Article Text

Abstract
Purpose Bintrafusp alfa is a bifunctional agent consisting of an anti-human PD-L1 antibody linked to two TGFβRII. It is designed to act both as a checkpoint inhibitor and to ‘trap’ TGFβ in the tumor microenvironment. Phase I and II clinical studies demonstrated clinical activity in patients with a range of human papillomavirus (HPV)-associated cancers. The purpose of the studies reported here was the interrogation of various aspects of the peripheral immunome in patients with HPV-associated cancers, both prior to and early in the treatment regimen of bintrafusp alfa to better understand the mode of action of the agent and to help define which patients are more likely to benefit from bintrafusp alfa treatment.
Patients and methods The peripheral immunome of patients (n=65) with HPV+ malignancies was analyzed both prior to treatment with bintrafusp alfa and day 14 post-treatment for levels and changes in (1) 158 different immune cell subsets, (2) multiple plasma soluble factors including analytes reflecting immune stimulatory and inhibitory status, (3) complete blood counts, and in a subset of patients (4) TCR diversity and (5) HPV-specific T-cell responses.
Results Interrogation of the peripheral immunome prior to bintrafusp alfa treatment revealed several factors that associated with clinical response, including (1) higher levels of sCD27:sCD40L ratios, (2) lower levels of TGFβ1 and 12 additional factors associated with tumor mesenchymalization, and (3) higher CD8+ T cell:MDSC ratios. Analysis at 2 weeks post bintrafusp alfa revealed that eventual clinical responders had fewer increases in IL-8 levels and the neutrophil to lymphocyte ratio, and higher levels of HPV-16 specific CD8+ T cells. This study also provided information concerning differences in the peripheral immunome for patients who were naïve versus refractory to prior checkpoint inhibition therapy. While preliminary, two multivariate models developed predicted clinical benefit with 76%–91% accuracy.
Conclusions These studies add insight into the mechanism of action of bintrafusp alfa and provide evidence that the interrogation of both cellular and soluble components of the peripheral immunome of patients with HPV-associated malignancies, either prior to or early in the therapeutic regimen, can provide information as to which patients are more likely to benefit with bintrafusp alfa therapy.
- therapies, investigational
- biomarkers, tumor
- immunity
- immunotherapy
- immunoassay
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known
Tumor biopsies of metastatic lesions of patients with most solid tumors, such as those with human papillomavirus (HPV)-associated malignancies, are often not available or difficult to obtain, and define only one point in time in the evolution of a tumor mass or masses.
What this study adds
This study was undertaken to determine if analysis of the peripheral immunome would aid in determining which patients with HPV-associated malignancies would most likely benefit clinically from treatment with the novel immunotherapeutic agent anti-PDL1/TGFβRII, bintrafusp alfa. The results of the study demonstrate that interrogation of both cellular and soluble components of the peripheral immunome, either prior to therapy, or early in the therapeutic regimen, can help define which patients are most likely to benefit clinically.
Implications of this study
This study also provides further evidence to the field that, in addition to analysis of tumor biopsies, interrogation of the peripheral immunome can aid in defining the mechanism of action of a given immunotherapeutic and potentially provide valuable prognostic information.
Introduction
Bintrafusp alfa is a bifunctional agent consisting of a human IgG1 anti-PD-L1 antibody covalently linked to the extracellular domains of two transforming growth factor (TGF)-βRII.1–3 It is designed to bind to PD-L1 on tumor cells to act as a checkpoint inhibitor, and to escort TGFβRII to the tumor microenvironment (TME) and act as a ‘TGFβ trap.’ Numerous prior studies involving murine in-vitro and in-vivo models, human in-vitro studies, and studies in NSG-β2m−/− mice bearing human tumor xenografts and reconstituted with human peripheral blood mononuclear cells (PBMC), have investigated the various modes of action of this agent.1–10 These include: (1) reduction of TGFβ signaling in the TME via reduction of SMAD2 signaling,1 5 (2) reduction of regulatory T cell (Treg) immunosuppressive activity,3 (3) antibody-dependent cell cytotoxicity (ADCC) activity employing human natural killer (NK) effectors and human tumor cells,3 4 (4) alteration of tumor cell phenotype from a more invasive mesenchymal phenotype to a less invasive epithelial phenotype,2 (5) inhibition of tumor cell growth via interference of PD-1/PD-L1 interactions,1 5 and (6) activation of CD8+ and NK cells in the periphery and the TME.1 5 6
A phase I trial of bintrafusp alfa in 19 patients with advanced solid tumors showed preliminary evidence of clinical activity at the different dose levels tested, including one complete response (CR) and one near partial response (PR) in cervical cancer patients, two durable PRs in an anal cancer patient and a pancreatic cancer patient, and prolonged stable disease in two other patients.11 The maximum tolerable dose was not reached. The responses in the two cervical and the anal cancer patients were of interest since both tumor types are human papillomavirus (HPV) associated. Prior preclinical and genome-wide association studies, moreover, have shown a link between HPV-associated malignancies and the TGFβ pathway.12–15
Prior clinical studies in patients with HPV+ cancers employing the PD-1 inhibitors nivolumab and pembrolizumab demonstrated overall response rates (ORRs) from 12% to 24%.16–21 Pembrolizumab underwent accelerated FDA approval for PD-L1+ cervical cancer with an objective response rate of 14.6% (n=82).21 A recent clinical study employing bintrafusp alfa was conducted in patients (n=59) with HPV+ malignancies (cervical, head and neck, others) who were checkpoint treatment naïve.22 The confirmed objective response rate using RECIST criteria was 30.5% and included five CRs. Three patients had delayed PRs following initial progression, indicating a clinical response rate of 35.6%; eight patients had stable disease for a disease control rate of 44.1%. In light of the favorable response rates employing bintrafusp alfa versus prior studies using checkpoint inhibitors, we sought to better understand the mode of action of bintrafusp alfa in mediating tumor responses and control by interrogation of the peripheral immunome, both prior to, and early in the bintrafusp alfa therapeutic regimen. In addition to conventional analyses such as analyses of neutrophil to lymphocyte ratios (NLR) and plasma cytokines, evaluations included the interrogation of 158 immune cell subsets, and a range of plasma analytes reflecting immune stimulatory or suppressive activities. Any correlations with clinical benefit, either prior to therapy, or early in the therapy, were also evaluated.
The studies reported here provide preliminary evidence that the immune profile of patients prior to therapy associates with clinical response to bintrafusp alfa, and early changes in the peripheral immunome, that is, following one cycle of bintrafusp alfa and prior to restaging, also associate with clinical responses. Moreover, a distinct immune profile was seen prior to bintrafusp alfa therapy in patients who are checkpoint naïve vs checkpoint refractory. These and subsequent studies may provide a better understanding of the mode of action of bintrafusp alfa as well as aid in determining which patients may most benefit from bintrafusp alfa therapy.
Methods
Patients and collection of research samples
Immune parameters were evaluated in 65 patients with HPV-associated malignancies enrolled in an open label, multicenter phase 1 trial (NCT02517398), and an open-label, single center phase 2 trial (NCT03427411) of bintrafusp alfa (online supplemental figure 1 and tables 1,2). These patients had cervical (n=28), head and neck squamous cell carcinomas (H&N, n=18), anal (n=10), or rare (n=9) HPV-related tumors. Patients evaluated in the current study consisted of those who had either not received prior immune checkpoint inhibitors (ICI naïve, n=43), or had received and progressed on prior ICI therapy (ICI refractory, n=22). Each patient provided signed informed consent before study enrollment. For comparisons of immune parameters with clinical response, patients were classified as having clinical benefit from bintrafusp alfa (responders, R) if based on CT or MRI imaging they had a best overall response (BOR) of CR, PR, mixed response (MR), or stable disease (SD) for at least 4 months, and non-responders (NR) if they had a BOR of progressive disease (PD) after treatment with bintrafusp alfa. The clinical outcome of patients with HPV-associated cancers enrolled in NCT02517398 and NCT03427411 has been reported.11 22 Research bloods collected from patients at baseline and 2 weeks (after one cycle) and 6 weeks (after three cycles) after initiation of treatment of bintrafusp alfa therapy were evaluated in the current study. Complete blood counts (CBC) with differential were performed at the National Cancer Institute’s Center for Cancer Research, and NLR was subsequently calculated. For plasma assays, blood was collected in EDTA tubes, centrifuged, and stored at −80°C prior to analysis. For serum assays, blood was collected in serum separator tubes, centrifuged, and stored at −80°C prior to analysis. For the analysis of PBMCs, blood was collected in sodium heparin tubes and PBMCs were isolated after Ficoll-Hypaque density gradient separation. Cells were cryopreserved in 90% heat-inactivated human AB serum and 10% dimethyl sulfoxide at a concentration of 1×107 cells/mL prior to analysis.
Supplemental material
Plasma factors
Plasma levels of cytokine/soluble factors were evaluated in 64 patients with available samples, before and after bintrafusp alfa treatment, using commercially available kits per the manufacturers’ instruction. Interleukin (IL)-8 was measured by AlphaLISA (PerkinElmer, Waltham, Massachusetts, USA), soluble (s) CD27 (sCD27) and sCD40L were measured using Instant ELISA kits (Life Technologies, Carlsbad, California, USA), sPD-1, sPD-L1 and sCD73 were measured with ELISA kits from Abcam (Cambridge, UK), and TGFβ1, Granzyme B, and sCTLA4 were measured using ELISA kits from R&D Systems (Minneapolis, Minnesota, USA). Plasma samples from 62 patients prior to therapy were also analyzed using the Olink Target 96 Immuno-Oncology panel for biomarker discovery (Olink, Watertown, Massachusetts, USA). Levels of TGFβ1 were also determined in the serum of select patients.
Peripheral blood immune subsets
Cryopreserved PBMCs collected from 31 patients with available PBMCs before and after bintrafusp alfa therapy were examined by multicolor flow cytometry using 30 markers in 4 panels (online supplemental table 3) to identify 158 peripheral immune cell subsets,23 following methods previously described.24 25 Subsets evaluated included 10 parental cell types (CD4+ and CD8+ T cells, Tregs, NK cells, NK-T cells, conventional dendritic cells (cDCs), plasmacytoid dendritic cells (pDCs), B cells, myeloid-derived suppressor cells (MDSCs), and monocytes), and 148 refined subsets related to the maturation/function of the parental cell types. Flow cytometry files were acquired on an LSR Fortessa equipped with five lasers and analyzed using FlowJo V.9.9.6 for Macintosh, with nonviable cells excluded and negative gates based on fluorescence-minus-one controls. The frequency of all subsets was calculated as a percentage of PBMCs to eliminate any bias that might occur in the smaller populations with fluctuations in leukocyte subpopulations.
T-cell receptor repertoire analysis
DNA was isolated from cryopreserved PBMCs from 12 patients before and after 1 cycle of bintrafusp alfa using the Qiagen DNeasy Blood and Tissue Kit (Qiagen, Hilden, Germany). TCR Vβ CDR3 sequencing (TCRseq) at the deep resolution was performed at the NCI genomic core facility (Frederick, Maryland, USA) using the immunoSEQ platform (Adaptive Biotechnologies, Seattle, Washington, USA). Raw sequence reads were analyzed using the immunoSEQ ANALZER 3.0 (Adaptive Biotechnologies). Repertoire size, a measure of TCR diversity, was determined by calculating the number of individual clonotypes represented in the top 25th percentile ranked by molecule count, after sorting by abundance.
Antigen-specific T cell analysis
Tumor-associated antigen (TAA) specific T cells were analyzed in cryopreserved PBMCs isolated from 44 patients before and after bintrafusp alfa therapy, where sufficient samples were available. PBMCs were stimulated in vitro with overlapping 15-mer peptide pools encoding for HPV-16 E6 and E7 oncoproteins, as well as for HPV-18 E6 and E7, and MUC-1, and analyzed by intracellular cytokine staining using methods previously described.22 26 Peptide pools encoding for human leukocyte antigen (HLA) and CEFT (a mixture of peptides of cytomegalovirus, Epstein-Barr virus, influenza, and tetanus toxin) served as negative and positive controls, respectively. The absolute number of viable CD4+ or CD8+ T lymphocytes producing cytokine (interferon-γ (IFN-γ), tumor necrosis factor-α (TNFα), IL-2) or positive for a degranulation marker (CD107a) at the end of expansion was calculated per 1×106 cells plated at the start of the stimulation assay. This calculation takes into account not only the percentage but also the total number of viable antigen-specific T cells expanded in the stimulation assay. The background signal (obtained with the HLA peptide pool) and any value obtained prior to therapy were subtracted from those obtained after therapy ((post-TAA – post-HLA) – (pre-TAA – pre-HLA)). Following this calculation, a patient was scored as developing an antigen specific T-cell response if the patient had more than 250 CD4+ or CD8+ T cells that produced IFN-γ, TNFα, or IL-2 or were positive for CD107a per 1×106 cells, as well as a>2 fold increase in the number of positive cells post (vs pre) therapy. Multifunctional TAA responses, defined as CD4+ or CD8+ T cells expressing two or more of IFN-γ, TNFα, IL-2, or CD107a, were also quantified before and after bintrafusp alfa. The frequency of patients developing a >2 fold increase in multifunctional TAAs after vs before therapy was determined.
Statistical analysis
Statistical analyses were performed using GraphPad Prism (GraphPad Software, La Jolla, California, USA), RStudio (Boston, Massachusetts, USA), and SAS/STAT software V14.3 (SAS Institute, Inc., Cary, North Carolina, USA). Changes in immune parameters between two time points were assessed for statistical significance using a Wilcoxon signed-rank test. Immune parameters compared between patients who responded to treatment vs those who did not were assessed for the significance of the difference using a Mann-Whitney test. Binary measures were compared between two groups using Fisher’s exact test. All p values are two-tailed and reported without adjustment for multiple comparisons in this hypothesis generating study; p values <0.05 were considered statistically significant.
Logistic regression analyses were performed to determine if models could be generated based on levels of plasma analytes and CBCs to predict clinical response and overall survival. For this analysis, plasma analytes and CBC measures were available for 58 patients both at baseline and after one cycle (2 weeks) post bintrafusp alfa. Patients with a BOR of CR, PR, MR, or SD >4 months were compared with patients with a BOR of PD. Patients were divided into a training set (n=43) and a test set (n=15 patients, who were subsequently enrolled). Forward, backward, and all-possible-combination selection methods were used to detect two-factor and three-factor models from baseline and week 2 levels of 91 potential risk factors in the training set. Logarithmic transformations were applied to the factors as appropriate to reduce skewness prior to analysis. Receiver operating characteristic (ROC) curves were generated for models that showed strong associations between the response outcome and the individual risk factors in the training set, and the area under the curve (AUC) was evaluated for each. Data from the test set (n=15) were entered into these models with the parameters estimated from the training set. Logistic regression was similarly performed on logarithmic transformed plasma and CBC analytes obtained from patients at baseline only. For this analysis, data was available for 63 patients, and patients with an overall survival ≥180 days were compared with patients with an overall survival <180 days. Patients were randomized at a 2:1 ratio into a training set (n=42) and a test set (n=21). P values reported were not corrected for multiple comparisons.
Results
Differences in the immune profile of patients enrolled with different types of HPV-associated cancers
The current study evaluates the immune effects in the periphery of bintrafusp alfa treatment of patients with HPV-associated cancers, including patients with cervical (n=28), H&N (n=18), anal (n=10) and rare (n=9) carcinomas. We first evaluated whether there were differences in the immune profile of patients with cervical vs H&N cancers, which represented the two largest cohorts of patients enrolled. Differences noted at baseline, included (1) higher plasma levels of IL-12, CXCL5, and MCP3 (figure 1A), (2) greater absolute lymphocyte counts (ALC) (figure 1B), and (3) greater frequencies of naïve CD8+ T cells, and CD8+ T cells that express CD73 (figure 1C) in patients with cervical cancer compared with those with H&N cancer. CD73 is an immune checkpoint involved in adenosine metabolism. There were no significant differences, however, in the analyses of the major groupings of immune cell subsets, the other refined (n=158 total) immune cell subsets, or the other plasma analytes examined. Thus, patients with different HPV-related cancers were analyzed together in subsequent studies.

Differences at baseline in the immune profile of patients with cervical versus head and neck (H&N) cancer, and in patients with human papillomavirus (HPV)-associated cancers that are immune checkpoint inhibitor (ICI) naïve versus refractory. Levels of (A) plasma analytes (measured by Olink assay), (B) absolute lymphocyte count (ALC), and (C) refined immune cell subsets that were different between patients with cervical cancer (n=28) and H&N cancer (n=18). Levels of (D) plasma analytes, (E) absolute neutrophil counts (ANC), (F) classic peripheral blood mononuclear cells (PBMC) subsets, and (G) refined PBMC subsets that were different in patients who are ICI naïve and ICI refractory prior to treatment with bintrafusp alfa. Graphs display median frequency of analytes. Differences were defined by p<0.05 and >1.5 fold difference between cervical and H&N patients in A, and p<0.05 in B-G. P value was calculated using the Mann-Whitney test. For analyses of cervical vs H&N patients, plasma analytes were analyzed in n=45 (n=27 cervical, n=18 H&N), CBC measures in n=46 (n=28 cervical, n=18 H&N), and immune cell subsets in n=24 (n=15 cervical, n=9 H&N). For analyses of ICI naïve versus refractory patients, plasma cytokines/soluble factors were analyzed in n=64 (n=42 ICI naïve, n=22 ICI refractory), CBC measures in n=65 (n=43 ICI naïve, n=22 ICI refractory), and immune subsets in n=31 (n=14 ICI naïve, n=17 ICI refractory). CBC, complete blood counts; cDC, conventional dendritic cells; CM, central memory; CTLA4, cytotoxic T lymphocyte antigen 4; EM, effector memory; MDSC, myeloid derived suppressor cell; NK, natural killer cell; PD1, programmed death receptor 1; PDL1, programmed death receptor ligand 1; TCR, T-cell receptor.
Differences in the immune profile of patients who are ICI naïve vs ICI refractory
We next evaluated if differences existed in the immune profile of patients with HPV-associated cancers who had not received prior ICI (ICI naïve) versus those who had received and progressed on prior ICI therapy (ICI refractory). Compared with ICI naïve patients, ICI refractory patients had substantially elevated plasma levels of sPD-1, sCD73, and sCTLA4, all of which have been associated with immune suppression; lower levels of sCD27:sCD40L, which is indicative of immune activation, were also noted in ICI refractory patients (figure 1D). Evaluation of additional plasma analytes with Olink’s immuno-oncology panel revealed nine additional factors (PDCD1, PDL1, FGF2, CXCL9, CXCL10, CCL20, NOS3, MMP12, and MUC16) that were also elevated in ICI refractory compared with ICI naïve patients (figure 2A). Using unsupervised clustering, most ICI refractory patients clustered together and apart from those patients who were ICI naïve (figure 2B). A number of immune cell differences were also noted between these two cohorts of patients; ICI refractory patients had a higher absolute neutrophil count (ANC, figure 1E), and among classic PBMC cell types, had lower levels of CD4+ T cells, and higher levels of cDCs, MDSCs, and monocytes, than ICI naïve patients (figure 1F). Compared with ICI naïve patients, ICI refractory patients also had lower frequencies of effector memory and central memory CD4+ T cells, lower frequencies of activated T cells, such as PD-1 expressing CD4+ and CD8+ T cells and CTLA4 expressing CD8+ T cells, and higher frequencies of cells associated with immune inhibition such as PD-L1 expressing MDSCs and monocytes and Ki67+ Tregs; higher levels of mature NK cells that express the activating receptor NKp46 were also noted in ICI refractory patients (figure 1G).

Plasma analytes measured by Olink’s immuno-oncology panel that were elevated at baseline in immune checkpoint inhibitor (ICI) refractory patients compared with ICI naïve patients. Patients included in this analysis (n=62) were ICI naïve (n=40) or refractory (n=22) prior to treatment with bintrafusp alfa. (A) Plasma analytes with p<0.05 and a >1.5 fold difference prior to bintrafusp alfa therapy between ICI refractory and ICI naïve cohorts. Analytes were log2 transformed (NPX values) and plots display median frequency of analytes. P value was calculated using the Mann-Whitney test. (B) Unsupervised hierarchical clustering of patients by the nine analytes identified in A; higher levels of expression are indicated in red and lower levels of expression are indicated in blue. Analytes were rescaled from 0 to 1 for each attribute, and samples were clustered with the complete method. Stars identify patients who are ICI refractory. CR, complete response; MR, mixed response; N, naïve; NPX, normalized protein expression; PD, progressive disease; PR, partial response; R, refractory; SD, stable disease.
Effect of bintrafusp alfa on immune parameters in patients with HPV-associated cancers
We next determined the effect of treatment with bintrafusp alfa on various immune parameters in patients with HPV-associated cancers. Among a panel of plasma cytokines and soluble factors evaluated, dramatic reductions were noted in the immunosuppressive cytokine TGFβ1 after 2 weeks of therapy (online supplemental figure 2A). This decrease in TGFβ1 was sustained throughout the dosing period with bintrafusp alfa (figure 3A). The reduction in TGFβ1 could be measured with a high level of concordance in both serum and plasma samples (online supplemental figure 2B). Increases in a number of plasma analytes were also observed after one and/or three cycles of bintrafusp alfa (online supplemental table 4A); levels of sPD-1, sCTLA4, sCD73, sCD27, and the ratio of sCD27:sCD40L were increased after one cycle, and with the exception of sCD73, all remained elevated after three cycles compared with baseline. Increases in the levels of the immunosuppressive cytokine IL-8 were also observed after three cycles of bintrafusp alfa, with 48% of patients having a >25% increase in this analyte. Changes in CBCs were also noted after therapy (online supplemental table 4B); white blood cell count (WBC), ANC, the NLR, and absolute monocyte count (AMC) were increased after one and three cycles of therapy, with the majority of patients having a >25% change in these parameters after three cycles. Among the classic cell types evaluated, there were decreases in CD8+ T cells (after one cycle), CD4+ T cells (after three cycles), and NK-T cells (after one and three cycles), and increases in monocytes (after one cycle); however, in each of these instances, the change was minor with the majority of patients having a <25% change in these subsets (online supplemental table 4C). Reductions in specific refined subsets, including effector memory CD4+ T cells that express the inhibitory marker CD73 were seen after one cycle of bintrafusp alfa, and remained reduced after three cycles of therapy (online supplemental table 4D).

Effect of bintrafusp alfa on plasma TGFβ1, and baseline level of soluble analytes associate with the development of clinical benefit to bintrafusp alfa in human papillomavirus (HPV)-associated cancers. (A) Sustained reduction in plasma levels of TGFβ1 after multiple doses of bintrafusp alfa in patients with HPV-related cancer (n=4). Baseline levels of plasma analytes measured by ELISA (B–D) and Olink’s immuno-oncology panel (E) that were different between patients deriving clinical benefit from bintrafusp alfa, compared with those not deriving clinical benefit. Patients were classified as deriving clinical benefit (responders, R) if they had a best overall response (BOR) of complete response, partial response, mixed response, or stable disease for at least 4 months, and not deriving clinical benefit (non-responders, NR) if they had a BOR of progressive disease after treatment with bintrafusp alfa. Differences were defined by p<0.05 in B-D and p<0.05 and >1.5 fold difference between R and NR in E. (F) Unsupervised hierarchical clustering of analytes identified in E; higher levels of expression are indicated in red and lower levels of expression are indicated in blue. Analytes were rescaled from 0 to 1 for each attribute, and samples were clustered with the complete method. For B-E, patients with BOR of complete responses or partial responses are indicated in red. Graphs display median frequency of analytes and p values were calculated using the Mann-Whitney test. Plasma factors were evaluated in n=62–64 (n=38 NR, n=24–26 R). Star indicates responders. NPX, normalized protein expression.
The immune status of patients with HPV-associated cancers prior to therapy associates with clinical response to bintrafusp alfa
We next evaluated whether the immune status of patients with HPV-associated malignancies prior to treatment with bintrafusp alfa associated with clinical response. Following treatment with bintrafusp alfa, patients were classified as responders if they had a BOR of CR, PR, MR, or SD for at least 4 months, and non-responders if they had a BOR of PD. Among a panel of plasma cytokines and soluble factors evaluated by ELISA, patients developing clinical responses had lower levels of the suppressive factors TGFβ1 (figure 3B) and soluble CD73 (sCD73, figure 3C), and higher levels of the ratio of soluble CD27 to soluble CD40L (sCD27:sCD40L, figure 3D), which is indicative of increased immune activation, prior to therapy than non-responders. Evaluation of 92 additional plasma analytes using Olink’s immuno-oncology panel identified 12 additional factors (CD40L, FGF2, HGF, IL-6, TGFβ1, TNFSF14, NOS3, CXCL1, CXCL5, IL-7, MUC16, and PTN, figure 3E) that were lower at baseline in those patients who responded compared with non-responders. Unsupervised clustering of patients by these analytes showed that most clinical responders clustered with one another and apart from the majority of non-responders (figure 3F). Ingenuity pathway analysis of these analytes identified an enrichment in pathways relating to regulation of the epithelial to mesenchymal transition by growth factors, and the tumor microenvironment in clinical non-responders compared with responders (online supplemental figure 3).
Prior to therapy differences in specific immune cell subsets were also noted in individuals who developed clinical benefit from bintrafusp alfa compared with those who did not. Notable differences in CBC parameters, including lower levels of WBC (figure 4A), ANC (figure 4B), AMC (figure 4C), and platelets (figure 4D) were seen at baseline in clinical responders than non-responders. Specific PBMC subsets were also differently expressed at baseline between responders and non-responders. Among the classic cell types, no differences were noted between responders and non-responders in the frequency of CD4+ or CD8+ T cells, Tregs, NK, NK-T, B cells, cDCs or pDCs; however, patients developing a clinical response to bintrafusp alfa had lower levels of MDSCs (figure 4E) and monocytes (figure 4F), and higher levels of the ratio of CD8+ T cells to MDSCs (figure 4G) than non-responders. Prior to therapy, responders also had higher levels of specific refined PBMC subsets indicative of enhanced immune activation, including effector memory CD4+ T cells (figure 4H) and PD-1 expressing CD4+ T cells, CD8+ T cells, and NK cells (figure 4I–K). Notably lower levels of naïve CD4+ and CD8+ T cells (figure 4L–M), as well as immune subsets indicative of immune suppression, such as CD73+CD8+ T cells (figure 4N) and PD-L1 expressing MDSC and monocytes (figure 4O–P), were observed prior to therapy in responders compared with non-responders.

Baseline levels of complete blood counts (CBCs), classic and refined immune cell subsets, and TCR diversity associate with the development of clinical benefit to bintrafusp alfa in human papillomavirus (HPV)-associated cancers. Patients were classified as deriving clinical benefit (responders, R) if they had a best overall response (BOR) of complete response, partial response, mixed response, or stable disease for at least 4 months, and not deriving clinical benefit (non-responders, NR) if they had a BOR of progressive disease after treatment with bintrafusp alfa. Baseline levels of (A–D) CBC measures, (E–G) classic subsets and ratios, (H–P) refined subsets, and (Q) level of TCR diversity (measured by the metric of repertoire size) that are different between NR and R. Values in Q indicate the number of individual clonotypes comprising the top 25th percentile ranked by molecule count after sorting by abundance. Patients with BOR of complete response or partial response are indicated in red, and graphs display median frequency of analytes. Differences were defined by p<0.05 in A-D, and p<0.05 and a frequency above 0.01% of PBMCs for E–P. P value was calculated using the Mann-Whitney test. CBC measures were evaluated n=65 (n=39 NR, n=26 R), immune subsets in n=31 (n=20 NR, n=11 R), and TCR diversity in n=12 (n=6 NR, n=6 R). AMC, absolute monocyte count; ANC, absolute neutrophil count; EM, effector memory; MDSC, myeloid derived suppressor cell; NK, natural killer cell; PD1, programmed death receptor 1; PDL1, programmed death receptor ligand 1; TCR, T-cell receptor; WBC, white blood cell count.
At baseline, although with samples from only a few patients available, trends of lower levels of TCR diversity were also noted in the peripheral blood of responding than non-responding patients, with 5/6 responders (83%) vs 2/6 (33%) of non-responders having less than 400 unique TCR clones comprising the top 25% of the T cell repertoire (figure 4Q).
Early immune changes induced after bintrafusp alfa associate with clinical response in patients with HPV-associated cancers
Following one cycle of bintrafusp alfa, a time point that precedes the restaging of patients enrolled in this trial, differences between responders and non-responders in the percent change of specific plasma analytes and CBC measures were observed. More patients who derived clinical benefit from bintrafusp alfa had decreases in IL-8 (figure 5A), increases in ALC (figure 5B), and decreases in ANC (figure 5C) and the NLR (figure 5D) than non-responders. The early differences noted in IL-8, ANC and NLR between responders and non-responders persisted after three cycles of therapy (figure 5E–G).
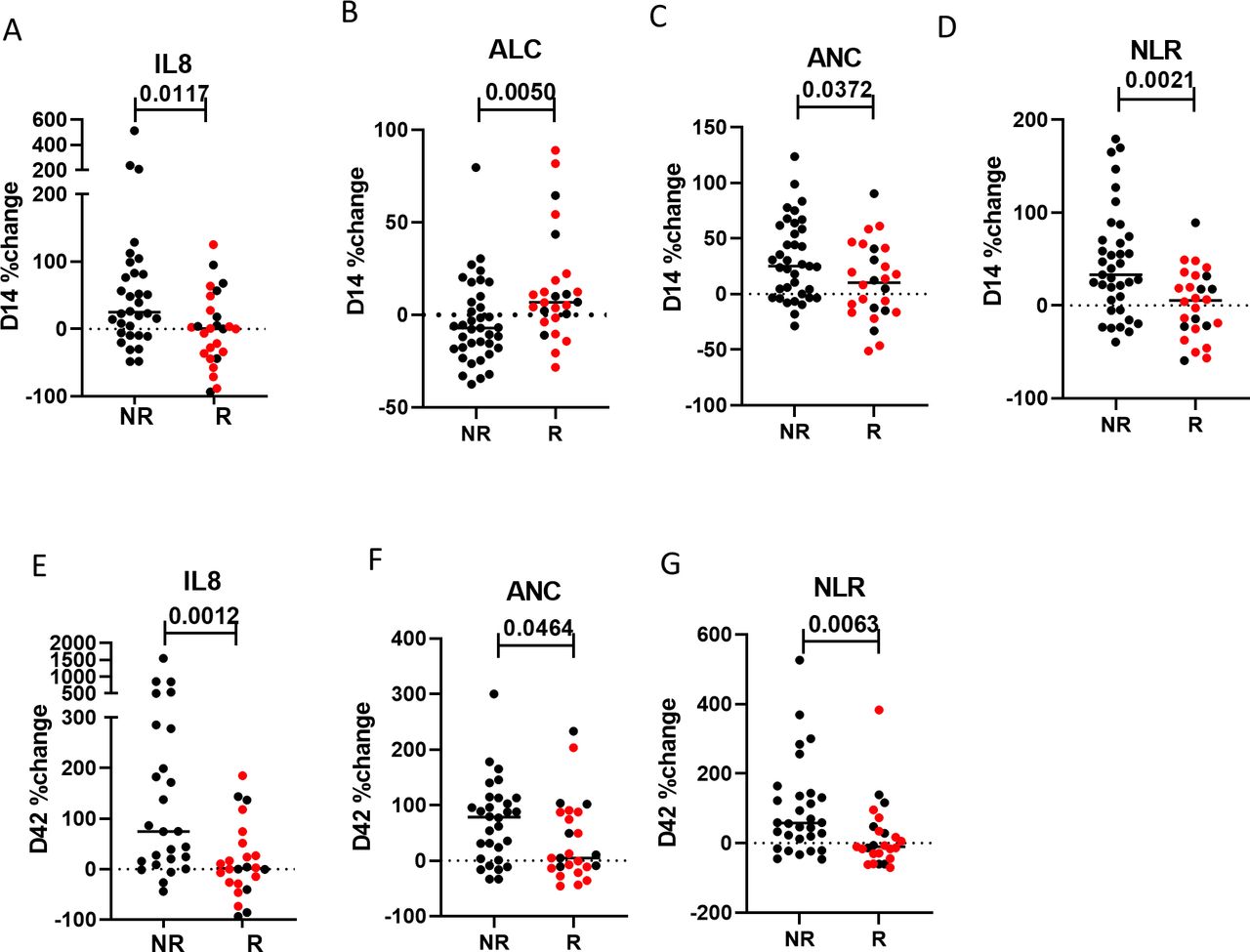
Early changes in soluble analytes and complete blood counts (CBCs) associate with the development of clinical benefit to bintrafusp alfa in HPV-associated cancers. The percent change in analytes after one cycle of bintrafusp alfa (vs pre, (A–D)) and three cycles of bintrafusp alfa (vs pre, (E–G)) that are different in patients deriving clinical benefit from bintrafusp alfa, compared with those not deriving clinical benefit. Patients were classified as deriving clinical benefit (responders, R) if they had a best overall response (BOR) of complete response, partial response, mixed response, or stable disease for at least 4 months, and not deriving clinical benefit (non-responders, NR) if they had a BOR of progressive disease after treatment with bintrafusp alfa. Patients with BOR of complete response or partial response are indicated in red, and graphs display median values of analytes. Differences were defined by p<0.05; p value was calculated using the Mann-Whitney test. Changes in plasma analytes were evaluated in n=58 (n=32 NR, n=26 R) and CBC measures in n=63 (n=37 NR, n=26 R) before and after one cycle of bintrafusp alfa. Changes in plasma analytes were measured in n=50 (n=26 NR, n=24 R) and CBC measures in n=56 (n=31 NR, n=25 R) before and after three cycles of bintrafusp alfa. ALC, absolute lymphocyte count; ANC, absolute neutrophil count; NLR, neutrophil to lymphocyte ratio.
Immune parameters that associate with clinical response within the ICI naïve and ICI refractory cohorts of patients
We also evaluated whether there were specific immune parameters at baseline, or early changes in immune parameters after one cycle of therapy, that associate with the development of clinical response within the ICI naïve and ICI refractory groups of patients separately. Minor differences were observed within each cohort (online supplemental figures 4 and 5); however, it should be noted that these analyses included small numbers of patients.
Models to predict response to bintrafusp alfa in patients with HPV-associated cancers
In patients with HPV-associated cancers, we next performed logistic regression analyses first using only plasma analytes and CBC parameters, where data were available for 58 patients both at baseline and the 2-week time point post bintrafusp alfa. Here, patients with a BOR of CR, PR, MR, or SD >4 months were compared with patients with a BOR of PD, and patients were split into a training set (n=43) and a test set (n=15). The ROC curve generated from a 3-factor model developed in the training set using log transformed levels of baseline TGFβ1 and the percent change after 2 weeks of therapy in IL-8 and the NLR produced a global χ2 of 23.93 and AUC of 0.892 (figure 6A). This model was used to calculate the response probability for individual patients. Using a cut-off of 0.5, this model could predict clinical response with 84% accuracy in the training set (figure 6B), 80% accuracy in the test set (figure 6C), and 83% accuracy in the training and test sets combined (figure 6D). The median overall survival of patients with a response probability >0.5 generated with this model was significantly longer (1222 days) than the overall survival of patients with a response probability ≤0.5 (142 days, p=0.0004, figure 6E).

Logistic regression analyses to predict clinical response in patients with human papillomavirus (HPV)-associated cancers. Logistic regression analyses were performed to develop models to predict clinical response. (A) Receiver operating characteristic (ROC) curve generated from a three-factor model based on log transformed levels of baseline TGFβ1, and the % change after one cycle vs pre in IL-8 and the NLR, had a global χ2 of 23.93 and area under the curve (AUC) of 0.892. For this model, patients with a best overall response (BOR) of complete response, partial response, mixed response, or stable disease >4 months were compared with patients with a BOR of progressive disease. The model generated in A was used to calculate the response probabilities for individual patients in the training set (B), the test set (C), and the training and test sets combined (D). The overall survival of patients with a response probability >0.5 generated from the model in A was significantly greater (1222 days) than the overall survival of patients with a response probability <0.5 (142 days) (E). For A-E, plasma analytes and CBC measures were available for 58 patients both at baseline and the 2-week time point post bintrafusp alfa, and patients were divided into a training set (n=43) and a test set (n=15). (F) ROC curve generated with data from a three-factor model based on log transformed levels of baseline TGFβ1, IL-8 and NLR and overall survival had a global χ2 of 16.32 and AUC of 0.841. For this model, patients with an overall survival >180 days were compared with patients with an overall survival <180 days. The model generated in F was used to calculate the response probabilities for individual patients in the training set (G), the test set (H), and the training and test sets combined (I). The overall survival of patients with a response probability >0.5 generated from the model in F was significantly greater (1061 days) than the overall survival of patients with a response probability <0.5 (109 days) (J). For F–J, plasma analytes and CBC measures were available for 63 patients at baseline, and patients were divided into a training set (n=42) and a test set (n=21). OS, overall survival; NLR, neutrophil to lymphocyte ratio.
We also developed a second model using plasma analytes and CBC for patients at baseline only, where data were available from 63 patients. Here, patients with an overall survival >180 days were compared with those patients with an overall survival <180 days, and patients were split into a training set (n=42) and a test set (n=21). The ROC curve generated from a three-factor model developed in the training set using log transformed levels of baseline TGFβ1, IL-8, and the NLR produced a global χ2 of 16.32 and AUC of 0.841 (figure 6F). This model was used to calculate the response probability for individual patients. Using a cut-off of 0.5, this model could predict overall survival ≥180 days with 76% accuracy in the training set (figure 6G), 91% accuracy in the test set (figure 6H), and 81% accuracy in the training and test sets combined (figure 6I). The median overall survival of patients with a response probability >0.5 generated with this model was significantly longer (1061 days) than the overall survival of patients with a response probability <0.5 (109 days, p<0.0001, figure 6J).
Increase in TAA-specific T cells after bintrafusp alfa in clinical responders and non-responders with HPV-associated cancers
We finally interrogated whether there were differences in the development of T cells specific for the TAAs HPV-16 E6/E7, HPV-18 E6/E7, and MUC1 in responding and non-responding patients with HPV-associated cancers, treated with bintrafusp alfa. This analysis was performed by intracellular cytokine staining following stimulation of PBMCs with overlapping peptides encoding the indicated TAAs and negative control (HLA) and positive control (CEFT) peptide pools. While no differences were noted in the development of CD4+ or CD8+ T cells specific for HPV-18 or MUC1 in responding and non-responding patients, significant associations with clinical response were detected in the development of HPV-16-specific CD8+ T cells after treatment with bintrafusp alfa. After one and three cycles, a greater frequency of responders than non-responders developed CD8+, but not CD4+, HPV-16 specific T cells (figure 7A). In addition, the magnitude of the CD8+ HPV-16 T cells developed after one and three cycles was significantly greater in clinical responders than non-responders (figure 7B). Significantly greater increases were also noted in the magnitude of multifunctional CD8+ HPV-16 T cells developed after one cycle of bintrafusp alfa in clinical responders than non-responders (figure 7C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Increase after bintrafusp alfa in CD8+ T cells targeting human papillomavirus (HPV)-16 associates with clinical response in HPV-associated cancers. Changes in CD4+ and CD8+ T cells specific for HPV-16 E6/E7 were evaluated after (vs before) one and three cycles of bintrafusp alfa and compared in patients deriving clinical benefit versus those not deriving clinical benefit from bintrafusp alfa. Patients were classified as deriving clinical benefit (responders, R) if they had a best overall response (BOR) of complete response, partial response, mixed response, or stable disease for at least 4 months, and not deriving clinical benefit (non-responders, NR) if they had a BOR of progressive disease after treatment with bintrafusp alfa. (A) The frequency of NR and R who developed an increase in HPV-16 CD4+ or CD8+ T cells after one and three cycles of therapy. (B) The magnitude of HPV-16 CD8+ T cells developed in NR and R, after one and three cycles of bintrafusp alfa. Each point in B indicates the magnitude of a single cytokine/CD107a measure, with four measures per patient (CD8+IFN-γ+, CD8+TNF-α+, CD8+IL-2+, CD8+CD107a+). (C) The magnitude of multifunctional HPV-16 CD8+ T cells developed after one and three cycles of therapy in NR and R. Each point in C indicates a single measurement per patient (CD8+ T cells positive for two or more among IFN-γ, TNF-α, IL-2 and CD107a). Graphs display mean±SEM. P value was calculated using Fisher’s exact test in A and the Mann-Whitney test in B–C. Changes in HPV-16 specific T cells were evaluated in n=44 (n=42 before and after one cycle and n=33 before and after three cycles of bintrafusp alfa). IFN-γ, interferon-γ; IL-2, interleukin-2; TNF-α, tumor necrosis factor-α.
Discussion
Despite the unparalleled success of HPV preventive vaccines, HPV-associated malignancies, including carcinomas of the cervix, vulva, penis and oropharyngeal cavity, remain a major health concern with 44,000 new cases annually in the US and 630,000 new cases annually worldwide. As detailed above, while the reported and ongoing clinical studies of bintrafusp alfa are relatively small, compared with the response rates observed employing other checkpoint inhibitor antibodies, we believe further evaluation of the bifunctional agent in HPV-associated cancers is merited.
An optimal evaluation of the mode of action of any agent would include analyses of tumor biopsies as well as the peripheral immunome. Tumor biopsy specimens, unfortunately, were not available for the vast majority of patients involved in the study reported here. The various components of the peripheral immunome analyzed here demonstrated the changes in both multiple immune subsets and plasma analytes as a consequence of treatment with bintrafusp alfa. Moreover, these analyses conducted both prior to therapy and early in the therapeutic regimen also provided some hypothesis generating, biologically reasonable associations with clinical outcomes. For example, in analyses prior to bintrafusp alfa therapy, an association with clinical response was seen in patients with higher levels of ratios of sCD27:sCD40L. sCD27 has been reported to be associated with T-cell activation27 while sCD40L has been reported to be associated with T-cell suppression.28 Responding patients also had lower levels of TGFβ1 at baseline. Analyses of 12 additional plasma analytes using an Olink panel and ingenuity pathway analyses identified clinical responses associated with multiple factors involved in the regulation of the epithelial to mesenchymal growth pathway. At baseline patients developing a clinical response also had lower levels of MDSCs and monocytes, higher CD8+ T cell:MDSC ratios, and lower levels of CD73+CD8+ T cells. Trends of lower levels of TCR diversity at baseline were also noted in patients who eventually responded; however, this finding should be interpreted as preliminary, based on the small number of patients evaluated.
Most striking were the associations observed between clinical responders and non-responders when the analyses were carried out following cycle 1 of bintrafusp alfa, a time point 2 weeks post-treatment and preceding restaging. For example, clinical responders had less of an increase in IL-8 than non-responders, and less of an increase in the NLR. IL-8 is a well-known immunosuppressive chemokine produced by leukocytes (monocytes, T cells, neutrophils) and non-leukocytes (endothelial cells, fibroblasts, epithelial cells), with multiple protumorigenic roles within the tumor microenvironment; IL-8 stimulates tumor cells into a migratory or mesenchymal phenotype, increases angiogenesis, and recruits immunosuppressive cells into the tumor.29 The observation that non-responders had greater early increases after bintrafusp alfa in the immunosuppressive cytokine IL-8 than responders provides the rationale for potential combination therapies of bintrafusp alfa with inhibitors of IL-8 to potentially increase the percentage of patients responding to therapy.
This study also provided information concerning the peripheral immunome in patients who were immune checkpoint naïve versus refractory that may help to explain the different level of clinical activity of bintrafusp alfa observed among these populations. For example, checkpoint refractory patients clearly had higher levels at baseline of sPD-1, sCD73, sCTLA4, and lower sCD27:sCD40L ratios. Moreover, checkpoint refractory patients had higher levels of immunosuppressive immune subsets, including PD-L1 expressing MDSC and Ki67 Tregs. The finding that checkpoint refractory patients had higher levels of sCD73 and sCTLA4 at baseline provides the rationale for potential combination therapies of bintrafusp alfa with CTLA4 inhibitors and/or adenosine pathway inhibitors. There were no major differences in the peripheral immunome at baseline in patients with cervical (n=28) vs HPV+ head and neck cancers (n=18), the two major groups analyzed here. Future studies in which both tumor biopsy and peripheral immunome specimens are available will hopefully provide a more comprehensive view of the anti-tumor mechanisms involved in bintrafusp alfa therapy, as well as a better understanding of tumor escape mechanisms.
The two multivariant models developed here, which predicted clinical benefit with 76%–91% accuracy, employed analyses at baseline or shortly after treatment initiation (and prior to first restaging); while preliminary, analyses such as these may eventually offer an additional tool to help select patients who are more likely to benefit from treatment, or for switching patients to other therapies who are less likely to benefit. Numerous prior studies have shown the prognostic potential of serum or cell-based analyses of patients with solid tumors treated with ICIs. For example, levels of soluble granzyme and IL-8 have shown prognostic value in patients with NSCLC, urothelial and bladder cancer among other cancer types.30–33 Plasma proteomics and soluble factors have shown prognostic value in patients with NSCLC and prostate cancer.34 35 In terms of analyses of peripheral cell subsets, ratios of neutrophils to lymphocytes have shown prognostic value in patients with NSCLC, SCLC, and urothelial cancers,36–39 and subsets of CD4+ and CD8+ T cells as well as B cells have shown prognostic value in various solid tumor types including renal cell and NSCLC.40–42
As in the trial reported here, biopsies of most solid tumor metastasis are often difficult to obtain. Perhaps more importantly, for most non-melanoma solid tumors, the only pretreatment biopsies available are those that were obtained years prior to the immunotherapy trial. It is also well known that most solid tumors are heterogeneous, will evolve phenotypically with time, and may well be phenotypically altered as a consequence of any prior therapeutic regimens; tumors at different sites within a given individual have also been shown to vary.43–45 Usually at the time of disease recurrence in patients with HPV-associated malignancies the primary lesions have been definitively treated and often these patients have advanced or metastatic disease limited to retroperitoneal nodes, mediastinal nodes or pulmonary lesions.
Analysis of a tumor biopsy can provide valuable information concerning the phenotype of tumor and the spatial distribution of immune cells relative to tumor. Multiplex analyses of tumor can provide information concerning one or two subtypes of a given cell type, but not the 158 subset platform analyzed in the study reported here. Moreover, cytokines such as IL-8 or TGFβ, chemokines, or other soluble factors can have profound influence on tumor sensitivity and/or resistance to immunotherapy–an analysis that cannot be determined interrogating a biopsy. The analyses of peripheral immune subsets and soluble factors also provide an accessible real time evaluation of the immune status of a patient immediately prior to therapy, and/or early in the therapeutic regimen, such as the day 14 post-treatment values reported here, that could provide potential prognostic value prior to the first restaging.
The prior studies carried out with bintrafusp alfa in patients with non-HPV-associated malignancies demonstrated mixed results. Three randomized studies, two studies in lung cancer (NCT03631706, NCT03840902) and one in biliary tract cancer (NCT04066491), were discontinued. These studies were stopped early for futility, but not necessarily because the agent did not have clinical activity. The encouraging results seen in patients with HPV-associated cancers vs those seen in lung and biliary tract cancer may be due to the type of cancer being evaluated and/or the trial design such as enrollment and endpoint criteria. The types of analyses carried out in the studies reported here may help provide answers to those questions. It is possible that the immunomes associating with clinical response in patients with HPV-associated cancers may be applied to identify those patients with non-HPV-cancers who may benefit from bintrafusp alfa therapy.
The observation here that patients who benefited from bintrafusp alfa treatment developed higher levels of HPV-specific T cells including higher levels of multifunctional T-cell responses provides the rationale for combining bintrafusp alfa therapy with other therapeutic strategies that target HPV. Future studies may be performed to try and identify specific TCRs that recognize HPV epitopes that are expanded after bintrafusp alfa, which may be able to be used in adoptive transfer strategies in combination with bintrafusp alfa. Recent preclinical studies have demonstrated that combining bintrafusp alfa with an HPV therapeutic vaccine and an IL-12 tumor targeting immunocytokine (NHS-IL12) leads to higher anti-tumor responses, and increased T-cell clonality in tumors, compared with monotherapies or doublets of these agents.10 Preliminary results of an ongoing phase II study combining bintrafusp alfa, PDS0101 HPV therapeutic vaccine and NHS-IL12 in patients (n=24) with HPV-associated malignancies are demonstrating an ORR of 42% with tumor reduction in 54% of patients, including patients with checkpoint refractory disease.46 Comparison of the results using the various assays of the bintrafusp alfa monotherapy trial reported here with subsequent results of assays interrogating the triplet trial may help gain further insight into our understanding of tumor control and escape mechanisms in patients with HPV-associated cancers.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The studies were conducted in accordance with all applicable regulatory requirements, and the protocols were approved by the Institutional Review Board of the Center for Cancer Research at the National Institutes of Health.
Acknowledgments
Merck KGaA, Darmstadt, Germany, reviewed the manuscript for medical accuracy only before journal submission. The authors thank Debra Weingarten for her editorial assistance in the preparation of this manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @gulleyj1
JS and RND contributed equally.
Contributors Conception/design: Y-TT, JSt, JLG, JSc and RND. Provision of study materials or patients: JSt, JLG and JSc. Collection and/or assembly of data: Y-TT, NJT, CJ, DJV and RND. Data analysis and interpretation: Y-TT, JSt, NJT, CJ, DJV, JLG, JSc and RND. Manuscript writing: Y-TT, DJV, JSt and RND. Final approval of manuscript: all authors. JSc responsible for the overall content as the guarantor.
Funding Funding was provided by the Intramural Program of the Center for Cancer Research of the National Cancer Institute (NCI), National Institutes of Health, and via an NCI Cooperative Research and Development Agreement (CRADA) with EMD Serono/Merck. NCT02517398 was sponsored by Merck KGaA, Darmstadt, Germany, and was previously part of an alliance with GlaxoSmithKline.
Disclaimer The authors are fully responsible for the content of this manuscript, and the views and opinions described in the publication reflect solely those of the authors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.