Article Text

Abstract
Fibrolamellar carcinoma (FLC) is a rare cancer of the liver that most commonly affects children and young adults. There is no clear standard of care for the disease, whose response to treatment seems to be very different from that of hepatocellular carcinoma. We present a case of FLC in a patient in her mid 30s that recurred and persisted despite resection and multiple lines of treatment. Following transcriptomic analysis, a combination of ipilimumab (anti-CTLA4) and nivolumab (anti-PD-1) led to complete remission, although common biomarkers for immune checkpoint blockade were all negative in this case. The patient is still in remission. Here, combined checkpoint blockade guided by novel transcriptomic analysis led to complete remission after failure of several lines of treatment.
- Biomarkers, Tumor
- Genetic Markers
- Immunotherapy
- Liver Neoplasms
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Insights
Innovative transcriptomic analysis based on synthetic rescue markers unexpectedly predicted response to anti-CTLA4 combined with anti-PD-1 immunotherapy in a patient with DNAJB1-PRKACA-bearing fibrolamellar cancer, and administration of this therapy yielded a complete remission, despite the tumor having progressed on anti-PD-L1 immunotherapy, and being PD-L1 negative, tumor mutational burden low, and microsatellite stable.
Background
Fibrolamellar carcinoma (FLC) is a rare liver cancer that primarily occurs in adolescents and young adults who have no history of liver disease. In the early stages of the disease, affected patients often have no symptoms; therefore, by the time the cancer is found, it may have already spread beyond the liver.1 2 FLC is different from hepatocellular carcinoma (HCC) in that it affects young people with normal liver function and no known risk factors. It is also distinct pathologically in that the large polygonal tumor cells are arranged in cords, nests and sheets and embedded in a dense collagen matrix in which the collagen fibrils are oriented parallel to the tumor cells. There is a paucity of standardized treatment protocols or guidelines for affected individuals. Due to the rarity of the disease, there are also a dearth of treatment trials that have been conducted on large patient cohorts. Instead, various treatments including chemotherapy have been reported in the medical literature as part of smaller studies. In the setting of metastatic disease, as in our patient, 5-year survival rates are ~39%.3 Chemotherapy may be helpful in cases of unresectable or metastatic FLC. Frequently used chemotherapy agents include cisplatin, epirubicin, and 5-fluorouracil; however, FLC does not, in general, respond well to chemotherapy.3
The molecular hallmark of FLC is the DNAJB1-PRKACA fusion, as noted in our patient.4 The chimeric RNA is predicted to code for a protein containing the amino-terminal domain of DNAJB1, a homolog of the molecular chaperone DNAJ, fused in frame with PRKACA, the catalytic domain of protein kinase A.4 The DNAJB1-PRKACA fusion is an oncogenic driver that upregulates protein kinase activity. Although initially considered specific to FLC, it is now known that DNAJB1-PRKACA can occur, although rarely, in other oncocytic pancreatic and biliary neoplasms.5 There is no known manner to target this fusion.
Case presentation
A patient in her mid 30s (non-smoker) with an unremarkable medical and family history was found to have a 7 cm hepatic mass on ultrasonography, and was diagnosed with FLC, following liver segmentectomy, removal of a hilus hepatis lymph node, and pathologic review. Two months after the resection, metastatic disease was identified in the lungs, mediastinum, and the liver hilum through CT scan, further confirmed by MRI. A sample from the liver resection was sent for a TEMPUS xT DNA and RNA analysis (https://www.tempus.com/oncology/genomic-profiling/), which revealed the presence of chromosomal rearrangement resulting in a DNAJB1-PRKACA fusion, consistent with the pathological diagnosis of FLC. No other pathogenic variants were identified. The patient tested negative for hepatitis B and C virus infection, and standard immuno-oncology biomarkers showed negative PD-L1 immunohistochemistry, microsatellite stable disease, and tumor mutational burden of 1.6 mutations/megabase. We performed subsequent analysis of the sequencing data for homologous recombination deficiency (HRD), which has been shown to be associated with higher sensitivity to immunotherapy. Testing for germline and somatic mutations in HRD-associated genes commonly used in clinical gene panels,6 we found no relevant alterations. In addition, reviewing the patient’s somatic mutations reveals a mostly-sparse mutational profile. We further examined the patient somatic mutations for evidence of COSMIC mutational signature 3, which has been shown to be associated with HRD.6 Out of 20 somatic mutations observed, analysis using SignatureAnalyser7 labeled 8 mutations as Signature-3-derived, determing the patient as HRD-negative (based on a threshold of 31 mutations as described by6).
She was treated with a combination of atezolizumab (PD-L1 immune checkpoint inhibitor) and bevacizumab (VEGF-A-antibody) for three courses, but a follow-up CT 6 weeks later demonstrated progression in all metastatic sites. Two months later, capecitabine by mouth was added to the treatment regimen. Her disease progressed and she developed severe pain in the right chest and shoulder.
At that point, she presented to our hospital (Sheba Medical Center) and new imaging results at the time of admission for pain (May 2020) confirmed progressive disease, mainly in the lung bases (figure 1A). Complete blood count and metabolic panel was within normal range. Out of serum oncology markers workup (carcinoembryonic antigen, CA-15–13, CA-125, CA19-9 αFP), only CA19-9 was mildly elevated, at 43 u/mL (normal range=0–37 u/mL).
{kind=link}
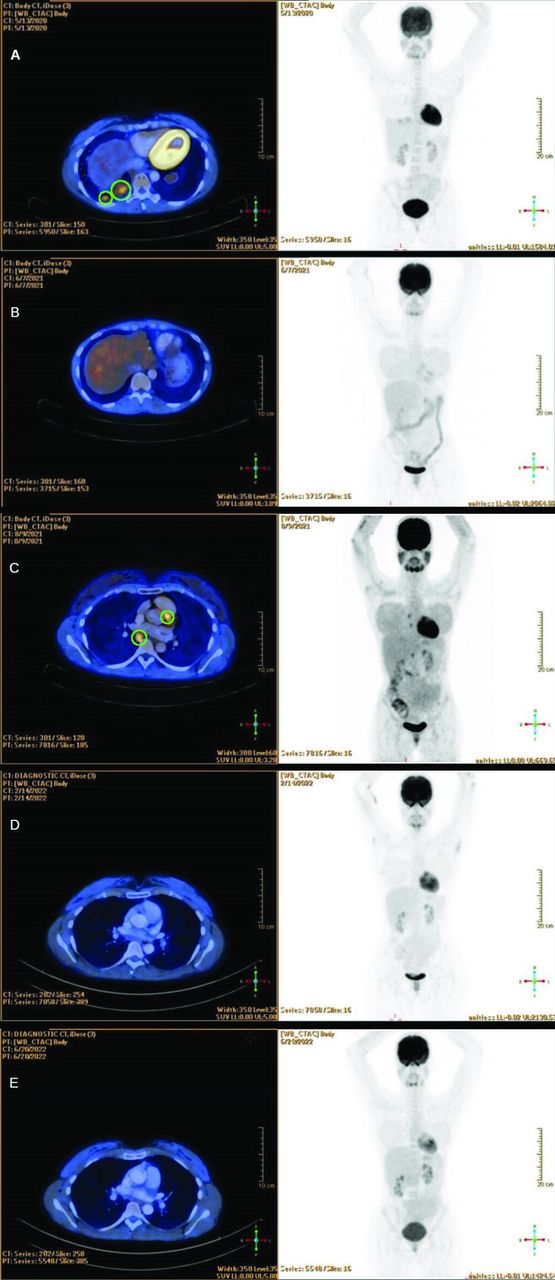
Serial PET-CT scans are shown. (A) Sub pleural masses prior to Ipilimumab nivolumab treatment (May 2020). (B) Radiographic complete response after treatment with combination of nivolumab 3 mg/kg and ipilimumab 1 mg/kg intravenously every 3 weeks for four doses, followed by nivolumab 3 mg/kg intravenously every 2 weeks for another 12 doses (February 2021). (C) Mediastinal disease relapse after discontinuation of treatment (August 2021). (D) Complete remission after resuming ipilimumab nivolumab therapy (February 2022). (E) Complete remission continues under nivolumab treatment (June 2022). PET-CT, positron emission tomography-computed tomography.
The patient’s tumor was referred for further molecular analysis by Pangea Biomed (https://pangeabiomed.com)—a computational precision oncology company—in search of potential treatment options based on computational analysis of the tumor transcriptome. The company’s ‘ENLIGHT’ engine analyzes gene expression patterns in the tumor’s RNAseq, to predict the tumor’s response to a wide array of targeted and immuno-oncology therapies.8 9 Briefly, a ‘synthetic rescue’ (SR) interaction is a genetic interaction in which the inactivation of one gene reduces cell viability, but an alteration in the activity of another gene, termed the rescuer, restores (rescues) viability.10 11 The ENLIGHT pipeline first identifies a set of clinically relevant genetic interactions (SR and synthetic lethal interactions) from big data to build drug-specific genetic interaction networks. Then, given a transcriptomic profile of an individual patient’s tumor, ENLIGHT infers the activation state of each gene interacting with a cancer drug’s target, and based on the latter it assigns an ENLIGHT Matching Score (EMS) to each drug. This score denotes the predicted likelihood that this patient will respond to the respective drug, and drugs with higher EMS scores are highlighted for the physician’s further consideration (for more details on ENLIGHT, see Dinstag et al 9).
By analyzing the activation state of genes interacting with the targets of immune checkpoint blockers, a very high probability of response to PD-1 inhibition, and a high probability of response to CTLA4 inhibition was predicted. Predicted positive contributions to the CTLA4 inhibition score included CD44, THBD (high expression), CCL13, IL22RA2, and CD274 (normal expression). For PD1 inhibition, score contributions were by CD27, LTBR, TNFRSF13B+C, IFITM2, ICAM4 and CXCL16 (high expression), and CD4 (normal expression). As can be seen in table 1, PD-1 inhibition was the highest scoring treatment according to ENLIGHT, and CTLA4 inhibition (ipilimumab) ranked third, after alpelisib (targeting PIK3CA). It should be noted that ENLIGHT only produced predictions for monotherapies. The known synergistic effects and clinical utility of CTLA4+PD-1 inhibitor combinations12 and the high EMS both treatments received led to the decision to treat the patient with a combination of nivolumab and ipilimumab.
ENLIGHT scores for PD-1 inhibitor (nivolumab), ipilimumab and other monotherapies for the current FLC patient and 6 FLC patients from the TCGA
Treatment was therefore begun in June 2020 with a combination of nivolumab 3 mg/kg and ipilimumab 1 mg/kg intravenously every 3 weeks for four doses, followed by nivolumab 3 mg/kg intravenously every 2 weeks, per the Checkmate 214-type protocol.13 Two months after treatment initiation, positron emmission tomography-computed tomography (PET-CT) showed reduction in the size of lung masses (eg, left basal node at 2.5 cm vs 3.2 cm in previous test). Lymph nodes in the mediastinum and lung hilum also showed size reduction (eg, a subcarinal node of 4.4 cm in the previous test was measured at 2.7 cm). The only side effect observed was pruritus, treated by 5 mg daily prednisone by mouth. Shortly thereafter, per the protocol, ipilimumab was discontinued, and the patient continued to receive 240 mg nivolumab on a biweekly basis. Subsequent PET-CT performed 3 months later (November 2020) demonstrated minimal absorption in lungs and mediastinum, suggesting only small sites of viable residual disease. Additional PET-CT scans in the following 6 months (February (figure 1B) and June 2021—9 and 12 months since starting treatment) showed complete response to treatment. After 16 cycles of treatment, medication was discontinued due to grade 2 pruritus and grade 2 diarrhea. Follow-up imaging 12 weeks later (August 2021) showed relapse in the mediastinum and liver hilum (figure 1C). The patient returned to the original ipilimumab/nivolumab regimen for four cycles, followed by nivolumab as monotherapy. PET-CT in February 2022 again showed complete response (figure 1D). The complete response was ongoing as of the last PET-CT scan, in June 2022 (figure 1E), and the patient is still in remission as of September 2022.
Discussion
Current precision oncology methodologies rely primarily on identifying ‘actionable mutations’ or fusion events, which can be matched with suitable targeted agents. Although targetable alterations may be found in most tumors, and addressing a majority of actionable alterations (high matching score) in each cancer can be effective in treating patients with cancer,14 many important drivers—such as the DNAJB1-PRKACA fusion seen in FLC—have no known way in which to impact them from a therapeutic standpoint. Of interest, expression aberrations are highly abundant in tumor cells, and could serve as a basis for broadening the application of precision oncology treatments beyond the DNA level.15 Recently, such an approach has been proposed, based on computational analysis of the tumor transcriptome.8 The ENLIGHT computational platform based on the same principles has demonstrated that it is applicable both for personalized medicine applications and for optimizing patient stratification in clinical trials.9 Specifically, in a real-world data computational analysis, patients receiving a therapy with a high EMS are shown to be markedly more likely to respond to treatment than ones whose therapy received a low EMS.9 Notably, the EMS is based on analysis of transcriptomic data and, as illustrated in this case, can generate actionable insights beyond those provided by standard biomarkers.
Of special interest, the patient described herein had not benefitted from treatment with atezolizumab (anti-PD-L1), but responded remarkably well to the combination of ipilimumab (anti-CTLA4) and nivolumab (anti-PD-1). This clinical result is consistent with our EMS analysis suggesting that both CTLA4 and PD-1 are important in her FLC. PD-1 interacts with both PD-L1 and PD-L2 ligands,16 whereas PD-L1 expressed on tumor cells and tumor-infiltrating immune cells interacts with PD-1 and with B7.1 expressed on T cells. Therefore, the action of PD-L2 as well as of CTLA4 may explain why the patient failed to respond to the anti-PD-L1 agent atezolizumab (which, by definition, attenuates the action of PD-L1, but not of PD-L2, on PD-1), but did respond to the anti-PD-1 agent nivolumab combined with the anti-CTLA4 agent. The hypothesis gains support from the observation that PD-L1 RNA expression in this case was relatively low (in the 38th percentile relative to hepatocellular patients in The Cancer Genome Atlas), whereas PD-L2 expression was high (72nd percentile). Of interest, response to an anti-PD-1 agent after progression on an anti-PD-L1 agent has previously been reported anecdotally in non-small cell lung cancer.17
Following the exceptional response in this case, with the patient achieving complete remission, and another recent report of a near-complete, long-lasting clinical response to ipilimumab plus nivolumab in an FLC patient with advanced disease who had failed other systemic therapies, we examined whether or not a similar transcriptomic signature could apply in other cases of FLC. To that end, we computed EMS for six FLC patients within The Cancer Genome Atlas data, three of whom were originally misclassified as HCC and identified by Dinh et al. 18 Strikingly, all six FLC cases indeed received high EMS for treatment with nivolumab. EMS for treatment with ipilimumab were variable. Of further interest, a prior case of a patient with fibrolemellar carcinoma achieving a near complete response on nivolumab and ipilimumab has been published19; as with our patient, PD-L1 immunohistochemistry was negative, tumor mutational burden was low and microsatellite status was stable. Therefore, response to anti-PD-1/anti-CTLA4 agents was non-intuitive.
In sum, the complete response of this patient’s FLC to nivolumab and ipilimumab after progression of the disease on the anti-PD-L1 agent atezolizumab points to the potential benefit of checkpoint inhibitor therapy in some FLC cases, to the fact that failure of an anti-PD-L1 agent does not rule out response to an anti-PD-1-based immunotherapy regimen, and to the potential of tumor transcriptome-based advanced analytics in precision oncology to guide treatment, even in patients whose DNA alterations are considered undruggable. Further large-scale prospective trials are warranted.
Ethics statements
Patient consent for publication
Acknowledgments
We wish to thank Mark Furth, Scientific Director of the Fibrolamellar Cancer Foundation, for reading the report and providing valuable references.
References
Footnotes
Twitter @TiroshOmer, @BekerTuvik
RB, TB and RK contributed equally.
Contributors RB treated the patient, presented the case for analysis to Pangea Biomed, administered the treatment described in the report, and took part in writing the report. GD and TB presented and interpreted the results of the Pangea Biomed ENLIGHT report. GD and OT performed further analysis of this case and other FLC cases from the TCGA. RB, TB, ES, ER and RK wrote the report. All authors discussed the case, contributed to literature search, and provided feedback on drafts of this report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests RB Serves on Pangea Biomed’s Scientific advisory Board. GD, OT, ES and TB are employees of Pangea Biomed. ER is a cofounder of Pangea Biomed (now divested) and serves on its Scientific Advisory Board as an unpaid consultant. RK has received research funding from Boehringer Ingelheim, Debiopharm, Foundation Medicine, Genentech, Grifols, Guardant, Incyte, Konica Minolta, Medimmune, Merck Serono, Omniseq, Pfizer, Sequenom, Takeda, and TopAlliance as well as consultant and/or speaker fees and/or advisory board for Actuate Therapeutics, AstraZeneca, Bicara Therapeutics, Inc., Biological Dynamics, EISAI, EOM Pharmaceuticals, Iylon, Merck, NeoGenomics, Neomed, Pfizer, Prosperdtx, Regeneron, Roche, TD2/Volastra, Turning Point Therapeutics, X-Biotech; has an equity interest in CureMatch Inc. and IDbyDNA; serves on the Board of CureMatch and CureMetrix, and is a co-founder of CureMatch.
Provenance and peer review Not commissioned; externally peer reviewed.