Article Text

Abstract
Until recently, most patients with sentinel lymph node-positive (SLN+) melanoma underwent a completion lymph node dissection (CLND), as mandated in published trials of adjuvant systemic therapies. Following multicenter selective lymphadenectomy trial-II, most patients with SLN+ melanoma no longer undergo a CLND prior to adjuvant systemic therapy. A retrospective analysis of clinical outcomes in SLN+ melanoma patients treated with adjuvant systemic therapy after July 2017 was performed in 21 international cancer centers. Of 462 patients who received systemic adjuvant therapy, 326 patients received adjuvant anti-PD-1 without prior immediate (IM) CLND, while 60 underwent IM CLND. With median follow-up of 21 months, 24-month relapse-free survival (RFS) was 67% (95% CI 62% to 73%) in the 326 patients. When the patient subgroups who would have been eligible for the two adjuvant anti-PD-1 clinical trials mandating IM CLND were analyzed separately, 24-month RFS rates were 64%, very similar to the RFS rates from those studies. Of these no-CLND patients, those with SLN tumor deposit >1 mm, stage IIIC/D and ulcerated primary had worse RFS. Of the patients who relapsed on adjuvant anti-PD-1, those without IM CLND had a higher rate of relapse in the regional nodal basin than those with IM CLND (46% vs 11%). Therefore, 55% of patients who relapsed without prior CLND underwent surgery including therapeutic lymph node dissection (TLND), with 30% relapsing a second time; there was no difference in subsequent relapse between patients who received observation vs secondary adjuvant therapy. Despite the increased frequency of nodal relapses, adjuvant anti-PD-1 therapy may be as effective in SLN+ pts who forego IM CLND and salvage surgery with TLND at relapse may be a viable option for these patients.
- Melanoma
- Adjuvants, Immunologic
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Prior to 2017, most patients with clinically node-negative, sentinel lymph node-positive (SLN+) melanoma underwent completion lymph node dissection (CLND). Several clinical trials have explored the prognostic value of SLN status and the clinical benefit of CLNDs. The results of the multicenter selective lymphadenectomy trial-I (MSLT-I) demonstrated significantly worse melanoma-specific survival among patients with a positive SLN biopsy compared with patients with a negative SLN biopsy, and found that pathological status as identified by SLN biopsy had significant prognostic value.1
In the MSLT-II trial, patients with SLN+ melanoma were randomized to CLND or nodal basin ultrasound surveillance, and the 3-year melanoma-specific survival rates were similar between groups.2 In the DeCOG-SLT trial, there was also no significant difference in the 5 year recurrence-free survival (RFS) or overall survival (OS) rates between the CLND or observation groups.3 As a result of these studies, most patients with SLN+ melanoma no longer undergo a routine CLND; instead, these patients are monitored with imaging and clinical exams at regular intervals.
Currently, there are several adjuvant systemic therapies available for patients with melanoma. In the CheckMate-238 trial, adjuvant nivolumab resulted in significantly longer RFS (4-year RFS rate, 51.7% vs 41.2%; p<0.001) than adjuvant ipilimumab4 in patients with resected stage IIIB, IIIC, or IV melanoma.5 In the EORTC1325/Keynote-054 trial, patients with stage IIIA/B/C melanoma randomized to adjuvant pembrolizumab similarly had a significantly longer RFS than those who received placebo (3-year RFS rate, 63.7% vs 44.1%; p < 0.001).6 In the COMBI-AD trial of adjuvant BRAF/MEK-inhibitor therapy, dabrafenib and trametinib also demonstrated improved RFS and OS compared with placebo.7
One key eligibility factor common to all the aforementioned clinical trials of adjuvant therapy was that a CLND needed to be performed after a positive SLN biopsy before study enrollment and commencement of adjuvant therapy. (In preliminary data presented from the CheckMate-915 trial comparing adjuvant nivolumab + ipilimumab to nivolumab in stage IIIB/C/D/IV melanoma, 64% of patients underwent CLND.8
In contrast, because of the results of the MSLT-II and DeCOG-SLT studies and current treatment algorithms,9 most patients with SLN+ melanoma currently forgo CLND before starting adjuvant systemic therapy, leading to a large proportion of SLN-positive patients receiving adjuvant anti-PD1 therapy without CLND. However, outcomes for patients treated with adjuvant systemic therapy after a positive SLN+ without a CLND are not known. In this international multicenter retrospective analysis, we explored real-world outcomes associated with adjuvant systemic therapy, particularly anti-PD-1 therapy, among patients with SLN+ melanoma who did not undergo an immediate (IM) CLND.
Methods
Patients
We conducted a multicenter retrospective analysis of patients with SLN+ melanoma treated at 21 centers in the USA, Europe, and Australia. Patients were eligible if they had cutaneous melanoma, underwent wide local excision of the primary site, and had an SLN biopsy demonstrating pathologically involved SLN(s) after July 1, 2017 (the month that the MSLT-II trial results were published), regardless of whether they had a CLND. SLN biopsy and any subsequent CLND were performed per standard techniques.10 Eligible patients were ≥18 years of age with melanoma of any tumor thickness and clinically negative regional lymph nodes before excision and SLN biopsy. Tumor specimens were evaluated per the pathology protocols from each participating institution. Tumors were to have clear margins after wide excision (including cases that required re-excision to achieve this), with metastatic involvement of SLN(s). SLN biopsies and subsequent treatment, including the administration of adjuvant treatments, were performed at each participating site per the discretion of the treating physicians. Patients were also selected for a CLND surgery per the discretion of the treating physicians at each participating institution. Data collected included patient demographics, tumor pathology, operative details, imaging results, and adjuvant treatment details, follow-up, and types of treatments received if there was disease relapse. The aims of this analysis were to assess RFS, OS, patterns of relapse and postrelapse treatments used among patients undergoing adjuvant systemic therapy in a real-world setting since publication of the MSLT-II trial.
Statistical analyses
The Kaplan-Meier method was used to estimate survival probabilities (RFS and OS) and corresponding 95% CIs. RFS was defined as the date from SLN biopsy to the date of melanoma relapse, and OS was defined as the date from SLN biopsy to death from any cause. Groups were compared using the log-rank test. A Cox proportional hazards regression model was used to assess associations with baseline factors. Response outcomes were summarized using frequency and proportions. Statistical analyses were performed using SAS V.9.4. All tests were two sided; p values≤0.05 were considered statistically significant.
Results
Patient characteristics
A total of 1162 patients from 21 institutions met the above eligibility criteria (online supplemental figure 1). Of these patients, 462 (40%) received adjuvant systemic therapy after a positive SLN biopsy, and 74 of them underwent a prior CLND, with regional differences: 20% (67) of 338 patients from USA underwent CLND, with 12% (4) of 33 of patients from Europe and 3% (3) of 91 patients from Australia. Data from the entire cohort including the 700 patients who did not receive adjuvant systemic therapy was previously reported,11 but as a whole, these patients were statistically more likely to have stage IIIA vs IIIC/D melanoma than those who received adjuvant systemic therapy (per American Joint Committee on Cancer, AJCC v8; 42% vs 19%; p < 0.00001) and more likely to have only 1 (vs ≥2) SLN+(p < 0.00001).
Supplemental material
Adjuvant anti-PD-1 therapy with or without prior CLND
Of the 462 patients treated with adjuvant systemic therapy, 386 received adjuvant anti-PD-1 monotherapy (table 1). Nearly all patients received adjuvant nivolumab, except for 36 (9%) who received pembrolizumab. The 24-month RFS for these 386 patients was 66% (95% CI 61% to 71%). Online supplemental figure 2 shows differences in RFS between various clinical characteristics. Of these 386 patients, 60 underwent IM CLND before receiving adjuvant anti-PD-1 treatment, whereas the remaining 326 did not have IM CLND. These 326 patients were significantly less likely to have extranodal extension (ENE) (p < 0.001) or stage IIIC disease (p=0.008), or received adjuvant nodal basin radiation compared with those who underwent IM CLND (p<0.001) (table 1). Median follow-up was 21 months; median duration of anti-PD-1 treatment was 11 months, with 44 patients (13%) still on treatment.
SLN+ melanoma and adjuvant anti–PD-1 therapy—patients with and without immediate CLND
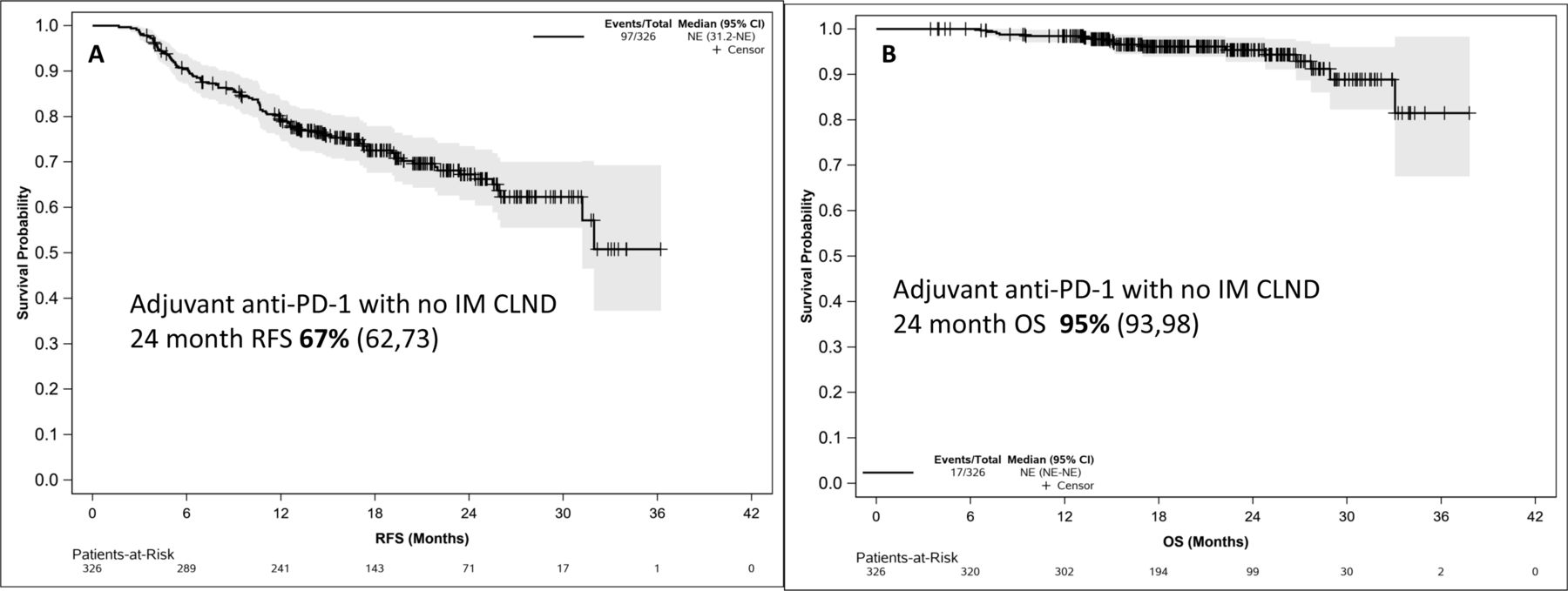
In the 326 patients who received adjuvant anti-PD-1 without IM CLND, the 12-month and 24-month RFS rates were 79% and 67%, respectively (median not reached) (figure 1A). The 24-month OS rate was 95% (93, 98). (Figure 1B) In the Keynote-054 adjuvant trial, patients with stage IIIA melanoma per AJCC v7 staging needed at least one lymph node metastasis >1 mm for eligibility; from the 326 patients without IM CLND, 258 patients met this lymph node criteria. For this subgroup of 258 patients, the 24 month RFS rate was 64% (57, 71). (online supplemental figure 3) For stage III disease, the CheckMate-238 adjuvant trial only included those with AJCC V.7 stage IIIB/C melanoma; for the 193 patients from the 326 who met these particular criteria, the 24-month RFS rate was also 64% (57, 72). (online supplemental figure 3)
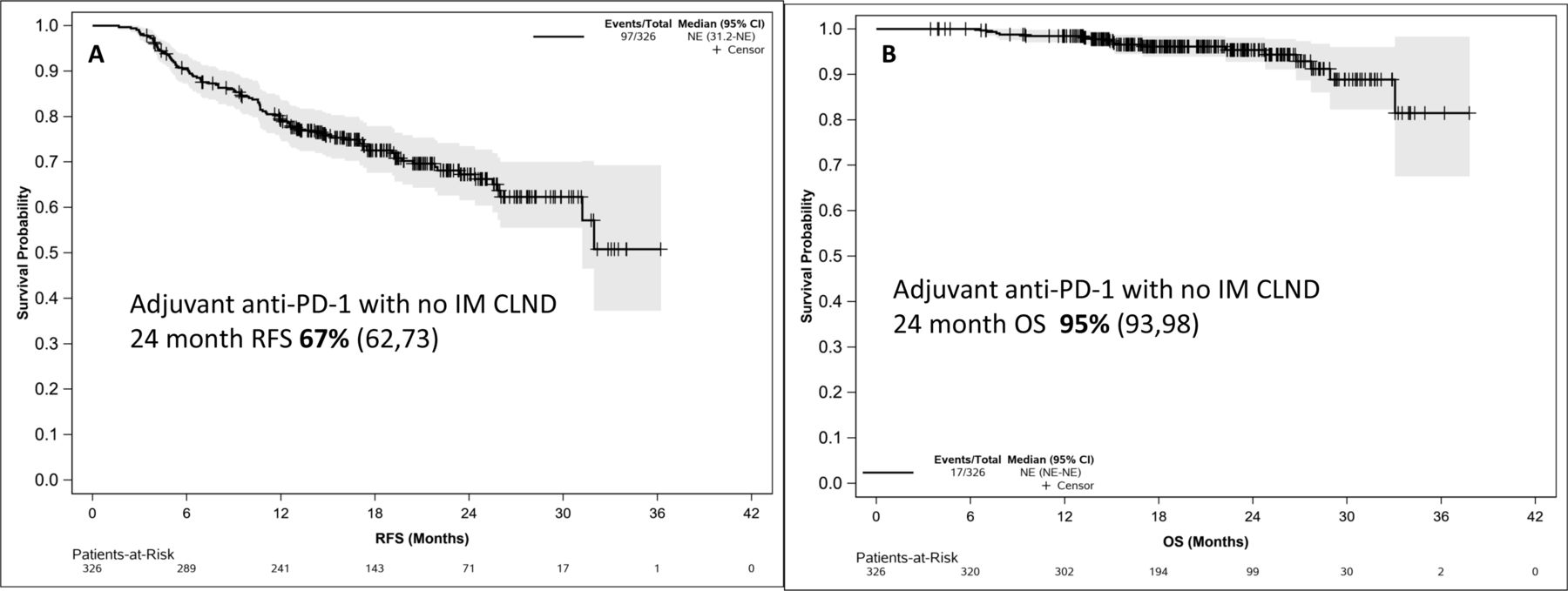
(A) RFS and (B) OS in SLN+ melanoma with adjuvant anti-PD-1 therapy in patient with no immediate CLND (n=326). CLND, completion lymph node dissection; IM, immediate; OS, overall survival; RFS, relapse-free survival; SLN+, sentinel lymph node-positive.
Figure 2 shows differences in RFS between various characteristics in the 326 total patients treated with adjuvant anti-PD-1 therapy without IM CLND. Patients with an SLN tumor deposit >1 mm had worse RFS than those with ≤1 mm (24-month RFS 60% vs 75%, HR 2.11, p=0.0006); median SLN tumor deposit was 2 mm and 0.95 mm, respectively, for patients with and without relapse. Worse RFS rates were seen in patients with an ulcerated primary (24 month RFS 63% vs 75% in non-ulcerated; HR 1.59 (95% CI 1.04 to 2.45), p=0.03) and with AJCC V.8 stage IIIC/D melanoma (24 month RFS, 61% vs 82% with stage IIIA melanoma; HR 2.36 (95% CI 1.27 to4.39) p=0.02).

Relapse-free survival between different baseline characteristics. In the 326 patients without CLND treated with adjuvant anti-PD-1, RFS based on ulcerated primary (A), stage (B), head/neck primary (C), number of positive SLN (D), extranodal extension (E), and SLN tumor deposit (F) is shown. CLND, completion lymph node dissection; RFS, relapse-free survival; SLN, sentinel lymph node.
There was a trend toward worse RFS with ENE (24-month RFS 56% vs 68% without ENE; HR 1.72 (95% CI 0.86 to 3.45), p=0.12), which did not reach statistical significance perhaps due to only 9 patients with ENE in this group. The number of SLN+ tumors (one vs ≥2, p=0.3) the location of the primary tumor, head/neck versus other (p=0.7), or presence or lack of microsatellitosis (p=0.7) did not impact RFS.
In the 60 patients who had IM CLND prior to adjuvant anti-PD-1, 12 months and 24 months RFS was 63% and 56% respectively, with median RFS of 33.5 months. When accounting for difference in staging (compared with the no-CLND patients) using a multivariable Cox proportional hazards regression model, there was no statistically significant difference in RFS between the IM CLND and no IM CLND groups (HR 1.40; 95% CI 0.90 to 2.19; p=0.133). There was also no difference in RFS between patients with SLN tumor deposit >1 mm vs ≤1 mm, although as 45 of the 60 patients in this cohort had stage IIIC/D melanoma, this likely blunted observing effects of tumor characteristics on RFS (online supplemental figure 4).
Other adjuvant therapies without prior CLND
Of the 76 patients who received an adjuvant systemic treatment other than anti-PD-1, 44 received adjuvant BRAF/MEK-inhibitors; the remaining 32 were treated on clinical trials (such as nivolumab plus ipilimumab) or with adjuvant ipilimumab. Of the 44 patients who received adjuvant BRAF/MEK-inhibitors, 37 did not undergo IM CLND. There was also no difference in RFS (24-month RFS 65% (47, 91)) between the 37 patients who received adjuvant BRAF/MEK-inhibitor therapy and the 81 patients with BRAFV600-mutant melanoma who received adjuvant anti-PD-1 without IM CLND (p=0.1). This RFS was also similar to the 24 month RFS rate of 67% observed in the COMBI-AD trial which required CLND.7
Patterns of relapses and postrelapse treatments
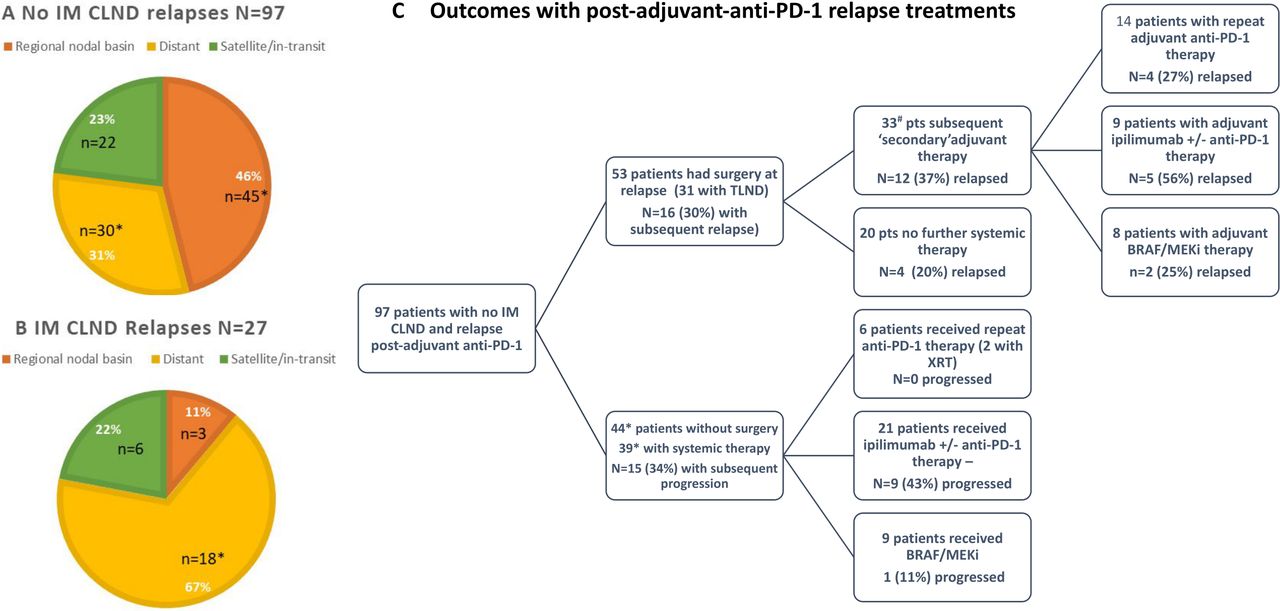
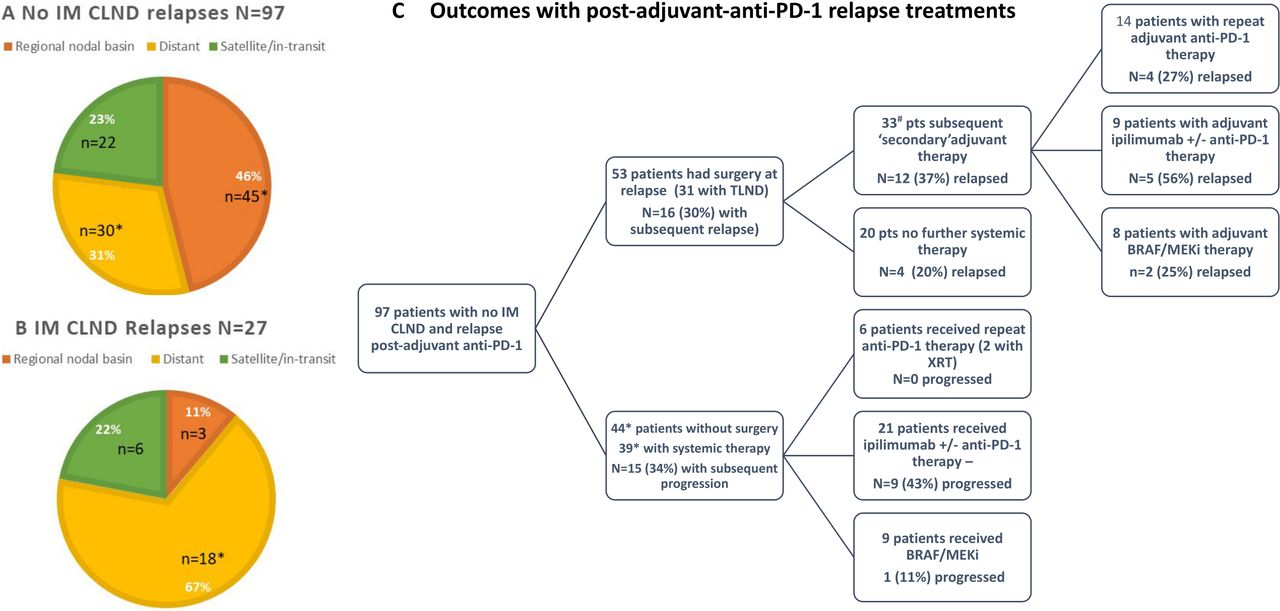
Of the patients who relapsed on adjuvant anti-PD-1 therapy, those without IM CLND had a higher rate of relapse in the regional nodal basin at first recurrence than those with IM CLND (46% vs 11%, respectively, p=0.001) (figure 3). Median follow-up postrelapse was 10.4 months. Of the 97 patients without IM CLND who relapsed after adjuvant anti-PD-1 therapy, 53 (55%) underwent complete surgical excision (with 30% relapsing again). Of the 53, 31 patients underwent a therapeutic lymph node dissection (TLND). Thirty-three of these 53 patients (63%) postsurgery underwent what may be termed ‘secondary’ adjuvant therapy (figure 3 and online supplemental table 1).
Supplemental material
{kind=link}
{kind=link}
{kind=link}
Patterns of relapse and postrelapse treatments in patients. (A) *11 patients with regional nodal Basin relapse had concurrent intransit/satellite relapse *9 patients with distant relapse had concurrent nodal relapse. (B) *One patient with distant relapse had concurrent nodal relapse and two had concurrent in-transit relapse. (C) *5 of 44 patients with relapse without further surgery or drug therapy—1 intralesional therapy, 1 radiation only, 1 unknown treatment—3 of 5 decreased. Of 39 patients, 3 enrolled in clinical trials (anti-PD-1 with intralesional therapy). #2 of 33 with chemotherapy or unknown systemic treatment. CLND, completion lymph node dissection; IM, immediate; TLND, therapeutic lymph node dissection; XRT, radiation therapy.
For these 53 patients with surgery at first relapse, there was no statistically significant difference in secondary relapse rates between those who received secondary adjuvant systemic therapy (n=33) or who were placed on observation (n=20) (p=0.2) There was no difference in relapse rates between different types of secondary adjuvant therapy (anti-PD-1 (n=14) vs BRAF/MEKi (n=8), p=0.9; anti-PD-1 vs ipilimumab-based therapy (n=9), p=0.17). For the 44 patients without surgery at first relapse, there were also no difference in rates of disease progression based on type of systemic therapy received (anti-PD-1 (n=6) vs BRAF/MEKi (n=9), p=0.09; anti-PD-1 vs ipilimumab-based therapy (n=21), p=0.06).
Of the 27 of 60 patients who relapsed with adjuvant anti-PD-1 therapy after IM CLND, 23 (85%) received further systemic therapy, while only 7 (26%) underwent surgical excision at relapse (for intransit/satellite recurrences) (online supplemental table 1).
Detection of sites of relapse
For the 97 patients without IM CLND who relapsed post adjuvant anti–PD-1, 33 (34%) of relapses were primarily were detected via clinical exam, 9 (9%) primarily via ultrasound of the SLN+ nodal basin, and the remaining 57% with CT or PET/CT imaging. For the 27 patients who relapsed with IM CLND, 7 (26%) were detected primarily with clinical exam, none via ultrasound, and remaining 74% with CT or PET/CT.
Discussion
Although previous trials studying adjuvant therapy mandated CLND for patients with SLN+ melanoma, this practice has fallen out of favor following the publication of the MSLT-II and DeCOG-SLT studies. As a result, following a diagnosis of SLN+ melanoma, oncologists in many countries now routinely start patients on adjuvant systemic therapy without a prior CLND.
The 24-month RFS rate of 67% with adjuvant anti-PD-1 without IM CLND in these 326 patients is similar to rates reported in the adjuvant nivolumab5 and pembrolizumab6 trials (71% and 68.3%, respectively), despite the fact that these trials mandated a CLND for all SLN+ disease. In the Keynote-054 trial, the 517 patients treated with adjuvant pembrolizumab had a 24-month RFS of 68.3%, similar to the 64% observed in the subgroup of 258 patients without IM CLND who fit the same eligibility criteria used in the Keynote-054 trial. The Keynote-054 trial included a smaller percentage of patients with AJCC v8 Stage IIIA melanoma (8%), than the patients in this analysis (21%), while the ratio of patients with stage IIIC/D melanoma was similar at 58% vs 55%. The Keynote-054 trial data were also reanalyzed using the AJCC v8 criteria, with similar RFS across the stages, with 24 month RFS of approximately 85% compared with 82% with this cohort for stage IIIA, 72% for stage IIIB compared with 68% for this cohort, 65% and 45% for stage IIIC and IIID, respectively, compared with 61% for this cohort.
In the CheckMate-238 trial, the 24-month RFS was 64% for the 368 patients treated with nivolumab with stage IIIB/IIIC melanoma per AJCC V.7 criteria.12 In the subgroup of 193 patients meeting those staging criteria treated with anti-PD-1 but without CLND, 24 month RFS was similar at 64%. Furthermore, in the preliminary data from the CheckMate-915 trial where two-thirds of patients had IM CLND, 2-year RFS rate for the nivolumab alone arm was 63.2%. While a direct comparison to clinical trial data from adjuvant anti-PD-1 trials is not possible, these RFS rates nonetheless suggest that omitting upfront CLND prior to adjuvant therapy does not appear to impact RFS.
However, the results of this analysis indicate there may be differences in the patterns of relapse. The patients with no IM CLND before adjuvant anti-PD-1 had a significantly higher rate of locoregional relapses (69% vs 33%) compared with those who underwent IM CLND. In the Keynote-054 and CheckMate-238 trials, of the 135 and 154 patients who relapsed in the pembrolizumab and nivolumab arms, respectively, 57 (42%) and 61 (40%) relapsed with initial locoregional-only relapse, while remaining relapses were distant, similar to the IM CLND group rates in this cohort. Larger SLN tumor deposit also increased the risk of relapse in those without IM CLND, which may be related to the rate of increased regional nodal basin relapse in this group.
Given the much higher rate of locoregional relapse on adjuvant anti-PD-1 without IM CLND, over one-third of these patients underwent a TLND at the time of relapse, suggesting it may be possible to use lymph node dissection as salvage therapy. The rate of surgery overall at relapse was much lower in the IM CLND cohort. This also highlights the benefit of active surveillance of the at-risk nodal basin via imaging, as two-thirds relapses in these patients were detected via imaging. Of the patients without IM CLND who had surgery for relapse with adjuvant anti-PD-1, there was no significant difference in rates of a second relapse between patients who received secondary adjuvant therapy vs observation. There was also no significant difference in relapse rates between different types of secondary adjuvant therapy, although follow-up is limited.
Thus, questions arise on how to best treat these patients post-surgical resection of relapsed melanoma—is there a role for secondary adjuvant systemic therapy versus observation until/if there is another relapse? If secondary adjuvant therapy is used, is it beneficial to continue a patient post-TLND on the same presurgery adjuvant anti-PD-1 regimen that perhaps prevented a distant relapse, or is changing to an adjuvant regimen that includes ipilimumab or BRAF-targeted therapy preferable in these cases? The widely differing practices within and across the 21 institutions demonstrate the lack of conclusive answers to these questions, which longer follow-up and future clinical trials may help to answer. In addition, an analysis of 147 patients with stage III/IV melanoma who relapsed with adjuvant anti-PD-1 therapy suggests that whether patients relapsed while on or off adjuvant anti-PD-1 may also be a factor in benefit from rechallenging with the same drug.13
The limitations of this analysis include its retrospective approach, the physicians’ biases and patients’ preferences that may have influenced deciding which patients underwent a CLND after a positive SLN biopsy, and the types of treatments patients received both post-resection and at the time of relapse. In addition, a median follow-up of 21 months may not reflect patterns of late relapses that might be seen in patients who may recur many years after adjuvant systemic therapy.
In conclusion, this is the largest analysis to date of adjuvant systemic therapy among patients with SLN+ melanoma not treated with IM CLND. In the modern era of managing SLN+ melanoma without upfront CLND, despite a much higher rate of nodal relapses and surgical salvage, adjuvant anti-PD-1 therapy confers a similar benefit to that historically seen in trials in which CLND was mandated.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study concept was approved by the institutional review board of each participating institution and conducted in accordance with Good Clinical Practice guidelines as defined by the International Conference on Harmonization.
Acknowledgments
Editorial assistance was provided by the Moffitt Cancer Center’s Scientific Editing Department by Dr. Paul Fletcher & Daley Drucker. No compensation was given beyond their regular salaries.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @davidgyorki, @SurginSydney, @jamessunmd
JZ and NIK contributed equally.
ZE and KKB contributed equally.
Contributors All authors contributed to the acquisition of data for this work and revised and reviewed manuscript. ZE, KB, JZ, and NIK contributed to the planning of this manuscript and ZE drafted the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests ZE: Advisory boards: Array, Pfizer, OncoSec, Regeneron, Genentech, Novartis, Natera. Research funding: Novartis, Pfizer, Boehringer-Ingelheim. JFT: Advisory boards: BMS Australia, MSD Australia, GSK, Provectus Inc. Travel support: GSK, Provectus Inc and Novartis. TJH: Research funding: Genentech, SkylineDX. EKB: Research funding: SkylineDx, Honorarium: Excite International inc. DEG: Honoraria: BMS, Novartis, Q biotics. GK; Advisory Board: Merck. AVA: Advisory Boards: Amgen, Bristol-Myers Squibb, Novartis, MSD-Merck, Merck-Pfizer, Pierre Fabre, Provectus, Sanofi, Sirius Medical, 4SC Research funding: Amgen, Merck-Pfizer. JV: Speaker: Caste Biosciences. GB: Research funding: Istari Oncology, Delcath, Oncosec Medical, Replimune, Checkmate Pharmaceuticals. ROB: Advisory boards: Amgen, BD/BARD, Bristol-Myers Squibb, Merck Sharp & Dohme, Novartis, Roche and Sanofi Genzyme. Research funding: Bristol-Myers Squibb, SkyLineDx. Speaker honorarium: Roche and Pfizer. Shareholder in SATMEG Ventures AB. NIK: Advisory boards: Bristol-Myers Squibb, AstraZeneca, Regeneron, Array, Immunocore, Merck, Incyte, Jounce Therapeutics,Pfizer,Novartis, Nektar,Castle Biosciences, Instil Bio. Research funding: Bristol-Myers Squibb, Merck, Novartis, Celgene, Replimune, Amgen, Regneron, HUYA, GlaxoSmithKline Stocks: Bellicum Pharmaceuticals, Amarin Corporation, Asensus Surgical.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.