Article Text

Abstract
Biomarkers for predicting response to anti-programmed death-1 (PD-1) immune checkpoint blockade (ICB) in non-small cell lung cancer (NSCLC) remain in demand. Since anti-tumor immune activation is a process, early dynamic changes of the acute-phase reactant C reactive protein (CRP) may serve as a predictive on-treatment biomarker. In a retrospective (N=105) and prospective (N=108) ICB-treated NSCLC cohort, early CRP kinetics were stratified after the start of immunotherapy until weeks 4, 6, and 12 as follows: an early doubling of baseline CRP followed by a drop below baseline (CRP flare-responder), a drop of at least 30% below baseline without prior flare (CRP responders), or those who remained as CRP non-responders. In our study, we observed characteristic longitudinal changes of serum CRP concentration after the initiation of ICB. In the prospective cohort, N=40 patients were defined as CRP non-responders, N=39 as CRP responders, and N=29 as CRP flare-responders with a median progression-free survival (PFS) of 2.4, 8.1, and 14.3 months, respectively, and overall survival (OS) of 6.6, 18.6, and 32.9 months (both log-rank p<0.001). Of note, CRP flare-responses, characterized by a sharp on-treatment CRP increase in the first weeks after therapy initiation, followed by a decrease of CRP serum level below baseline, predict ICB response as early as 4 weeks after therapy initiation. Of note, early CRP kinetics showed no predictive value for chemoimmunotherapy or when steroids were administered concurrently. On-treatment CRP kinetics had a predictive value for both major histological NSCLC subtypes, adenocarcinoma and squamous cell carcinoma. The results were verified in an independent retrospective cohort of 105 patients. In conclusion, CRP flare predicted anti-PD-1 monotherapy response and survival in two independent cohorts including a total of 213 patients with NSCLC, regardless of histology. Due to its wide clinical availability, early CRP kinetics could become an easily determined, cost-efficient, and non-invasive biomarker to predict response to checkpoint inhibitors in NSCLC within the first month.
- biomarkers, tumor
- immunotherapy
- lung neoplasms
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The treatment landscape for advanced non-small cell lung cancer (NSCLC) has been changing rapidly in recent years. The introduction of immunotherapy with blockade of the programmed death-1 (PD-1)/programmed death ligand-1 (PD-L1) axis (immune checkpoint blockade (ICB)) constituted a major breakthrough, prolonging survival and offering treatment options beyond cytostatic chemotherapy and targeted therapy. For the first time, long-term survival in metastatic NSCLC has been observed in a significant percentage of patients. However, not all patients benefit from ICB and immune-related adverse events (irAEs) can be life threatening.1 2
Robust predictive biomarkers are of great clinical interest to maintain the balance between potential irAE and therapeutic benefit.3 Since anti-tumor immune activation is a dynamic process, on-treatment inflammatory biomarkers such as acute-phase reactants have great potential to capture the precise tumor-immune interplay and might serve as accurate prediction tools.
Previous studies have demonstrated the use of different liquid biopsy-based biomarkers to predict ICB response in NSCLC and other tumors.4–6 An early increase in proinflammatory cytokines such as interleukin 6 (IL-6) or tumor necrosis factor α (TNF-α) after the onset of ICB correlated with response in NSCLC.4 After initiation of ICB treatment, characteristic longitudinal CRP kinetics were associated with response to anti-PD-1 monotherapy and combination therapy in two independent retrospective cohorts of metastatic renal cell carcinomas (RCCs), but without prospective validation.6 7 Patients were divided into three groups based on their on-treatment CRP levels as defined by Fukuda et al.6 ICB treatment was most effective in patients with a so-called CRP flare-response meaning an early CRP increase after ICB initiation (‘flare’) and a subsequent drop of serum CRP level below baseline. The early increase of proinflammatory cytokines, for example, IL-6 is the main stimulus for hepatic CRP production, after the onset of the antitumor immune response seems to be the immunological basis for this early CRP kinetics. Due to its broad availability and relatively low cost, CRP kinetics appears to be an excellent easy-to-implement biomarker to predict immunotherapy response. Here, we assessed whether early CRP kinetics predicts response to immunotherapy and treatment outcomes in NSCLC using a representative retrospective discovery and a prospective validation cohort, each including N>100 patients.
Materials and methods
Clinical sample collection
Two independent NSCLC cohorts receiving (chemo)immunotherapy were analyzed: Discovery Cohort: a retrospective cohort of patients with NSCLC treated at the University Medical Center Bonn (UKB) and Center for Integrated Oncology, Germany (CIO NSCLC, N=105). Inclusion into the retrospective CIO NSCLC cohort required measurement of CRP at baseline (maximum 30 days before first ICB application), at least once within 30 days after the start of ICB treatment and at the time of first staging or clinical progression. Validation Cohort: patients with NSCLC receiving anti-PD-1/PD-L1 treatment within the prospective immune monitoring of immune therapy study (IMIT NSCLC, N=108), which was conducted in four Swiss centers (Kantonsspital St Gallen, Spital Grabs, Spital Wil, and Spital Flawil) from July 1, 2016, to January 15, 2021.8 Response data according to RECIST criteria at first staging were available for N=88 patients. In both cohorts, relevant steroid comedication was defined as prednisolone 10 mg or equivalent dosage of other steroids. Patients who only received steroids as an antiemetic agent in combination with chemotherapy were not included in the ‘concurrent steroid medication’ subgroup.
Measuring serum parameters in blood samples
Baseline and longitudinal serum CRP concentrations were measured in accredited routine laboratories for both cohorts. A CRP value of above 5 mg/L was considered as elevated. For the validation cohort, lactate dehydrogenase (LDH) was measured in accredited routine laboratories, and values above 250 U/L were considered elevated.
Neutrophil-to-lymphocyte ratio
The neutrophil-to-lymphocyte ratio (NLR) was calculated on the basis of the differential blood count as neutrophils divided by lymphocytes. The median NLR of the IMIT NSCLC validation cohort was 4.7 and considered as the threshold for elevated NLR.
Definition of early CRP kinetics
Patients were classified according to the CRP kinetics definition as previously described.6 CRP flare-response was defined as at least twofold increase of baseline CRP within 30 days after ICB treatment followed by a decrease of serum CRP level below baseline. CRP response was defined as serum CRP level falling 30% below baseline within 12 weeks in at least one measurement. All other patients were classified as CRP non-responders. In an exploratory analysis, early CRP kinetics definition was applied at 4 or 6 weeks after initiation of immunotherapy in the prospective IMIT NSCLC validation cohort.
Statistical analysis
R studio (V.1.4.1106) using the ‘survminer’ package was used to perform statistical analyses. Kruskal–Wallis rank-sum test, Pearson’s χ2 test, and Fisher’s exact test were applied to perform intergroup comparisons. Progression was defined according to the RECIST V.1.1 criteria including death from any cause. Progression-free survival (PFS) and overall survival (OS) after ICB initiation were estimated by univariable Kaplan–Meier regression and tested with the log-rank test. Univariable and multivariable Cox regression analyses were performed to compare the prognostic value of early CRP kinetics (CRP flare-responders, CRP responders vs CRP non-responders) with baseline characteristics with respect to PFS and OS after ICB initiation. Variables were only included in multivariable Cox regression models if survival effects were significant in univariable analyses. All tests were two-sided, and p values <0.05 were considered significant.
Results
Retrospective CIO NSCLC discovery cohort
To determine the relevance of serum CRP kinetics for the efficacy of ICB in NSCLC, we retrospectively analyzed N=105 patients receiving (chemo)immunotherapy for advanced NSCLC at the UKB between 2005 and 2020. Using previously described criteria for serum CRP kinetics,6 we determined a CRP flare-response (twofold increase of baseline CRP within 30 days after ICB and drop of serum CRP below baseline within 12 weeks on-treatment) in 29.5% (N=31) of the patients, 39.0% (N=41) showed a CRP response (CRP level falling 30% below baseline at least once within 12 weeks on-treatment), and 31.4% (N=33) were classified as CRP non-responder (patients that did not meet the above-mentioned criteria) (online supplemental figure 1A). Among CRP non-responders, median PFS and OS were 2.6 and 11.8 months compared with 12.1 and 28.2 months for CRP responder and 9.2 and 21.5 months for CRP flare-responder (online supplemental figure 1B). Baseline characteristics were similar with regard to age, gender, and PD-L1 tumor proportion score (TPS) across all three CRP kinetics groups (online supplemental table 1). Results for univariable Cox regression are summarized in online supplemental table 2. In conclusion, the CRP (flare)-response in our discovery cohort was associated with prolonged PFS and OS in patients with NSCLC treated with ICB.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Prospective IMIT NSCLC validation cohort
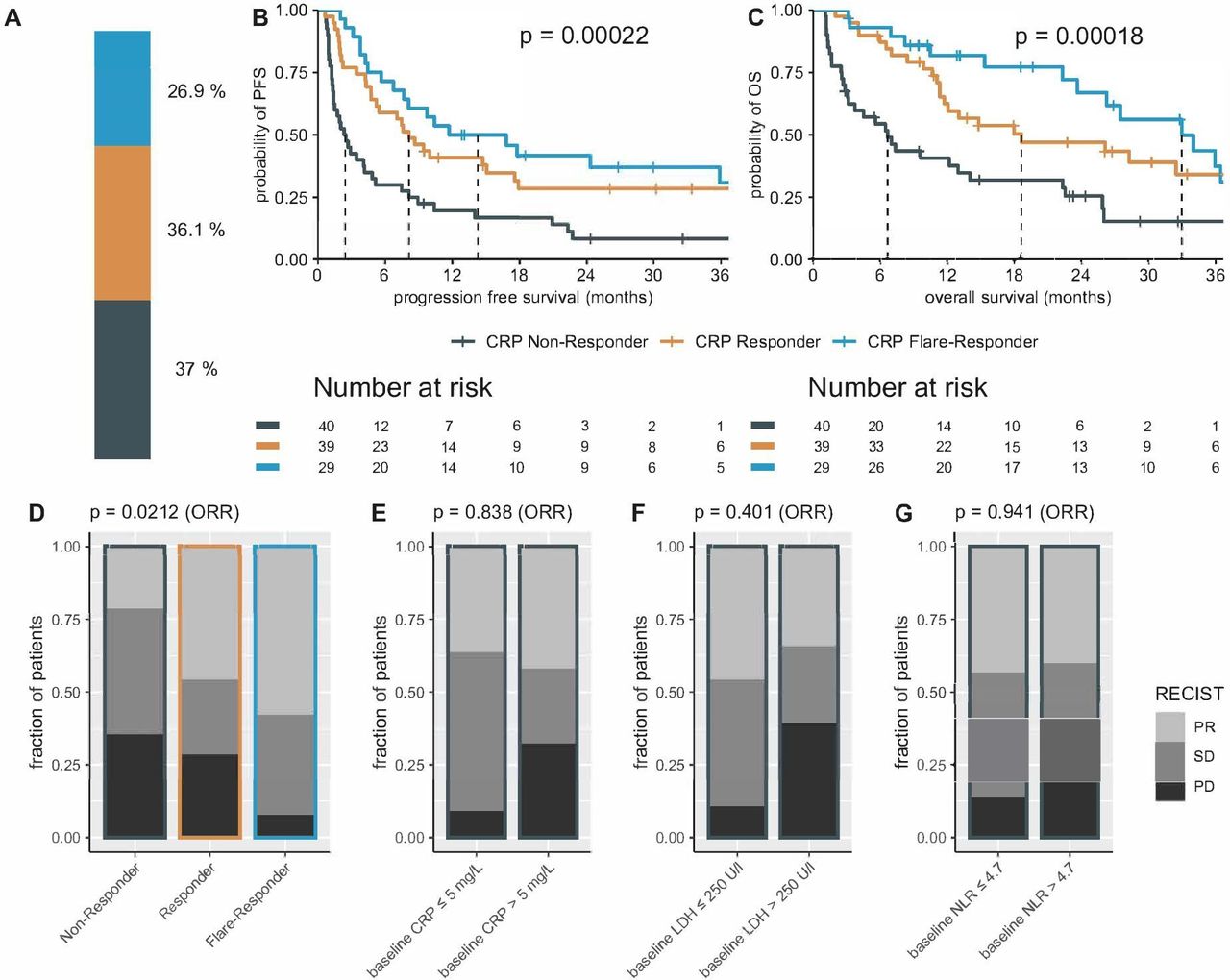
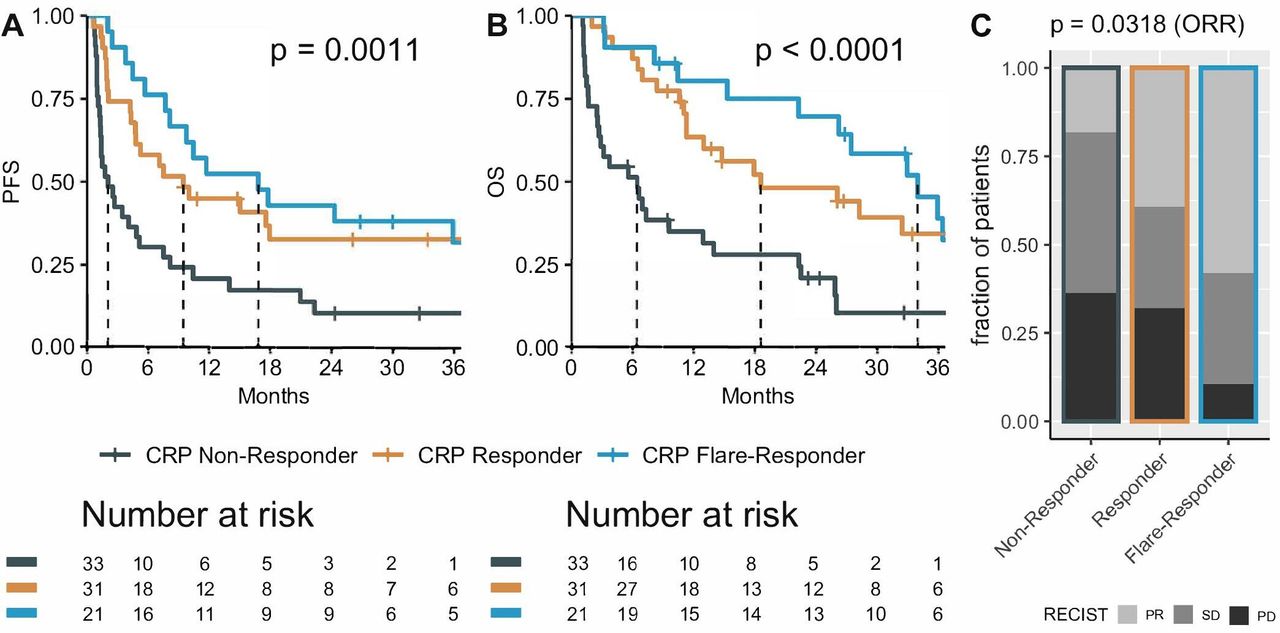
To validate our findings, we examined early CRP kinetics in N=108 patients with NSCLC (stage IIIb–IV) treated with ICB within the prospective IMIT observational study (baseline characteristics are shown in table 1). Similar to our discovery cohort, 37.0% (N=40) were classified as CRP non-responders, 36.1% (N=39) as CRP responder, and 26.9% (N=29) as CRP flare-responder (figure 1A). Median PFS for CRP non-responders, CRP responders, and CRP flare-responders was 2.4, 8.1, and 14.3 months; OS was 6.6, 18.6, and 32.9 months, respectively (figure 1B,C). Cox regression analyses showed that CRP flare-responders have a multivariable adjusted risk reduction of 78% (HR=0.22, 95% CI 0.10 to 0.48, p<0.001) for death compared with CRP non-responders (table 2). The objective response rate (ORR) differed significantly for the CRP kinetics groups and was 22.2% for CRP non-responders, 44.4% for CRP responders, and 60.0% for CRP flare-responders (figure 1D). In line with previous data,9 we could show that baseline CRP, LDH, and NLR have a prognostic value in ICB-treated patients with NSCLC, but of those, only baseline LDH remained a significant predictor of OS in multivariable Cox analysis (table 2). In addition, the static CRP, LDH, or NLR did not predict ORR at the first staging (figure 1E–G). Thus, our data obtained from two independent cohorts demonstrate that early CRP kinetics predicts immunotherapy response and is associated with improved survival in NSCLC.
Comparison of baseline parameters between CRP flare-responders, CRP responders, and CRP non-responders in the IMIT NSCLC validation cohort
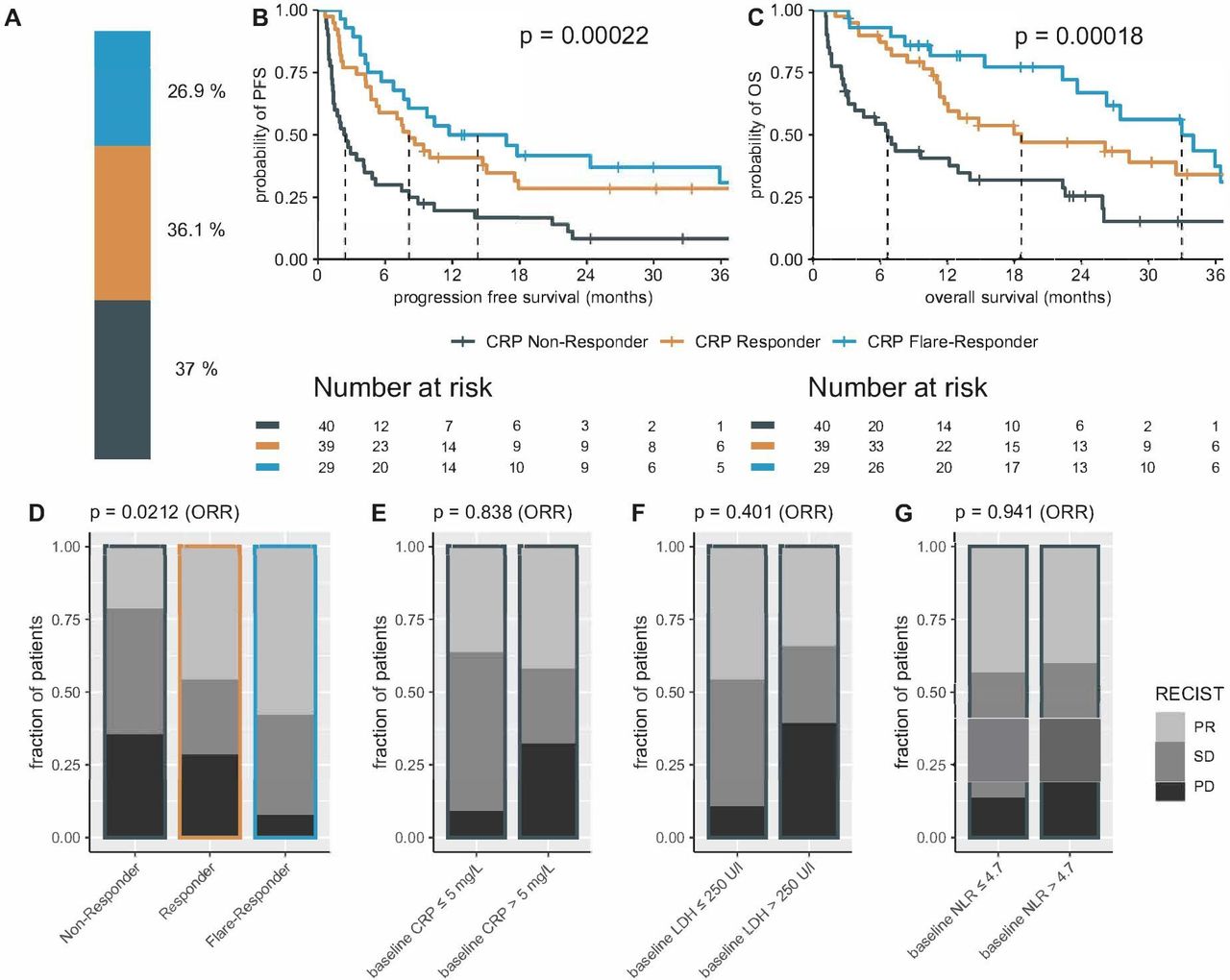
Distinct early on-treatment C reactive protein (CRP) kinetics correlates with progression-free survival (PFS) and overall survival (OS) in immune checkpoint blockade-treated patients with NSCLC. (A) The bar plot shows the frequency of patients categorized into three CRP kinetic subgroups in the immune monitoring of immune therapy NSCLC validation cohort. (B, C) Kaplan–Meier survival curves showing the PFS and OS after ICB initiation stratified according to CRP kinetics groups. Median PFS/OS is depicted as dotted lines. Distribution of response at first staging according to RECIST among the different CRP kinetics groups (D), as well as for patients with non-elevated or elevated CRP (E), lactate dehydrogenase (F), and neutrophil-to-lymphocyte ratio (G) at baseline. P values in (D–G) are calculated using the χ2 test for the objective response rate (ORR). NLR, neutrophil-to-lymphocyte ratio; NSCLC, non-small cell lung cancer; PD, progressive disease; PR, partial remission; SD, stable disease.
Univariable and multivariable Cox regression analysis regarding progression-free and overall survival after immunotherapy start in the IMIT NSCLC validation cohort
Association of early CRP kinetics with NSCLC histology
In both the discovery and the validation cohorts, early CRP kinetics were significantly associated with prolonged PFS and OS for the two major histological subtypes adenocarcinoma and squamous cell carcinoma (online supplemental figure 2).
Effect of concurrent chemotherapy and steroid medication on early CRP kinetics
Both the discovery and the validation cohorts included patients receiving anti-PD-1 monotherapy and chemoimmunotherapy in first or later lines (table 1 and online supplemental table 1). In our validation cohort, the predictive value of CRP kinetics was found to be independent of the line of therapy (online supplemental table 3). However, the impact of CRP flare-response was more pronounced in the first-line setting, with a ~90% risk reduction for progression and death compared with the CRP non-responders (online supplemental table 3). Most patients receiving chemoimmunotherapy were treated with a platinum-containing doublet chemotherapy and only a minority of N=8 patients in our discovery cohort received atezolizumab in combination with bevacizumab, carboplatin, and paclitaxel. Of note, in both cohorts early on-treatment CRP kinetics predicted ICB response, which was associated with PFS and OS solely in the patient subgroup without concurrent chemotherapy (figure 2, online supplemental tables 3 and 4). Furthermore, the predictive value of CRP kinetics was not evident in the patient subgroup with relevant concomitant steroid medication defined as prednisolone 10 mg or equivalent dose (online supplemental tables 3 and 4).
Supplemental material
Supplemental material

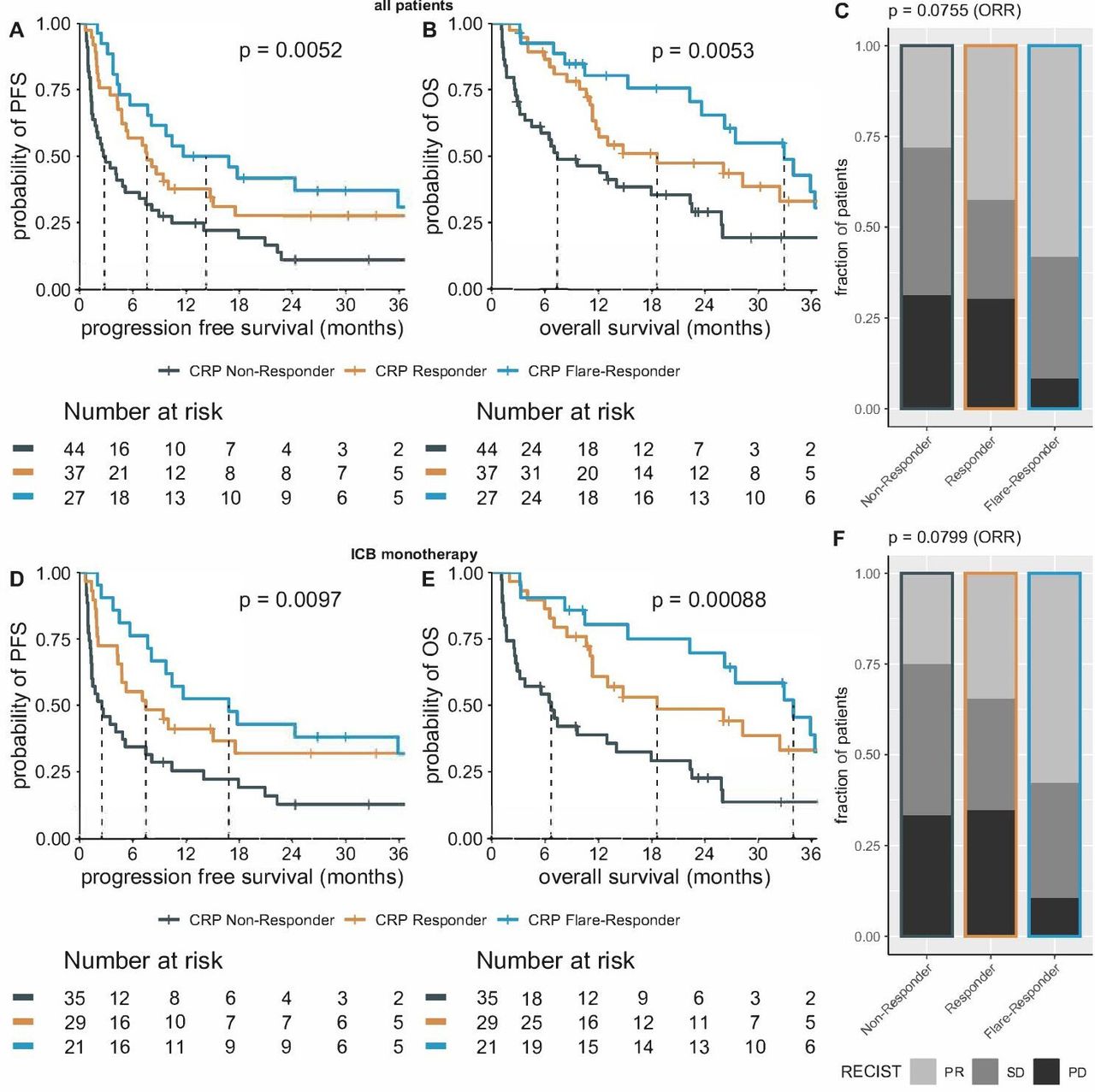
Early on-treatment CRP kinetics predicts treatment response and outcome of anti-PD-1 monotherapy. Kaplan–Meier survival curves showing the progression-free survival (PFS) (A) and overall survival (OS) (B) after immune checkpoint blockade initiation stratified according to CRP kinetics groups for the anti-PD-1 monotherapy subgroup of the immune monitoring of immune therapy non-small cell lung cancer validation cohort. (C) Distribution of response at first staging according to RECIST among the different CRP kinetics groups. p value based on χ2 test for ORR. CRP, C reactive protein; ORR, objective response rate; PD, progressive disease; PR, partial remission; SD, stable disease.
Early CRP kinetics predicts response to ICB at 4 weeks on-treatment
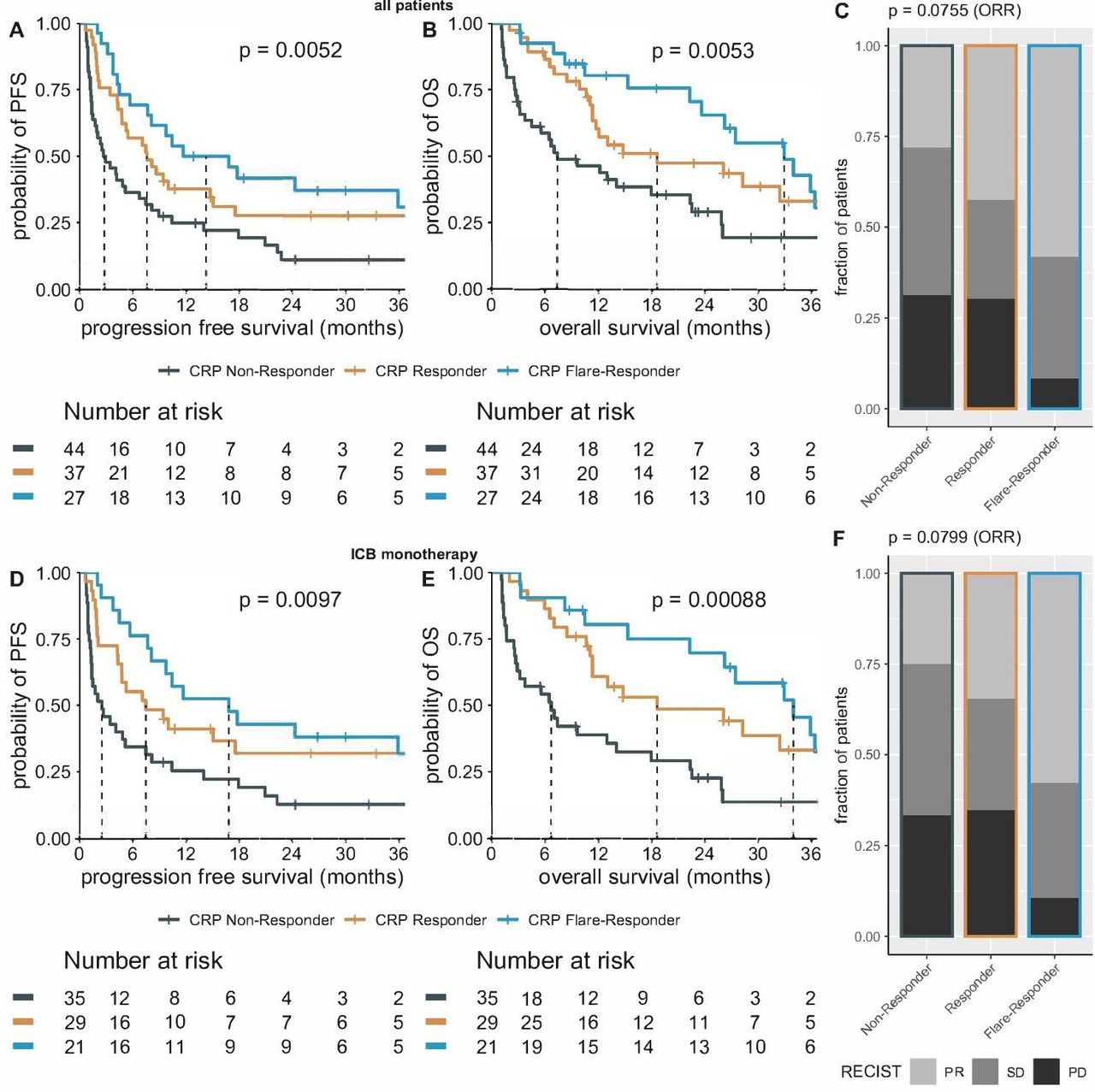
In the study protocol of our prospective validation cohort, CRP levels were measured at baseline and weeks 1, 2, 4, 6, 10 after the initiation of ICB, which allowed a more detailed analysis of early on-treatment CRP kinetics (figure 3). While the initial definition of CRP kinetics allows identification of responders or non-responders until the first radiological assessment after 12 weeks, individual CRP dynamics suggest that refined criteria may allow differentiation between responders and non-responders at an earlier stage. Indeed, two-third of the CRP flare-responders and >90% of the CRP responders could be correctly classified 4 weeks after the start of ICB therapy (figure 3B,C). After 6 weeks, >90% of CRP flare-responders had dropped below baseline CRP levels and thus met the criteria for a CRP flare-response (figure 3C). Of note, the predictive value of early CRP kinetics remained stable in both the overall cohort and the anti-PD-1 monotherapy subgroup when the definition was changed to an observation interval of 4 weeks (figure 4). Considering only the subgroup that received first-line anti-PD-1 monotherapy, early on-treatment CRP kinetics stratified until week 4 showed a strong association with outcome despite the relatively small subgroup (online supplemental figure 3). Since the majority of CRP (flare)-responders were already identified as early as 4 weeks on-treatment, while routine staging is usually performed after 12 weeks, a large therapeutic window (on anti-PD-1 monotherapy) opens for early response evaluation and the chance for therapy adjustments.
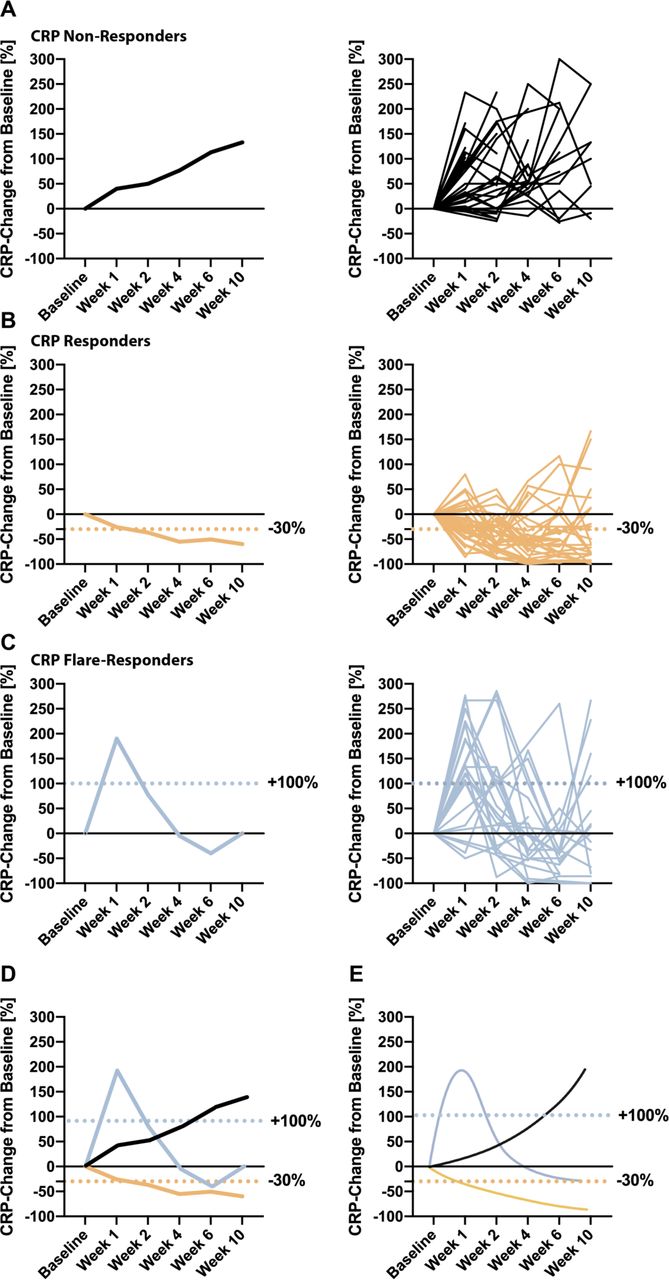
Longitudinal CRP changes from baseline after initiation of immunotherapy in the three early on-treatment CRP kinetics subgroups. (A) For CRP non-responders, (B) for CRP responders, and (C) for CRP flare-responders: median CRP change from baseline in per cent is shown in the left panel; the CRP changes of the individual patients are shown in the right panel. The dashed lines indicate the thresholds for CRP responder and CRP flare-responder subgroups. (D) Integration of median change in baseline CRP of the three CRP kinetics subgroups in the immune monitoring of immune therapy non-small cell lung cancer validation cohort and (E) conceptual representation of early on-treatment CRP kinetics. CRP, C reactive protein.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Refined early on-treatment CRP kinetics criteria lead to robust prediction of immunotherapy response in NSCLC as early as week 4. Application of early CRP kinetics definition until week 4 after immunotherapy start for all patients included in the immune monitoring of immune therapy NSCLC validation cohort (A, B) and the ICB monotherapy subgroup (D, E). Progression-free survival (PFS) after ICB initiation stratified according to CRP kinetics groups is depicted in A+D, overall survival (OS) in B+E. CRP kinetics stratification predicts response to ICB, but this does not reach statistical significance based on χ2 test for ORR (C, F). P value based on χ2 test for ORR. CRP, C reactive protein; ICB, immune checkpoint blockade; ORR, objective response rate; PD, progressive disease; PR, partial remission; SD, stable disease.
Discussion
In our study, in both a retrospective discovery and a prospective validation cohort, we were able to demonstrate that early CRP kinetics can robustly predict immunotherapy response in NSCLC regardless of histological subtype. Early on-treatment CRP kinetics is an easily determined cost-effective non-invasive biomarker for predicting response to immunotherapy as early as 4 weeks after therapy initiation and has the potential to optimize therapy monitoring. We therefore propose that evaluation of early CRP kinetics should be used as a standard-of-care tool for patients with NSCLC (both adenocarcinoma and squamous cell carcinoma) undergoing immunotherapy.
The original definition of CRP flare-response is based on a retrospective cohort of 42 patients with metastatic RCC and assumed a treatment interval of 3 months for ‘early’ CRP kinetics assessment.6 Using a retrospective discovery and prospective validation cohort including a total of 213 patients, we were able to demonstrate great predictive potential of CRP flare-response kinetics in ICB-treated patients with NSCLC. Furthermore, we were able to refine the definition of on-treatment CRP kinetics to an observation interval of 4 weeks, thus significantly increasing its clinical value for early therapy adjustments, for example, in the context of biomarker-stratified intervention studies. Our data suggest that early CRP kinetics is a biological cancer-independent phenomenon and thus, early CRP kinetics may represent an interesting tool for improved therapy monitoring in the era of immuno-oncology and warrants further investigation in other cancer types.
Currently, ICB is used as monotherapy or in combination with chemotherapy for metastatic NSCLC. In both cohorts, we found that early CRP kinetics predicted treatment response and outcome only in the setting of anti-PD-1 monotherapy without concurrent chemotherapy or steroid medication. This could be due to the immunomodulatory effect of concomitant chemotherapy or steroids. However, further studies are needed to clarify the role of early CRP kinetics in patients receiving chemoimmunotherapy or concomitant steroids. Recently, for the first-line treatment of metastatic RCC, we have shown that early CRP kinetics predicts response and is associated with improved PFS also for the immunotherapy combinations, anti-PD-1 either plus anti-CTLA-4 or tyrosine kinase inhibitor, suggesting that early CRP kinetics seems to be relevant not only for anti-PD-1 monotherapy.7
Further, within the framework of the prospective validation cohort, we were able to closely examine early CRP kinetics through the standardized study visits. Our data demonstrate that CRP kinetics can stratify patients as early as 4 weeks after the onset of ICB, a significant period before the first radiological assessment which is usually performed at week 8–12. The majority of CRP (flare)-responders can be correctly stratified at 4 weeks after immunotherapy start. This easy-to-implement on-treatment biomarker therefore opens a therapeutic window for earlier therapy adjustments. Of note, in patients who received first-line anti-PD-1 monotherapy, CRP kinetics showed a strong association with PFS and OS, even in a small subgroup of N=21 patients (online supplemental figure 3). Early CRP kinetics could thus identify the vulnerable CRP non-responder subgroup on (first-line) anti-PD1 monotherapy, who could benefit from early therapy switch or escalation, for example, in the context of biomarker-stratified studies, well before the first routine staging. We therefore suggest future CRP kinetics-stratified study protocols, which could lead to therapy escalation (eg, radiation, chemotherapy, additional ICB such as LAG3 or TIGIT, immune-activating drugs) in the CRP non-responder arm as early as 4 weeks after anti-PD-1/PD-L1 monotherapy. In addition to therapy escalation for CRP non-responders, therapy de-escalation, for example, early cessation of concomitant chemotherapy (for PD-L1 low/negative NSCLC) or drug holiday for CRP flare-responders, also seems a rational concept for this well-performing patient subgroup.
Anti-tumor immune infiltration after the start of immunotherapy can lead to pseudoprogression via inflammatory tissue edema with subsequent enlargement of the tumor lesions.10 11 CRP kinetics could potentially help to distinguish more accurately between true disease progression and pseudoprogression. However, a prospective radiological assessment using iRECIST criteria with simultaneous assessment of early CRP kinetics is required to address this hypothesis in the future.11
PD-L1 expression is the only widely used predictive biomarker in patients with NSCLC to date, although it has numerous limitations.3 We did not observe significant differences in PD-L1 TPS within our CRP subgroups. Importantly, early CRP kinetics can identify patients who will respond to ICB independent of the static tissue biomarker PD-L1. In our examined NSCLC cohorts, PD-L1 TPS had no prognostic value in univariable Cox regression models, and therefore, early CRP kinetics may even outperform static pretreatment PD-L1 expression in the future. If early on-treatment CRP kinetics would prospectively prove to be a more robust tool for evaluating immunotherapy response compared with PD-L1 expression in NSCLC or other tumor types, this would further emphasize its potential for future biomarker-stratified intervention studies.
Elevated CRP or LDH level at baseline has been correlated with inferior survival in NSCLC and other tumors, partially due to its role as a measure of tumor burden.9 12 We found that baseline CRP, LDH, and NLR had prognostic value in univariable Cox regression analysis, but none of them predicted objective immunotherapy response measured by RECIST (figure 1E–G, table 2). In multivariable Cox regression analysis, apart from early CRP kinetics, only baseline LDH remained a significant predictor for OS (table 2). Low NLR and early on-treatment reduction of NLR have recently been associated with prolonged survival in NSCLC and metastatic RCC under immunotherapy.13 14 Our data confirm this observation, but an early decline in NLR on ICB within the first month was not predictive of response to ICB in our prospective validation cohort (data not shown). Given the urgent need for a predictive biomarker for the response to immunotherapy, we propose to consider implementing early CRP kinetics into clinical practice, as it yields information about immunotherapy response instead of only being a prognostic parameter.
The immunological basis of our observed CRP kinetics is not clear. Immunogenicity of the tumor as well as immunological factors such as pre-existing shared tumor antigens of the individual patient might contribute to the observed CRP kinetics. Elucidating the molecular basis of this phenomenon will help to further improve our understanding of ICB response heterogeneity and develop rational strategies to overcome some shortcomings in the immuno-oncology era.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and the IMIT study protocol was approved by the Ethikkommission Ostschweiz. Reference #232/21. Participants gave informed consent to participate in the study before taking part.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @niklas_kluemper, @Doc_Bald
Contributors Concept and design: NK, LF, TB; acquisition, analysis, or interpretation of data: NK, JS; drafting of the manuscript: NK, JS, TB; critical revision of the manuscript for important intellectual content: all authors; statistical analysis: JS; administrative, technical, or material support: FB, CL, NW, AH, FGB, JE, PB, SD, MJ, MF, MR; supervision: MH, LF, TB.
Funding This study was supported by a Ferdinand Eisenberger grant of the Deutsche Gesellschaft für Urologie (German Society of Urology), grant ID KIN1/FE-19 (NK), and junior research group funding by the BONFOR Program of the Medical Faculty of the University of Bonn, grant ID 2020-2A-12 (NK). This study was funded in part by grant PP00P3_157448 from the Swiss National Science Foundation and by grant KLS-4409-02-2018 from the Swiss Cancer League (to LF). The study coordination of the IMIT NSCLC cohort was supported by a grant from the Forschungsförderung of the Kantonsspital St Gallen. MH and TB are funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) under Germany’s Excellence Strategy – EXC2151–390873048.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.