patients experienced a short-lived stabilization (SD) followed by disease progression. Four patients received chemotherapy (carboplatin plus etoposide or cisplatin plus etoposide) as second-line treatment. Two of these 4 patients showed partial remission under chemotherapy and were re-exposed to avelumab after tumor progression. One of these 4 patients received third-line therapy with the PD-1 inhibitor nivolumab. All 3 patients showed PD to third-line PD-L1 or PD-1 inhibition, respectively. One patient was treated with nivolumab and another patient with a Mdm2 inhibitor as second-line treatment. The remaining 8 patients did not receive a systemic therapy in between avelumab and IPI/NIVO.
Therapy outcome IPI/NIVO
All 14 patients received combined IPI/NIVO (10 patients with IPI 3 mg/kg plus NIVO 1 mg/kg; 4 patients with IPI 1 mg/kg plus NIVO 3 mg/kg) as subsequent later-line therapy. Three out of 4 patients responded to the flipped-dose (IPI 1 mg/kg plus NIVO 3 mg/kg). Seven (7/ 14; 50%) patients had normal lactate dehydrogenase levels and Eastern Cooperative Oncology Group Performance Score was ≤1 in 78.6% (11/14) of the patients prior to IPI/NIVO. A median number of 4 cycles (range 1–4) IPI/NIVO was administered. Only 1 patient (1/14; 7.1%) received additive radiotherapy accompanying IPI/NIVO and showed PD as BOR.
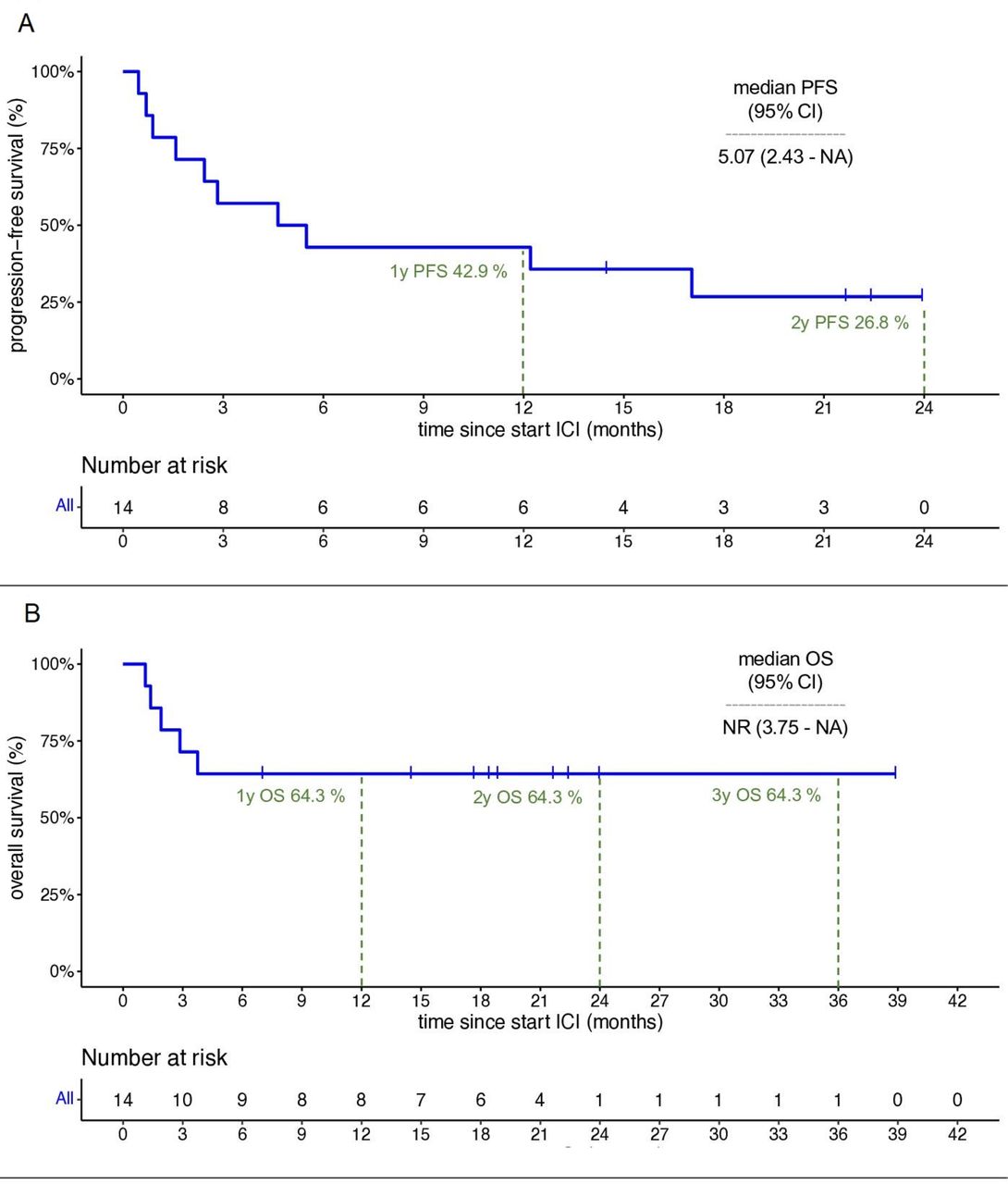
Seven out of 14 patients (1 × CR; 6 × PR) responded to combined IPI/NIVO according to RECIST V.1.1 resulting in an ORR of 50%. A waterfall plot showing the best change in target lesion diameters can be found in online supplemental figures 1A. The median PFS (mPFS) on IPI/NIVO was 5.07 (95% CI 2.43 to not available (NA)) months (figure 1A). The PFS rates were 42.9% at 12 months and 26.8% at 24 months (figure 1A). The median OS (mOS) from start of IPI/NIVO has not been reached after a median follow-up of 18.85 months (figure 1B). The OS rate at the landmarks 12 months, 24 months and 36 months is 64.3% (figure 1B). Detailed outcome data can be found in table 2.
Supplemental material
Supplemental material
{kind=link}
Kaplan-Meier analyses. (A) Progression-free survival (PFS) for all patients (n=14). (B) Overall survival (OS) for all patients (n=14). Dashed lines indicate 1-year (1y), 2-year (2y) and 3-year (3y) landmarks. ICI, immune checkpoint inhibition; mOS, median overall survival; mPFS, median progression-free survival; NA, not available; NR, not reached.
Outcome associated with later-line IPI/NIVO
Adverse events and safety
In our analysis, 57.1% (8/14) of the patients experienced an irAE of any grade according to CTCAE V.5, with 50% (4/8) graded mild to moderate (grade 1–2) and 50% (4/8) graded severe (≥ grade 3). Involved organ systems were, as previously described, the gastrointestinal (colitis), respiratory (pneumonitis) and endocrine system (adrenal insufficiency). In 1 patient cycles 3 and 4 of IPI/NIVO were delayed and 3 patients received less than 4 cycles of IPI/NIVO due to an irAE. Two of the 3 patients who did not receive 4 cycles of IPI/NIVO due to an irAE showed PD in the first tumor assessment while the remaining patient showed PR and is receiving nivolumab as maintenance therapy despite the former toxicity. Detailed information is shown in table 3.
Immune-related adverse events associated with later-line therapy with IPI/NIVO
Follow-up
At a median follow-up of 18.85 months (IQR 17.63–22.40), 64.3% (9/14) of the included patients were still alive. Of these 9 patients, 44.4% (4/9) have not progressed so far. Of these 4 patients showing ongoing responses, two are receiving maintenance therapy with nivolumab. Five patients (5/14, 35.7%) died due to tumor progression (online supplemental figures 1B).
Of note, 1 patient showed a CR after 4 cycles of IPI/NIVO. Unfortunately, he relapsed twice after combined ICI. He was treated with surgery (PFS 12.2 months) and re-exposed to IPI/NIVO following relapse after surgery. Ten months after re-exposition to IPI/NIVO tumor assessment showed a CR again (re-exposure PFS 10.6 months).
Discussion
In this multicenter analysis, later-line combined ICI showed a meaningful response rate and durable responses in patients with avelumab-refractory MCC. For these patients, data on subsequent systemic therapies have so far been reported in rather heterogenous and small patient cohorts. LoPiccolo et al reported a heterogenous case series with in total 13 patients of which only 2 patients received palliative avelumab monotherapy and subsequent combined ICI with IPI/NIVO.8 While one patient was primary resistant to avelumab, the other patient showed an initial PR. Both patients did not respond to subsequent IPI/NIVO. Shalhout et al recently published a retrospective study of 13 patients with anti-PD-L1 or -PD-1-refractory MCC receiving subsequent IPI/NIVO.9 In their analysis, 9/13 (69%) received PD-1 blockade with either pembrolizumab or nivolumab and only 4/13 (31%) PD-L1 blockade with avelumab as first-line therapy. Fifty-four percent were primary refractory to their first-line treatment and no patient responded to subsequent IPI/NIVO in terms of a CR or PR. Median PFS was 1.3 months and mOS was 4.7 months. These findings indicate that prior PD-L1 vs PD-1 blockade as well as primary versus acquired resistance to PD-L1/PD-1 blockade might influence outcome of later-line IPI/NIVO. Our extended analysis still shows a high ORR of 50% to subsequent IPI/NIVO in patients being primary resistant to avelumab while Shalhout et al reported an ORR of 0% (no CR or PR).9 Apart, survival outcome in our analysis fundamentally differs with median OS not being reached after 36 months. For first-line avelumab, the JAVELIN Merkel 200 trial resulted in a median OS of 20.3 months in the total cohort.10 Survival data for the subgroup with PD (41.1%), indicating primary resistance to first-line avelumab, have not been published so far and is NA for indirect comparison.10 Similarly, the recently published real-world data analysis on avelumab in metastatic MCC does not provide accurate conclusions on OS of the subgroup with primary resistance to avelumab.11 When comparing our data to those by Shalhout et al, primary (not acquired) resistance to PD-L1 (not PD-1) blockade seems to be the crucial factor for response to subsequent CTLA-4- and PD-1-blockade in our cohort, possibly explaining the huge differences in ORR and OS. Since activity of combined IPI/NIVO has also been observed in patients with PD-1-refractory advanced melanoma,12 our data now suggest that IPI/NIVO is a rational option for second-line or later-line systemic treatment in those cutaneous malignancies causing the majority skin cancer related deaths. However, the just published randomized, open-label, phase 2 trial on first-line IPI/NIVO±stereotactic body radiation with an impressive ORR of 100% in ICI-naïve patients now gives justified reason to possibly even prefer IPI/NIVO as first-line therapy over PD-L1 or PD-1 monotherapy.13
Clinical characteristics and other biomarkers might predict response to immunotherapies. MCC shows a particular biology with MCPyV being integrated into ~70% of the tumor genomes, while the remaining 30% presumably are linked to UV irradiation showing a strikingly high tumor mutational burden (TMB).14–16 Both factors provide a promising rationale for response to ICI.4 17 In our cohort, MCPyV status was analyzed in 10 patients with response to subsequent IPI/NIVO in 62.5% (5/8) of the MCPyV positive and 50% (1/2) of the MCPyV negative tumors. These results are congruent to the so far published data showing response to first-line pembrolizumab, second-line avelumab or neoadjuvant nivolumab in both, patients with MCPyV-positive and MCPyV-negative MCC.18–20 Thus, negative MCPyV status does not seem to be associated with resistance to ICI. Although a high TMB is known as a marker for response to ICI in other entities,17 only a weak association with PFS and OS could be shown for second-line avelumab in metastatic MCC.19 Hence, the significance of this surrogate marker in MCC remains unclear and therefore was not analyzed in our cohort. Taken together, the presence of MCPyV and high TMB indicate immunogenicity of this entity rather than providing a predictive value for clinical decision making or predicting response to ICI.
The JAVELIN Merkel 200 trial revealed better response and survival data in the subgroup with positive PD-L1 status for patients with previously treated metastatic MCC receiving subsequent avelumab (mOS 12.9 vs 7.3 months) and for patients receiving first-line avelumab (ORR 61.9% vs 33.3%, mOS not reached vs 15.9 months).10 21 Unfortunately, PD-L1 status could be evaluated in only 50% (7/14) of our patients. All analyzed tumors were negative for PD-L1 which could be a possible surrogate marker associated with primary resistance to PD-L1 monotherapy in these patients.10 However, there are also data showing that PD-L1 expression by tumor cells is not associated with response to both PD-1 or PD-L1 blockade in MCC patients.22 The data from Spassova et al also show a better probability of disease control to PD-1 blockade compared with PD-L1 blockade which could in part explain response to IPI/NIVO in PD-L1 resistant patients. Despite these controversial data and on the basis of our results as well as the data from the JAVELIN Merkel 200 trial, we hypothesize that patients with metastatic MCC with negative PD-L1 status could be more likely to benefit from dual agent CTLA-4- and PD-1 targeting ICI similar to data from the Checkmate-067 trial in patients with metastatic melanoma.23 24 To validate this hypothesis which at the moment is based on few and heterogenous data, a prospective clinical trial with PD-L1 status as stratification criterium is needed.
IPI/NIVO is known for a high rate of severe irAE.23 In our cohort, 57% of patients experienced an irAE of any grade while only 29% showed a severe irAE. Moreover, only 3 (21.4%, 3/14) patients did not receive all 4 cycles of IPI/NIVO due to an irAE. In this context, it must be noted that 3 (21.4%, 3/14) patients did not receive all 4 cycles of IPI/NIVO due to rapid tumor progression. In these patients, no irAE were documented which might bias our data. Still the rate of severe irAE is rather low in our cohort indicating a surprisingly good tolerability in these elderly patients. Since the toxicity of combined ICI seems to depend on the dosing of IPI,25 the dosing with IPI 1 mg/kg and NIVO 3 mg/kg (dosing chosen according to the ongoing CheckMate-358 study) in 4 patients might, at least in part, explain the rather low percentage of high grade AE in our cohort.
Our study has several limitations. The main limitations are the small number of patients as well as the registry-based data collection. In addition, adverse events might be under-reported in this registry which could be an additional explanation for the rather low rate of severe irAE in this cohort.
In conclusion, this multicenter ADOREG analysis showed promising OS and ORR to later-line combined ICI with IPI/NIVO in patients with advanced or metastatic MCC with primary resistance to first-line avelumab. To further investigate the efficacy of IPI/NIVO in avelumab-refractory patients as well as to identify biomarkers of response prospective, randomized clinical trials are needed.
Data availability statement
Data are available upon reasonable request. Data will be provided by the corresponding author upon request for reasonable academic studies.
Ethics statements
Patient consent for publication
Ethics approval
Patients were enrolled into ADOREG after written informed consent after approval by central (University Hospital Essen, 14–5921-BO) and local ethics committees. The study was conducted according to the Declaration of Helsinki.
Acknowledgments
Valerie Glutsch and Patrick Schummer are supported by TWINSIGHT, a fellowship program of the University Hospital Würzburg funded by the Else Kröner-Fresenius Foundation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors VG: conceptualisation, methodology, validation, formal analysis, investigation, resources, writing – review and editing, data curation, writing – original draft, visualization. PS: validation, formal analysis, investigation, resources, writing – review and editing, visualization. HK, AG, MG, CP, CG, SH, LZ, JCB, UL, MW and DS: validation, investigation, resources, writing – review and editing. DK: validation, investigation, resources, data curation, writing – review and editing. SU: validation, investigation, resources, writing – review and editing, project administration. BS: conceptualisation, methodology, validation, formal analysis, investigation, resources, writing – review and editing, data curation, writing – original draft, supervision, project administration.
Funding This publication was supported by the Open Access Publication Fund of the University of Wuerzburg
Competing interests VG has received honoraria from Bristol-Myers Squibb and reports travel support from Novartis, Pierre Fabre Pharmaceuticals, Bristol-Myers Squibb, Merck Sharp & Dohme, Sanofi Genzyme and SUN Pharmaceuticals Industries, outside the submitted work. PS has received honoraria from Bristol-Myers Squibb, an institutional research grant from Novartis, reports travel support from Bristol-Myers Squibb, Lilly, Sanofi-Aventis, Novartis, Pierre Fabre Pharmaceuticals and Sun Pharmaceuticals. HK declares no conflicts of interest. AG speaker's honoraria from Allmiral, Bristol-Myers Squibb, MSD Sharp & Dohme and Roche; intermittent advisory board relationships with Amgen, Bristol-Myers Squibb, Novartis, MSD Sharp & Dohme, Pierre Fabre Pharmaceuticals, Pfizer, Roche and Sanofi Genzyme; travel and congress fee support from Bristol-Myers Squibb, MSD Sharp & Dohme, Novartis, Pierre Fabre Pharmaceuticals and Roche. Clinical studies: Amgen, Array, Bristol-Myers Squibb, GSK, Novartis, Merck, MSD Sharp & Dohme, Pfizer and Roche. MG has received speaker’s and advisory board honoraria from Argenx, Biotest, GSK, Janssen, Leo Pharma, Lilly, Novartis and UCB outside the submitted work. DK declares no conflicts of interest. CP received honoraria and travel support from BMS, MSD, Pierre-Fabre, Sanofi, MERCK, SunPharma, Pelpharma, Almirall, and Novartis outside the submitted work. CG is on the advisory board or has received honoraria from Almirall, Amgen, Beiersdorf, BioNTech, Bristol-Myers Squibb, Immunocore, Janssen, MSD Sharp & Dohme, Novartis, Pierre-Fabre Pharma, Roche, Sanofi Genzyme, SUN Pharma and Sysmex Inostics, research funding from Novartis and Sanofi Genzyme, and travel support from Bristol-Myers Squibb, Pierre Fabre Pharma and SUN Pharma, outside the submitted work; he is co-founder of Dermagnostix and Dermagnostix R&D and holds leadership roles for DeCOG, Hiege-Stiftung and Roggenbuck Stiftung. SH has received speaker and advisory board honoraria from Bristol-Myers Squibb and MSD Sharp & Dohme. LZ served as consultant and/or has received honoraria from Bristol-Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre-Fabre, Sunpharma and Sanofi; Research funding to institution: Novartis; travel support from Merck Sharp & Dohme, Bristol-Myers Squibb, Amgen, Pierre-Fabre, Sunpharma, Sanofi and Novartis, outside the submitted work. JCB is receiving speaker’s bureau honoraria from Amgen, Pfizer, Recordati and Sanofi, is a paid consultant/advisory board member/DSMB member for Almirall, Boehringer Ingelheim, InProTher, ICON, MerckSerono, Pfizer, 4SC, and Sanofi/Regeneron. His group receives research grants from Bristol-Myers Squibb, Merck Serono, HTG, IQVIA, and Alcedis. UL is receiving speaker’s honoraria from Sanofi, Sun Pharma, is a paid advisory board member Almirall, Sanofi/Regeneron, Sun Pharma, MSD, Novartis and Roche and gets travel support from Sun Pharma and Sanofi. Her group receives research grants from MSD outside the submitted work. MW declares research support from BMS and MSD; speaker and/or advisory board honoraria from BMS, MSD, Merck Serono, Medac, Novartis, Pierre Fabre, Roche, Sanofi, Sun Pharma and Takeda. DS reports grants (or contracts) from (with) Amgen, Array/Pfizer, Bristol-Myers Squibb, MSD, Novartis and Roche; consulting fees from 4SC, Amgen, Array Biopharma, AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo, Haystick, Immunocore, InFlarX, Innocent, LabCorp, Merck Serono, MSD, Nektar, NeraCare, Novartis, OncoSec, Pfizer, Philogen, Pierre Fabre, Replimune, Roche, Sandoz, Sanofi/Regeneron, Sun Pharma; honoraria from Bristol-Myers Squibb, MSD/Merck, Merck Serono, Novartis, Roche, Sanofi and Sun Pharma; support for attendings meetings or travel support from Bristol-Myers Squibb, MSD, Merck Serono, Novartis, Pierre Fabre and Sanofi; participation on drug safety monitoring or advisory boards for 4SC, Amgen, Array Biopharma, AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo, Immunocore, InFlarX, Merck Serono, MSD, Nektar, NeraCare, Novartis, OncoSec, Pfizer, Philogen, Pierre Fabre, Replimune, Roche, Sandoz, Sanofi/Regeneron and SunPharma; leadership roles for DeCOG, German Cancer Society, Hiege-Stiftung, Deutsche Hautkrebsstiftung, NVKH e.V. and EuMelaReg. SU declares research support from Bristol Myers Squibb and Merck Serono; speakers and advisory board honoraria from Bristol Myers Squibb, Merck Sharp & Dohme, Merck Serono, Novartis and Roche, and travel support from Bristol Myers Squibb, Merck Sharp & Dohme, and Pierre Fabre. BS is on the advisory board or has received honoraria from Immunocore, Almirall, Pfizer, Sanofi, Novartis, Roche, BMS and MSD, research funding from Novartis and Pierre Fabre Pharmaceuticals, and travel support from Novartis, Roche, Bristol-Myers Squibb and Pierre Fabre Pharma, outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.