Article Text

Abstract
Cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS) are severe, potentially life-threatening side effects of chimeric antigen receptor T-cell (CAR T) therapy caused by the release of cytokines by proliferating and activated CAR T-cells. Current mainstay treatment includes interleukin-1 and interleukin-6 (IL-6) blockade and steroids. The use of steroids is still controversial, since they may have the potential to irreversibly damage CAR T-cells and thus increase the risk of relapse. Therefore, additional treatment options need to be explored. We report the successful treatment of a patient with a grade 3 CRS and grade 4 ICANS refractory to IL-6 blockade and steroids with the tyrosine kinase inhibitor dasatinib. The use of dasatinib for treatment of CAR T-cell therapy-related severe complications warrants further studies.
- Case Reports
- Cytokines
- Adjuvants, Pharmaceutic
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Chimeric antigen receptor T-cell (CAR T) therapy is an established and effective option in the treatment of lymphoid malignancies. In adults and children with B-cell malignancies, anti-CD19 directed CAR T-cell therapy showed high response rates.1 In relapsed or refractory multiple myeloma, BCMA-targeted CAR T-cells demonstrated promising results in heavily pretreated patients.2
However, CAR T-cell therapy may have severe adverse events. Common and potentially life-threatening side effects are immune effector cell-associated neurotoxicity syndrome (ICANS) and cytokine release syndrome (CRS), latter caused by CAR T-cell activation and the release of various proinflammatory cytokines.3 Interleukin-6 (IL-6), along with other cytokines such as Interleukin-1 (IL1), plays an important role in the pathogenesis of CRS; therefore, anti-IL-6 receptor/anti-IL-6 agents such as tocilizumab/siltuximab or anti-IL-1 receptor agents such as anakinra were introduced for the treatment of CRS.4 5
In patients with worsening, severe CRS despite treatment with anti-IL-6 agents steroids are added.3 Studies have shown that early use of corticosteroids can reduce the incidence of severe CRS and ICANS and eventually reduce the cumulative steroid dose.6 On the other hand, earlier and higher use of corticosteroids may impair CAR T-cell function and thus increase the risk of disease relapse.7 Therefore, additional treatment options need to be explored.
Dasatinib is a tyrosine kinase-inhibitor and inhibitor of the breakpoint cluster region abelson murine leukemia viral oncogene homolog 1 (BCR-ABL) fusion protein and approved in the treatment of chronic myelogenous leukemia and Philadelphia chromosome positive acute lymphoblastic leukemia.
Mouse models and in vitro experiments have demonstrated that dasatinib induces in CAR T-cells a reversible inactive state from which they recover immediately on dasatinib withdrawal.8 9
It has been shown that transient rest of CAR T-cells can suppress CAR T-cell-induced cytotoxicity, cytokine production, and cell proliferation. In mice, dasatinib administration thereby counteracted the development of severe CRS.8 9 In addition, dasatinib can protect CAR T-cells from exhaustion by putting the cells in this temporary off state and then reactivating them.10 This unique property makes dasatinib a promising therapeutic option for the treatment of CRS and ICANS, although this has not been investigated so far.
We present a patient in their late 60s with relapsed diffuse large B-cell lymphoma (DLBCL) not otherwise specified (NOS), germinal centre B-cell like (GCB type), Lugano stage IV, without CNS involvement. Tisagenlecleucel (3.9×108 CAR positive viable T-cells, 0.18 transgene copies/cell, 80% cell viability, 13.9% CAR positive viable cells by flow cytometry) was administered after lymphodepleting chemotherapy with fludarabine 25 mg/m2 (day -4 to day -2) and bendamustine 90 mg/m2 (day -4 to day -3). At the start of lymphocyte-depleting chemotherapy, DLBCL was clearly progressive with extensive bone marrow infiltration but still no CNS involvement. No infection was detected at the time of infusion. CRP was 19.5 mg/L (normal range <10 mg/L) and ferritin was 2598 μg/L (normal range 30–300 μg/L) before therapy.
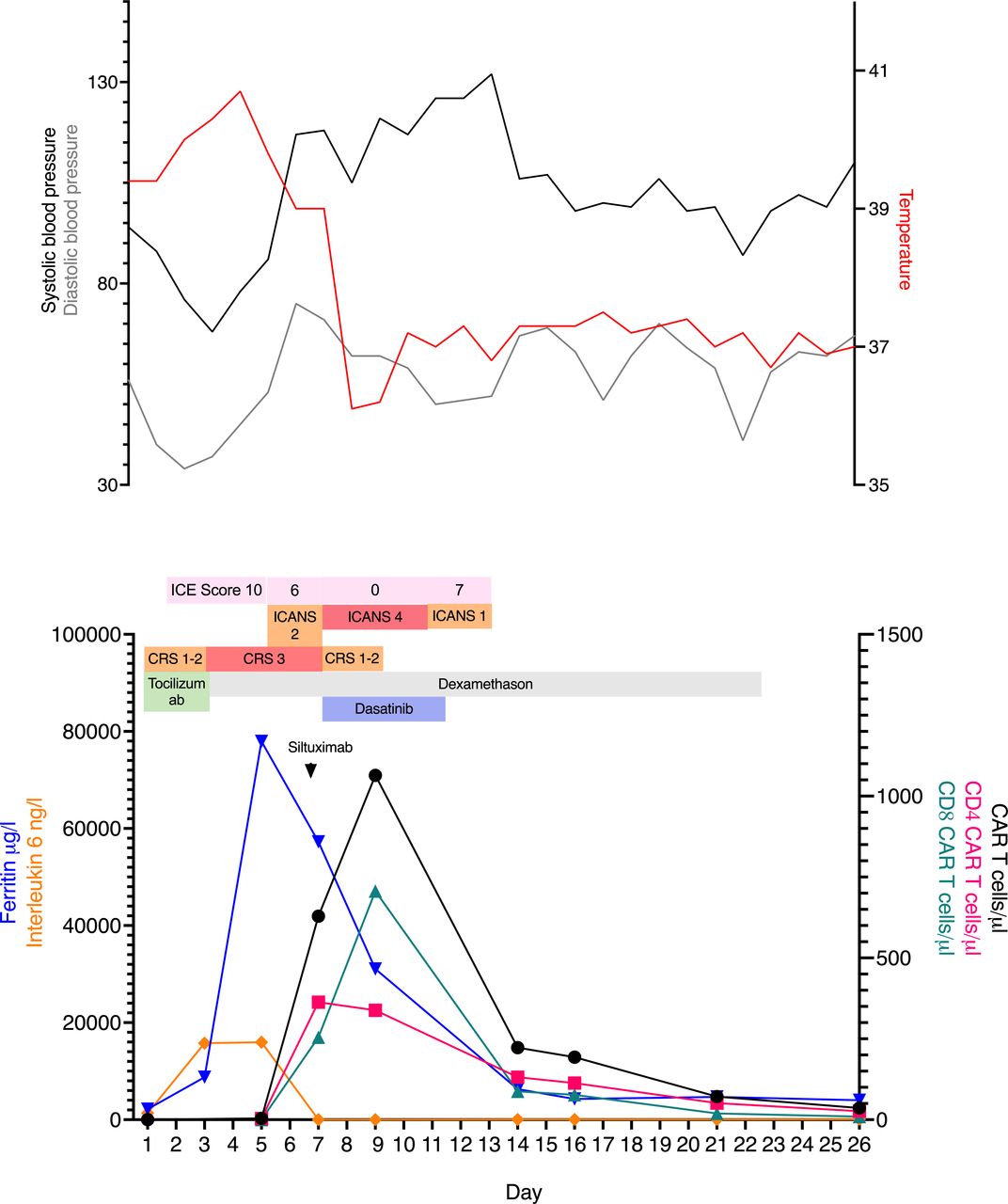
On the same day of CAR T-cell infusion, the patient developed fever of 38.1°C and required a fluid bolus to stabilize blood pressure (CRS grade 2). Tocilizumab (8 mg/kg, 700 mg) was immediately administered. Despite continuous fluid administration, the patient remained hypotensive and showed respiratory deterioration. He was transferred to the intensive care unit on day 3 because of CRS grade 3. In addition to four further doses of tocilizumab, continuous treatment with dexamethasone intravenously (40 mg/day, days 3–4, 80 mg/day, days 5–8) was started. Inflammatory markers increased rapidly over the next few days, with a maximum of 77,945 μg/L for ferritin and 15,777 ng/L (normal range <7 ng/L) for IL-6 on day 5. On day 6, one dose of siltuximab, a monoclonal antibody against IL-6, was added, however, his clinical condition further deteriorated.
The CAR T-cells, measured by flow cytometry, using a PE-Labeled Human CD19 (20-291) Protein, Fc Tag (Cat. No. AMS.CD9-HP254, Amsbio, Abington, UK), together with a backbone of antibodies for T-cell identification (CD3 FITC, CD2 PE-Cy7, CD56 APC, CD8 APC-H7, CD4 V450, CD45 V500, all from Becton Dickinson, Franklin Lakes, New Jersey, USA) and 7-AAD (Becton Dickinson, Franklin Lakes, New Jersey, USA) for live/dead staining, expanded rapidly to a maximum of 1064 cells/µL on day 9, CD4/CD8 ratio 0.47.
Despite early and aggressive management of CRS, the patient’s condition worsened. He developed hallucinations, sensory aphasia, apraxia, and disorders of consciousness corresponding to an ICANS grade 4. On day 7, he suffered a generalized seizure requiring protective intubation and anticonvulsant medication with levetiracetam. A cerebrospinal fluid puncture was not performed at that time due to severe thrombocytopenia and overt disseminated intravascular coagulation. At this time, we decided to add dasatinib. Dasatinib was administered at a dose of 100 mg/day for 7 days (days 7–13) via a nasogastric tube. Consent for off-label treatment was obtained from family members.
In the further course, body temperature returned normal within 48 h hours after initiation of dasatinib. Continuous venovenous hemadiafiltration, initiated for oliguria on the same day that dasatinib was started, was suspended 4 days later.
After rapid neurological improvement, the patient could be extubated already 1 day after the start of dasatinib treatment. Due to initial agitation as well as psychotic symptoms after extubation, anticonvulsant therapy was switched to lacosamide and medication with quetiapine was started.
On day 13 (7 days after initiation of dasatinib), the patient could be transferred to the normal ward with 2 L oxygen requirement and in an awake and adequate neurological state. There was no rebound of CRS or ICANS after discontinuation of dasatinib and no further administration of tocilizumab or siltuximab was required. Dexamethasone was discontinued on day 23. Overall, the patient received a cumulative dose of 602 mg dexamethasone over 21 days (40 mg/day, days 3–4, 80 mg/day, days 5–8, 40 mg/day, days 9–12, 10 mg/day, days 13–14, 8 mg/day, day 15, 4 mg/day, day 16, 2 mg/day, days 17–19, 1 mg/day, days 20–23).
Although the inflammatory parameters such as ferritin and IL-6 already decreased on day 5 under therapy with steroids and tocilizumab, significant clinical improvement of CRS and ICANS occurred only after administration of dasatinib.
After initiation of dasatinib treatment on day 7, CAR T-cells initially continued to increase until they peaked on day 9; thereafter, CAR T cell expansion declined markedly (figure 1). In contrast to the published data from in vitro and mouse experiments, we could not observe a renewed CAR T-cell expansion after discontinuation of dasatinib.8 9 The timing of dasatinib initiation could be a possible explanation. One may speculate, if CAR T-cell peak expansion was already achieved after starting dasatinib. In their mouse experiments, Mestermann et al administered dasatinib between days 3 and 5 after CAR T-cell infusion.9 Moreover, in the Juliet study, CAR-T cell expansion peaked as early as day 9.1
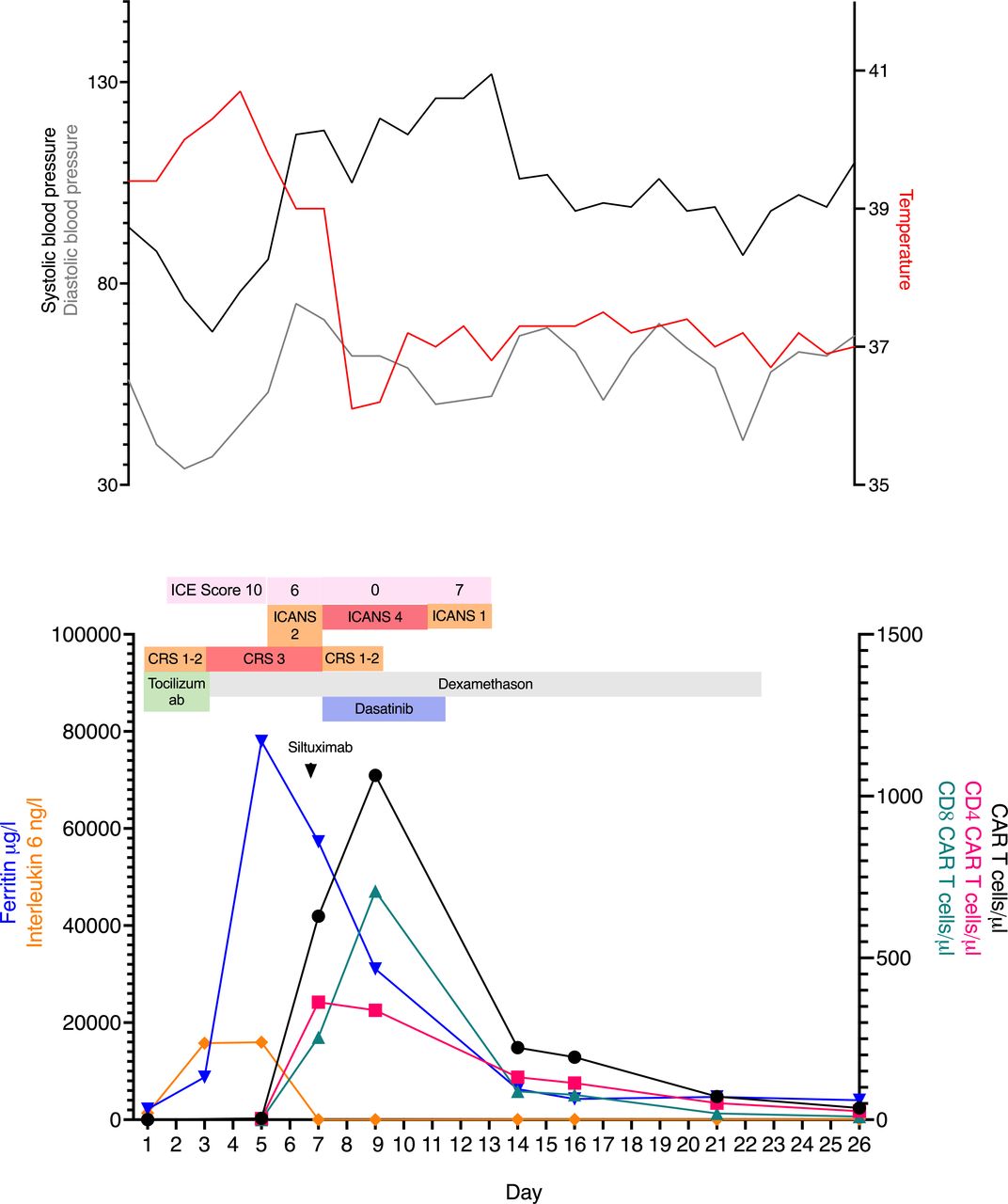
Course of CAR T-cell expansion during treatment with dasatinib. Clinical course, selected laboratory parameters and CAR T-cell expansion in the first 26 days after CAR T-cell infusion. The upper graph shows the changes in body temperature and systolic and diastolic blood pressure after infusion; the red line shows the maximum temperature, the black line shows the minimum systolic blood pressure, and the gray line indicates the minimum diastolic blood pressure per day. The graphic below shows the course of the inflammatory markers (ferritin and interleukin-6) as well as the course of the CAR T-cells and the interventions. Dexamethasone treatment was started on day 3 and tapered over 23 days. Five doses of tocilizumab were administered between days 1 and 4, and siltuximab on day 6. Dasatinib was administered from day 7 to day 13. The CAR T-cells were measured by flow cytometry and given as absolute values (cells/μL). CAR T, Chimeric antigen receptor T-cell; CRS, cytokine release syndrome; ICANS, immune effector cell-associated neurotoxicity syndrome; ICE, immune effector cell encephalopathy.
In addition, we have only quantitative CAR T-cell measurements and no qualitative measurements of CAR T-cell function after discontinuation of dasatinib. Nevertheless, 1 month after infusion the patient showed complete remission of the lymphoma according to the PET scan. He is currently in an ongoing remission more than 2 years after CAR T-cell infusion, suggesting a preserved function of the remaining CAR T-cells after treatment with dasatinib.
In addition, more than 2 years after infusion, we are still able to detect CAR T-cells in the patient’s blood (2.22 cells/µL after 3 months, 1.56 cells/µL after 6 months and 1.46 cells/µL after 9 months, 0.2 cells/µL after 2 years; sensitivity of the assay: 0.1% of CD3+T cells).
The patient developed very severe, prolonged cytopenias, which were probably caused by the high tumor burden with marked bone marrow infiltration at the time of CAR T-cell infusion, as well as the severity of ICANS and CRS (figure 2). However, the CAR-HEMATOTOX score prior to CAR T-cell infusion was already 2 points, which is associated with an increased risk for the incidence as well as a longer duration of cytopenia.

{kind=link}
{kind=link}
Long-term outcome after CAR T-cell therapy. Course of cytopenias as well as CAR T-cell expansion over the first 5months after CAR T-cell infusion. Red line indicates hemoglobin levels (g/L); purple line indicates platelets (G/l); blue line indicates absolute neutrophil count (count/μL) and black lines represents CAR T-cell count (cells/μL). CAR T, Chimeric antigen receptor T-cell.
Repeated G-CSF administration was required for the first 6 months to treat severe neutropenia and the patient required regular platelet and red blood cell transfusions. In addition, the patient developed long-lasting B-cell aplasia, requiring regular immunoglobulin substitutions for up to 2 years.
To the best of our knowledge, this is the first clinical case describing the use of dasatinib for the treatment of severe CRS and ICANS. Therapy with dasatinib was well tolerated and no drug-related side effects or relevant interactions occurred. Despite prior treatment with various anti-inflammatory agents such as tocilizumab, siltuximab and steroids (figure 1), clinical improvement occurred only after initiation of therapy with dasatinib.
Despite the clear temporal relationship, we cannot conclusively determine whether the improvement was due to dasatinib alone, the additional anti-inflammatory agents, and/or the natural history.
In conclusion, dasatinib is a promising option for the treatment of severe CAR T-cell therapy-related toxicities and warrants further clinical applications and studies including more detailed cell analysis.
Ethics statements
Patient consent for publication
Footnotes
Contributors KB and AH collected and analyzed the data, and wrote the manuscript; KB designed the figures. JCD did measurement of the CART-cell expansion by flow cytometry. KB and AH wrote the manuscript. All authors contributed to the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.