Article Text

Abstract
Adoptive cell therapies (ACT) have demonstrated promise in the treatment of patients with cancer, leading to long-lasting responses and, in some cases, even cure. Technological advances have brought these individualized therapies closer to reality, establishing them as credible therapeutic option. However, to date, few efforts have been made to understand patients' experience during ACT trials. Patient-reported outcomes (PROs) and patient-reported outcome measures (PROMs), which are instruments used to report PROs, are increasingly being used in oncology to capture patients’ perspective, provide real-world data on treatment safety, and support decision-making processes, such as health economic decisions. Due to the inherent complexity of ACT, the inclusion of PROMs in this field remains limited. In this commentary, we discuss the benefit of capturing PROs in ACT trials, the challenges of PROM administration and collection, and we propose simple and actionable recommendations to promote their adoption in ACT trials.
- Clinical Trials as Topic
- Immunotherapy, Adoptive
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Patient-reported outcomes (PROs) such as health-related quality of life are essential in evaluating patients’ perspectives and experiences during oncological treatments. They reflect patients’ perceived benefits and harms of the provided intervention, which are not necessarily captured by other investigator-assessed endpoints. Both the American Society of Clinical Oncology and regulatory agencies such as the Food and Drug Administration and the European Medicines Agency formally include PROs among the parameters considered for the evaluation of the clinical value of anticancer treatments.1 Practice guidelines providing key recommendations on patients’ reported outcomes measurement (PROMs) during the continuum of clinical cancer care have been recently released by the European Society of Medical Oncology (ESMO).2 Nevertheless, PROs remain poorly investigated in phase I–II oncological clinical trials.2 3 Dose-limiting toxicity or grade 3/4 adverse events, traditionally based on the assessment and reporting by investigators, still represent the primary endpoints of early-phase trials. However, these assessments may not appropriately reflect the patient’s perception regarding the tolerability of the received treatment.
Adoptive cell therapies (ACT) are a category of advanced therapy medical products with the potential to revolutionize cancer treatment. These products can be autologous, made specifically for each patient from their own biological material, mostly in the case of T cells; or allogeneic, derived from healthy donors, as in the case of natural killer cells.4 The main types of T-cell therapies include chimeric antigen receptor therapy (CAR-T), T-cell receptor therapy (TCR-T), and tumor-infiltrating lymphocytes (TIL) therapy. Today, ACT constitutes the largest number of agents in development in the immuno-oncology field, with more than 1400 ongoing trials and a yearly increase of 30%.5
While CAR-T has already revolutionized the hematological field, research is ongoing to expand the success of ACT in solid tumors.
Interestingly, only 6.8 % of the recently published CAR-T trials investigated PROs as a primary or secondary outcome measure,6 and none of the TIL-ACT clinical trials in solid tumors included PROs as corollary endpoints. Indeed, much of academia’s and industry’s efforts to date have been aimed at shifting the cost-effectiveness balance of these therapies by understanding biological features of efficacy (cancer target identification, T-cell product characteristics, biomarkers of response, etc), improving the manufacturing pipeline, and scalability. Surprisingly, limited efforts have been directed to understand patients’ perspectives during cell-therapy trials.
Challenges in implementing PROMs in ACT trials
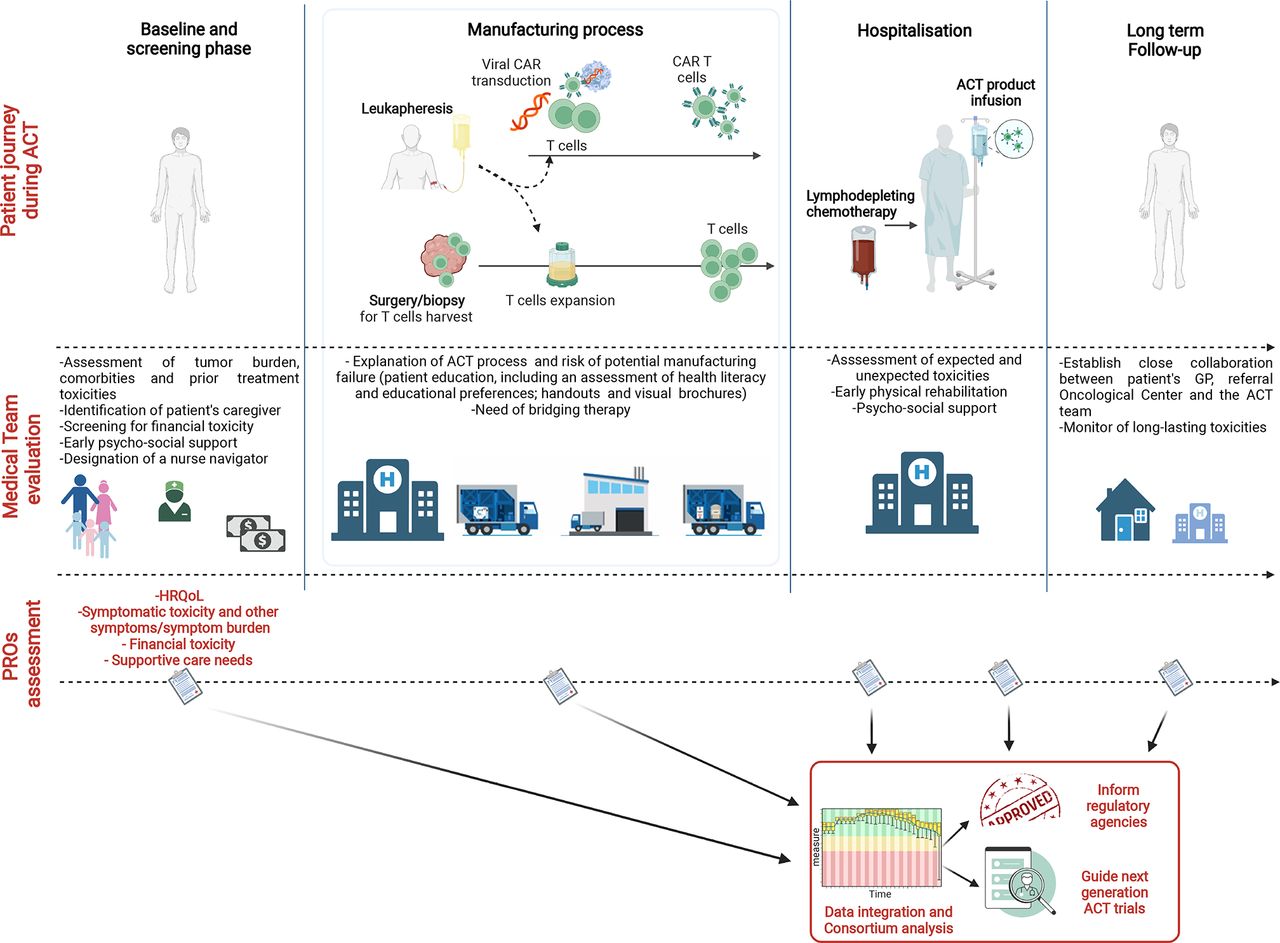
Due to the unique journey of patients enrolled in these trials, incorporating PROMs into ACT trials is challenging (figure 1). The ACT pipeline is a complex multistep process, requiring leukapheresis, biopsy or surgery for tumor harvest and TILs expansion, and still a long manufacturing and quality control period until the cell-therapy product is released and infused. This makes the ACT pipeline different from any other drug-based early-phase trials in relation to several aspects: (1) the need for repetitive medical and surgical procedures for biopsy collection; (2) the possible disease progression during the manufacturing window, necessitating additional bridging therapy; (3) the risk of cell-manufacturing pitfalls and eventually failure. All of these elements of uncertainty can increase patient distress and anxiety and should be assessed at baseline to detect changes or specific psychological needs throughout the entire process. Second, ACT patients frequently have advanced, heavily pretreated metastatic tumors. Indeed, the form of the underlying disease, tumor burden, pre-existing comorbidities, and cumulative toxicities from previous therapies should all be evaluated at the beginning of the ACT process and followed-up longitudinally. However, considering the lack of evidence regarding PROMs in this setting, it remains unclear whether generic, cancer, and/or symptom-specific PROMs may be used in these trials.

{kind=link}
Schematic representation of the patient journey during the adoptive cell-therapy process with key recommendations to capture patient-reported outcomes. Upper part: Patient journey through cell-therapy process. Middle part: Key recommendations for the clinical team to recognize and address the potential barriers early during the ACT process. Lower part: Key points that should be captured by patient-reported outcome measures longitudinally. ACT, adoptive cell therapies; CAR, chimeric antigen receptor; GP: general practitioner; HRQoL, health-related quality of life; PROs, patient-reported outcomes. Figure created with BioRender.com.
Third, ACT trials combine common toxicities (eg, lymphodepleting chemotherapy) with a unique spectrum of toxicities appearing during different time windows, such as capillary leak syndrome due to interleukin (IL)-2 administration (in case of TIL therapy), cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS) in case of TCR or CAR-T therapy,4 or more rarely, hemophagocytic lymphohistiocytosis and macrophage activation syndrome. The clinical assessment and grading of CRS, ICANS, and IL-2-related toxicity is established by international guidelines but patients’ perception of these toxicities is still undervalued.
Fourth, while several PROMs used in oncology trials have been recently applied to the CAR-T field (table 1), it is still difficult to draw conclusions on the selection of the appropriate PROMs tool and the ideal timing and frequency of PROMs administration due the highly heterogeneous nature of these trials and the low data availability.
Main PROMs used in clinical trials of hematologic and solid tumor
Unsurprisingly, the usage of PROMs in CAR-T trials is below the industry average of 27%.6 For these reasons, qualitative approaches could be initially used to understand the experience, specific needs and outcomes that are relevant to this patient population and their families. This will inform future investigations about the need for development or adaptation of the most relevant PROMs, together with the most suitable timing for administration.
Finally, combining clinical monitoring with PROMs collection following cell-therapy product administration may be important for collecting real-world data on both acute and long-term toxicities. For example, the monitoring of neurological toxicities along with the use of specific psychological questionnaires has been recently proposed as a strategy for an early detection of long-term consequences related to ICANS.7 This approach would allow not only the identification of patients at high risk but also guide early interventions and personalized follow-up strategies.
PROMs and ACT: cost-effectiveness balance and regulatory approvals
Implementing PROMs during ACT trials could also be important for patients and healthcare organizations to better understand their cost-effectiveness balances. Financial toxicity due to the high cost of ACT therapies could lead to emotional distress in patients and caregivers.8 Prices for approved ACT products can range from US$373,000 up to US$475,000, without accounting for additional procedures, such as leukapheresis, length of hospital stay, lymphodepleting chemotherapy, and management of toxicities. This out-of-pocket expenditure for patients might vary depending on different healthcare systems and insurance coverage. Screening for financial toxicity has been advocated in various countries through the use of validated PROMs instruments such as the COST (COmprehensive Score for financial Toxicity) in the USA or the PROFFIT (Patient Reported Outcome for Fighting FInancial Toxicity of cancer) in Italy.2 These measures should also be implemented in cell-therapy trials.
Finally, the international regulatory and health policy community is increasing its interest in the incorporation of PROs into the clinical decision-making process also to support regulatory review and reimbursement.1 PROMs could be incorporated into the real-world assessment of patient outcomes, which is important for the approval and reimbursement of cellular therapies in several countries. However, while the European Society for Blood and Marrow Transplantation has issued guidance for the construction of a post-approval registry to collect long-term toxicities from CAR-T recipients, no PROs data is currently collected in national registry.
Recommendation to address gaps
We recommend early and simple actions to eliminate barriers that could affect patients’ perspective during the ACT process, while in parallel, assessing PROs at different time points (figure 1). These include assessing the supportive care needs of the patient and family at the beginning of the process in order to provide targeted counseling, screening for financial toxicity, and offering prompt psychosocial assistance.9 A specific team member, such as a nurse navigator, may also be required to accompany the patient and his family, administer, review, and act on PROMs data, provide patient-education and supportive care, and improve communication between the patient and other clinical teams. Beyond the ethical and legal requirements of informed consent, a complete understanding of the complexities of the ACT journey (perhaps through the use of handouts and visual aids) is of the paramount importance.
The experience of caregivers in the ACT domain remains understudied. This population provides essential support for patients receiving ACT and may endure significant distress and have a decreased quality of life, increased depression and post-traumatic stress symptoms.10 Future research is needed on how to better support caregivers during ACT and to identify unmet caregiver needs.
Cell-therapy centers should work closely with the patient’s primary care physician and oncologists in referral centers to ensure adequate monitoring for potential long-term side effects that could be captured by PROMs at later time points.
We advocate that investigators, industry, and regulatory agencies enforce higher PROs data integration requirements in ACT trials. While we acknowledge that there are currently a variety of PROMs instruments and item libraries available, choosing the best PROMs and method for accurate assessment, interpretation and intervention necessitates an international consortium involving a variety of stakeholders, including patient representatives, clinicians, scientists, and policymakers. We do, however, recognize that patients may find it time-consuming and burdensome to complete comprehensive PROMs and repeat them at several time points. Similarly, convincing stakeholders and payers to invest in PROMs requires discussing the robust evidence that PROMs collection adds value in these trials.
In conclusion, ACT can potentially change the treatment of metastatic cancers with limited treatment options. However, they are also associated with substantial risks and psychological burden for patients and caregivers, with financial toxicity and present complex clinical and infrastructural challenges. Implementing PROMs in early-phase ACT trials is critical to understand patients’ and families’ perceptions of these innovative therapies of high potential but as-yet-uncertain efficacy.
Further research is needed to identify the needs of this population in order to select the most suitable PROMs and define the most appropriate time points to measure them. This will ultimately lead to improved clinical trial design incorporating PROMs as endpoints and substantially increasing the body of knowledge on the short-term and long-term outcomes of these therapies.
We are at the beginning of a cell-therapy revolution driven by technological advances in genomics, immunology, and manufacturing, allowing sophisticated and personalized treatments with the potential to be curative. It is now time to fill the gap between science, technology and patients’ perspectives.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Twitter @MMorotti, @sacola00
Contributors EG, MM, and MDM conceptualized the work. EG and MM researched data for the article. EG, MM, and SC-L contributed to writing early drafts of the paper. EG, MM, SC-L, ME, LT, GC, and MDM made substantial contributions to the discussion of the content of the article and edited the manuscript before submission. All authors revised and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests GC reports grants from Celgene, grants from Boehringer-Ingelheim, personal fees from Genentech, grants from Roche, personal fees from Roche, grants from BMS, personal fees from BMS, personal fees from AstraZeneca, grants from Iovance Therapeutics, grants from Kite Pharma, personal fees from NextCure, personal fees from Geneos Tx, and personal fees from Sanofi/Aventis. MDM received grants or contracts to his institution from Tesaro and GSK, consulting fees from Novartis, Roche, AstraZeneca, Merck Serono, Pfizer, Merck Sharp & Dohme, Janssen, Eisai, Takeda, Boehringer Ingelheim, Servier; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Novartis, Roche, AstraZeneca, Pfizer, Merck Sharp & Dohme, Janssen, Astellas, Boehringer Ingelheim; participation on a Data Safety Monitoring Board or Advisory Board for Merck Sharp & Dohme, Janssen, Astellas and Amgen. ME reports grants or contracts to her institution from Kaiku Health, Novartis, Roche, Vifor, BMS and Payment or honoraria for lectures, presentations from Roche, BMS and Vifor. The other authors have no conflict of interest to declare.
Provenance and peer review Not commissioned; externally peer reviewed.