Article Text

Abstract
Background As an integral part of the tumor microenvironment (TME), tumor-associated neutrophils play a crucial role in tumor development. The objective of this study was to investigate the plasticity of tumor-associated N1 and N2 neutrophils in the TME of pancreatic ductal adenocarcinoma (PDAC), along with its impact on survival and association with immune infiltrations.
Methods The primary and validation cohorts including 90 radical resection patients from September 2012 to May 2016 and 29 radical resection patients from September 2018 to October 2019, respectively, with complete survival data, were enrolled. Immunofluorescence staining was used to identify tumor-associated N1 and N2 neutrophils, and the N1/N2 ratio was used to evaluate N1 and N2 plasticity. Thereafter, the association between tumor-associated N1/N2 neutrophil plasticity, clinical features, and immune infiltrations was investigated.
Results There was a significant increase in tumor-associated N2 neutrophils compared with tumor-associated N1 neutrophils. Low N1/N2 ratios were associated with the poorer differentiation of tumors, easier lymph node metastases, and a higher TNM stage. The median overall survival (OS) and recurrence-free survival (RFS) of the high tumor-associated N1 neutrophil group were significantly longer than those of the low group, while the tumor-associated N2 neutrophils played an opposite role. The multivariable analysis revealed that a high N1/N2 ratio was a significant prognostic indicator for OS and RFS. In addition, tumor-associated N1/N2 neutrophils showed an opposite correlation with tumor-infiltrating CD8+ T cells and Tregs.
Conclusion The plasticity of tumor-associated N1/N2 neutrophils was identified as a crucial prognostic indicator that might reflect the TME and immune escape in patients with PDAC. On further investigation and validation, our findings may be used to further stratify patients with varying prognoses to optimize treatment.
- Tumor Biomarkers
- Tumor Microenvironment
Data availability statement
Data are available on reasonable request. The data that support the findings of this study are available on request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Neutrophil diversity and their plasticity in cancers are responsible for the dual potential of tumor-associated neutrophils (TANs) in the tumor microenvironment.
WHAT THIS STUDY ADDS
The infiltration of tumor-associated N2 neutrophils in the pancreatic ductal adenocarcinoma microenvironment was higher than that of N1 neutrophils.
The plasticity of tumor-associated N1/N2 neutrophils is an independent prognostic indicator of overall survival and recurrence-free survival, and correlated with CD8+ T cell and Treg infiltration.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The targeting of TAN polarization may promote the immune response and increase their therapeutic efficacy.
Introduction
Pancreatic ductal adenocarcinoma (PDAC) is an extremely lethal malignancy, with a 5-year survival rate of about 11%.1 The poor prognosis of this disease is associated with difficulties during early diagnosis, limited treatment options, and high recurrence rates. Therefore, there is an urgent need for the development of novel biomarkers and therapies based on their characteristics. Several studies have revealed that the tumor microenvironment (TME), which contains cancer cells, extracellular components, and stromal cells, is important for the occurrence and progression of PDAC.2 It is thought that the dense stroma and extensive immunosuppression of the TME in PDAC promote tumor growth and immune escape.3 4 PDAC exhibits an immunosuppressive phenotype, and patients with highly immunosuppressive PDAC tend to have poor prognosis.5 Despite numerous advances during the past decade in the field of immuno-oncology, there are currently no therapeutic options for PDAC, possibly due to the distinctive landscape of immune cell infiltration in this disease.6 7 Thus, it is crucial to identify tumor-infiltrating cell subtypes associated with tumor prognosis and to develop multimodal approaches to remodel the TME of PDAC.
Increasing evidence has suggested that tumor-associated macrophages (TAMs) represent an important immune cell population in the PDAC stroma, displaying an extensive range of plasticity in both anti-tumorigenic M1-like phenotypes and protumorigenic M2-like phenotypes through metabolic approaches.8 Tumor-associated neutrophils (TANs) are another crucial component of the TME. Many studies have demonstrated that TANs play a crucial role in the PDAC microenvironment, and both peripheral neutrophils and TANs are found to be associated with cancer survival.9 10 Nonetheless, the specific role of TANs still remains unclear. Some studies have reported on their association with poor prognosis,11 while others have reported on a favorable outcome.12 According to Jaillon et al,13 TANs contributed to tumor-promoting inflammation through extracellular matrix remodeling, angiogenesis, immunosuppression, and metastasis. On the contrary, they may also exert antitumor responses through the direct killing of cells and cell signaling networks. Thus, the neutrophil plasticity and diversity of cancers may be responsible for the dual potential of TANs in the TME.
TANs are reported to be similar to TAMs in that they can be classified into two distinctive phenotypes: anti-tumorigenic N1 neutrophils and protumorigenic N2 neutrophils.14 N1 neutrophils exert powerful antitumor properties through antibody-dependent or direct cytotoxicity,15 ROS-mediated coupling,16 and the generation of neutrophil extracellular traps (NETs).17 Similarly, N2 neutrophils contribute to tumor angiogenesis through secretions, such as matrix metallopeptidase 9 and vascular endothelial growth factor,18 promote metastasis by enhancing the expression levels of premetastatic proteins, such as Bv8, S100A8, and S100A9, and recruit immune suppressive subtypes, such as regulatory T cells (Tregs), into the TME.19 Numerous studies have reported on the clinical prognostic potential of TANs in cancers. However, the plasticity and value of tumor-associated N1/N2 neutrophils in PDAC remain unclear.
Taken together, we aim to provide an understanding of the plasticity of tumor-associated N1/N2 neutrophils within the TME of PDAC and their association with immune infiltration. In addition, the clinical prognostic value of tumor-associated N1/N2 neutrophils were assessed and validated to understand the polarization of neutrophils in PDAC patients following radical resection. This is the first study to elucidate the prognostic value of tumor-associated N1/N2 neutrophil plasticity in PDAC patients.
Materials and methods
Patient selection and tissue microarrays (TMA)
Patients at our hospital who received pancreaticoduodenectomy (PD) or distal pancreatectomy from September 2012 to May 2016 and from September 2018 to October 2019 with complete survival data were enrolled in this study, and their tissue microarray (TMA) samples were collected. Each of these independent cohorts contained 90 and 29 patients with PDAC, respectively. The inclusion and exclusion criteria were: (1) a histological diagnosis of PDAC without neoadjuvant therapies; (2) no history of other malignancies; (3) complete R0 resection as determined through pathological examination; (4) complete clinical and follow-up data; (5) no postoperative participation in clinical trials involving immune or targeted therapies; (6) no distant metastases or undetermined origins.
Using these PDAC samples, the formalin-fixed, paraffin-embedded (FFPE) tissue blocks were prepared. Then, representative tissue areas confirmed by experienced pathologists were marked and tissue cylinders that were 3.0 mm in diameter were punched out. Detailed clinicopathological data were collected on the TMAs, and included age, gender, preoperative blood examinations, primary site, tumor differentiation, tumor size, lymph node metastasis, perineural invasion, and follow-up data (as of December 2021). The data were collected by one surgeon from the record system and verified by another.
Immunohistochemistry staining and immunofluorescence staining
H&E staining was performed on the TMA specimens, and the results were assessed by an experienced pathologist. For the immunohistochemistry (IHC) staining, anti-CD8 (Cell Signaling Technology, Danvers, Massachusetts, USA) and anti-FoxP3 (R&D Systems, Tustin, California, USA) monoclonal antibodies were utilized, as previously described.20 21 The average number of tumor-infiltrating immune cells per high-power fields (HPF) were assessed by three independent ×400 HPF.
Immunofluorescence (IF) staining was performed on the TMA specimens of FFPE tissue. In this study, we used anti-myeloperoxidase (MPO) (Abcam, ab208670, Cambridge, UK), anti-CD11b (Abcam, ab133357), and anti-CD206 (Abcam, ab64693) monoclonal antibodies as the primary antibodies at room temperature for 1 hour of incubation. Next, the specimens were incubated for an additional hour with Alexa Fluor 488 (B40953), Alexa Fluor 555 (B40955), and Alexa Fluor 647 (B40958) along with Tyramide Reagent (ThermoFisher Scientific, Waltham, Delaware, USA). As the final step, the specimens were incubated for 20 min with DAPI (Solarbio, #C0060). A fluorescence microscope (Olympus, Tokyo, Japan) was used to visualize the cells.
Survival follow-up
All patients were regularly postoperatively followed-up, as previously described.22 The overall survival (OS) was calculated from the surgical date until death for any reason or until the last follow-up (December 2021). Recurrence-free survival (RFS) was defined as the period between the date of surgery and the date of recurrence of the disease or death, whichever occurred first or the last follow-up.
Statistical analysis
All statistical analyses in this study were performed using SPSS V.21.0 software (SPSS). The optimal cut-off values for the tumor-associated N1 and N2 neutrophils, the tumor-infiltrating CD8+ T cells and Tregs were determined using receiver operating characteristic (ROC) curves. Continuous variables presented as medians and IQR were compared using the Student’s t-test or Mann-Whitney U test. The relationships between the tumor-associated N1/N2 neutrophils and clinicopathological features were examined using Pearson’s χ2 test or Fisher’s exact test, while the correlations between two continuous variables were assessed using Spearman’s correlation analysis. The log-rank test was used on the Kaplan-Meier curves to assess OS and RFS. Univariate and multivariate Cox proportional analyses were applied to evaluate independent prognostic risks. A two-tailed analysis with a p<0.05 was used to determine statistical significance.
Results
Demographical and clinicopathological characteristics
In the primary cohort, 56 of the 90 patients (62.2%) were male, and their median age was 64.5 (IQR 56.0–70.0) years old. A total of 57.8% of patients had undergone PD. Approximately 25% of the PDAC patients included in this cohort were of advanced T stages (T3 and T4), while 41.1% of patients were of aggressive N stages (N1 and N2). Referring to the American Joint Committee on Cancer (AJCC) eighth TNM staging system, 41, 34, and 15 patients had stages I, II and III of the disease, respectively. About 88.9% of patients showed perineural invasion under pathological detection. An elevated serum CA19-9 level was observed in 75.6% of the PDAC patients and an elevated serum carcino embryonie antigen (CEA) level in 24.4% of the patients. In addition to liver function, nutrition condition and glycometabolism, other indicators of the patient status are shown in table 1. The validation cohort included 29 patients with resected PDAC who met the inclusion criteria of this study. The validation cohort consisted of 75.8% male patients, with a median age of 63.0 (IQR 57.0–69.5). In addition, all clinicopathological characteristics were compared between the primary and validation cohorts and no significant differences were observed, except for the gamma-glutamyl transpeptidase (GGT) level (table 1).
The demographic and clinicopathological characteristics of patients with resected PDAC in the primary and validation cohort
The plasticity of tumor-associated N1/N2 neutrophils in the TME of PDAC
As shown in figure 1A and online supplemental figure 1, MPO+CD11b+CD206- neutrophils were identified as tumor-associated N1 neutrophils and MPO+CD11b+CD206+ neutrophils were identified as tumor-associated N2 neutrophils.23 The median number of tumor-associated N1 and N2 neutrophils were 10.7 (IQR 7.6–24.3) and 20.0 (IQR 14.4–28.8), respectively, in the primary cohort. The validation cohort did not show any significant differences from the primary cohort in terms of tumor-associated N1 and N2 neutrophils counts, with median values of 15.0 (IQR 8.3–32.8) and 14.7 (IQR 9.6–31.5), respectively (table 1). The unpaired analysis indicated that the mean number of tumor-associated N2 neutrophils was 22.8, which is higher than that of the tumor-associated N1 neutrophils in the primary cohort (16.4, p<0.001, figure 1B). Concomitantly, a discrepancy between the tumor-associated N1 and N2 neutrophils was also observed when the paired analysis was performed (p=0.004, figure 1C). However, the validation cohort did not show any significant differences possibly due to its smaller size (p=0.989 and 0.991, respectively, figure 1D, E).
Supplemental material
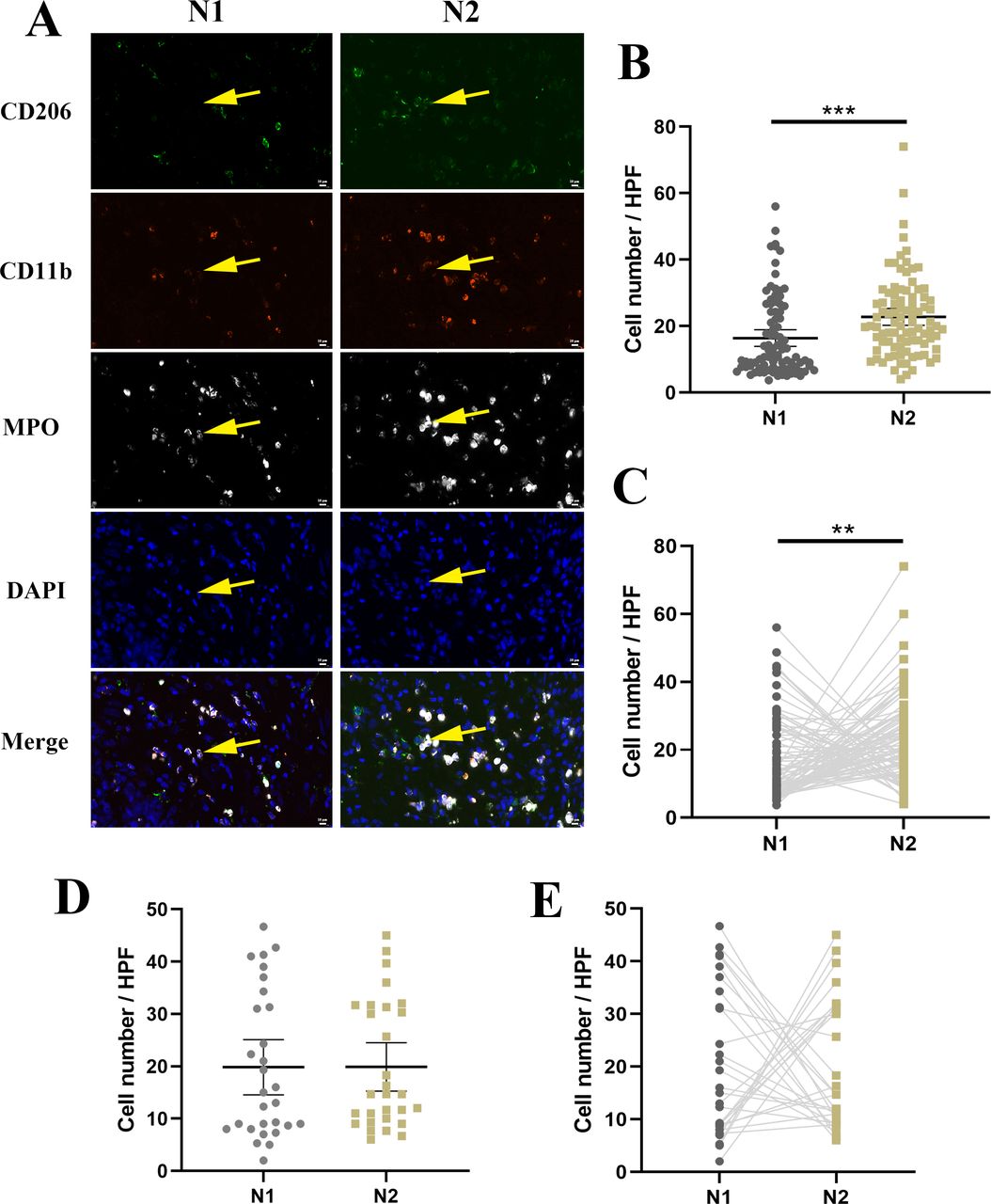
Identification of the plasticity of tumor-associated N1/N2 neutrophils within PDAC. (A) Representative images of IF staining for tumor-associated N1/N2 neutrophils marked by yellow arrow. (B) A comparison of the numbers of tumor-associated N1/N2 neutrophils in the primary cohort by unpaired analysis. (C) A comparison of the numbers of tumor-associated N1/N2 neutrophils in the primary cohort by paired analysis. (D) A comparison of the numbers of tumor-associated N1/N2 neutrophils in the validation cohort by unpaired analysis. (E) A comparison of the numbers of tumor-associated N1/N2 neutrophils in the validation cohort by paired analysis. **P < 0.01, ***P < 0.001. HPF, high-power field; IF, immunofluorescence; PDAC, pancreatic ductal adenocarcinoma.
Relationship between tumor-associated N1/N2 neutrophil plasticity and clinicopathological features
The optimal cut-off values of the tumor-associated N1, N2, and N1/N2 ratios were determined as 9.5, 29.7, and 0.87, respectively, based on the ROC curves of the primary cohort. Accordingly, 52 patients were classified into the high infiltration of tumor-associated N1 neutrophil group, 21 patients into the high infiltration of tumor-associated N2 neutrophil group, and 31 patients into the high N1/N2 ratio group. As shown in table 2, tumor-associated N1 neutrophil infiltration was significantly correlated with tumor differentiation (p=0.038), AJCC N stage (p=0.020), TNM stage (p=0.025), total bilirubin (TBIL, p=0.013), alanine aminotransferase (ALT, p=0.009), and aspartate aminotransferase (AST, p=0.037) but not with any other factors. Tumor-associated N2 neutrophil infiltration was significantly associated only with tumor location (p=0.037). The N1/N2 ratio was used to evaluate N1 and N2 plasticity to balance N1 and N2 variation, and the results showed remarkable correlations between the N1/N2 ratio and tumor differentiation (p=0.001), AJCC N stage (p=0.010), TNM stage (p=0.022), and perineural invasion (p=0.031). Therefore, patients with a lower N1/N2 ratio may be prone to worse cell differentiation, easier lymph node metastasis, and perineural invasion, as well as belong to a higher TNM stage.
Relationships between tumor-associated N1, N2 and N1/N2 ratio and clinicopathological characteristics in the primary cohort
Correlations between tumor-associated N1/N2 neutrophils and intratumoral infiltration of CD8+ T cells and Tregs
To increase our understanding of immune killing and suppression mechanisms in the TME, we recounted and reanalyzed the TMAs that had previously been stained for detection20 21 (figure 2A). In the primary cohort, the median number of CD8+ T cells in the TME was 32.2 (IQR 15.6–56.2), and the median number of tumor-infiltrating Tregs was 6.0 (IQR 2.9–14.4). The optimal cut-off values for tumor-infiltrating CD8+ T cells and Tregs were 26.3 and 9.2, respectively. The median OS and RFS of the high tumor-infiltrating CD8+ T cell group were longer than those of the low group (OS: 39 vs 14 months, p<0.001, HR=0.254, 95% CI 0.139 to 0.465, figure 2B; RFS: 23 vs 10 months, p<0.001, HR=0.362, 95% CI 0.212 to 0.620, figure 2C). A higher number of tumor-infiltrating Tregs was significantly correlated with shorter OS (16 vs 32 months, p<0.001, HR=2.415, 95% CI 1.335 to 4.368, figure 2D) and RFS (9 vs 22 months, p<0.001, HR=2.427, 95% CI 1.409 to 4.179, figure 2E). As we previously determined, the ratio between CD8+ T cells and Tregs was remarkably associated with long-term survival.20 Therefore, the prognostic values of the CD8/Treg ratio were also estimated, and its optimal cut-off value was determined to be 2.69 in the primary cohort, based on the ROC curves. Consequently, 58 patients were classified into the high CD8/Treg ratio group, and the median OS and RFS of these patients were found to be longer than patients in the low group (OS: 36 vs 13 months, p<0.001, HR=0.262, 95% CI 0.135 to 0.508, online supplemental figure 2A; RFS: 22 vs 9 months, p<0.001, HR=0.387, 95% CI 0.217 to 0.692, online supplemental figure 2B).
Supplemental material

Correlation between tumor-associated N1/N2 neutrophils and infiltration of intratumoral CD8+ T cells and Tregs in the primary cohort. (A) Representative images of IHC staining for CD8+ T cells and Tregs. (B, C) Kaplan-Meier plots for OS and RFS according to the different density of tumor-infiltrating CD8+ T cells. (D, E) Kaplan-Meier plots for OS and RFS according to the different density of tumor-infiltrating Tregs. (F–H) Comparison of tumor-infiltrating CD8+ T cell and Treg numbers within different N1, N2 and N1/N2 ratio groups. **P < 0.01, ***P < 0.001. IHC, immunohistochemistry; OS, overall survival; RFS, recurrence-free survival.
The correlation analysis revealed that higher tumor-associated N2 neutrophil infiltration was significantly associated with lower infiltration of CD8+ T cell (p<0.001) and higher Treg infiltration (p=0.003). However, no significant correlation was observed for the tumor-associated N1 neutrophils. Furthermore, higher N1/N2 ratios were associated with higher CD8+ T cell (p=0.001) and lower Treg (p<0.001) infiltration (table 2). Accordingly, in the low tumor-associated N1 neutrophil group, the median number of CD8+ T cells and Tregs in the TME was 26.7 (IQR 15.1–63.0) and 8.8 (IQR, 5.0–14.8), respectively, whereas that of the high tumor-associated N1 group was 34.0 (IQR 18.1–53.2, p=0.373) and 5.2 (IQR 2.3–13.8, p=0.058), respectively (figure 2F). Significant differences were observed between the low and high tumor-associated N2 neutrophil group in terms of the infiltration of CD8+ T cells in the TME (39.7 (IQR 21.2–66.7) vs 17.3 (IQR 12.7–26.7), p=0.002, figure 2G), and the median number of tumor-infiltrating Tregs was significantly lower in the low N2 group (5.3 (IQR 2.3–10.5) vs 14.3 (IQR 6.2–26.5), p<0.001, figure 2G). Moreover, the median count of tumor-infiltrating CD8+ T cells in the low N1/N2 group was 24.0 (IQR 13.3–48.0), which was lower than that of the high N1/N2 group (41.7, IQR 28.7–77.3, p=0.007, figure 2H), whereas the tumor-infiltrating Tregs numbers were higher (10.3 (IQR 5.0–19.7) vs 3.0 (IQR 1.7–6.0), p<0.001, figure 2H). Furthermore, the tumor-associated N1/N2 ratio was moderately correlated with the CD8/Treg ratio (Spearman’s r=0.515, p<0.001, online supplemental figure 2C) and mildly associated with the peripheral lymphocyte to neutrophil ratio (LNR) (Spearman’s r=−0.199, p=0.048, online supplemental figure 2D), while no significant correlations were observed between the peripheral LNR and tumor-infiltrating CD8+ T cells or Tregs alone (online supplemental figure 2E-F). Thus, tumor-associated N1/N2 neutrophil plasticity may potentially reflect the TME and immune escape.
Tumor-associated N1/N2 neutrophils as independent prognostic predictors of PDAC
Based on the primary cohort, patients with PDAC who had undergone radical resection were found to have a median OS and RFS of 21 and 15 months, respectively. There was an 83.1%, 33.8%, and 26.2% OS rate at 1, 3 and 5 years, respectively, while there was a 58.3%, 22.0%, and 17.3% RFS rate at 1, 3 and 5 years, respectively. Significant differences were observed in the median OS and RFS between the high tumor-associated N1 neutrophil group and the low tumor-associated N1 neutrophil group (OS: 37 vs 16 months, p<0.001, HR=0.250, 95% CI 0.136 to 0.459, figure 3A; RFS: 23 vs 9 months, p<0.001, HR=0.318, 95% CI 0.181 to 0.559, figure 3B). Accordingly, the median OS and RFS of the high tumor-associated N2 neutrophil group were statistically shorter than those of the low tumor-associated N2 neutrophil group (OS: 13 vs 30 months, p<0.001, HR=4.359, 95% CI 1.799 to 10.560, figure 3C; RFS: 9 vs 20 months, p<0.001, HR=3.498, 95% CI 1.616 to 7.570, figure 3D). When the N1/N2 ratio was compared for outcomes, remarkable distinctions were observed between the low and high N1/N2 groups (OS: 17 vs 78 months, p<0.001, HR=0.198, 95% CI 0.118 to 0.332, figure 3E; RFS: 10 vs 50 months, p<0.001, HR=0.229, 95% CI 0.142 to 0.369, figure 3F).

Survival analysis in the primary cohort in terms of the tumor-associated N1/N2 neutrophil plasticity. (A, B) Kaplan-Meier plots for OS and RFS according to the different density of tumor-infiltrating N1 neutrophils. (C, D) Kaplan-Meier plots for OS and RFS according to the different density of tumor-infiltrating N2 neutrophils. (E, F) Kaplan-Meier plots for OS and RFS according to the different level of N1/N2 ratio. OS, overall survival; RFS, recurrence-free survival.
The univariate Cox analysis demonstrated that N stage (p<0.001 and p<0.001, respectively), TMN stage (p<0.001 and p=0.001, respectively), perineural invasion (p=0.046 and p=0.026, respectively), tumor-associated N1 neutrophils (p<0.001 and p<0.001, respectively), tumor-associated N2 neutrophils (p<0.001 and p<0.001, respectively), tumor-infiltrating CD8+ T cells (p<0.001 and p<0.001, respectively), and tumor-infiltrating Tregs (p=0.001 and p<0.001, respectively) were significantly associated with OS and RFS (table 3). In addition, poor tumor differentiation was a risk factor for OS (p=0.036). The further multivariate Cox analysis revealed tumor-associated N1 neutrophils (p<0.001, HR=0.205, 95% CI 0.105 to 0.398 and p=0.001, HR= 0.376, 95% CI 0.207 to 0.683, respectively), tumor-associated N2 neutrophils (p=0.019, HR=2.215, 95% CI 1.142 to 4.296 and p=0.009, HR=2.236, 95% CI 1.219 to 4.099, respectively), tumor-infiltrating CD8+ T cells (p<0.001, HR=0.186, 95% CI 0.095 to 0.364 and p=0.001, HR=0.368, 95% CI 0.207 to 0.656, respectively) and tumor-infiltrating Tregs (p=0.041, HR=1.921, 95% CI 1.027 to 3.593 and p=0.042, HR=1.774, 95% CI 1.021 to 3.082, respectively) were all verified as independent prognostic indicators for OS and RFS (table 3). The AJCC N stage was also determined to be an independent risk feature for OS (p=0.026, HR=2.427, 95% CI 1.110 to 5.308).
Univariate and multivariate analysis of prognostic factors associated with overall survival and recurrence-free survival in the primary cohort
To further confirm the prognostic value of immune cells in the TME, univariate and multivariate analyses were reperformed using the tumor-infiltrating immune cells as continuous variables. As shown in online supplemental table 1, tumor-associated N1 neutrophils, tumor-associated N2 neutrophils, tumor-infiltrating Tregs, and CD8+ T cells were significantly associated with the OS and RFS in the univariate analysis of the primary cohort. A further multivariate Cox analysis indicated that tumor-associated N1 neutrophils (p<0.001, HR=0.877, 95% CI 0.833 to 0.924 and p<0.001, HR=0.906, 95% CI 0.869 to 0.938, respectively), tumor-associated N2 neutrophils (p=0.023, HR=1.030, 95% CI 1.004 to 1.057 and p=0.018, HR=1.026, 95% CI 1.004 to 1.048, respectively), and tumor-infiltrating Tregs (p=0.014, HR=1.032, 95% CI 1.006 to 1.059 and p=0.001, HR=1.043, 95% CI 1.018 to 1.070, respectively) were verified as independent prognostic indicators for OS and RFS, while tumor-infiltrating CD8+ T cells (p=0.025, HR=0.990, 95% CI 0.981 to 0.999) were identified as an independent prognostic factor for only OS.
Supplemental material
Validation of tumor-associated N1/N2 neutrophil plasticity along with immune infiltration and survival
In the validation cohort, tumor-infiltrating CD8+ T cells were found to be significantly correlated with tumor-associated N1 (p=0.010) and N2 (p=0.019) neutrophils, as well as the N1/N2 ratio (p=0.001). However, no significant differences were found between tumor-infiltrating Tregs and tumor-associated N1 (p=0.071) or N2 (p=0.119) neutrophils, or N1/N2 ratio (p=0.089), although there was a potential correlation among them (online supplemental table 2). According to the further analysis, the median number of CD8+ T cells in the high tumor-associated N1 neutrophil group was higher (29.3 (IQR 21.3–35.2) vs 15.3 (IQR 6.5–20.6), p=0.001, online supplemental figure 3A), while tumor-infiltrating Tregs displayed no significant differences (8.7 (IQR 7.0–15.7) vs 13.7 (IQR 9.2–19.4), p=0.223, online supplemental figure 3A). In addition, similar results were found by analyzing the tumor-associated N2 neutrophils (tumor-infiltrating CD8+ T cells: low group 29.3 (IQR 21.3–32.0) vs high group 12.2 (IQR 7.1–17.1), p<0.001; tumor-infiltrating Tregs: low group 8.6 (IQR 7.0–15.3) vs high group 14.7 (IQR 10.8–21.8), p=0.066, online supplemental figure 3B) and the N1/N2 ratio (tumor-infiltrating CD8+ T cells: low group 13.7 (IQR 7.1–20.4) vs high 29.7, IQR (26.0–38.3), p<0.001; tumor-infiltrating Tregs: low group 13.7 (IQR 8.3–20.3) vs high group 8.7 (IQR 7.0–15.3), p=0.162, online supplemental figure 3C).
Supplemental material
Supplemental material
The Kaplan-Meier curves were analyzed to determine the importance of tumor-associated N1/N2 neutrophil plasticity in validating the prognostic value of tumor-infiltrating CD8+ T cells and Tregs. The median OS did not differ significantly between the tumor-infiltrating CD8+ T cell groups (17 months vs not reached, p=0.106, HR=0.395, 95% CI 0.126 to 1.233, online supplemental figure 3D) nor between tumor-infiltrating Treg groups (not reached vs 20 months, p=0.058, HR=3.793, 95% CI 1.210 to 11.890, online supplemental figure 3E), respectively. Although, the median RFS for the high tumor-infiltrating CD8+ T cell group was significantly longer than that of the low group (not reached vs 9 months, p=0.005, HR=0.270, 95% CI 0.102 to 0.713, online supplemental figure 3F), while that of the high tumor-infiltrating Treg group was remarkably shorter (9 months vs not reached, p=0.003, HR=5.239, 95% CI 2.021 to 13.580, online supplemental figure 3G). Although the infiltration of CD8+ T cells and Tregs in the validation cohort were not proven to be significantly associated with OS, the CD8/Treg ratio was further validated, and it was found that the median OS and RFS of the patients in the high CD8/Treg ratio group were significantly longer than those in the low group (OS: not reached vs 20 months, p=0.017, HR=0.129, 95% CI 0.041 to 0.406, online supplemental figure 4A); RFS: not reached vs 9 months, p<0.001, HR=0.069, 95% CI 0.027 to 0.179, online supplemental figure 4B). Similarly, the tumor-associated N1/N2 ratio was moderately correlated with the CD8/Treg ratio (Spearman’s r=0.633, p<0.001, online supplemental figure 4C) and was associated with peripheral LNR (Spearman’s r=−0.376, p=0.044, online supplemental figure 4D), while no significant associations were observed between the peripheral LNR and the tumor-infiltrating CD8+ T cells or Tregs alone, as well (online supplemental figure 4E-F).
Supplemental material
The survival results of the validation cohort were consistent with those obtained from the primary cohort. As a result, the median OS and RFS of the high tumor-associated N1 neutrophil group were significantly longer than those of the low group (OS: not reached vs 16 months, p<0.001, HR=0.163, 95% CI 0.044 to 0.606, figure 4A; RFS: 20 vs 8 months, p=0.011, HR=0.328, 95% CI 0.105 to 1.023, figure 4B). In contrast, the median OS and RFS of the high tumor-associated N2 neutrophil group were significantly shorter than those of the low group (OS: 16 vs not reached months, p<0.001, HR=9.043, 95% CI 2.444 to 33.46, figure 4C; RFS: 8 vs 29 months, p<0.001, HR=5.513, 95% CI 1.701 to 17.870, figure 4D), while the median OS and RFS of the high N1/N2 ratio group were longer than the low group (OS: not reached vs 17 months, p<0.001, HR=0.150, 95% CI 0.044 to 0.509, figure 4E; RFS: 29 vs 8 months, p<0.001, HR=0.287, 95% CI 0.101 to 0.818, figure 4F).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival analysis in the validation cohort in terms of the tumor-associated N1/N2 neutrophil plasticity. (A, B) Kaplan-Meier plots for OS and RFS according to the different density of tumor-infiltrating N1 neutrophils. (C, D) Kaplan-Meier plots for OS and RFS according to the different density of tumor-infiltrating N2 neutrophils. (E, F) Kaplan-Meier plots for OS and RFS according to the different level of N1/N2 ratio. OS, overall survival; RFS, recurrence-free survival.
Furthermore, the univariate Cox analysis revealed that tumor-associated N1 neutrophils (p=0.002 and p=0.017, respectively), tumor-associated N2 neutrophils (p<0.001 and p<0.001, respectively), and tumor-infiltrating CD8+ T cells (p=0.083 and p=0.008, respectively) exerted significant prognostic effects on OS and RFS. Furthermore, the presence of tumor-associated N2 neutrophils was further confirmed as an independent risk indicator for both OS (p=0.019, HR=8.796, 95% CI 1.430 to 54.116) and RFS (p=0.036, HR=7.939, 95% CI 1.148 to 54.888) (online supplemental table 3), which may partially result from the dominant role played by tumor-associated N2 neutrophils and their limited volume in the validation cohort. Likewise, the univariate and multivariate analyses were reperformed using continuous tumor-infiltrating immune cell counts, and the results further validated the results of the categorical statistical analysis described above (online supplemental table 4). These validation studies indicate that tumor-associated N2 neutrophils may exert a dominant effect in the PDAC microenvironment, and support the general view that TANs promote tumor progression.
Supplemental material
Supplemental material
Discussion
Our study first investigated whether tumor-associated N1/N2 neutrophils in the PDAC microenvironment were plastic and evaluated their prognostic value. According to our study, tumor-associated N1/N2 neutrophils are independent prognostic predictors of PDAC, and are also associated with adverse clinicopathological characteristics. Furthermore, tumor-associated N1/N2 neutrophil plasticity may be a reflection of the TME and immune escape.
As it is well known, inflammation plays a vital role in the onset and progression of PDAC.24 As a crucial element of the innate immune system, TANs are implicated in promoting tumor formation and progression by inhibiting the adaptive immune response and assisting in tumor cell proliferation, extravasation, and metastasis.25 Recent studies have reported on the associations between neutrophils and prognosis in various cancers. However, most studies have focused on peripheral blood neutrophils rather than the TME. Both early and advanced solid tumors with elevated levels of NLRs have been reported to produce worse outcomes.22 26 Concomitantly, most of the research studies have shown that patients with higher TANs have worse outcomes in many cancers, such as esophageal cancers, head and neck cancers, and renal cell carcinoma.26 On the contrary, TANs can be considered as a favorable prognostic factor and a predictor of chemotherapeutic outcomes in a few studies.12 27 It has been reported that higher TANs are associated with worse OS in PDAC.9 28 29 In addition, NETs, similar to TANs, also functioned as independent prognostic indicators of PDAC.30 During recent years, studies have focused on the markers of TANs, as well as their complexity and inconsistent association with prognosis. A number of markers, including MPO, HE staining, CD66b, and CD15, can be used to identify TANs.31 MPO is present in the aniline blue granules of myeloid cells, neutrophils in particular, and is thus one of the most common markers used to identify neutrophils using IHC.32 33 CD11b in neutrophils is vital and indispensable for cell adhesion and transmigration via the activated endothelium and phagocytosis.34 Therefore, our study identified TANs through the co-localization of MPO and CD11b. Furthermore, the ‘M2-like’ function (N2) of TANs has been previously reported on.35 However, a marker of N2 neutrophils is yet to be identified. Therefore, there is a necessity to identify a suitable surface marker for N2, even if it may not be specific enough. The effective use of CD206 as a neutrophil marker has recently been reported, and its effect is similar to its distinctive properties in macrophages.23 36 In addition, we tried to divide the neutrophils into CD206- neutrophils and CD206+ neutrophils based on the MRC1 expression via the scRNA-seq based transcriptome analyses. The Gene Set Enrichment Analysis results showed that a strong enrichment of the extracellular matrix degradation pathway was found in the CD206+ neutrophils, while neutrophil degranulation, antigen processing cross presentation, defense response to bacterium and fungus, and inflammation-related pathways were significantly enriched in the CD206- neutrophils, which were in accordance with the functions of tumor-associated N1 and N2 reported previously (unpublished data). In this study, CD206 expression was evaluated in TANs and was proven to be suitable to distinguish between TANs with different prognostic effects, which demonstrated the plasticity of the tumor-associated N1/N2 neutrophils in the PDAC microenvironment.
Several studies have revealed that a number of cytokines are released by PDAC cells to recruit neutrophils, including growth factors, CXC family, CD200, and IL-1β.29 37 38 TANs are highly plastic and can adapt to different microenvironments depending on their phenotype.39 40 A study demonstrated that transforming growth factor-β (TGF-β) could polarize neutrophils into pro-tumorigenic phenotype (N2), while the blocking of TGF-β resulted in the accumulation of the anti-tumor phenotype (N1).14 We have previously reported on the abundance of the expression of TGF-β in PDAC,20 thus, it may be explained through our findings that tumor-associated N2 neutrophil counts were higher than that of tumor-associated N1 neutrophils. Meanwhile, patients in our study with lower N1/N2 ratios were found to have undergone easier lymph node metastases, perineural invasion, and to be of a higher TNM stage, which was consistent with previous findings that tumor-associated N2 neutrophils could promote metastases and angiogenesis via the release of reactive oxygen species (ROS), matrix metalloproteinases, oncostatin M, reactive nitrogen species, neutrophil elastase, and hepatocyte growth factor.41 42 Concomitantly, a lower N1/N2 ratio was also found to be associated with poor tumor differentiation, further supporting the findings of the study that showed that neutrophils preferred chemotaxis in undifferentiated pancreatic carcinomas.43
In our study, in terms of prognostic factors, tumor differentiation, AJCC N stage, TNM stage, and perineural invasion were confirmed to be correlated with OS or RFS in the primary cohort, which was consistent with the results of previous studies.44 45 However, only tumor-associated N1 neutrophils, tumor-associated N2 neutrophils, tumor-infiltrating Tregs, and tumor-infiltrating CD8+ T cells were identified as independent prognostic predictors of OS and RFS through the multivariate analysis, which may result from the significant relationships between tumor-associated N1/N2 neutrophils and these clinicopathological features. Here, the tumor-associated immune infiltration may indirectly and preferentially reflect the tumor malignant behavior and its invasive abilities, which is similar to the gene signature established by Kandimalla et al.46 However, only tumor-associated N2 neutrophils were significantly confirmed to be an independent predictor of OS and RFS in the small validation cohort, which may partially support the most recent studies on TANs with a protumorigenic function.31 47 Thus, we speculated that tumor-associated N2 neutrophils may play a dominant role in the PDAC microenvironment. Another reason for this phenomenon may be that N2 neutrophils have a longer lifespan and lower cytotoxicity than N1 neutrophils, while exerting strong immunosuppressive and tumor-promoting functions,48 including the release of a large amount of ARG-1 to suppress T cells in tumors.49 50
Balachandran et al51 have previously reported that the neoantigen qualities and CD8+ T-cell infiltration stratification can be used to predict the survival of PDAC patients. Greater densities of CD8+ T cells were found in the tumors of long-term survivors using the IHC and IF staining of the TMAs, which was consistent with our finding that patients in the high tumor-infiltrating CD8+ T cell group had a significantly longer survival. We also found that fewer CD8+ T cells and more Tregs had infiltrated into patients with a high proportion of N2 neutrophils or low N1/N2 ratio. Meanwhile, the correlation between the tumor-associated N1/N2 ratio and the CD8/Treg ratio was determined in this study. This is an interesting finding and this phenomenon may be caused by the crosstalk between tumor-infiltrating immune cells. As far as we know, tumor-associated N1 neutrophils can release certain pro-inflammatory and immunostimulatory cytokines to promote the recruitment of CD8+ T cells. Meanwhile, CD8+ cells and neutrophils have been reported to concomitantly infiltrate colorectal cancer cells, while TANs could enhance CD8+ T cell responsiveness, which may explain why the combined infiltration of neutrophils and CD8+ T cells resulted in better prognoses than CD8+ T cell infiltration alone.52 In contrast, immunosuppressive cytokines, such as TGF-β, which polarizes N2 neutrophils and IL-10, which are released by tumor cells and immune cells in PDAC, may be able to recruit Tregs.53
Our research mainly focused on the prognostic value of tumor-associated N1/N2 neutrophil plasticity in PDAC patients. In this study, we confirmed the potential role of CD206 in distinguishing between N1 and N2 in a clinical setting. The TANs were further divided into N1 and N2 subsets for further investigation and this would be an inevitable direction for future research. It is quite necessary to explore the different functions of the CD206+ and CD206- TANs. Meanwhile, the associations between tumor-associated N1/N2 neutrophil plasticity and the infiltration of CD8+ T cells and Tregs are intriguing and their underlying mechanisms warrant further study. Thereafter in our study, the plasticity of tumor-associated N1/N2 neutrophils was identified as an independent prognostic predictor, and its incorporation into TNM staging and other clinical features may provide a superior level of prognostic stratification for PDAC patients. Furthermore, several studies have revealed that TANs could mediate resistance to chemotherapy and immunotherapy, thus further investigations on the association between the plasticity of tumor-associated N1/N2 neutrophils and therapeutic responses would enable us to select better therapeutic strategies.
However, it is important to note that this study has certain limitations. First, this study is a retrospective and single-center study, which may weaken its universality. Although a small sample size validation cohort was used in this study, a large, prospective, and multicenter validation cohort will be required in further studies. Second, our study did not evaluate the mechanism by which TANs are polarized into N1/N2 neutrophils. Therefore, further experimental studies are necessary to uncover the mechanism of N1/N2 neutrophil polarization and their specific roles in PDAC. Third, the distinction between N1/N2 neutrophils using markers is yet to be elucidated, and further research is needed to explore other markers and rigorously validate the CD206 marker.
Conclusion
Taken together, our study demonstrates that N1/N2 neutrophils are associated with the retention of the plasticity of tumors, which reflects the TME and immune escape. Tumor-associated N1/N2 neutrophils are of significant prognostic values, while tumor-associated N2 may play a dominant role in the TME within PDAC. The exploration of neutrophil polarization and its correlation with clinical features in PDAC would significantly enhance our understanding of its pathophysiology and enable us to develop better treatment strategies.
Supplemental material
Data availability statement
Data are available on reasonable request. The data that support the findings of this study are available on request from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
Informed consent was obtained from all patients and the study protocol was authorized by the Ethics Committee of Zhongshan Hospital, Fudan University (No. B2020-346R).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors QC, HY, SL and SS: data acquisition, data analysis, statistical analysis, manuscript writing, manuscript review. ND, JZ, YJ, DW, TK, XX and JY: data acquisition, manuscript review. WW, WL: funding acquisition, data acquisition, manuscript review. NP: funding acquisition, data acquisition, statistical analysis, manuscript writing, manuscript review, guarantor.
Funding This study was funded by the National Natural Science Foundation of China (82103409), China Postdoctoral Science Foundation (2021M690037), Shanghai Sailing Program (21YF1407100), National Key R&D Program of China (2019YFC1315902), Youth Fund of Zhongshan Hospital Fudan University (LCBSHZX003), Health Science Popularization Project of Pancreatic Cancer of Zhongshan Hospital (ZX2021-002) and Shanghai ShenKang Hospital Development Centre Project (SHDC2020CR2017B).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.