Article Text

Abstract
Non-melanoma skin cancer (NMSC) includes a wide range of cutaneous tumors, the most frequent of which are basal cell carcinoma (BCC) and cutaneous squamous cell carcinoma (CSCC). Although NMSC is usually cured by surgical resection, in rare cases it can progress to locally advanced and metastatic disease. Risk factors for advanced disease include comorbidities, neglect, and immunosuppression. Advanced NMSC may require systemic treatment if surgery and radiation are not feasible. Chemotherapy, epidermal growth factor receptor (EGFR) inhibitors in CSCC, and hedgehog inhibitors in BCC have been used but are generally of limited benefit, with responses often short-lived and toxicity issues. Given the high mutational burden of NMSC, the use of immunotherapy has been investigated and two anti-PD-1 antibodies, cemiplimab and pembrolizumab, are approved for the treatment of advanced CSCC not curable by surgery or radiation. Both have shown durable responses with good tolerability in patients in phase II trials and anti-PD-1 therapy is now the standard of care for locally advanced and metastatic CSCC. PD-1 blockade is also approved as second-line therapy in advanced BCC, with frequent and durable responses after failure on hedgehog inhibitor therapy. PD-1 checkpoint inhibition is being assessed for NMSC in combination with other modalities, including oncolytic viruses and EGFR inhibitors. Adjuvant and neoadjuvant use of cemiplimab and pembrolizumab is also being investigated with several ongoing trials. Further clinical trials of immunotherapy must be prioritized in NMSC for further improvement in outcomes.
- Immunotherapy
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Non-melanoma skin cancer (NMSC) includes a wide range of cutaneous tumors, the most frequent of which are basal cell carcinoma (BCC), a non-melanocytic cancer arising from basal cells, and cutaneous squamous cell carcinoma (CSCC), which develops through malignant proliferation of epidermal keratinocytes. BCC accounts for around 70% of all NMSCs, with CSCC accounting for 20% and the remaining 10%, a variety of rare tumors such as dermatofibrosarcoma protuberans, primary cutaneous B cell lymphoma, Kaposi sarcoma, carcinosarcoma and Merkel cell carcinoma. BCC and CSCC are the most frequently occurring cancers in Caucasians and their incidence and prevalence is increasing, due largely to the aging of populations and lifestyle changes resulting in increased exposure to ultraviolet (UV) radiation. In data from the International Agency for Research on Cancer GLOBOCAN 2020 database, the number of new cases of NMSC (excluding BCC) was estimated at 1,198,073 patients, accounting for 6.2% of all cancers, with 63 731 deaths (including BCC).1 However, NMSC is typically excluded from standardized reporting of cancer and so estimates of its incidence and prevalence are typically based on smaller subcohorts of various populations. For example, in Germany, analysis of insurance claims database indicated a prevalence of NMSC of 0.65% and incidence of 0.15%, which translates to 376,004 persons across the whole population with an incidence of 84,618 patients annually.2 In Italy, the AIRTUM 2019 report estimated 19,000 new cases of CSCC in 2018, with an overall estimated incidence of about 0.19% and a higher incidence in northern vs southern Italy.3
NMSC with low risk for further disease-associated damage accounts for around 95% of patients and is usually managed by curettage and electrodesiccation, for patients with well differentiated tumors in low-risk locations, or standard surgery.4 Surgical excision alone results in successful treatment of most NMSCs, with cure rates of over 90%.5 Mohs or micrographic-controlled surgery yields higher clearance rates and smaller wounds than standard excision and may be the preferred option, especially for high-risk complex lesions of the head and neck.6 Radiation therapy represents an alternative to surgery for small tumors in low-risk areas in elderly patients, as a primary treatment for inoperable tumors, that is, those lesions where a radical surgical excision is not possible, or if surgery is unacceptable to the patient. Radiation may also be used in the adjuvant setting for tumors excised with positive margins or with extensive perineural or nerve involvement. Treatment approaches which include radiation oncology are usually based on decisions made in multidisciplinary tumor boards.
Although NMSC is usually cured by surgical resection, in rare cases it can progress. In CSCC, the risks of local recurrence, nodal metastasis, and death have been estimated as 3.0%, 4.0%, and 1.5%, respectively.7 In cases of BCC, it has been estimated that up to 10% are advanced, although metastatic disease is less frequent than with CSCC, accounting for <0.5%.8 Despite the low proportion of patients with advanced NMSC, the frequency of the disease means the overall incidence is still substantial. Advanced NMSC includes two different groups of patients with different features and response criteria. Locally advanced disease typically includes a single very large tumor or multiple primary tumors that are not amenable to either surgery or radiotherapy with a reasonable curative intent, while metastatic disease involves locoregional or distant metastases. Risk factors for advanced disease include comorbidities, neglect, and immunosuppression. Guidelines also indicate tumor clinical diameter, high-risk location, vertical histological thickness (>6 mm), poor grade differentiation, desmoplasia, histological perineural invasion and histological margin status as risk factors for progression.9
There is currently no single universally adopted staging system for NMSC. The most widely used staging system for CSCC is that of the American Joint Committee on Cancer (AJCC) but alternatives developed by Brigham and Women’s Hospital (BWH) and the US National Comprehensive Cancer Network are also used.10–12 The AJCC seventh edition (AJCC 7) was the first in which CSCC was given its own category (BCC is rarely staged due to low risk of recurrence or metastases); however, a major limitation is that most poor outcomes occur in T2 patients, with T3 and T4 reserved for bone invasion. An alternative to AJCC 7, the BWH staging system, subdivided T2 tumors into low-risk T2a and high-risk T2b and showed improved homogeneity and monotonicity over AJCC staging.11 13 The AJCC eighth Edition (AJCC 8) includes an updated CSCC tumor classification only for patients with head and neck lesions. An analysis of head and neck CSCC tumors showed that AJCC eight was superior to AJCC seven with a higher proportion of poor outcomes in T3 and T4 disease categories.7 However, another study reported that AJCC 8 T2 and T3 cases were indistinguishable in terms of outcomes and that use of BWH tumor classification may minimize upstaging.14 The continued lack of an accurate CSCC staging system means the identification of tumors with significant risk of recurrence, metastases or death is an ongoing problem, that requires the involvement of multidisciplinary tumor boards. However, key factors in defining patients as high-risk should include Breslow thickness, a lesion larger than 2 cm, neuronal invasion and desmoplastic-like features, and immunosuppression.
Although surgery may be considered in some cases of locally advanced CSCC with no lymph node involvement, systemic treatment is usually required. However, the use of systemic therapies for advanced disease has generally been disappointing. Chemotherapy has been used, especially cisplatin and carboplatin-based regimens, although is precluded in many patients with pre-existing comorbidities due to toxicity. Moreover, responses are mostly short-lived and do not lead to a curative effect.15–17 Epidermal growth factor receptor (EGFR) inhibitors, in particular cetuximab which is approved for the treatment of head and neck squamous cell carcinoma although not CSCC, have also been used. However, despite some promise, this approach has been generally disappointing in patients with advanced disease.9 16 17 In particular, skin-related adverse events predominantly affecting the face can have a major impact on patients’ quality of life. Similarly, although the hedgehog pathway inhibitors, vismodegib and sonidegib, are approved for the treatment of locally advanced or metastatic BCC, adverse events and treatment discontinuations is a frequent concern and treatment resistance often occurs over time.
Chronic UV radiation exposure is the most important risk factor for NMSC. Both CSCC and BCC are associated with a UV mutation signature, and a high tumor mutational burden (TMB), with some of the highest rates of somatic mutations among solid tumors. Mutated proteins can act as neoantigens which are recognized by the immune system and a high TMB has been associated with increased response rates to immunotherapy.18 Immunosuppression is another well-recognized risk factor for NMSC, with the immunosuppressed including recipients of solid organ transplant and those with HIV infection or chronic lymphocytic leukemia, suggesting the importance of the immune response.19 These provide a strong rationale for the investigation of programmed death (PD)−1 immune checkpoint blockade in NMSC.
Treatment of advanced CSCC with PD-1 inhibitors
The efficacy of anti-PD-1/PD-ligand (L)1 antibodies in melanoma and other solid tumors is well established. Two anti-PD-1 antibodies have also been approved for the treatment of advanced CSCC, cemiplimab and pembrolizumab.
Pembrolizumab was initially approved in the USA for recurrent or metastatic CSCC not curable by surgery or radiation, with this indication later expanded to include locally advanced CSCC. Pembrolizumab is not yet approved for CSCC in Europe. Approval of pembrolizumab was based on the open-label, non-randomized, phase II KEYNOTE-629 trial, in which 159 patients with locally advanced or recurrent/metastatic CSCC received pembrolizumab 200 mg every 3 weeks for up to 35 cycles.20 In the recurrent/metastatic cohort of 105 patients, 87% of whom had received≥1 prior systemic therapy for recurrent/metastatic CSCC, objective response rate (ORR) was 35.2% (95% CI 26.2%–45.2%), including 10.5% of patients with a complete response and 24.8% with a partial response. In the locally advanced cohort of 54 patients, of whom 22% had received prior systemic therapy for curative intent, ORR was 50.0% (95% CI 36.1 to 63.9), including 16.7% of patients with a complete response and 33.3% with a partial response. Median duration of response was not reached in either cohort. In the locally advanced cohort, of the 27 responders with a confirmed response, 77.8% had ongoing responses as of the data cut-off date; 88% had responses that lasted ≥6 months and 84.1% had responses that lasted ≥12 months. The safety profile was similar to that seen with pembrolizumab monotherapy in melanoma and non-small-cell lung cancer. Grade 3–5 treatment-related adverse events occurred in 11.9% of patients. Laboratory abnormalities occurring at a higher rate included lymphopenia (10%) and decreased sodium (10%).
Pembrolizumab was also assessed in the open-label phase II CARSKIN study, which enrolled 57 treatment-naïve patients in primary and expansion cohorts.21 Across both cohorts, ORR after 15 weeks was 42% (95% CI 29% to 56%), with 35% partial and 7% complete responses. In the expansion cohort, the ORR was higher among patients with PD-L1-positive disease than those with PD-L1-negative disease (55% vs 17%; p=0.02). At a median follow-up of 22.4 months, median progression-free survival (PFS) was 6.7 months and median overall survival (OS) was 25.3 months in the primary cohort.
Cemiplimab is a fully human immunoglobulin G4 anti-PD-1 antibody that is approved for the treatment of metastatic CSCC or locally advanced CSCC not amenable to curative surgery or curative radiation in both Europe and the USA. Promising clinical activity was shown in a phase I study of 26 patients with locally advanced or metastatic CSCC, with an ORR of 50%.22 In the metastatic-disease cohort of a phase 2 study, a response was observed in 28 of 59 patients (47%; 95% CI 34% to 61%) with a median follow-up of 7.9 months. In the cohort of 78 patients with locally advanced CSCC in this phase 2 trial, ORR was 34%, with 13% patients with a complete response and 31% with a partial response.23 In a biomarker evaluation of this cohort, responses to cemiplimab were observed irrespective of either baseline PD-L1 tumor proportion score or median TMB, suggesting neither are of utility in predicting clinical benefit. Other candidate biomarkers that might better predict treatment response to cemiplimab are required.
The efficacy and safety of cemiplimab were further investigated in the phase II, non-randomized, open-label EMPOWER-CSCC 1 clinical trial.24 In this study, 193 patients with advanced CSCC who were not suitable for curative surgery or radiation were treated with either cemiplimab 3 mg/kg every 2 weeks (group 1 with metastatic disease and group 2 with locally advanced disease) or a fixed dose of 350 mg every 3 weeks (group 3, metastatic CSCC). The primary endpoint was ORR according to independent central review as per Response Evaluation Criteria in Solid Tumors (RECIST) V.1.1. At a median duration of follow-up of 15.7 months, ORR in all patients was 46.1% (95% CI 38.9% to 53.4%) with a complete response rate of 16.1%. Disease control rate was 72.5% (95% CI 67.5% to 78.7%). Median observed time to response was 2.1 months (95% CI 1.7 to 3.7). In group 3, which represents the subsequently approved dosing regimen of cemiplimab 350 mg every 3 weeks, ORR was 41.1% with a disease control rate of 57.1%. Among all patients with an objective response, 87.8% (95% CI 78.5% to 93.3%) had ongoing responses at 12 months from first response, with median duration of response not reached. Estimated median PFS was 18.4 months (95% CI 10.3 to 24.3) for all patients and estimated 2-year PFS rate was 44.2% (95% CI 36.1% to 52.1%) (figure 1). Median OS was not reached and estimated 2-year OS rate was 73.3% (95% CI 66.1% to 79.2%). Treatment was well tolerated with a safety profile that appears to be consistent with that of other anti-PD-1/PD-L1 agents and no new safety signals. The most frequent adverse events were fatigue and diarrhea. Overall, 9% of patients had grade ≥3 immune-related adverse events, with a low treatment discontinuation rate of 10%.

PFS and OS in patients with locally advanced or metastatic CSCC treated with cemiplimab. CSCC, cutaneous squamous cell carcinoma; OS, overall survival; PFS, progression-free survival.
In another phase II trial which included 63 patients with metastatic (n=39) and locally advanced (n=24) CSCC, an extended-dose regimen of cemiplimab 600 mg every 4 weeks for up to 48 weeks was investigated.25 At a median follow-up of 9.2 months, the ORR was 58.7% (95% CI 45.6% to 71.0%), and the rate of complete responses was 17.5%. Although the median duration of response had not been reached, the estimate of ongoing response at 12 months was 89.4% (95% CI 70.0% to 96.6%). Durable disease control rate was 76.2% (95% CI 63.8% to 86.0%). The most frequent treatment-emergent adverse events were diarrhea (23.8%), pruritus (23.8%), and fatigue (22.2%). Grade ≥3 immune-related adverse events occurred in eight (12.7%) patients. This extended dosing regimen appears feasible given comparable efficacy and safety with the approved every 3 weeks regimen and may offer greater flexibility and convenience for some patients.
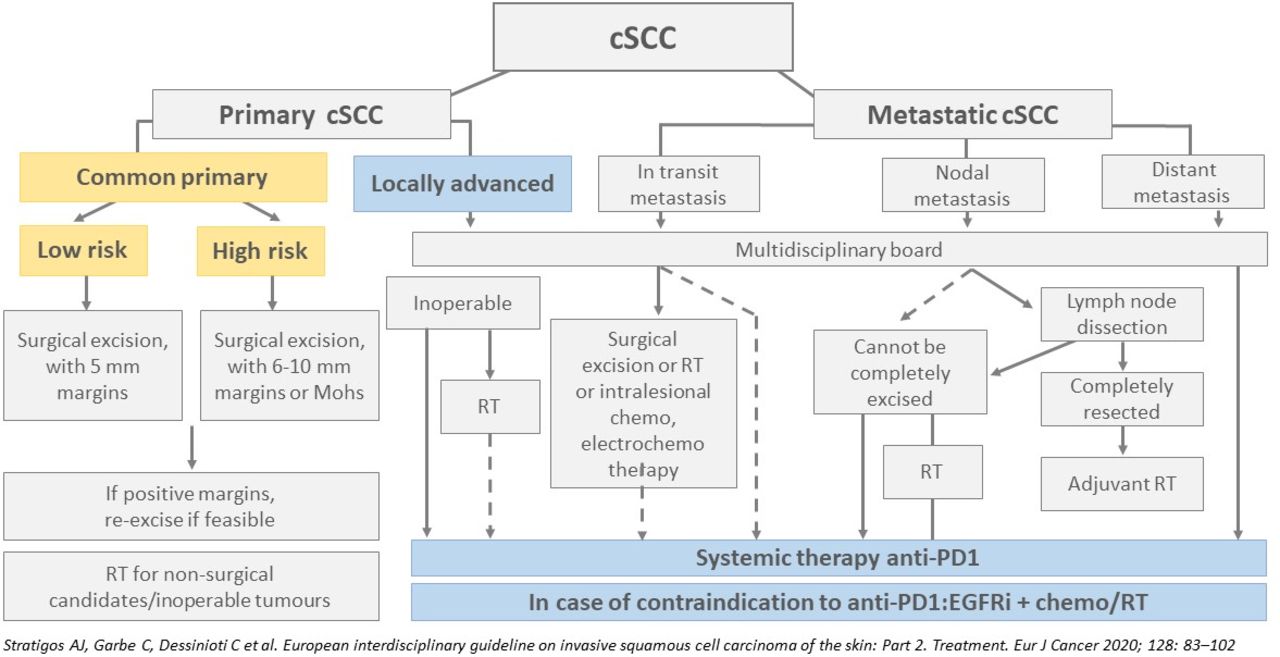
Real-world studies of use of cemiplimab in advanced CSCC suggest responses are similar to those observed in clinical trials and that treatment is tolerable and appears feasible, even in elderly patients with severe comorbidities.26 27 Currently, immune checkpoint inhibitors are the first-line standard of care and only approved therapy for CSCC, in both locally advanced and metastatic CSCC. As yet,there is no standard salvage therapy in CSCC (figure 2).

European guideline recommendations for the management of high-risk and advanced CSCC. European guidelines developed by a multidisciplinary panel of experts from the European Dermatology Forum, the European Association of Dermato-Oncology and the European Organization of Research and Treatment of Cancer. Recommendations were based on evidence-based literature review, guidelines and expert consensus.9 CSCC, cutaneous squamous cell carcinoma; RT, radiotherapy.
Treatment of advanced BCC with PD-1 inhibitors
Advanced BCC is rare but very difficult to treat. BCC can progress to locally advanced or to metastatic disease in less than 1% of patients, which has a very poor prognosis with a median survival of 8–14 months and a 5-year survival rate of 10%.
The hedgehog signaling pathway is activated in many cancers, including BCC. Patched homologue 1 (PTCH1) inhibits the hedgehog signaling pathway by binding to G protein-coupled receptor-like protein smoothened (SMO), which is a pathway activator. Over 90% of all BCCs have a deletion mutation in PTCH 1 or activating mutation in (SMO), which lead to upregulation of the Hedgehog pathway and development of BCC.28 The hedgehog pathway inhibitors, vismodegib and sonidegib, are both effective in the treatment of locally advanced or metastatic BCC, with response rates of around 36%–48%.29 30 However, there is a high occurrence of adverse events and treatment discontinuation, mainly due to fatigue, dysgeusia, and muscle cramps is frequent, especially in elderly patients. This can be managed in practice by treatment delay/interruption or dose modification.31 However, resistance also eventually develops in most patients.32
Several case reports of patients with advanced BCC treated with PD-1 inhibitors have been reported, with patients achieving partial or complete responses.33 In the open-label, multicenter, single-arm, phase 2 EMPOWER-BCC 1 trial, 84 patients with locally advanced BCC who had progressed on or were intolerant to previous hedgehog inhibitor therapy were treated with cemiplimab 350 mg every 3 weeks for up to 93 weeks or until progression or unacceptable toxicity.34 Two-thirds of patients were male, 61% had an ECOG performance status of 0, and head or neck was the primary tumor site in 89% of patients. Reasons for discontinuation of previous hedgehog inhibitor therapy were disease progression in 71% and unacceptable toxicity in 38% of patients. At a median duration of follow-up of 15.9 months, ORR per independent central review was 32.1% (95% CI 22.4% to 43.2%) of patients; six patients (7.1%) had a complete response and 21 (25%) had a partial response.35 Median duration of response in 27 responders had not been reached at the time of data cut-off; Kaplan-Meier estimates for duration of response was 91.7% (95% CI 70.6% to 97.8%) at 6 months. Estimated PFS was 16.5 (95% CI 8.6% to 21.8%) months and estimated 1-year PFS rate was 56.7% (95% CI 44.5% to 67.1%). Median OS had not been reached; estimated 1-year OS was 92.2% (95% CI 83.4% to 96.4%). The safety profile was acceptable and consistent with what is known for anti-PD-1 therapy. The most common grade ≥3 treatment-related adverse events were colitis, fatigue, and adrenal insufficiency (2% each). Immune-related adverse events occurred in 22 (26.2%) patients; the most frequent were hypothyroidism in eight (10%) patients and immune-related colitis in five (6%) patients. Grade 3 immune-related adverse events occurring in more than one patient were colitis (n=3) and adrenal insufficiency (n=2); no grade ≥4 immune-related adverse events were reported. There were no treatment-related deaths.
The same trial also enrolled a cohort with metastatic disease. Although these data are not yet fully reported, interim analysis reported that objective responses were observed in 10 (28.6%, 95% CI 14.6% to 46.3%) of 35 patients.35 One patient had a complete response and nine patients had partial responses. Median duration of response was not reached (range 4.3 to 25.1+ months), with 90% of responders maintaining a response for at least 6 months. Estimated PFS was 6.6 months (95% CI 4.2 to 8.3) and estimated 1-year PFS rate was 28.8% (95% CI 14.5% to 44.8%). Median OS had not been reached; estimated 1-year OS was 87.7% (95% CI 70.5% to 95.2%).
Exploratory biomarker analyses of the cohort with locally advanced BCC showed no association between response and baseline PD-L1 status, TMB, or major histocompatibility class 1 (MHC-1) expression. In 50 patients with evaluable PD-L1 expression, the ORR was 26% in those with PD-L1 expression <1% (n=35) compared with 27% in patients with PD-L1 expression of ≥1% (n = 15), indicating a similar proportion of patients with low PD-L1 expression derive clinical benefit from cemiplimab.
Future studies should evaluate anti-PD-1 as first-line therapy before hedgehog inhibitor therapy. A pilot study of vismodegib in combination with or without pembrolizumab in 16 patients with advanced BCC did not suggest additive clinical activity, with an ORR at 18 weeks of 44% in the pembrolizumab monotherapy arm and 29% in the combined therapy arm (figure 3).36

{kind=link}
{kind=link}
{kind=link}
ORR, PFS and OS in patients with BCC treated with pembrolizumab with or without vismodegib. BCC, basal cell carcinoma; ORR, objective response rate; OS, overall survival; PFS, progression-free survival.
Treatment of immunosuppressed patients
Immunosuppression is a known risk factor for NMSC and immunosuppressed patients (eg, solid-organ transplant recipients, patients with chronic lymphocytic leukemia, patients with HIV) represent a substantial proportion of patients with NMSC and tend to have more aggressive disease. Due to their immunosuppressed nature, immunotherapy may be more challenging in these patients who have a higher risk of developing immune-related toxicities. Among solid organ transplant recipients, PD-1 blockade can cause allograft rejection through activation of the immune system. Despite this, several case reports have suggested that checkpoint inhibition for CSCC can be used in patients after solid organ transplant, including those receiving prednisone.37–39 A recent pilot study with seven solid organ recipients (kidney, liver, or lung) with metastatic head and neck CSCC reported a tumor response rate of 57.1% (one complete responder and three partial responders) with cemiplimab or pembrolizumab.40 Three patients who received prophylactic prednisone all responded to cemiplimab with preserved allograft function and no adverse events. Calcineurin inhibitor use was minimized and patients switched to mTOR inhibitors if required; steroids were also used. The ongoing phase 1/2 CONTACT trial (NCT04339062) is investigating the safety of checkpoint blockade in patients with metastatic CSCC who have previously received allogeneic hematopoietic stem cell transplant or a kidney transplant.
Future developments
In patients with high-risk CSCC who receive current standard-of-care surgical resection and adjuvant radiotherapy, up to 50% develop local recurrence and regional metastasis, so trials are assessing adjuvant use of cemiplimab and pembrolizumab. A randomized, placebo-controlled, multicenter phase III study will evaluate cemiplimab as an adjuvant treatment in 412 patients with high-risk CSCC (any one of nodal disease with extracapsular extension, in-transit metastases, T4 lesion, perineural invasion, or recurrent CSCC with at least one other risk factor) who have completed surgery and postoperative radiotherapy (NCT03969004).41 Similarly, adjuvant pembrolizumab after surgical resection and radiotherapy is being investigated in the phase III KEYNOTE-630 trial in patients with locally advanced CSCC with ≥1 high-risk feature at the primary site of malignancy, (NCT03833167).42 Cemiplimab has also been investigated in a neoadjuvant setting. In a pilot study, 20 patients with newly diagnosed or recurrent stage III-IVA CSCC of the head and neck who were amenable to surgery with curative intent received two cycles of neoadjuvant cemiplimab.43 Although only six patients had partial responses by RECIST, 14 patients (70%; 95% CI 45.7% to 88.1%) had a pathological complete response (n=11) or major pathological response (n=3). At a median follow-up of 22.6 months, one patient progressed and died, one died without disease, and two had recurrent disease; 1-year disease-free survival was 90% and 1-year OS was 95%. Of note, 55% of patients did not receive the planned adjuvant radiation based on pathological responses achieved. Treatment was well tolerated, with no serious adverse events occurring during or after neoadjuvant treatment. A multicenter phase II study is planned based on these preliminary results.
Another planned trial is the NeoCESQ study which will enroll 25 patients with confirmed stage III CSCC (NCT04632433). Patients will be treated with two cycles of neoadjuvant cemiplimab before surgery, followed by 1 year of adjuvant cemiplimab every 3 weeks. Stage III disease must be documented at screening and reassessed prior to surgery by CT or positron emission tomography scan.
Immune checkpoint inhibition is also being investigated in combination with other treatments. In the CERPASS trial, the safety and efficacy of cemiplimab in combination with RP1, an intratumorally injected oncolytic virus (HSV-1) that expresses a fusogenic glycoprotein (GALV-GP R-) and granulocyte macrophage colony-stimulating factor is being assessed vs cemiplimab alone in approximately 180 patients with metastatic or unresectable, locally advanced CSCC who are not candidates for/refuse surgery or radiotherapy.44 In a preliminary study, RP1 combined with nivolumab resulted in high response rates, including complete response, in patients with CSCC.45 Another therapeutic strategy, intended to increase the response rate of immunotherapy and to overcome mechanisms of resistance to progression, is the addition of an anti-EGFR agent. In the I-TACKLE trial (NCT03666325), patients are treated with pembrolizumab for 9 weeks with cetuximab being added to treatment for those patients without a response. Patients with a complete or partial response at 9 weeks continue on pembrolizumab alone, with clinical and radiological evaluation every 6 weeks and the addition of cetuximab if secondary resistance develops. In another trial, the PD-L1 inhibitor avelumab is being assessed with and without cetuximab, with PFS the primary endpoint (NCT03944941),
In patients with BCC, nivolumab alone or in combination with the CTLA-4 checkpoint inhibitor ipilimumab is being investigated in a phase 2 trial of patients with locally advanced unresectable or metastatic disease46 (NCT03521830). In cohort A of this trial, patients will receive nivolumab 480 mg every 4 weeks for up to 48 weeks alone, as either first-line therapy or second-line to hedgehog inhibitor therapy. In cohort B, patients with progressive BCC after anti-PD-1 therapy with or without a hedgehog inhibitor will receive nivolumab 240 mg plus ipilimumab 1 mg/kg every 3 weeks for 12 weeks followed by seven doses of single-agent nivolumab 480 mg every 4 weeks. Patients with BCC, as well as CSCC, are also included in the SWOG 1609 (DART) basket trial of rare cancers that is investigating nivolumab and ipilimumab47 (NCT02834013).
Hedgehog inhibitors increase CD8+T cell infiltration, indicating a potential synergistic effect in combination with immunotherapy. As such, the hedgehog inhibitor sonidegib is being assessed in combination with cemiplimab in 20 patients with advanced BCC48 (NCT04679480). After a lead-in phase with sonidegib, patients will receive cemiplimab combined with pulsed dosing of sonidegib (2 weeks on, 2 weeks off). Primary endpoint is best response at any time between treatment start and 26 weeks after the initiation of the treatment.
Talimogene laherperepvec (T-VEC) is an injectable modified oncolytic herpes virus approved for the treatment of melanoma that is being investigated alone or in combination with nivolumab in a phase 2 trial including cohorts of patients with CSCC and other advanced and/or refractory NMSC49 (NCT029786250). Patients may have received previous PD-1 inhibitor therapy and will initially be treated with T-VEC alone, with nivolumab being added if no objective response is achieved by week 12.
Daromun, which is administered intralesionally, consists of two antibody-cytokine fusions as active principles (L19IL2 and L19TNF), which act synergistically to directly kill tumor cells while also inducing a systemic antitumor immune response. A phase II neoadjuvant trial in patients with locally advanced injectable NMSC (CSCC and BCC) is underway (NCT04362711).50
Conclusions
NMSC is the most frequent tumors in humans and is increasing in prevalence, due to the aging of populations and increased chronic UV exposure, as well as greater disease awareness with earlier diagnosis. The majority of patients have simple lesions and are effectively treated with surgery with or without radiation. However, some patients progress to locally advanced or to metastatic disease, primarily because of immunosuppression, comorbidities, or neglect. Until recently, systemic therapy of advanced disease was largely unsuccessful, with chemotherapy and targeted therapy having limited benefits. NMSC has a high mutational burden with a UV gene signature which likely contributes to immunogenicity of these tumors. Anti-PD-1 with either cemiplimab or pembrolizumab is now the standard of care for locally advanced and metastatic CSCC. Cemiplimab is also the standard salvage approach in patients with BCC, with frequent and durable responses after failure on hedgehog inhibitor therapy. Clinical trials of immunotherapy must be prioritized for further improvement in outcomes. In addition, interdisciplinary tumor board decision-making is of critical importance to allow patients to gain access to those innovative and efficacious treatment options.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Acknowledgments
This activity was supported by an independent medical education unrestricted grant from Sanofi and Regeneron. A special thanks to 3P Solution for their support and cooperation.
References
Footnotes
Twitter @PAscierto
Contributors PAA prepared the manuscript collaboratively with input of DS. All authors read and approved the final manuscript.
Funding This activity was supported by an independent medical education unrestricted grant from Sanofi and Regeneron.
Competing interests PAA: Employment or Leadership Position: None; Consultant/Advisory Role: Bristol-Myers Squibb, Roche-Genentech, Merck Sharp & Dohme, Novartis, Merck Serono, Pierre-Fabre, AstraZeneca, Sun Pharma, Sanofi, Idera, Sandoz, Immunocore, 4SC, Italfarmaco, Nektar, Boehringer-Ingelheim, Eisai, Regeneron, Daiichi Sankyo, Pfizer, OncoSec, Nouscom, Lunaphore, Seagen, iTeos, Medicenna; Stock Ownership: None; Research Funding: Bristol-Myers Squibb, Roche-Genentech, Pfizer, Sanofi; Expert Testimony: None; Other Remuneration: None. DS: Honoraria: Roche/Genentech, Novartis, Bristol-Myers Squibb, Merck Sharp & Dohme, Immunocore, Merck Serono, Array BioPharma, Pfizer, Pierre Fabre, Philogen, Regeneron, 4SC, Sanofi/Regeneron, Neracare, Sun Pharma, InflarxGmbH, Ultimovacs, Sandoz, Amgen, Daiichi Sankyo Japan, LabCorp, Nektar, Replimune; Consulting or Advisory Role: Roche/Genentech, Novartis, Bristol-Myers Squibb, Merck Sharp & Dohme, Merck Serono, 4SC, Pierre Fabre, Sanofi/Regeneron, Nektar; Speakers’ Bureau: Bristol-Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre Fabre, Sanofi/Regeneron, Merck KGaA; Research Funding: Bristol-Myers Squibb, Novartis, Roche, MSD Oncology, Array/Pfizer, Amgen; Travel, Accomodation, Expenses: Roche/Genentech, Bristol-Myers Squibb, Merck Serono, Novartis, Merck Sharp & Dohme, Pierre Fabre, Sanofi/Regeneron.
Provenance and peer review Not commissioned; externally peer reviewed.