Article Text

Abstract
Background Patients with advanced renal cell carcinoma with sarcomatoid features (sRCC) have a poor prognosis and limited therapeutic options. First-line nivolumab plus ipilimumab (NIVO+IPI) provided efficacy benefits over sunitinib (SUN) in patients with intermediate/poor-risk sRCC at 42 months minimum follow-up in the phase 3 CheckMate 214 trial. In this exploratory post hoc analysis, we report clinical efficacy of NIVO+IPI in sRCC after a minimum follow-up of 5 years.
Methods In CheckMate 214, patients with clear cell advanced RCC were randomized to NIVO 3 mg/kg plus IPI 1 mg/kg every 3 weeks (four doses), then NIVO 3 mg/kg every 2 weeks versus SUN 50 mg once daily (4 weeks; 6-week cycles). Randomized patients with sRCC were identified via independent central pathology review of archival tumor tissue or histological classification per local pathology report. Overall survival (OS), as well as progression-free survival (PFS) and objective response rate (ORR) per independent radiology review using Response Evaluation Criteria in Solid Tumors V.1.1, were evaluated in all International Metastatic Renal Cell Carcinoma Database Consortium intermediate/poor-risk sRCC patients and by baseline tumor PD-L1 expression level (≥1% vs <1%). Safety outcomes are reported using descriptive statistics.
Results In total, 139 patients with intermediate/poor-risk sRCC were identified (NIVO+IPI, n=74; SUN, n=65). At 5 years minimum follow-up, more patients remained on treatment with NIVO+IPI versus SUN (12% vs zero). Efficacy benefits with NIVO+IPI versus SUN were maintained with median OS of 48.6 vs 14.2 months (HR 0.46), median PFS of 26.5 vs 5.5 months (HR 0.50), and ORR 60.8% vs 23.1%. In addition, median duration of response was longer (not reached vs 25.1 months), and more patients had complete responses (23.0% vs 6.2%) with NIVO+IPI versus SUN, respectively. Efficacy was better with NIVO+IPI versus SUN regardless of tumor PD-L1 expression, but the magnitude of OS, PFS, and ORR benefits with NIVO+IPI was greater for sRCC patients with tumor PD-L1 ≥1%. No new safety signals emerged in either arm with longer follow-up.
Conclusions Among patients with intermediate/poor-risk sRCC, NIVO+IPI maintained long-term survival benefits and demonstrated durable and deep responses over SUN at minimum follow-up of 5 years, supporting NIVO+IPI as a preferred first-line therapy in this population.
Trial registration number NCT02231749.
- Immunotherapy
- Programmed Cell Death 1 Receptor
- CTLA-4 Antigen
- Drug Therapy, Combination
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Bristol Myers Squibb’s policy on data sharing may be found online at https://www.bms.com/researchers-and-partners/independent-research/data-sharing-request-process.html
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Sarcomatoid differentiation is an aggressive histological growth pattern that is detected in 5% of renal cell carcinomas (RCCs), including 15%–20% of advanced disease.1 Patients with sarcomatoid RCC (sRCC) have poor prognosis and a longstanding unmet medical need for safe and effective therapeutic options.2 3 Recently, progress has been made to improve treatment modalities for sRCC with the introduction of immune checkpoint therapy.4 The use of anti-programmed death 1 (PD-1)/programmed death-ligand 1 (PD-L1) agents alone or in combination with anti-vascular endothelial growth factor (VEGF) or anti-cytotoxic T lymphocyte antigen-4 (CTLA-4) agents has led to improved efficacy and survival outcomes in sRCC, reporting objective response rates (ORRs) ranging from 47% to 61% with combination regimens.5–9 Such outcomes are a significant improvement from cytotoxic chemotherapies and molecular targeted agents (eg, VEGF signaling inhibitors, mTOR inhibitors), with historical ORRs ranging from 11% to 26% and very few complete responses (CRs).10 However, there are limited data on long-term outcomes in patients with sRCC treated with immune checkpoint therapy.5–8 11
In the phase 3 CheckMate 214 trial, nivolumab plus ipilimumab (NIVO+IPI) showed substantial long-term survival benefits and antitumor activity over sunitinib (SUN) in patients with sRCC and International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) intermediate/poor (I/P)-risk disease. With minimum follow-up of 42 months, patients treated with NIVO+IPI had an ORR of 60.8% vs 23.1% with SUN; CRs were observed in 18.9% vs 3.1%, respectively.9 On the basis of these results, the Society for Immunotherapy of Cancer recommended NIVO+IPI combination immunotherapy as a first-line treatment option for patients with sRCC.12 Here, we present long-term results in patients with sRCC from CheckMate 214 after minimum follow-up of 5 years.
Methods
CheckMate 214 was a global, multicenter, open-label, randomized phase 3 trial. Study design details were published previously.9 13 Briefly, adults with treatment-naïve advanced RCC (aRCC) with a clear cell component were randomized 1:1 to intravenous NIVO 3 mg/kg and IPI 1 mg/kg every 3 weeks (four doses), followed by NIVO 3 mg/kg every 2 weeks or oral SUN 50 mg once daily (4 weeks on and 2 weeks off; 6-week cycles). Randomized patients were stratified by geographical region and IMDC risk (favorable (0); intermediate (1-2); poor (3-6)). This post hoc, exploratory analysis reports long-term, 5-year minimum follow-up in the subpopulation of patients with IMDC I/P-risk sRCC. Patients with favorable-risk sRCC were not included in this analysis as CheckMate 214 focused primarily on I/P-risk disease and only six favorable-risk sRCC patients were identified within the intention-to-treat population.
This analysis identified aRCC patients with sarcomatoid histology via two distinct methodologies: central pathology review, which allowed for analysis of archived patient tissue samples, and local pathology reports, which reduced the risk of identifying false negatives due to limited tissue availability for central review (online supplemental figure S1). The percent of tumor area with sarcomatoid differentiation was independently assessed by three pathologists blinded to patient outcomes; discrepancies were resolved by consensus review. Sarcomatoid differentiation per independent central review was defined by criteria discussed at the International Society of Urological Pathology 2012 Consensus Conference.14 Randomized patients who demonstrated any percent of sarcomatoid histology by either method were identified as sRCC.
Supplemental material
Outcomes in patients with IMDC I/P-risk sRCC were exploratory, and not prespecified in the trial protocol. Overall survival (OS), as well as progression-free survival (PFS) and ORR by independent radiology review committee using Response Evaluation Criteria in Solid Tumors V.1.1, were evaluated. Outcomes were also assessed according to baseline tumor PD-L1 expression level (≥1% vs <1%) in IMDC I/P-risk sRCC patients. Baseline tumor PD-L1 expression was determined at a central laboratory using the Dako PD-L1 IHC 28-8 pharmDx assay. Safety was assessed in all treated IMDC I/P-risk sRCC patients. Treatment-free interval (TFI) was defined as the time between protocol therapy discontinuation and subsequent therapy initiation or last known date alive. Statistical analysis for this exploratory subgroup follows the overall trial methodology, as described.9 13
Results
Patients
In total, 1096 patients with aRCC were randomized in CheckMate 214 (NIVO+IPI, n=550; SUN, n=546).13 Of the 847 randomized patients with I/P-risk disease (NIVO+IPI, n=425; SUN, n=422), 139 (16.4%) were identified with sarcomatoid histology (74 in the NIVO+IPI arm and 65 in the SUN arm) and included in this analysis. Among all the 139 I/P-risk sRCC patients, 73 (98.6%) out of 74 patients in the NIVO+IPI group and all 65 (100%) in the SUN group received treatment. Baseline demographic and disease characteristics in the subgroup of patients with I/P-risk sRCC were largely similar between treatment arms and in comparison with the general I/P-risk study population in the NIVO+IPI arm (table 1); of note, a higher proportion of I/P-risk sRCC patients in the NIVO+IPI arm had baseline tumor PD-L1 expression ≥1% versus all patients with I/P-risk disease (50.7% vs 26.0%). In addition, a greater proportion of patients with sRCC had lung metastases at baseline and a smaller proportion had liver metastases compared with the general study population with I/P-risk disease.
Select baseline demographic and disease characteristics
At time of the database lock (February 24, 2021), the minimum study follow-up was 5 years for the subpopulation of patients in CheckMate 214 with I/P-risk sRCC (median, 5.6 years). The median duration of therapy (quartile (Q) Q1–Q3) in patients with I/P-risk sRCC was 7.9 (2.1–28.1) months in the NIVO+IPI arm and 4.7 (2.3–8.5) months in the SUN arm. Of all treated patients, 9 of 73 (12%) in the NIVO+IPI arm versus zero of 65 in the SUN arm remained on treatment. The primary reason for discontinuation was disease progression, observed in 27 of 73 (37.0%) treated patients in the NIVO+IPI arm and 46 of 65 (70.8%) in the SUN arm (online supplemental figure S2).
Supplemental material
Efficacy in patients with IMDC I/P-risk sRCC
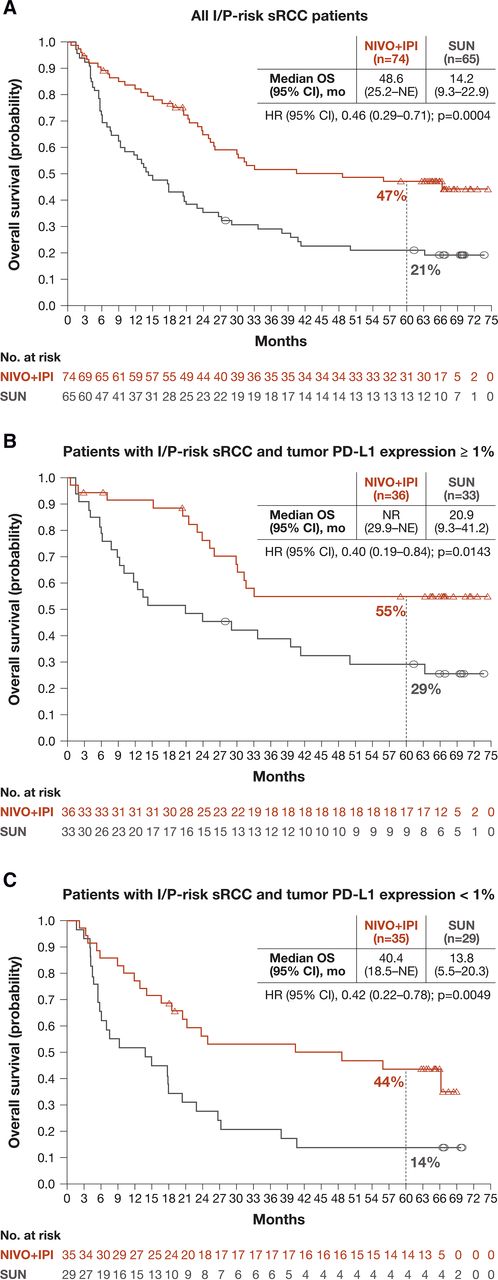
Survival benefit with NIVO+IPI versus SUN was maintained in patients with I/P-risk sRCC with minimum follow-up of 5 years. Median OS (95% CI) was 48.6 (25.2 to not estimable (NE)) months with NIVO+IPI vs 14.2 (9.3 to 22.9) months with SUN; HR for death was 0.46 (95% CI 0.29 to 71; p=0.0004; figure 1A). Median PFS (95% CI) was also longer with NIVO+IPI versus SUN: 26.5 (7.2-NE) months vs 5.5 (4.1 to 6.9) months; HR for disease progression or death was 0.50 (95% CI 0.32 to 0.80; p=0.0036; figure 2A). In addition, patients had higher ORR (95% CI) with NIVO+IPI versus SUN (60.8% (48.8% to 72.0%)) vs 23.1% (95% CI 13.5% to 35.2%); p<0.0001), with more ongoing responses (66.7% vs 40.0%) and CRs (23.0% vs 6.2%), respectively (table 2). Median duration of response (95% CI) was longer with NIVO+IPI versus SUN (not reached (22.5 to NE) months vs 25.1 (7.2 to 60.4) months). The probability of response at 5 years was 63% with NIVO+IPI vs 19% with SUN.

Kaplan-Meier plot of OS in (A) all patients with I/P risk and by tumor PD-L1 expression (B) ≥1% or (C) <1%. Symbols represent censored observations.

{kind=link}
{kind=link}
Kaplan-Meier plot of PFS per independent radiology review committee in (A) all patients with I/P risk and by tumor PD-L1 expression (B) ≥1% or (C) <1%. Symbols represent censored observations. PFS, progression-free survival.
Best overall confirmed response per RECIST V.1.1 in all patients with IMDC I/P-risk sRCC and by tumor PD-L1 expression levels
Outcomes in patients with IMDC I/P-risk sRCC by baseline tumor PD-L1 expression level
NIVO+IPI continued to demonstrate efficacy benefits over SUN, regardless of tumor PD-L1 expression level at this long-term follow-up. In all patients with sRCC and evaluable baseline tumor PD-L1 expression ≥1% (NIVO+IPI, n=36; SUN, n=33), median OS (95% CI) was not reached (29.9 to NE) months with NIVO+IPI vs 20.9 (9.3 to 41.2) months with SUN; HR for death was 0.40 (0.19 to 0.84; p=0.0143; figure 1B). Median OS among patients with sRCC and evaluable baseline tumor PD-L1 expression <1% (NIVO+IPI, n=35; SUN, n=29) was 40.4 (18.5 to NE) months with NIVO+IPI vs 13.8 (5.5 to 20.3) months with SUN; HR for death was 0.42 (0.22 to 0.78; p=0.0049; figure 1C). Median PFS (95% CI) in patients with baseline tumor PD-L1 expression ≥1% with NIVO+IPI versus SUN was not reached (9.1 to NE) months vs 5.6 (2.8 to 6.9) months (figure 2B), and the median PFS among patients with baseline tumor PD-L1 expression <1% was 9.0 (3.3 to 47.0) months with NIVO+IPI vs 5.4 (4.0 to 17.0) months with SUN (figure 2C). Furthermore, the ORR among patients with tumor PD-L1 expression ≥1% was 69.4% with NIVO+IPI vs 24.2% with SUN; of these, 25.0% (9 of 36) vs 9.1% (3 of 33) of patients had CRs, respectively. For patients with baseline tumor PD-L1 expression <1%, the ORR for NIVO+IPI versus SUN was 54.3% vs 20.7%. Of these patients, 22.9% (8 of 35) treated with NIVO+IPI and 3.4% (1 of 29) treated with SUN had CRs (table 2).
Safety
Any-grade treatment-related adverse events (AEs) occurred in 71 of 73 (97.3%) vs 63 of 65 (96.9%) patients treated with NIVO+IPI versus SUN, respectively (online supplemental table S1). Grades 3–4 treatment-related AEs occurred in 36 of 73 (49.3%) vs 29 of 65 (44.6%) patients, respectively. Treatment-related AEs leading to discontinuation occurred in 16 (21.9%) patients in the NIVO+IPI arm and eight (12.3%) patients in the SUN arm. Treatment-related select AEs (potentially immune-mediated) were less frequent in the pulmonary (NIVO+IPI, 9.6%; SUN, 0%) and renal (NIVO+IPI, 12.3%; SUN, 6.2%) categories, yet more common with regard to any-grade skin-related events (NIVO+IPI, 53.4%; SUN, 41.5%), any-grade gastrointestinal-related events (NIVO+IPI, 24.7%; SUN, 36.9%), any-grade hepatic-related events (NIVO+IPI, 21.9%; SUN, 10.8%), and any-grade endocrine-related events (NIVO+IPI, 37.0%; SUN, 18.5%). One treatment-related death, reported previously, occurred in a patient with I/P-risk sRCC treated with NIVO+IPI9; no deaths were reported among patients with I/P-risk sRCC treated with SUN.
Supplemental material
TFI in treated patients with IMDC I/P-risk sRCC
Overall, median TFI (range) was 2.9 (0.0–68.2) months with NIVO+IPI and 1.4 (0.1–65.8) months with SUN. In all patients who discontinued therapy due to treatment-related AEs, median TFI (range) was 12.3 (1.0–66.0) months with NIVO+IPI and 3.1 (0.7–65.8) months with SUN. Among all patients with an objective response, 22 of 45 (48.9%) responders treated with NIVO+IPI vs 6 of 15 (40.0%) treated with SUN discontinued therapy and never received subsequent therapy; median TFI (range) was 26.5 (0.0–68.2) months vs 15.9 (0.5–51.6) months with NIVO+IPI versus SUN in this group of patients, respectively (online supplemental figure S2). In addition, 15 of 45 (33.3%) responders in the NIVO+IPI arm compared with nine of 15 (60.0%) responders in the SUN arm discontinued therapy and received subsequent therapy; median TFI (range) was 2.8 (0.5–48.8) months with NIVO+IPI vs 2.5 (0.4–31.1) months with SUN.
Discussion
Before the introduction of immune checkpoint therapy, clinical trials in patients with sRCC treated with traditional therapies reported median OS of <1 year from the time of diagnosis.2–4 10 The results from this extended 5-year follow-up in the subgroup of patients with sRCC from the CheckMate 214 trial provide compelling data in long-term efficacy outcomes with the combination of NIVO+IPI.
With long-term follow-up of 5 years, dual checkpoint inhibition with NIVO+IPI showed enduring clinical benefit in patients with sRCC. Consistent with data reported at 42 months of follow-up,9 ORR was considerably higher, with greater depth of response, and long-term OS and PFS benefits favored treatment with NIVO+IPI over SUN. Since 42 months of follow-up, three additional CRs were observed by independent radiology review with NIVO+IPI treatment versus two additional CRs with SUN, and two additional responders in the NIVO+IPI arm experienced a TFI without subsequent therapy versus one additional responder in the SUN arm. This analysis showed particularly impressive CR rates of 23.0% with NIVO+IPI vs 6.2% with SUN among all patients with IMDC I/P-risk sRCC. The improvements in OS, PFS, and ORR were observed in patients treated with NIVO+IPI over SUN regardless of tumor PD-L1 expression. The similar clinical results in sRCC patients with or without PD-L1 expression highlight that the presence of sarcomatoid histology better differentiates clinical response to NIVO+IPI than does PD-L1 expression.
Outcomes in the overall I/P-risk population treated with NIVO+IPI in CheckMate 214 have been reported previously (n=425; median OS, 47.0 months; median PFS, 11.6 months; ORR, 42.1%; CR, 11.3%).15 Of note, the median duration of therapy among patients with I/P-risk sRCC was 7.9 months while that of the overall I/P-risk population was 7.4 months at 5 years follow-up. In addition, the median TFI among I/P-risk sRCC patients in the NIVO+IPI arm (2.9 months) was relatively short, whereas the median TFI among responders in the overall I/P-risk population was 33.2 months for NIVO+IPI and 8.1 months for SUN, suggesting a differential response in immunotherapy by sarcomatoid histology. However, it is important to note that TFI was only defined in patients who were off study treatment for I/P-risk sRCC patients, and in patients who were off study treatment and never received subsequent therapy for responders in the overall I/P-risk population. Further studies maybe helpful to understand these differences, as at present there are no data available from other sRCC trials for context.
The growing body of evidence supporting the use of immune checkpoint blockade therapies in RCC has generated a desire to further explore their role in various subpopulations, including patients with RCC and a sarcomatoid component.5–7 To our knowledge, this is the first trial in the sRCC population to demonstrate long-term efficacy that was maintained at extended follow-up of 5 years. The durability of responses with NIVO+IPI beyond 5 years in patients with sRCC underscores the key role of early CTLA-4 blockade when combined with PD-1 blockade, especially in an aggressive tumor such as sRCC with a clear cell component. The phase 2 HCRN GU16-260 study in patients with tumors (both sRCC and non-sRCC tumors) resistant to NIVO monotherapy (n=35/123) demonstrated low overall response and CR rates with salvage NIVO+IPI (ORR, 11.4%; CR, 2.9%; partial response, 8.6%).16 Contemporary data have shown that sRCC has a high expression of PD-1/PD-L1 and increased infiltration of T-regulatory cells in comparison with RCC without a sarcomatoid component.17 18 CTLA-4 is constitutively expressed on CD25+CD4+ T-regulatory cells and contributes to T-cell–mediated immunosuppression.19 In addition, increased expression of PD-1/PD-L1 and increased T-cell infiltration are associated with poor prognosis in RCC and sarcomatoid dedifferentiation.17 18 Thus, the addition of CTLA-4 blockade provides deep and durable responses in conjunction with PD-1 blockade in this population. Previous phase 3 clinical trials have reported favorable data from immunotherapy combinations with VEGF tyrosine kinase inhibitors (KEYNOTE-426, pembrolizumab plus axitinib; JAVELIN Renal 101, avelumab plus axitinib) and anti-VEGF antibodies (IMmotion151; atezolizumab plus bevacizumab).6–8 11 Most recently, the phase 3 CheckMate 9ER trial assessed NIVO plus cabozantinib (TKI) versus SUN in 75 patients with untreated sRCC, reporting a median PFS of 10.3 vs 4.2 months (HR 0.42; 95% CI 0.23 to 0.74), an ORR of 55.9% vs 22.0%, and CR rates of 8.8% vs 2.4%, respectively (minimum follow-up, 16 months).20 However, long-term benefits in patients with sRCC with these regimens have not been evaluated.
Although CheckMate 214 enrolled patients with predominantly clear cell RCC, favorable outcomes have also been reported in trials including patients with sRCC who were treated with NIVO+IPI.21 The phase 3b/4 CheckMate 920 trial (N=211) evaluated NIVO+IPI treatment in a subpopulation of patients with advanced RCC with brain metastases (n=28), and reported an objective response in two of three patients with sarcomatoid features.21 22 In addition, results from the subpopulation of patients with predominantly clear cell RCC treated with modified NIVO+IPI dosing (n=106) showed no differences in responses or safety compared with standard NIVO+IPI dosing, including those with sarcomatoid histology (n=12).23 NIVO-based treatment strategies and other combination therapies are currently being evaluated in ongoing, prospective trials that will include patients with sRCC.24–26
As described previously, the limitations of the current analysis include its non-prespecified, post hoc nature and small patient subgroups, although the distribution of patients with IMDC I/P-risk sRCC was well balanced between treatment arms. In addition, this analysis identified aRCC patients with sarcomatoid histology via two distinct methodologies: central pathology review and local pathology reports. However, sensitivity analyses of sRCC patients identified by these differing methodologies still showed similar efficacy outcomes, with the exception of CR rate at an earlier follow-up.9 The reason for this difference, which reflects only a small number of patients, remains unclear.
In conclusion, the results from this long-term analysis of patients with IMDC I/P-risk sRCC who were treated with NIVO+IPI versus SUN extend those previously reported and provide compelling support for the use of NIVO+IPI as the standard of care therapy in patients with IMDC I/P-risk sRCC.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Bristol Myers Squibb’s policy on data sharing may be found online at https://www.bms.com/researchers-and-partners/independent-research/data-sharing-request-process.html
Ethics statements
Patient consent for publication
Ethics approval
The CheckMate 214 study involves human participants and was approved by the institutional review board or ethics committee at each site and conducted in accordance with Good Clinical Practice guidelines per the International Conference on Harmonisation.
Acknowledgments
We thank the patients and their families for making this study possible, the clinical study teams who participated in the study, Bristol Myers Squibb (Princeton, New Jersey, USA) and Ono Pharmaceutical Company (Osaka, Japan), and Dako, an Agilent Technologies company, for collaborative development of the PD-L1 IHC 28-8 pharmDx assay (Santa Clara, California, USA). Professional medical writing and editorial assistance were provided by Erika Young, PharmD, of Parexel, funded by Bristol Myers Squibb.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @brian_rini, @DrChoueiri
Contributors All authors contributed to the data analysis and interpretation, drafting and revising of the manuscript, and provided final approval to submit the manuscript for publication.
Funding This study was sponsored by Bristol Myers Squibb (Princeton, New Jersey, USA) and Ono Pharmaceutical Company (Osaka, Japan). Patients treated at Memorial Sloan Kettering Cancer Center were supported in part by Memorial Sloan Kettering Cancer Center Support Grant (Core Grant, number P30 CA008748). The University of Texas MD Anderson Cancer Center is supported by the National Institutes of Health (grant P30 CA016672). Authors received no financial support or compensation for publication of this manuscript.
Competing interests BIR reports consulting or advisory role from Pfizer, Merck, Synthorx, Bristol Myers Squibb (BMS), AVEO, Surface Oncology, 3D Medicines, Corvus Pharmaceuticals, Aravive, Arrowhead Pharmaceuticals, Shionogi, Eisai, and GlaxoSmithKline; leadership role from MJH Life Sciences; travel accommodations and expenses from Pfizer, BMS, and Merck; stock ownership from PTC Therapeutics; and research funding (institutional) from Pfizer, Roche/Genentech, BMS, Merck, AstraZeneca/MedImmune, Incyte, Arrowhead Pharmaceuticals, Taris, Seattle Genetics, Immunomedics, Surface Oncology, Dragonfly Therapeutics, Aravive, and Exelixis. SS reports consulting or advisory role from BMS, AstraZeneca/MedImmune, Merck, and CRISPR Therapeutics AG; and research funding (institutional) from BMS, AstraZeneca, and Exelixis. TKC reports research grants from AstraZeneca, Aravive, AVEO, Bayer, BMS, Calithera, Circle Pharma, Eisai, EMD Serono, Exelixis, GlaxoSmithKline, IQVIA, Infinity, Ipsen Janssen, Kanaph, Lilly, Merck, NiKang, Nuscan, Novartis, Pfizer, Roche, Sanofi/Aventis, Surface Oncology, Takeda, Tempest, and UpToDate; consulting fees from AstraZeneca, Aravive, AVEO, Bayer, BMS, Calithera, Circle Pharma, Eisai, EMD Serono, Exelixis, GlaxoSmithKline, IQVIA, Infinity, Ipsen Janssen, Kanaph, Lilly, Merck, NiKang, Nuscan, Novartis, Pfizer, Roche, Sanofi/Aventis, Surface Oncology, Takeda, Tempest, and UpToDate; honoraria from AstraZeneca, Aravive, AVEO, Bayer, BMS, Calithera, Circle Pharma, Eisai, EMD Serono, Exelixis, GlaxoSmithKline, IQVIA, Infinity, Ipsen Janssen, Kanaph, Lilly, Merck, NiKang, Nuscan, Novartis, Pfizer, Roche, Sanofi/Aventis, Surface Oncology, Takeda, Tempest, and UpToDate; advisory board fees from AstraZeneca, Aravive, AVEO, Bayer, BMS, Calithera, Circle Pharma, Eisai, EMD Serono, Exelixis, GlaxoSmithKline, IQVIA, Infinity, Ipsen Janssen, Kanaph, Lilly, Merck, NiKang, Nuscan, Novartis, Pfizer, Roche, Sanofi/Aventis, Surface Oncology, Takeda, Tempest, and UpToDate; leadership role from NCCN, GU Steering Committee, ASCO, and ESMO; stock ownership in Pionyr, Tempest, Osel, and NuscanDx; institutional patents filed on molecular mutations and immunotherapy response, and ctDNA; medical writing and editorial assistance support funded by communications companies; mentored several non-US citizens on research projects with potential funding (in part) from non-US sources/Foreign Components; and independent funding (institutional) of drug companies or/and royalties potentially involved in research around the subject matter. DFM reports consulting or advisory role from BMS, Merck, Genentech/Roche, Pfizer, Exelixis, Novartis, Array BioPharma, Peloton Therapeutics, EMD Serono, Jounce Therapeutics, Alkermes, Lilly, Eisai, Calithera Biosciences, and Iovance Biotherapeutics; other fees from Beth Israel Deaconess Medical Center; research funding (institutional) from Prometheus, BMS, Merck, Genentech, Novartis, Alkermes, and Peloton Therapeutics; and uncompensated relationships with X4 Pharmaceuticals and AVEO. RJM reports consulting or advisory role from Novartis, Eisai, Exelixis, Merck, Genentech/Roche, Incyte, Lilly, Pfizer, AstraZeneca, EMD Serono, and Calithera Biosciences, travel accommodations and expenses from BMS; and research funding (institutional) from Pfizer, BMS, Eisai, Novartis, Genentech/Roche, Exelixis, and Merck. S George reports consultant or advisory role from AVEO, Bayer, BMS, Eisai, EMD Serono, Exelixis, Merck, Pfizer, QED Therapeutics, Sanofi/Genzyme, and Seattle Genetics; and local PI fees (institutional) from Agensys, Aravive, AVEO, Bayer, BMS, Calithera, Corvus, Eisai, Exelixis, Gilead, Merck, Novartis, Pfizer, Seattle Genetics, and Surface Oncology. TP reports research grants from AstraZeneca, Roche, BMS, Exelixis, Ipsen, Merck, MSD, Novartis, Pfizer, Seattle Genetics, Merck Serono, Astellas Pharma, Johnson & Johnson, and Eisai; consulting fees from BMS, Merck, AstraZeneca, Ipsen, Pfizer, Novartis, Incyte, Seattle Genetics, Roche, Exelixis, MSD, Merck Serono, Astellas Pharma, Johnson & Johnson, and Eisai; and travel accommodations and expenses from Pfizer, MSD, AstraZeneca, Roche, and Ipsen. FD reports research funding (institutional) from MSD Oncology. SST reports consulting or advisory role from Merck, Intellisphere, Natera, BMS, and Exelixis; research funding (institutional) from Genentech, BMS, MSD, Calithera Biosciences, Pfizer, Jounce Therapeutics, Nektar, Exelixis, and Clinigen Group; and Patent pending (institutional). SKP reports consultant or advisory role from F. Hoffmann LaRoche; travel accommodations and expenses; and research funding from Eisai, Genentech, Roche, and Pfizer. S Gupta, C-WL, and RJ are employed by and have stock ownership in BMS. NMT reports consulting or advisory role from Novartis, Exelixis, BMS, Nektar, Pfizer, Eisai, Ono Pharmaceutical, Oncorena, Surface Oncology, Neoleukin Therapeutics, Ipsen, MSD, Calithera Biosciences, and Lilly; travel accommodations and expenses from Pfizer, Nektar, BMS, Eisai, Surface Oncology, Lilly, Ipsen, and Calithera Biosciences; honoraria from Pfizer, Novartis, BMS, Exelixis, Nektar, Eisai, Ono Pharmaceutical, Lilly, Oncorena, Ipsen, Surface Oncology, Neoleukin Therapeutics, MSD, and Calithera Biosciences; and research funding from BMS, Exelixis, Pfizer, Nektar, Calithera Biosciences, Lilly, Mirati Therapeutics, Arrowhead Pharmaceuticals, Takeda, Epizyme, and Eisai.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.