Article Text

Abstract
Purpose Although recombinant human interleukin-15 (rhIL-15) has generated much excitement as an immunotherapeutic agent for cancer, activity in human clinical trials has been modest to date, in part due to the risks of toxicity with significant dose escalation. Since pulmonary metastases are a major site of distant failure in human and dog cancers, we sought to investigate inhaled rhIL-15 in dogs with naturally occurring lung metastases from osteosarcoma (OSA) or melanoma. We hypothesized a favorable benefit/risk profile given the concentrated delivery to the lungs with decreased systemic exposure.
Experimental design We performed a phase I trial of inhaled rhIL-15 in dogs with gross pulmonary metastases using a traditional 3+3 cohort design. A starting dose of 10 µg twice daily × 14 days was used based on human, non-human primate, and murine studies. Safety, dose-limiting toxicities (DLT), and maximum tolerated dose (MTD) were the primary objectives, while response rates, progression-free and overall survival (OS), and pharmacokinetic and immune correlative analyses were secondary.
Results From October 2018 to December 2020, we enrolled 21 dogs with 18 dogs reaching the 28-day response assessment to be evaluable. At dose level 5 (70 μg), we observed two DLTs, thereby establishing 50 µg twice daily × 14 days as the MTD and recommended phase 2 dose. Among 18 evaluable dogs, we observed one complete response >1 year, one partial response with resolution of multiple target lesions, and five stable disease for an overall clinical benefit rate of 39%. Plasma rhIL-15 quantitation revealed detectable and sustained rhIL-15 concentrations between 1-hour and 6 hour postnebulization. Decreased pretreatment lymphocyte counts were significantly associated with clinical benefit. Cytotoxicity assays of banked peripheral blood mononuclear cells revealed significant increases in peak cytotoxicity against canine melanoma and OSA targets that correlated with OS.
Conclusions In this first-in-dog clinical trial of inhaled rhIL-15 in dogs with advanced metastatic disease, we observed promising clinical activity when administered as a monotherapy for only 14 days. These data have significant clinical and biological implications for both dogs and humans with refractory lung metastases and support exploration of combinatorial therapies using inhaled rhIL-15.
- melanoma
- cytokines
- sarcoma
- clinical trials as topic
- killer cells, natural
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Although strategies to activate T cells are the focal point of the burgeoning immuno-oncology field, there is a growing appreciation that other immune cells, such as natural killer (NK) cells, play important roles in tumor surveillance and elimination and therefore represent attractive candidates for expanding the promise of immunotherapy. Dogs are outbred companion animals that develop spontaneous cancers in the setting of an intact immune system, allowing for the study of complex immune interactions during cancer therapies while also addressing endpoints of efficacy and toxicity.
WHAT THIS STUDY ADDS
This phase I clinical trial in dogs with gross pulmonary metastatic disease from osteosarcoma and melanoma builds on prior work in human and canine immunotherapy trials using immunostimulatory cytokine therapy to demonstrate that inhaled recombinant human interleukin-15, the prototypical NK stimulatory cytokine, induces encouraging antitumor responses using a novel, first-in-dog approach with evidence for clinical and immunologic activity.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
These interesting findings are expected to have relevance for the design and translation of ongoing innovative immunotherapy approaches in both dogs and people.
Background
Cytokine immunotherapies have been a key area of research focus in cancer immunotherapy given their ability to stimulate powerful immune responses.1 2 Interleukin-15 (IL-15) in particular has shown promise as an antitumor immunotherapeutic and has been used to stimulate endogenous cytotoxic natural killer (NK) and T cell responses against advanced cancers.3–9 However, while durable responses have been achieved in some patients, clinical trials of IL-15 monotherapy for patients with advanced cancer have frequently resulted in stable disease as the best response, and many of these trials were limited by systemic toxicity.10 11
Distinct from direct intratumoral therapy, inhaled cytokine therapy offers the advantages of regional delivery of immunotherapy to the lungs, a frequent site of gross metastatic disease, while limiting systemic exposure and potential toxicity. In addition, the lungs are known to harbor a unique immune microenvironment, likely secondary to frequent pathogen exposure, and significant tissue-resident NK and CD8 +T cell immune populations have been identified in the lungs with both a memory-like and heightened cytotoxic phenotype.12
Cytokine immunotherapy using the inhalation route of delivery has previously been administered and demonstrated to be safe using IL-2 therapy for both dogs and humans with pulmonary metastases.13–15 Inhaled IL-2 has also been used in human cancer trials with response rates of approximately 15%.14 16 17 Yet, interest in this approach did not materialize in part because of concerns regarding the immunosuppressive effects of IL-2, including upregulation of regulatory T cells (Tregs) and induction of activation-induced cell death in cytotoxic T cells.3 Given that there are critical differences in the mechanisms of action of IL-15 and IL-2, we sought to evaluate the safety and potential clinical efficacy of inhaled IL-15 as a phase I, proof-of-concept trial in dogs with pulmonary metastases from melanoma and osteosarcoma (OSA).
Dogs are companion animals that develop spontaneous cancers in the setting of an intact immune system, which allows for the study of complex immune interactions during cancer therapies while also addressing efficacy and toxicity endpoints. Melanoma and OSA are common canine malignancies, estimated to occur in approximately 20,000–100,000 US dogs per year.18 19 Additionally, perhaps more so than humans, melanoma and OSA are overwhelmingly lethal diseases in dogs18 20 21 with median survival times of less than 1 year. Although melanoma and OSA are associated with distinct immune tumor microenvironments (TMEs) and differential response to immunotherapy in humans, there are few, if any, effective immunotherapy options in dogs. Therefore, dogs with these cancers are ideal candidates for novel immunotherapy approaches.
Here, we report the results of a first-in-dog phase I clinical trial of inhaled recombinant human (rh) IL-15 in dogs with gross pulmonary metastases from melanoma or OSA. We observed 50 µg inhaled twice daily × 14 days to be the recommended phase 2 dose with two dose limiting toxicities (DLTs) observed in the 70 µg cohort. Among 18 evaluable patients, we observed an objective response rate of 11%, including one complete response (CR) that lasted >1 year and a clinical benefit rate of 39%. Immune correlative assays demonstrated systemic effects of therapy with evidence for delineation of responders and non-responders based on baseline absolute lymphocyte count (ALC) and correlation of ex vivo peripheral blood cytotoxicity assays with survival. Taken together, these data support ongoing evaluation of inhaled IL-15 as a strategy to improve immunotherapy outcomes in both dogs and people with gross pulmonary metastatic disease.
Methods
Patients
Client-owned pet dogs with metastatic melanoma or OSA were enrolled in this phase I study. Eligible dogs were required to be greater than 1 year old, weigh at least 8 kg, have a VCOG-CTCAE 1.2 performance score of 0 or 1, and have one or more lung lesions consistent with metastatic disease measuring at least 1 cm on thoracic radiographs. The clinical protocol for this trial is included in the online supplemental material. Dogs were also deemed able to be successfully trained to accept nebulization with owners willing to administer inhaled rhIL-15 twice daily. All owners provided signed informed owner-consent.
Supplemental material
Supplemental material
Supplemental material
We also performed two separate pilot, first-in-dog clinical trials to: (1) assess the feasibility of palliative radiation therapy (RT), allogeneic natural killer (NK) cell transfer, and subcutaneous (SQ) rhIL-15 (3 µg/kg) in dogs with locally advanced, non-metastatic melanoma and (2) the safety and preliminary assessment of response of ALT-803 in dogs with metastatic cancer.22 The clinical protocol for these trials are also included in the online supplemental material.
Study design
For the inhaled rhIL-15 trial, the primary objective was to determine the maximum tolerated dose (MTD) using a traditional 3+3 cohort design with a dose-escalation schedule.23 Escalation was based on assessment of DLTs, defined as any grade 3 non-hematologic or grade 4 hematologic toxicity as defined by the Veterinary Cooperative Oncology Group Common Terminology Criteria for Adverse Events (VCOG-CTCAE V.2).24 The starting dose of rhIL-15 was 10 µg. Dose escalation followed a fixed dose modified Fibonacci method, where the dose is escalated 100%, 67%, 50%, 40% and then 33% of the previous cohort dose.
Study treatment
The primary investigational agent used in this trial was Escherichia coli derived rhIL-15 manufactured by the Biopharmaceutical Development Program of the Division of Cancer Treatment and Diagnosis/National Cancer Institute using current Good Manufacturing Practices. Patients were treated with inhaled rhIL-15 twice daily for 14 days at dose levels of 10, 20, 33, 50 or 70 µg (figure 1A). The first treatment was performed at the UC Davis VMTH to ensure that the patient and the owners were properly trained and tolerated the therapy. The nebulizer was attached to a fitted veterinary anesthesia cone, and depending on patient comfort and tolerability, the cone was placed directly over the patient muzzle (online supplemental figure 1) or placed within a plastic boot cover that was placed over the muzzle during delivery. Owners were instructed to perform treatments a minimum of 8 hours apart, and owners were requested to complete a treatment log. ALT-803, also known as N-803, was a generous gift from Altor Bioscience, now merged with NantCell/ImmunityBio. Dogs received once weekly ALT-803 for a total of four treatments.
Supplemental material
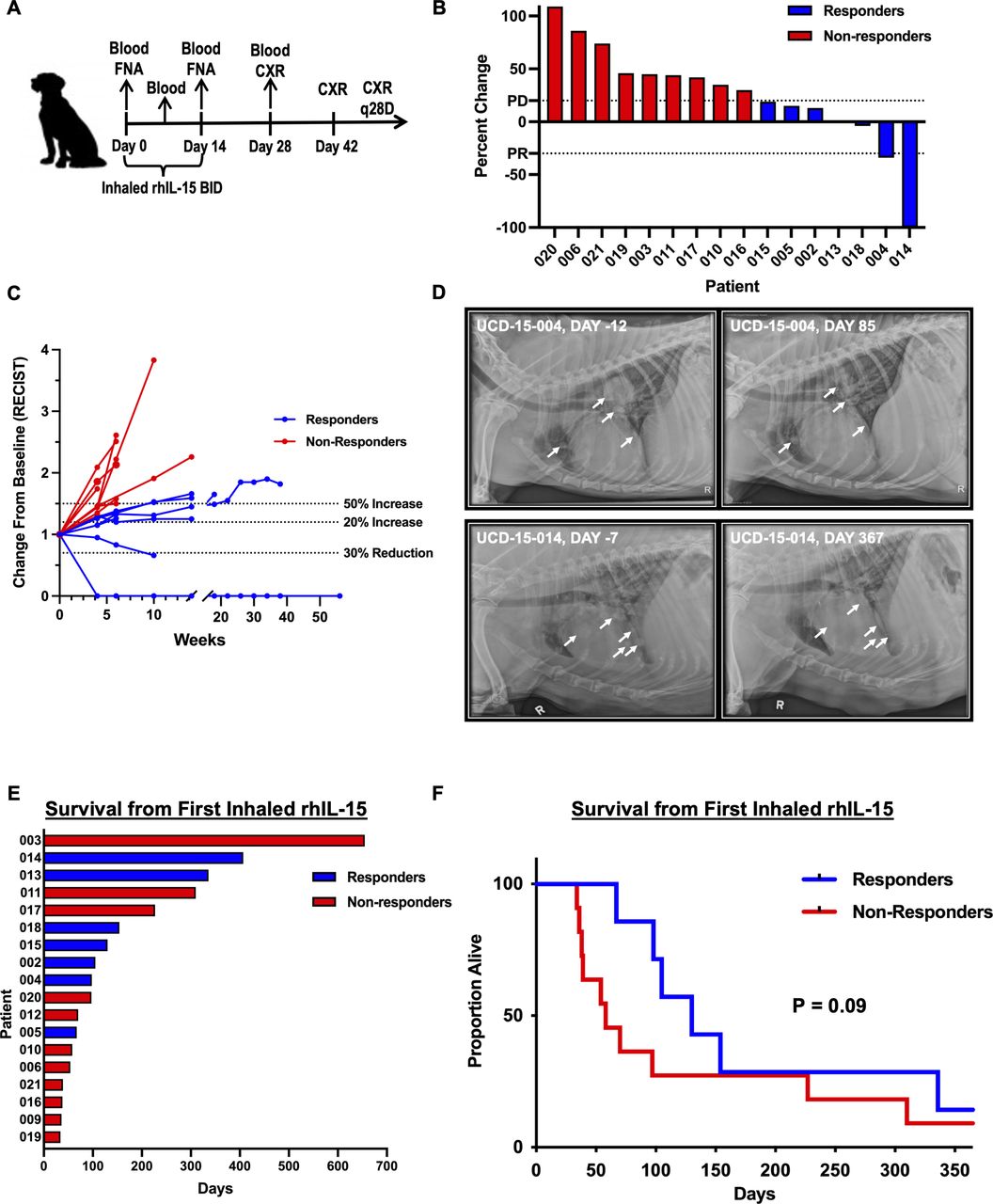
Study design and assessment of clinical responses. (A) Schema of first-in-dog clinical trial of inhaled rhIL-15 delivered by nebulizer twice daily for 14 total days. Blood was drawn prior to treatment as well as on days 7, 14 and 28, and response was evaluated by chest radiograph (CXR) on days 28, 42, 70, and 98. (B) Waterfall plot demonstrating percent change of target tumor sizes in responders and non-responders. Progressive disease (PD) ≥20% increase from baseline, and partial response (PR) >30% decrease from baseline. (C) Spider plot summarizing changes in sum of each patient’s longest tumor diameters from baseline over time. Evaluable patients were considered responders (blue) or non-responders (red) based on RECIST criteria. Stable disease was defined as within the thresholds of <20% increase and <30% decrease in tumor diameter as illustrated by dashed lines. (D) Representative radiographs illustrating changes in pulmonary lesions prior to and following treatment with inhaled rhIL-15. Patient 4 (top panel) experienced a PR with complete resolution of three out of five lesions at dose level 1, while patient 14 (bottom panel) showed a complete response with resolution of diffuse pulmonary metastatic lesions leading to remission that lasted >1 year after completion of treatment. (E) Survival from first inhaled rhIL-15 treatment for responders/patients having clinical benefit versus non-responders. (F) Kaplan-Meier curve from initiation of treatment showing a trend for improved survival among responders/patients with clinical benefit. rhIL-15, recombinant human interleukin-15.
Clinical and investigational assessments
Clinical assessments and vital signs were performed prior to the first treatment and then 1 hour, 3 hours, and 5 hours after the first treatment was completed. Blood work was performed at baseline and then at day 7, day 14, and day 28 of study. Plasma rhIL-15 concentrations were measured in a subset of patients analyzing samples collected prior to the first treatment, 5 min after starting treatment, at completion of the first inhaled treatment, and at 1, 4, and 6 hours post-treatment. Response was assessed based on the Response Evaluation Criteria for Solid Tumors in Dogs (RECIST V.1.0) by a board-certified veterinary radiologist (EGJ).25 Due to the frequent rapid progression of metastatic OSA and melanoma in canine patients, 10 mm lesions were considered acceptable for enrollment rather than 20 mm. To be considered stable disease (SD), patients had to have a minimum of 28 days between imaging to meet criteria for response assessment of between <20% increase and <30% decrease in longest tumor diameter. Three-view thoracic radiographs were performed within 1 month prior to beginning therapy and were repeated on days 28, 42, 70, and 98 after initiation of inhaled rhIL-15. Patients could be restaged early if clinically indicated, and patients surviving beyond day 98 were offered imaging every 28 days.
Flow cytometry and RNA sequencing
Canine whole blood was collected at indicated time points. Plasma EDTA and whole-blood serum samples were kept on ice and stored at −80°C within 30 min of collection. Peripheral blood mononuclear cells (PBMCs) were isolated from whole blood using density gradient centrifugation (Lymphocyte Separation Medium, Corning Life Sciences), followed by red blood cell lysis as described previously.26 Staining for flow cytometry was performed as described previously using the following antibodies: CD45-EF450 (clone YKIX716.13, Invitrogen # 48-5450-42), CD3-FITC (clone CA17.2A12, BioRad #MCA1774F), NKp46-PE (clone 48A, kind gift of Dr. Dean Lee), and CD8-APC (clone YCATE55.9, Invitrogen #17-5080-42).9 Live/dead staining performed using Fixable Viability Dye 780. Cells were processed for RNA isolation using the Total RNA Purification Plus Micro Kit (Norgen Biotek, Ontario, Canada). RNAseq libraries were prepared by the University of California, Davis, Bioinformatics Core. RNA sequencing data will be made available on NCBI GEO.
Human IL-15 ELISA
rhIL-15 plasma concentrations were measured using the Human IL-15 Uncoated ELISA kit (Invitrogen #88–760) according to the manufacturer’s instructions, with some modifications. In place of the kit standards, ELISA standards were generated using serial dilutions of the clinical stock rhIL-15 and ranged from 15.625 to 1000 pg/mL. Undiluted plasma (100 µL) was used per well, except for the samples from trial #21 620 (RT, allogeneic NK cells, and SQ rhIL-15), which were diluted 1:10. All samples were run in duplicate and repeated twice.
Cytotoxicity assays
Canine OSA (OSCA-78) and melanoma (M5) tumor cell lines were obtained from established immortalized stocks.22 Cytotoxicity was assessed by labeling target cells with carboxyfluorescein succinimidyl ester (CFSE,Invitrogen #C34554) for 5 min at room temperature prior to coculturing with thawed patient PBMCs. After 18 hours of overnight effector/target coculture, cells were stained with Fixable Viability Dye 780 and analyzed by flow cytometry. Per cent cytotoxicity was calculated according to the following formula: [CFSE+ FVD780+ / (CFSE+ FVD780+) + (CFSE+ FVD780−)]×100.9 Adjusted cytotoxicity was determined by subtracting spontaneous killing of target cells when no effectors were added (0 E:T).
Multiplex analysis of cytokines
Multiplex analysis was performed using the Luminex 200 system (Luminex, Austin, Texas, USA) by Eve Technologies Corp (Calgary, Alberta). Thirteen markers were measured in the samples using the Canine Cytokine 13-Plex Discovery Assay (MilliporeSigma, Burlington, Massachusetts, USA) according to the manufacturer’s protocol. The 13-plex panel consisted of GM-CSF, IFNγ, IL-2, IL-6, IL-7, IL-8/CXCL8, IL-10, IL-15, IL-18, IP-10/CXCL10, KC-like, MCP-1/CCL2, and TNFα. Assay sensitivities of these markers range from 3.2 to 21.0 pg/mL.
Statistical analysis
We used Excel (Microsoft), Prism software (GraphPad Software Inc), and SAS Enterprise Guide V.7.15 (Cary, North Carolina, USA) for graph generation and statistical analysis. Data are expressed as mean±SEM. Where appropriate, normality of distribution was confirmed using Shapiro-Wilk normality test. Differences between two groups were analyzed using the paired or unpaired Student’s t-test as appropriate for parametric data and the Mann-Whitney test or Wilcoxon signed-rank test for non-normally distributed data. For analysis of three or more groups, one-way analysis of variance tests were performed with Tukey’s or Dunnett’s post hoc test as appropriate. To analyze differences in fold change over time, we used a mixed effects model with a random intercept for the subjects and fixed effects for responders (Y or N). Correlations between two values were performed using Spearman correlation test. Kaplan-Meier curves and log-rank test were used to compare survival outcomes between subgroups. P<0.05 was considered statistically significant unless an adjusted p value was indicated.
Results
Patients and treatment
For the index trial of inhaled rhIL-15, a total of 21 dogs were enrolled including 11 dogs with melanoma and 10 dogs with OSA. Patient characteristics are summarized in table 1. Twenty dogs successfully completed the 14-day course of inhaled rhIL-15. One dog was euthanized after presenting with bicavitary effusion on day 14. A postmortem necropsy confirmed a previously undetected right atrial melanoma lesion extending through the wall of the heart into the cardiac lumen.
Patient demographics and response
Dose escalation and treatment related adverse events
Treatment-related serious adverse events (SAEs) are listed in table 2, and all study related AEs are provided independent of attribution (online supplemental table 1). No fevers, hypotension or other abnormalities were identified during the monitoring period following the first treatment. Several owners reported a mild increase in coughing during or immediately following inhaled treatments at home. One dog enrolled in the 10 µg dose level was allowed to enroll with a grade 3 alkaline phosphatase elevation, a grade 2 alanine transaminase (ALT) elevation, and normal aspartate transaminase (AST). At the completion of inhaled therapy, this patient presented with a new metastatic lymph node and progressive hepatopathy. These were determined to be grade 3 ALT and AST elevations. Based on progressive disease (PD), the owners withdrew the dog from the study without a hepatic ultrasound. The owners also declined necropsy at the time of euthanasia. Without confirmation of hepatic metastasis, the progressive hepatopathy was attributed possibly to treatment. Therefore, this dose level was expanded to enrol three additional dogs. No other SAEs were observed at this dose level, so the study was advanced to dose level 2 (20 μg). Treatment related SAEs were not documented in any additional patients until the 70 µg cohort was reached. At this dose level, we observed clinically evident (grade 3) necrosis or abscessation of confirmed metastatic melanoma in the lymph nodes of two of six dogs. These were categorized as DLTs, and dose escalation was stopped per protocol. Accordingly, the MTD was determined to be 50 µg.
Supplemental material
Treatment-related serious adverse events (AEs)
Clinical response and outcomes
Overall, three patients died or were euthanized prior to day 28 (and were thus not evaluable per protocol), leaving 18 patients evaluable for response (table 1). Among 18 evaluable dogs, 1 dog demonstrated a CR, 1 showed a partial response (PR), 5 had SD, and 11 had PD. Figure 1B depicts a waterfall plot of percent change in size of index lesions when best response was achieved as stratified by responders and non-responders. Figure 1C depicts the summary of all RECIST evaluable patient timepoints over time. Two patients (UCD-IL15-009, UCD-IL15-012) had extensive PD noted on radiographs that precluded RECIST evaluation. One patient with OSA treated at the 10 µg dose demonstrated a strong PR (figure 1D), and one patient with melanoma treated in the 50 µg cohort experienced a complete remission of diffuse metastatic pulmonary lesions (figure 1D). This CR was maintained >1 year until presentation with localizing neurologic signs of unclear etiology. The owners elected euthanasia and declined necropsy such that the cause of neurologic signs was undetermined, although brain metastases from melanoma remained within the differential diagnosis. Notably, there was no clinical or radiographic evidence of recurrent melanoma in any other location. Additionally, there were two patients with OSA with SD (46 and 55 days), and three patients with melanoma with SD (42, 56, and 147 days). Overall, the median survival time from the time of first inhaled rhIL-15 treatment was 82.5 days (range 36–655) for OSA patients and 113.5 days (range 34–407) for melanoma patients. Consistent with our response data (figure 1B,C), we observed that patients showing clinical benefit tended to have improved overall survival compared with non-responders (figure 1E,F), although the differences in survival between responders and non-responders were not statistically significant (p=0.09). The large majority of patients (16 of 18 evaluable dogs) had lung only disease at the time of therapy, having previously undergone treatment of the primary tumor. Interestingly, of the two patients with their primary tumor intact, the clinical course of the primary tumor mirrored the response of the lung metastases (one CR and one PD).
Plasma rhIL-15 quantitation and cytokine induction
Plasma sampling for rhIL-15 quantitation was instituted with patient UCD-IL15-011 (33 µg cohort) as part of our correlative assays. Results of our analysis correlate with human studies examining dosing of rhIL-15,6–8 demonstrating a time of maximum plasma concentration (Tmax) at approximately 4 hours (figure 2A). While rhIL-15 was numerically detectable and increased at 4 hours in all patients, concentrations were nevertheless below the limit of quantification (<20 pg/mL) at the 4-hour plasma sample in 2/2, 1/3, and 4/6 dogs in the 33, 50, and 70 µg cohorts, respectively. These results are consistent with minimal systemic exposure to rhIL-15 after inhalation (figure 2B), as quantifiable plasma levels of rhIL-15 ranged from 20 to 124 pg/mL. In contrast, plasma obtained from dogs with buccal melanoma treated SQ with 3 µg/kg rhIL-15 as part of a separate clinical trial of palliative RT and allogeneic NK transfer yielded 4-hour concentrations for rhIL-15 ranging from 740 to 2954 pg/mL (figure 2C). Demographic data for these patients receiving SQ rhIL-15 are included in online supplemental table 2. Importantly, baseline plasma levels of canine IL-15 were not detected with the human IL-15 ELISA nor was rhIL-15 detectable on the canine Luminex assay. Taken together, these data indicate that systemic exposure to inhaled rhIL-15 is low, but rhIL-15 exposure appears to be maintained at relatively stable plasma levels for up to 6 hours. These data also align with previously published studies demonstrating that the majority of radio-labeled inhaled rhIL-2 remains within the lungs of dogs after inhalation,13 but over 24 hours, slow release into the systemic circulation occurs. Despite low systemic exposure to rhIL-15 via the inhaled route, induction of KC-like and IL-8 were noted in the plasma 4 hours after treatment in the majority of dogs after either SQ or inhaled dosing (figure 2C). Interestingly, we observed that 4-hour plasma levels for both canine KC-like and IL-8 chemokines (figure 2D) were higher in responders compared with non-responders with the differences for KC-like reaching statistical significance (p=0.046), while for IL-8, the differences approached but did not reach statistical significance (p=0.09). In contrast, 4 hours following initial inhaled IL-15 treatment, there was no difference in plasma levels of human IL-15 between responders and non-responders (figure 2D). We did not observe any correlation between absolute canine IL-8 or KC-like plasma levels and human IL-15 levels at 4 hours, nor did we observe a correlation between changes in IL-8 or KC-like levels and change in plasma IL-15 levels (online supplemental figure 3). Unlike human studies examining systemic delivery of rhIL-15, plasma concentrations of IL-6 or IFNγ 4 hours post-treatment were largely unchanged in most dogs (online supplemental figure 4).
Supplemental material
Supplemental material
Supplemental material

Plasma rhIL-15 quantitation and cytokine response. (A) Samples were collected prior to first inhaled rhIL-15 treatment and then at indicated time points for 6 hours after treatment initiation and measured by ELISA. Changes in plasma rhIL-15 concentrations were plotted over time for two patients in each of the 33–70 µg cohorts. (B) Concentration of rhIL-15 in plasma of patients in the 33 µg, 50 µg, and 70 µg inhaled rhIL-15 cohorts as well as those from a separate canine clinical trial where dogs with locally advanced melanoma were treated with palliative RT, allogeneic NK transfer, and 3 µg /kg rhIL-15 SQ to promote NK engraftment. Bars represent plasma rhIL-15 pretreatment and at the presumed Tmax of 4 hours post-treatment for each patient. Plasma rhIL-15 was detectable in all patients but below the limit of quantitation in several patients. Individual groups were compared using one-way analysis of variance with Tukey’s multiple-comparison test. ***P<0.001; **p<0.01. (C) Cytokines induced by rhIL-15, IL-8 and KC-like were quantified in the plasma of all patients (left) as well as separately within the SQ rhIL-15 trial cohort (center) and inhaled rhIL-15 cohorts (right) using a canine multiplex assay. (D) Four-hour KC-like levels (left) were significantly higher in responders compared with non-responders (p=0.046), and a similar trend was noted with 4-hour IL-8 levels (middle) (p=0.092). Responders and non-responders did not show differences in 4-hour rhIL-15 levels (right). rhIL-15, recombinant human interleukin-15; SQ, subcutaneous.
Hematological evaluation
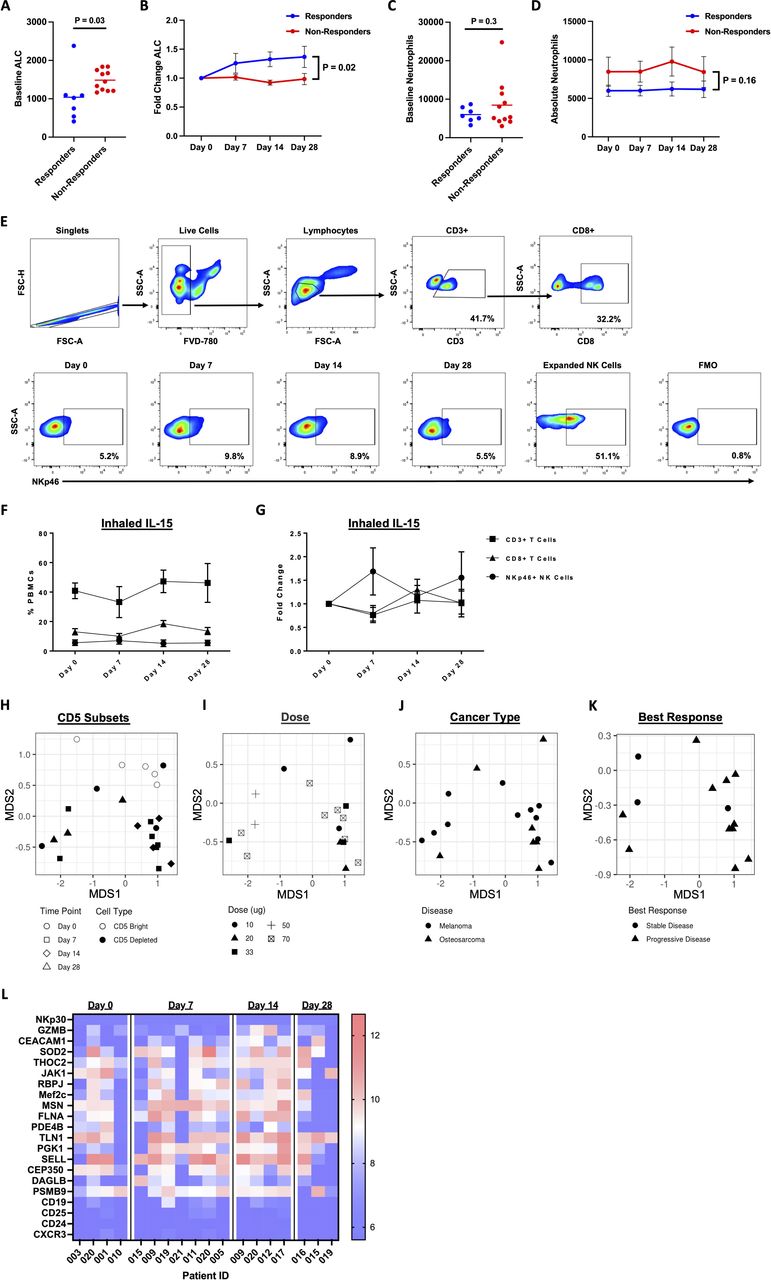
Baseline and induced hematological parameters have previously been shown to correlate with response and/or outcome in dogs and human patients undergoing cancer therapy.25 26 We, therefore, evaluated before, during, and after therapy in all evaluable dogs. As shown in figure 3A, dogs that demonstrated clinical benefit had significantly lower baseline ALC compared with patients with no clinical benefit (1040±650 vs 1485±268, p=0.03). Moreover, as shown in figure 3B, responding patients showed a significant greater fold change increase in ALC compared with non-responding patients (p=0.02). ALC fold change was on average 0.32 higher in responders than in non-responders (SE=0.12, p=0.02). Given that KC-like and IL-8 chemokines are classically associated with neutrophil recruitment and migration,27 we also evaluated blood levels of neutrophils in our inhaled rhIL-15 cohort. As shown in figure 3C, absolute numbers of neutrophils were higher at baseline in non-responders compared with responders (8464±6292 vs 5995±1920), but this difference was not statistically significant (p=0.33). Similarly, as shown in figure 3D, we observed higher blood neutrophil levels at all time points among non-responders compared with non-responders, but these differences were not statistically significant (p=0.16).

Baseline lymphopenia is associated with response to therapy. (A) Baseline absolute lymphocyte counts (ALCs) were determined. Day 0 ALC was lower among responders compared with non-responders (p=0.03 by Kruskal-Wallis Test). (B) Fold change from baseline ALC was on average 0.32 higher in responders than in non-responders (SE=0.12, p=0.020). (C) There is no difference in baseline neutrophil counts between responders and non-responders (p=0.3). (D) Neutrophil counts were higher in non-responders at all time points, but these differences were not statistically significant (p=0.16). (E) Representative flow cytometry staining is shown for PBMCs, including parent gating and CD3+, CD8+, and Nkp46 +lymphocyte subsets. NKp46 staining is shown for one patient for all time points along with primary cultured NK cells and Fluorescence Minus One (FMO) of positive and negative controls. (F) Frequencies of CD3+, CD8 + and NKp46 +lymphocyte subsets in the peripheral blood in patients over time. (G) Fold change of CD3+, CD8 + and NKp46 + lymphocyte subsets were calculated compared with day 0 values as the reference. (H) Multidimensional scaling (MDS) plots based on mathematical distances of differential gene expression for CD5 depleted versus CD5bright subsets using RNA sequencing on PBMC samples at indicated time points. Plot demonstrates significant differences in clustering. (I–K) MDS plot for differential gene expression of CD5 depleted PMBCs enriched for NK cells showing mathematical distances of gene profile based on inhaled IL-15 dose, cancer diagnosis, and best clinical response, respectively. (L) Heatmap of 21 genes of interest demonstrates subset of genes induced in CD5 depleted PBMCs at time points postinitiation of inhaled IL-15 compared with day 0 gene expression. NK, natural killer; PBMC, peripheral blood mononuclear cell.
We also evaluated the frequencies of circulating NK and T cells and differential gene expression of NK cell subsets from patients on the inhaled IL-15 trial using CD3-NKp46+ to identify canine NK cells (figure 3E).22 28 Overall, as shown in figure 3F,G, we observed no significant differences in NK, CD3+, or CD8 + cell frequencies or fold change over time. NK cell frequencies did increase by 1.69±1.11 fold on day 7 (figure 3G), but this was not statistically significant. Given that IL-15 superagonist ALT-803 has been demonstrated to act as a potent immunostimulant that is capable of eliciting both rapid and long-lasting antitumor effects and has shown exciting promise in early stage human clinical trials, including with PD-1 blockade,29 we also performed a first-in-dog proof-of-concept study of ALT-803 to evaluate the safety, toxicity, and preliminary data for response rates in dogs with metastatic cancer. Patient demographics for this small cohort are depicted in online supplemental figure 5A. Recognizing the limitations of analyzing a cohort of four dogs, we observed rapid progression of disease in three dogs with survival ranging from 6 to 26 days following start of ALT-803 therapy. Since these dogs did not reach the 30-day response assessment, they were deemed non-evaluable. The fourth dog demonstrated PD as the best response and survived 117 days from therapy initiation. We performed immune assessment for these patients where specimens were available (online supplemental figure 5B,C). Anecdotally, CD8 + frequencies appeared to increase more than NKp46 + NK cells in absolute numbers, while there was a 2.3±1.1 fold change in NK cell frequencies at day 7, which was not statistically significant (online supplemental figure 5D).
Supplemental material
Using RNA sequencing, we then analyzed the differential gene expression of CD5-depleted PBMCs from a subset of inhaled rhIL-15 dogs for which adequate samples were available (figure 3H–K). As shown by multidimensional scaling plots, there were significant differences in clustering between CD5-depleted and CD5bright subsets consistent with CD5 primarily representing a T cell marker, especially for the cells with strong expression (figure 3H). In contrast, we observed no significant clustering for the differential gene expression of enriched peripheral blood NK cells in the CD5 depleted subset when analyzed by inhaled rhIL-15 dose (figure 3I), cancer type (melanoma vs OSA, figure 3J), or even best response to therapy (figure 3K), reinforcing the complexities of the multiple host/cancer and genetic/epigenetic variables impacting gene signatures. We also analyzed patient’s samples for quantitative differences in differential gene expression at indicated time points (figure 3L). Overall, we did not observe significant changes in the gene expression of canonical NK genes in the peripheral blood of patients on trial, but we did see notable changes in genes linked to NK function and maturation. Three genes of particular interest which were upregulated in peripheral blood NK cells after initiation of therapy were: recombination signal binding protein for immunoglobulin kappa J region, which has been linked to reductions in NK cell populations in peripheral blood when deleted30; myocyte enhancer factor 2C, which has been associated with profound defects in the production of B cells, T cells, NK cells and common lymphoid progenitor cells when deficient31; and moesin, which causes NK cells to exhibit increased cell death and impaired signaling in response to IL-15 when deficient (figure 3L).32
Changes in PBMC cytotoxicity
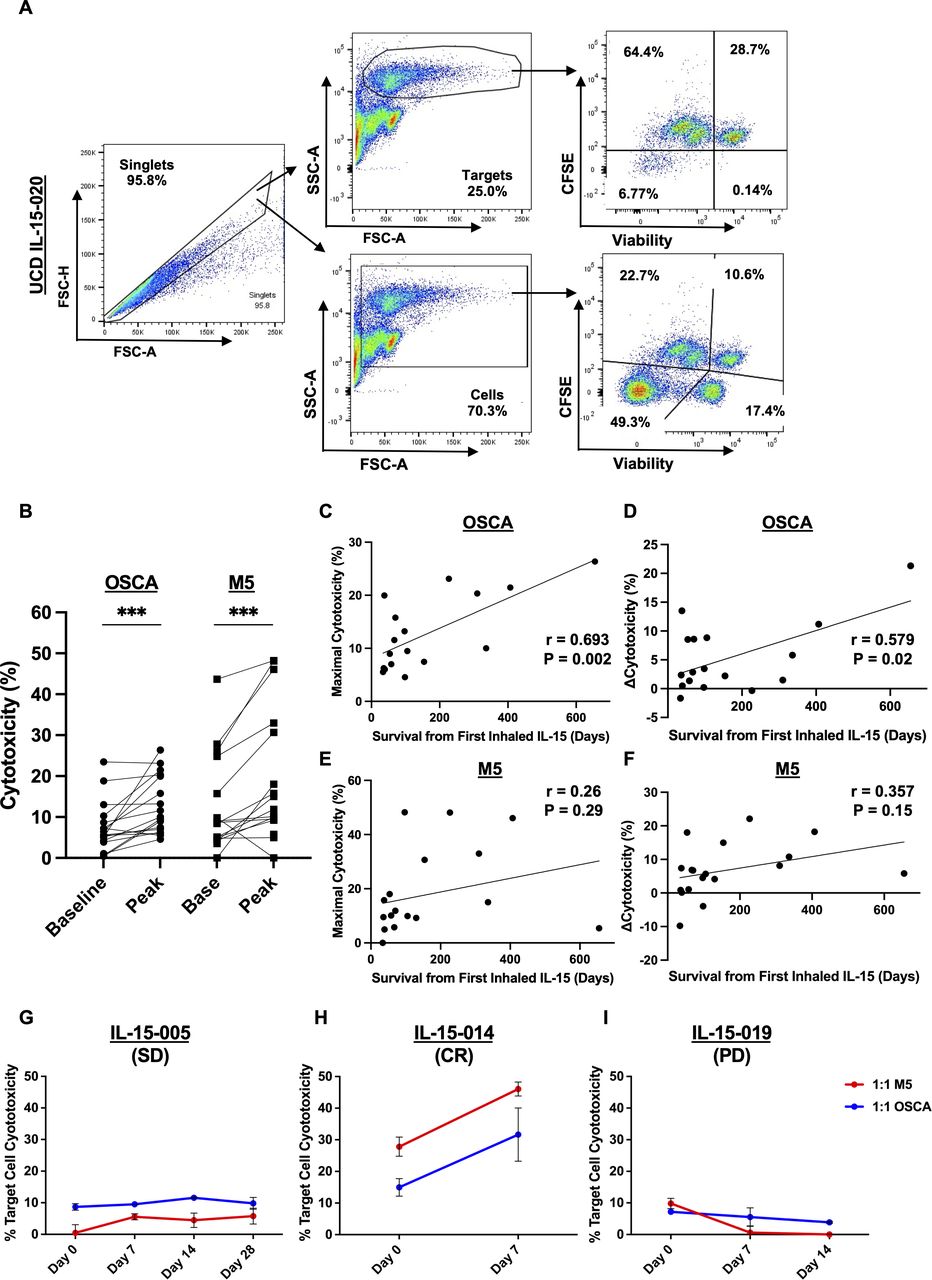
Given reports that have shown that cytotoxicity of circulating NK and cytotoxic T cells also correlates with cancer outcomes,33 34 we sought to analyze the cytotoxicity of patient PBMCs over time against OSA and melanoma targets in vitro using cryopreserved specimens from our patients. As shown in figure 4A, we used a CFSE-labeling technique to delineate target cells from effector cells in this in vitro assay. We verified that changes in cytotoxicity over time were related to treatment rather than random variation by confirming stable cytotoxicity in PBMCs over time from healthy beagles not undergoing therapy (online supplemental figure 2). As shown in figure 4B, PBMCs post-inhaled rhIL-15 treatment demonstrated significantly increased peak cytotoxicity against both OSA and melanoma tumor lines (p<0.001). As shown in figure 4C, cytotoxicity of PBMCs against OSCA-78 correlated significantly with patient survival from inhaled rhIL-15 treatment (r=0.693, p=0.002). Similarly, as shown in figure 4D, the change in cytotoxicity of PBMCs from baseline to peak also demonstrated a significant positive correlation with patient survival from inhaled rhIL-15 treatment (r=0.579, p=0.02). We did not observe a correlation of maximal cytotoxicity of PBMCs against M5 with patient survival from inhaled rhIL-15 (figure 4E) but noted a modest correlation between change in cytotoxicity of PBMCs from baseline to peak and patient survival, which was not statistically significant (r=0.357, p=0.15), as shown in figure 4F. Figure 5G–I represent examples of patients with SD, CR, and PD, respectively.
Supplemental material

Cytotoxic function of patient PBMCs pretherapy and post-therapy. (A) Representative flow cytometry gating distinguishes PBMC effectors from CFSE-labeled OSA and melanoma target cells with dead cells staining positive for Viability Dye 780. (B) Cytotoxicity, calculated by flow cytometry, of PBMCs against osteosarcoma (OSCA-78) and melanoma (M5) cell lines was significantly increased postinhaled rhIL-15 treatment (p<0.001). PBMCs targeting OSCA had significant correlation (Spearman correlation coefficient, ρ) of (C) maximal cytotoxicity and (D) change in cytotoxicity with survival. (E) Maximal cytotoxicity of PBMCs targeting M5 did not show significant correlation to survival. (F) Minimal correlation existed between change in cytotoxicity and survival in PBMCs targeting M5. Representative examples of changes in cytotoxicity, at 1:1 effector to M5 (red) or OSCA (blue) target ratios, in a patient with (G) stable disease (SD), (H) complete response (CR), and (J) progressive disease (PD). PBMCs, peripheral blood mononuclear cells.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
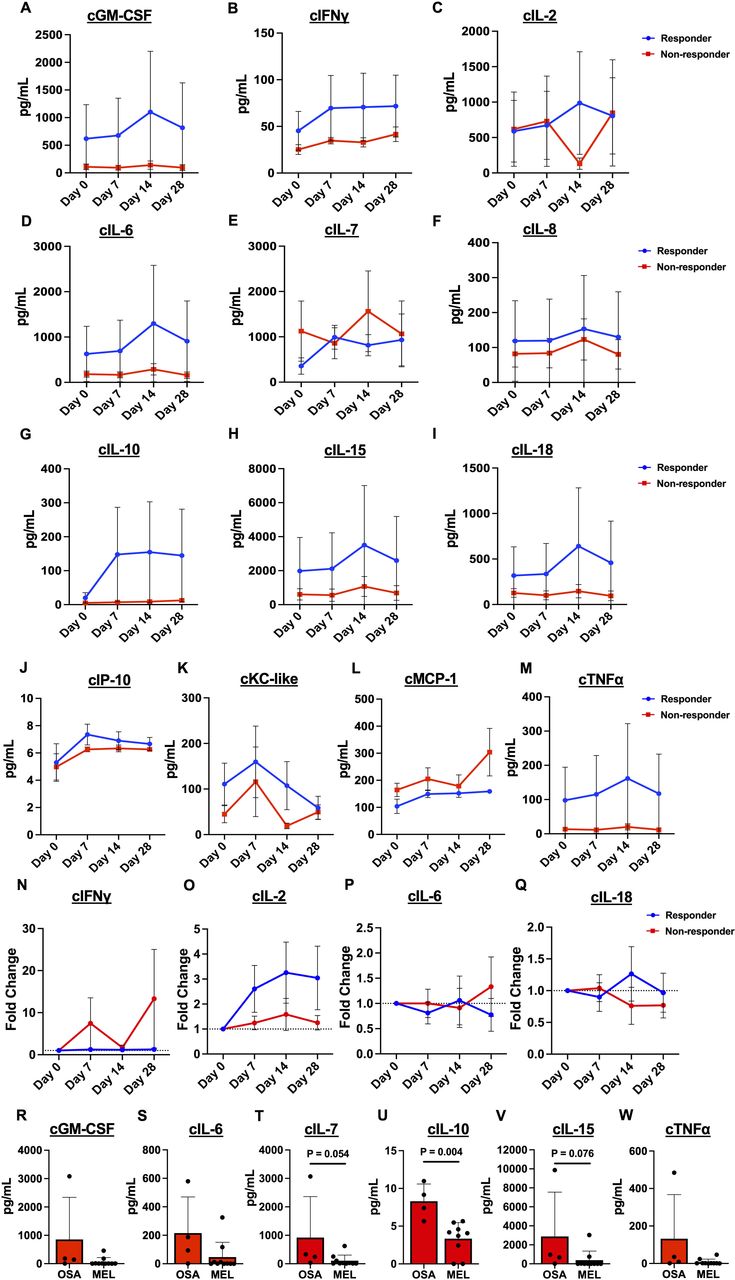
Plasma cytokine levels. Plasma cytokine values measured by canine Luminex assay are depicted comparing responders to non-responders over time: (A) cGM-CSF, (B) cINFγ, (C) cIL-2, (D) cIL-6, (E) cIL-7, (F) cIL-8, (G) cIL-10, (H) cIL-15, (I) cIL-18, (J) cCXCL10, (K) cKC-like, (L) cMCP-1, and (M) cTNFα. Fold change of (N) cINFγ, (O) cIL-2, (P) cIL-6, and (Q) cIL-18 levels fluctuated over time but were not significantly different between responders and non-responders. Concentrations of (R) cGM-CSF, (S) cIL-6, (T) cIL-7, (U) cIL-10, (V) cIL-15, and (W) cTNFα at baseline were higher in patients with OSA compared with those with melanoma with a significant difference observed in cIL-10 (p=0.004). OSA, osteosarcoma.
Analysis of plasma canine cytokines
To assess the effect of inhaled rhIL-15 on the induction of cytokines, we evaluated the absolute concentrations of canine (c) cytokines in plasma over time (figure 5A–M). There was marked variability in plasma concentrations of cGM-CSF, cINFγ, cIL-7, cIL-10, cIL-15, cIL-18, cKC-like, and cTNFα among subjects, and we did not observe any significant differences among responders and non-responders (figure 5A, B, E, G, H, I, K and M, respectively). Figure 5N–Q show the fold change of canine cytokines over time in responders compared with non-responders. Fold change of IFNγ, IL-2, IL-6, and IL-18 over time showed no differences between responders and non-responders, although responders generally showed greater fold change of IL-2 at each time point. Figure 5R–W demonstrate canine cytokine concentrations at baseline in dogs with OSA versus melanoma. The concentrations of cGM-CSF, cIL-6, cIL-7, cIL-10, cIL-15, and cTNFα at baseline were generally higher in the dogs presenting with OSA than those with melanoma. The concentrations of cIL-10 were significantly higher in dogs with OSA compared with those with melanoma (p=0.004, figure 5U). The levels of cIL-7 and cIL-15 were higher at baseline in dogs with OSA compared with those with melanoma, with the differences approaching statistical significance (p=0.054 and p=0.076, respectively) (figure 5T and V).
Discussion
To the best of our knowledge, this is the first study to implement inhaled rhIL-15 as a novel cancer immunotherapeutic in a first-in-dog clinical trial. The primary objectives of this phase 1 trial were to identify treatment-related adverse events (AEs), DLTs, and to determine a MTD for follow-up therapeutic trials. Attribution of AEs can present challenges in late-stage metastatic disease, particularly in subjects who experience rapid progression with short survival times.18 35 Importantly, but also somewhat surprisingly, we observed no evidence of pulmonary-related SAEs or DLTs despite the inhalational route. This is highly relevant for combination therapies, especially given the recent development of canine PD-1 and PD-L1 inhibitory antibodies for clinical usage since these agents in humans have been observed to cause potentially severe pneumonitis.36–38 Instead, the DLT we observed in two dogs in the 70 µg cohort was abscessation or necrosis within regional lymph nodes confirmed to harbor metastatic melanoma. While infection/necrosis of lymph nodes does occasionally occur in the natural progression of metastatic cancer, we concluded that rhIL-15 therapy might be related to the occurrence of these events in our patients. We therefore determined that the MTD of inhaled rhIL-15 in cancer-bearing dogs was 50 µg twice daily. Of note, although the rationale that the highest dose that does not cause dose-limiting toxicity will result in the greatest probability of efficacy may not apply in the era of immunotherapy where clinical benefit may not be dose dependent, our impression is that a higher dose of inhaled rhIL-15 is preferable for phase 2 studies, especially given the uncertainties of using biomarkers for dose selection.
Based on prior inhaled rhIL-2 data in dogs with primary or metastatic gross disease within the lungs, we anticipated that we might see responses to inhaled rhIL-15 in dogs with metastatic OSA or melanoma. While response was not a primary endpoint, we were encouraged to see documented responses, including a PR and a durable CR >1 year in dogs with diffuse and bulky metastatic disease. Equally important is that these responses were prolonged despite receiving a limited 2-week window of inhaled cytokine. This short treatment duration was based on the likelihood that dogs would generate neutralizing antibodies to rhIL-15, making prolonged treatment a risk for allergic responses and immune pathology. Ultimately, the documented response rate per modified RECIST criteria remains low in our study. Human clinical trials evaluating the efficacy of single-agent rhIL-15 for advanced solid tumors via SQ, intravenous bolus, or continuous infusion yielded significant induction of NK and lymphocyte populations, but no documented clinical responses were noted with monotherapy.6 39 While we did observe clinical responses in dogs treated via inhalation, the overall response rate of CR and PR remains relatively modest (11%), and the role for rhIL-15 may likely be most impactful in combination with other existing or novel immunotherapies. At the same time, we anticipate that studies of inhaled canine IL-15 will be highly informative given the potential for delayed responses with immunotherapy (which may convert some patients with SD at early time points to delayed responses after longer exposure). We hypothesize that a longer course of inhaled IL-15 using canine IL-15 will lead to a higher response rate and greater clinical benefit, especially since we and others have shown that canine cytokines (IL-2 and IL-15) are more potent in stimulating immune responses in canine PBMCs and canine NK cells than human cytokines.28 40
The finding that patients with low ALC at baseline were more likely to have responses or SD is also intriguing. While this finding was statistically significant, conclusions based on a small phase 1 study should be interpreted with caution as additional studies are clearly needed. While it is possible that a pre-existing cytokine profile could favor or enhance the activity of inhaled rhIL-15, it is also possible that responses in patients with low lymphocyte counts could be unrelated to the activity of rhIL-15. Depletion of lymphocytes improves the effect of adoptive cell transfer by eliminating Tregs and by removing endogenous lymphocytes, thereby leading to more ‘space’ for adoptively transferred cells to proliferate in the setting of increased availability of homeostatic cytokines like IL-7 and IL-15.41–43 Thus, the decreased baseline ALC seen in responders in our cohort could be linked to less competition for exogenous cytokine among endogenous NK and cytotoxic T cells.
Distinct tumor types may also contribute to differences in cytokine profiles and response to treatment. Although melanoma and OSA are both aggressive cancers with poor prognosis, they have unique immune phenotypes in both dogs and human.18 19 21 40 Plasma cytokine profiles were generally higher in dogs with OSA than dogs with melanoma, although only IL-10 was significantly higher in OSA. IL-10 can promote increased cytotoxicity and IFNy secretion in NK cells44 but has an overall immunosuppressive effect on immune cells, contributing to cancer cells’ immune escape.45 Concentrations of IL-7, a critical cytokine in the homeostatic expansion of T cells,43 46 showed a trend to be higher in OSA versus melanoma, although remained highly variable among patients. Overall, this suggests that cytokine elaboration can be related to tumor type although other immune-modifying factors such as age, sex, and body habitus are clearly also important. Similarly, immune cell populations and cytokine patterns in the blood may not represent mechanisms of response or resistance in the lung TME. For example, NK cells in healthy human lungs comprise approximately 10% of tissue-resident lymphocytes and primarily express a CD56dim perforinhigh phenotype.47 48 Neoplastic transformation of lung tissue recruits largely non-cytotoxic CD56bright cells,47 and intravenous infusion of IL-15 induces an expansion of CD56bright cells with enhanced cytotoxic function and increased cytokine production compared with CD56dim.4 Inhaled rhIL-15 ultimately may have many different effects in the target tissue versus PBMCs, and further studies are required to determine effects of inhaled rhIL-15 on the native lung and the TME of lung metastases, as well as any crosstalk.
In summary, our first-in-dog phase 1 clinical trial using a novel inhaled delivery route of rhIL-15 produced promising clinical activity and identified an MTD of 50 µg twice daily. We also observed that the cytotoxicity of circulating effector cells in the blood while on therapy as well as baseline ALC appear to correlate with clinical benefit. Ultimately, these results support ongoing investigation of inhaled rhIL-15 in treating dogs with metastatic melanoma and OSA with an emphasis on combinatorial approaches.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
All experiments involving canine patients were approved by the Veterinary Medical Teaching Hospital Clinical Trials Review Board and the Institutional Animal Care and Use Committee at the University of California, Davis. Ethical approval for all studies was obtained from the UC Davis Veterinary Medical Teaching Hospital Clinical Trials Review Board and the UC Davis Institutional Animal Care and Use Committee (IACUC #21949, #21620, and #20668).
Acknowledgments
Khurshid Iranpur, Ryan Nielsen, and Sharon Sanghar for expert technical assistance and data management. Teri Guerrero, Jacque Young, Emily Phenix, and Kate Hodges in the UC Davis Veterinary Center for Clinical Trials and the Clinical Trials Residents for providing compassionate patient care.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
RBR, DY and SMC contributed equally.
Contributors RBR, SLS, WJM, MSK, and RJC designed the study. RBR, DY, SJJ, LEF, RVB, EGJ, JHB, JW, LAW, KW, EES, SSW, KAS, SA-N, ATL, WC, MSK, and RJC conducted the experiments and collected the data. SLS provided statistical analysis. RBR, DY, SMC, SJJ, AMR, CD, SLS, AAG, and RJC analyzed the data. RBR, DY, SMC, AMR, and RJC wrote the manuscript. All authors provided critical review of the manuscript. RBR and RJC are responsible for the overall content as guarantors.
Funding This work was supported in part by National Institutes of Health/National Cancer Institute grant U01 CA224166-01 (RBR and RJC), R03CA252793 (RJC), K01OD026526 (LW), and T32CA251007 (AMR, RJC, and MSK). This work was also supported in part by funds from the UC Davis Comprehensive Cancer Center and the University of California Davis Flow Cytometry Shared Resource Laboratory with funding from the NCI P30 CA093373 (Cancer Center), and S10 OD018223 (Astrios Cell Sorter), and S10 RR 026825 (Fortessa Cytometer) grants, with technical assistance from Ms Bridget McLaughlin and Mr Jonathan Van Dyke. Additional support came from the UC Davis Center for Companion Animal Health and from Maxine Adler Endowed Chair funds.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.