Article Text

Abstract
Background Immune-related adverse events due to immune checkpoint inhibitors (ICIs) are not always effectively treated using glucocorticoids and it may negatively affect the antitumor efficacy of ICIs. Interventional studies of alternatives to glucocorticoids are lacking. We examined whether interleukin-6 blockade by tocilizumab reduced ICI-induced colitis and arthritis.
Patients and methods Patients with solid cancer experiencing Common Terminology Criteria for Adverse Events (CTCAE v5.0) grade >1 ICI-induced colitis/diarrhea (n=9), arthritis (n=9), or both (n=2) were recruited and treated with tocilizumab (8 mg/kg) every 4 weeks until worsening or unacceptable toxicity. Patients were not allowed to receive systemic glucocorticoids and other immunosuppressive drugs within the 14-day screening period. The primary endpoint was clinical improvement of colitis and arthritis, defined as ≥1 grade CTCAE reduction within 8 weeks. Secondary endpoints were improvements and glucocorticoid-free remission at week 24; safety; radiologic, endoscopic, and histological changes; and changes in plasma concentrations of C reactive protein, cytokines (IL-6, IL-8, and IL-17), and YKL-40.
Results Nineteen patients were available for efficacy analysis; one patient was excluded due to pancreatic insufficiency-induced diarrhea. Patients received treatment with pembrolizumab (n=10) or nivolumab (n=4) as monotherapy or ipilimumab and nivolumab (n=5) combined. Seven patients had been initially treated with glucocorticoids, and two of them also received infliximab. Ten patients continued ICI therapy during tocilizumab treatment. The primary endpoint was achieved in 15 of 19 (79%) patients. Additional one patient had ≥1 grade reduction at week 10, and another patient had stabilized symptoms. At week 24, ongoing improvement without glucocorticoids (n=12), including complete remission (n=10), was noted. Five patients had grades 3–4 treatment-related adverse events, which were manageable and reversible.
Conclusions Tocilizumab showed promising clinical efficacy and a manageable safety profile in the treatment of ICI-induced colitis and arthritis. Our findings support the feasibility of randomized trials of immune-related adverse events.
Trial registration number NCT03601611.
- Immunotherapy
- Cytotoxicity, Immunologic
- CTLA-4 Antigen
- Programmed Cell Death 1 Receptor
- Cytokines
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on the topic
Treatment with glucocorticoids is not always effectively treating immune-related adverse events and may negatively affect the antitumor efficacy. Tocilizumab, an anti-interleukin-6 (IL-6) receptor monoclonal antibody, may interfere with the immune system to decrease immune-related toxicities. We hypothesized that tocilizumab would result in reduced immune checkpoint inhibitor (ICI)-induced colitis and arthritis.
What this study adds
The results of this study demonstrate that tocilizumab has promising efficacy for management of ICI-induced colitis and/or arthritis (84% clinical benefit rate) and manageable safety profile.
How this study might affect research, practice, or policy
Further studies are required to confirm these results and to eventually compare efficacy of tocilizumab with currently standard approaches in the treatment of ICI-induced toxicities.
Background
Immune checkpoint inhibitors (ICIs) targeting the cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and the programmed cell death protein 1 (PD-1) pathway have shown exceptional efficacy and durable responses in a wide range of solid tumors.1 2 However, ICIs may induce potentially severe and even lethal immune-related adverse events (irAEs) involving any organ.1 3 Conversely, several studies have reported a favorable relationship between irAEs and antitumoral response.4–7 Although irAEs are usually mild and manageable, ICI discontinuation and initiation of glucocorticoids for moderate to severe irAEs are indicated. Yet, if the severity of irAEs does not decrease during initial glucocorticoids, an immunosuppressive drug should be initiated.2 3 8–10
The impact of glucocorticoids and other immunosuppressive drugs on the antitumoral effects of ICIs remains controversial and needs to be explored further. The exact pathophysiology underlying irAEs has not been fully elucidated; however, it is considered to be linked to disturbances of the immune checkpoints that generally maintain immunologic homeostasis.1 In addition, an increase in T cell activation and proliferation, impaired regulatory T cell survival and increased counts of 17 T-helper (Th17) cells, proinflammatory cytokines, cross-reactivity, autoantibodies, and microbiome are speculated to be involved in irAEs, such as colitis and rheumatic disorders.2 Especially, Th17 cells that induce interleukin-17 (IL-17) production are involved in several immune diseases, including inflammatory bowel diseases, rheumatoid arthritis, and ICI-induced colitis.2 11 Interleukin-6 (IL-6) is a proinflammatory cytokine and a major player in inflammation and cancer progression.12–14 IL-6 stimulates the differentiation of naïve CD4+ cells into Th17 cells, and the inhibition hereof may alter the Th17–regulatory T cell balance without inhibiting the Th1 CD4+ T cell subtypes that support cancer cell attacks.11 13 Tocilizumab, an IL-6 receptor monoclonal antibody, has been approved for the management of rheumatic diseases (including rheumatoid arthritis, giant cell arteritis, systemic sclerosis), chimeric antigen receptor T cell therapy (CAR T) related cytokine release syndrome (CRS), and COVID-19.15–18 In addition, a threefold increase of IL-17 and IL-6 parallel with the incidence of fulminant colitis has been reported in a patient with presumed ipilimumab-induced colitis.19 Importantly, tocilizumab has been effective in managing severe CRS without compromising the antitumoral efficacy.20 Clinical improvement in various irAEs has been observed after administration of tocilizumab in case series.21–24 These observations of blocking IL-6 and whereby reducing IL-17, made the authors hypothesize if patients with ICI-induced colitis and arthritis could benefit from treatment with tocilizumab without using glucocorticoids. The purpose of this clinical trial was to assess the efficacy and safety of tocilizumab for treating ICI-induced colitis/diarrhea and arthritis/arthralgia, some of the most frequently occurring irAEs in patients with cancer treated with ICIs.9 25 26
Methods
Study design
This investigator-initiated, single-arm, signal-seeking study enrolled patients from January 24, 2019 to February 19, 2020 at the Copenhagen University Hospital (Herlev and Gentofte, Denmark). Patients received tocilizumab (8 mg/kg, maximum dose: 800 mg) every 4 weeks for at least two cycles or until worsening or lack of improvement of ICI-induced colitis/diarrhea and arthritis, unacceptable toxicity, withdrawal of consent, clear clinical deterioration, or according to the investigator’s judgment. In case of lack of reduction or worsening symptoms, tocilizumab was discontinued, and glucocorticoids were initiated according to local guidelines. Continued treatment with ICIs was allowed if deemed safe according to the investigator’s judgment. Reintroduction of tocilizumab was offered to patients who had reduced colitis/diarrhea or arthritis but experienced worsening within 6 months after the last infusion. The initial stage with the efficacy assessment in seven patients, performed in June 2019, was followed by an expansion phase with an additional 13 patients (online supplemental figure S1). The study adhered to the Consolidated Standards of Reporting Trials reporting guideline (online supplemental table S1). Written informed consent was obtained from all patients.
Supplemental material

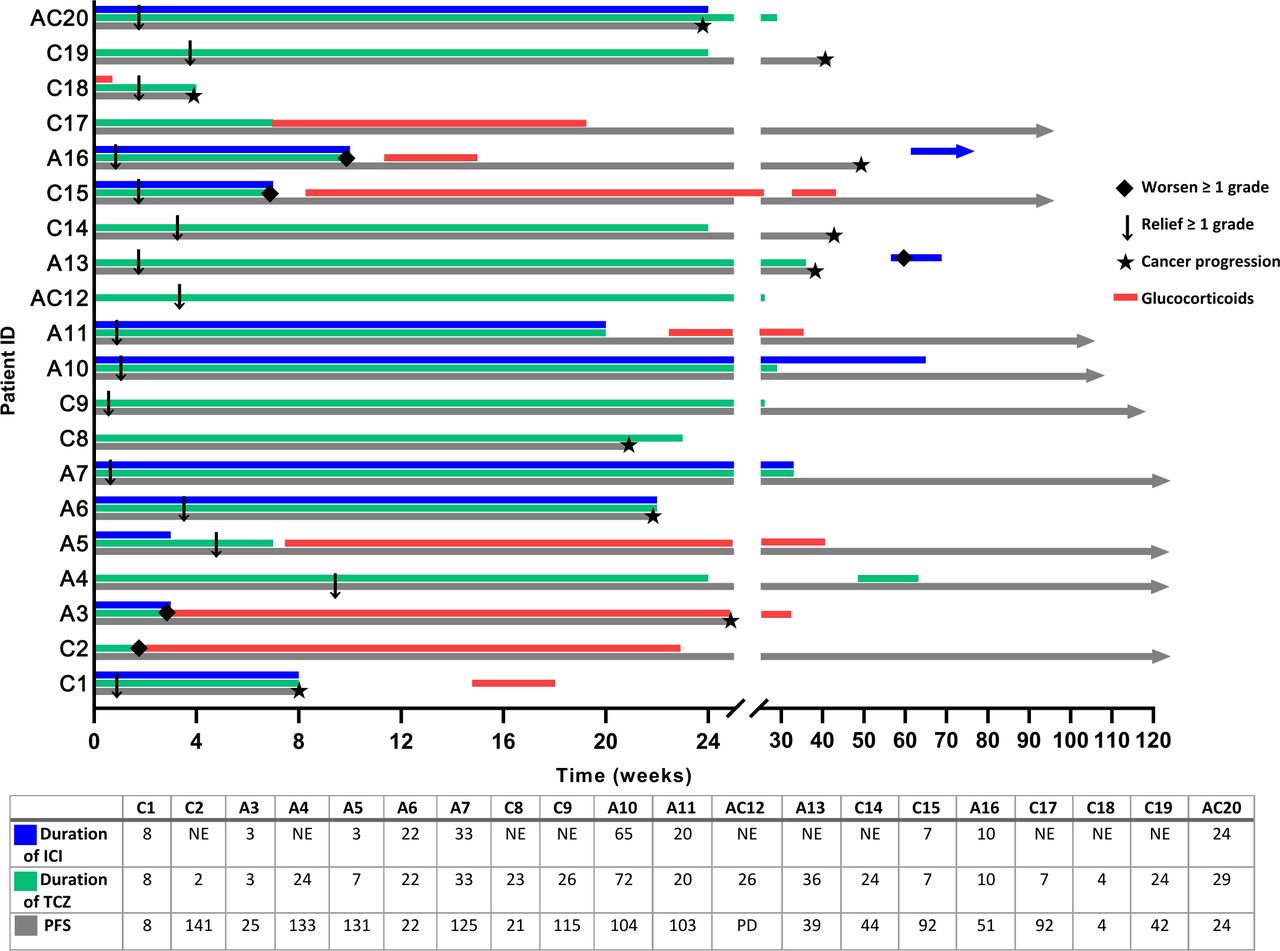
Treatment overview. All 20 patients are illustrated. Patient C8 was excluded from efficacy analysis due to pancreatic insufficiency-induced diarrhea. Treatment for ICIs and tocilizumab are shown from the time point of tocilizumab initiation. Nine of 20 patients received systematic therapy with systemic glucocorticoids. Six patients experienced cancer progression within the study period (24 weeks), including C18 with melanoma, who had new melanoma moles which were surgically resected and followed by a durable complete response. At the cut-off for disease status in October 2021, three additional patients experienced cancer progression; two were rechallenged with a PD-1 inhibitor. ICI, immune checkpoint inhibitor; NE, not evaluable; PD, progressive disease; PFS, progression-free survival; TCZ, tocilizumab.
Patient population
Patients aged ≥18 years with solid tumors were eligible if they had new-onset, glucocorticoid-refractory and/or glucocorticoid-dependent colitis/diarrhea or arthritis per Common Terminology Criteria for Adverse Events (CTCAE V.5.0) grade >1 induced by ICIs: Colitis was classified from grade 1, asymptomatic to grade 4, life-threatening, urgent intervention indicated; and diarrhea as grade 1, increase <4 stools/day over baseline to grade 4, life-threatening. Arthritis was graded as grade 1, mild pain with inflammation, erythema, or joint swelling to grade 3, severe pain associated with signs of inflammation, erythema, or joint swelling, irreversible joint damage, limiting self-care activities of daily living.27 The grading of ICI-induced colitis/diarrhea and arthritis was conducted at the time point for starting tocilizumab. To diminish any disturbances, exposure to systemic glucocorticoids and other immunosuppressive drugs was not allowed within a 14-day screening period.
Assessments
Oncologists evaluated all patients with assistance from gastroenterologists or rheumatologists for the assessment of colitis/diarrhea and arthritis. Gastrointestinal assessment was scheduled at tocilizumab initiation and repeated after 1 month, including the following: history, physical examination, fecal analysis (pathogenic viral and bacterial species including Clostridioides difficile and calprotectin), and computed tomography (CT) or combined positron emission tomography CT scans. All patients with colitis/diarrhea underwent colonoscopy with biopsies at treatment initiation, including: histopathology, physicians’ global assessment, and a colitis activity score (Mayo Score, online supplemental methods). Colonoscopies were repeated after 1–3 months. Rheumatological evaluation included history, physical examination, and measurement of circulating levels of autoantibodies (antinuclear antibodies, rheumatoid factor, and anticyclic citrullinated peptide antibodies). Imaging tests were performed if indicated. We examined the patients twice in week 1, followed by every 2–3 weeks according to the investigator’s judgment and irAE severity. Patients were followed up for at least 30 days (±5 days) for CTCAE assessment and then every 8–12 weeks for 6 months after the last tocilizumab dose. Plasma concentrations of C reactive protein (CRP) as part of routine analyses, cytokines (IL-6, IL-8, and IL-17), and YKL-40 were measured before initiation and every 2–3 weeks until the end of the treatment (online supplemental methods).
Outcomes
The primary endpoint was clinical benefit, defined as ≥1 grade reduction of ICI-induced colitis/diarrhea and/or arthritis using CTCAE V.5.0 within 8 weeks after tocilizumab initiation. The secondary endpoints were safety, ≥1 grade reduction without glucocorticoids within 8 weeks of treatment initiation, and sustained glucocorticoid-free remission at week 24. The exploratory endpoints were radiologic, endoscopic, and histological changes and changes in plasma concentrations of CRP, cytokines (IL-6, IL-8, and IL-17), and YKL-40 during tocilizumab.
Statistical analysis
A sample size of 20 was required according to Simon’s 2-stage optimal design to obtain a significance level of 5% and a power of 80% in the one-sided test of the null hypothesis (<50% clinical benefit rate) against the alternative hypothesis (≥80% clinical benefit rate). In the first stage, seven patients were treated, and in the case of ≤4 patients with reduction of symptoms, accrual would be terminated. Otherwise, the trial would include an additional 13 patients in the second stage. The null hypothesis would be rejected if ≥14 of 20 patients with clinical benefit were observed.
All patients with ICI-induced colitis/arthritis who met the inclusion criteria and received ≥1 cycle of tocilizumab were analyzed for treatment efficacy (evaluable populations). Time to symptom reduction was defined as the time from treatment initiation (tocilizumab) to the date of ≥1 CTCAE grade reduction of symptom. Complete remission of symptoms was defined as the time from tocilizumab initiation to CTCAE grade 0 of colitis/diarrhea and arthritis.
Descriptive statistics were used to summarize the characteristics of the cohort and to report adverse events (AEs). Continuous outcome measures were presented as medians and ranges. CIs were estimated by using binomial tests. Statistical analyses were performed by using Microsoft Excel v2002 and R Studio V.1.2.5001.
Results
Patient characteristics
Of 27 patients screened, 20 patients with arthritis (n=9), colitis/diarrhea (n=9), or both (n=2) induced by ICIs were enrolled. Seven patients were excluded: four declined to participate, two did not meet the inclusion criteria (non-ICI-related arthralgia), and one patient failed the glucocorticoid tapering. One patient with diarrhea was subsequently excluded from the efficacy analysis due to diarrhea caused by pancreatic insufficiency with no relation to ICIs (online supplemental figure S2). None had a history of autoimmune diseases. Before initiating tocilizumab treatment, the median duration of colitis/diarrhea and arthritis symptoms was 26 days (3–787) and 71 days (3–922). Seven patients had initially received systemic glucocorticoids for colitis and/or arthritis, and two of them also received treatment with infliximab for colitis (tables 1 and 2). All patients stopped receiving glucocorticoid therapy or other immunosuppressive drugs within the 14-day screening period; however, those with hypophysitis continued regular hydrocortisone substitution.

{kind=link}
{kind=link}
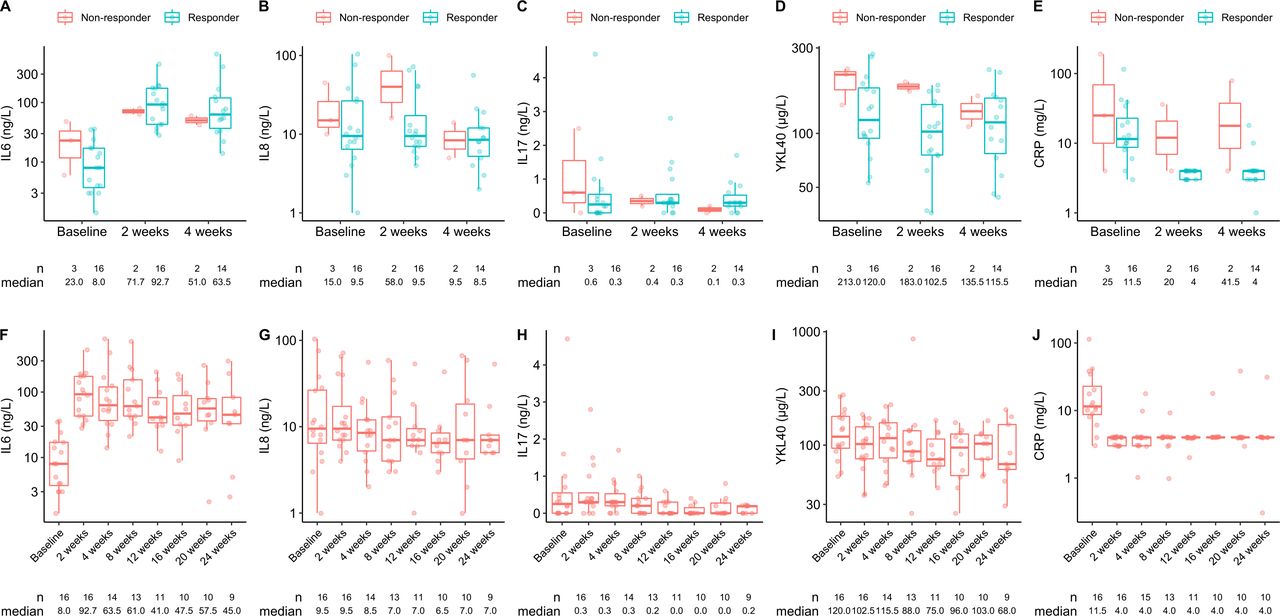
Plasma concentrations of IL-6, IL-8, IL-17, YKL-40, and C reactive protein (CRP). (A–E) Plasma concentrations of IL-6, IL-8, IL-17, YKL-40, and CRP during the first 4 weeks of tocilizumab among responders and non-responders. (F–J) Plasma concentrations of IL-6, IL-8, IL-17, YKL-40, and CRP in responding patients. IL, interleukin; YKL-40, chitinase-3-like-protein 1.
Characteristics of patients with colitis treated with tocilizumab
Characteristics of patients with arthritis treated with tocilizumab
Eight of 10 patients with confirmed ICI-induced colitis/diarrhea had CT-verified bowel wall thickening; five (50%) had endoscopic changes with edema of either the entire colon or left colonic segments. The median Mayo Score was 4 (1–10). All 10 patients had biopsy-proven colitis in the absence of enteritis. Fecal calprotectin levels available in five patients ranged from 109 to >1800 µg/mg. Five of the 11 patients with arthritis were positive for antinuclear antibodies, and two for a low-level rheumatoid factor.
Efficacy outcomes
At week 8, 15 of 19 patients (79%, 95% CI 54% to 94%) had ≥1 grade reduction of symptoms without using glucocorticoids. The median time from tocilizumab initiation to reduction was 14 days for both colitis (3–28) and arthritis (5–72). One of the two patients with stable symptoms who continued treatment responded at week 10. Two patients experienced worsening symptoms after a single infusion and started glucocorticoids after 12 and 24 days, respectively. All six patients with persistent colitis or arthritis (duration of ≥90 days) responded to tocilizumab treatment.
Within 24 weeks, 16 of 19 patients (84%, 95% CI 60% to 96%) achieved ≥1 grade reduction following treatment with tocilizumab. At week 24, 12 patients had ongoing reduction of symptoms, 10 of which achieved durable complete remission of symptoms; however, one patient received glucocorticoids due to other irAEs. In total, 9 of the 19 (47%) patients received systemic glucocorticoids (tables 1 and 2).
In patients with colitis, 8 of 10 (80%) patients showed a reduction in symptoms (table 1). Furthermore, patients with suspicion of cytomegalovirus (CMV) were tested negative. One patient with initial symptom reduction experienced relapse of colitis after restarting ICI therapy before evaluation and was treated with glucocorticoids. Another patient discontinued tocilizumab due to treatment-related allergic reaction but experienced reduction of colitis. Two patients did not respond to tocilizumab; one patient experienced worsening of diarrhea on day 12 (advanced from grade 1 to grade 2), and one with stable symptoms was later diagnosed with microscopic colitis; both patients were then treated with glucocorticoids. Six patients had endoscopic and histologic improvements without glucocorticoids (table 3, online supplemental figures S3,S4). Six patients showed radiological improvements. A follow-up colonoscopy was performed on three patients during a second evaluation (12–16 weeks after the last tocilizumab infusion, table 3). All three were still in remission of colitis.
Radiologic, endoscopic, and histological features in patients with ICI-induced colitis
Five patients with arthritis required local treatment at tocilizumab initiation. Within 8 weeks, none required arthrocentesis and intra-articular glucocorticoids; however, one patient treated with concomitant ICIs and tocilizumab did not achieve any clinical benefit from tocilizumab and shifted to systemic glucocorticoids on day 24. In total, 10 of 11 patients had reduced symptoms of arthritis (table 2).
Treatment exposure
All patients received ≥1 dose of tocilizumab. The median number of infusions and treatment duration were 5 (1–10) and 24 weeks (2–36), respectively. Three patients discontinued tocilizumab after one infusion (worsening symptoms (n=2) or an infusion-related reaction (n=1)). One patient was readministered with tocilizumab owning arthritis relapse. Within 24 weeks, 10 patients received concomitant ICI and tocilizumab therapy with a median duration of 10 weeks (3–65) (figure 1).
Safety
Sixteen of 20 (80%) patients had AEs of any grade related to tocilizumab, none of which were fatal. Five patients (25%) experienced grades 3–4 treatment-related AEs (TRAEs): Neutropenia (n=2, one of them developed new-onset hypophysitis and severe infection/septic shock); thrombocytopenia (n=1); colitis with ulcerations (n=1), and allergic reaction (n=1) requiring glucocorticoids and observation at the hospital (table 4).
Safety table
Inflammatory markers
An increase in IL-6 level was observed in all patients regardless of response as expected. Plasma levels of IL-8, IL-17, CRP, and YKL-40 decreased mainly in patients who responded to treatment. One patient with glucocorticoid-refractory colitis had a notable decrease in IL-17 levels, correlating with clinical response (figure 2, online supplemental figures S5,S6).
Cancer status
From tocilizumab initiation and during the study period of 24 weeks, six of 20 (30%) patients experienced cancer progression (data are shown in figure 1, for further description, see online supplemental results and online supplemental figures S7A–B and S8A–B).
Discussion
To the best of our knowledge, this is the first study to demonstrate that tocilizumab, an IL-6-receptor inhibitor, can be safely used to treat ICI-induced colitis/diarrhea and arthritis. The majority (15/19, 79%) of evaluable patients had a reduction of CTCAE grade by ≥1 within 8 weeks and additional one had ≥1 grade reduction at 10 weeks. Thus, the threshold for primary efficacy was met. At week 24, symptom reduction was experienced by 16 (84%) patients and durable responses by 12 patients, including complete remission of symptoms in 10 patients. During this treatment, half of the patients were able to continue ICIs.
Importantly, we observed acceptable toxicity during ICIs and tocilizumab combination therapy; however, colon ulceration and an increased risk of infection should be considered, especially in patients with cancer. In this study, only patients previously treated with chemotherapy developed neutropenia and thrombopenia, both well-known TRAEs. Nevertheless, we cannot exclude these two severe above-mentioned events could be influenced by ICI exposure or combination with tocilizumab. One patient achieving clinical benefit permanently discontinued tocilizumab due to an infusion-related reaction after the first infusion. Hypersensitivity reactions related to tocilizumab have been reported in <1% of patients.28 It is unknown if ICI-treated patients are more prone to develop hypersensitive drug reactions compared with ICI-naïve patients; however, ICIs might activate drug-responsive T-cells, which are effectors of hypersensitivity.29
The use of tocilizumab to manage irAEs has been previously investigated in retrospective studies and case series with promising results. Stroud et al reported clinical improvements in 27 of 34 patients treated with tocilizumab and glucocorticoids for severe pneumonitis, serum sickness, and cerebritis.21 The benefit of tocilizumab for ICI-induced arthritis, polymyalgia rheumatica, myositis, myocarditis, CRS, and hemophagocytic syndrome has been reported.22 24 30 Recently, tocilizumab was successful in treating multiple irAEs and preventing flare of pre-existing autoinflammatory diseases in 21 of 22 patients with melanoma.23 In our study, two patients experienced worsening of colitis and arthritis after one tocilizumab infusion (on day 12 and day 24, respectively). We cannot exclude the possibility that a more prolonged treatment exposure to tocilizumab is required due to increased tocilizumab clearance. In patients with inflammatory signatures of CAR T-cell induced CRS, tocilizumab infusion is usually repeated if symptoms do not improve within 48 hours.20 31 One patient with stabile symptoms was diagnosed with microscopic colitis, a histopathological subgroup of ICI-induced colitis, and did not respond to tocilizumab treatment. The patient was then effectively treated with budesonide, as reported by Hughes et al.32
Although the antitumoral efficacy of ICIs has been extensively studied, crucial concerns regarding resumption of ICIs following moderate to severe irAEs, concomitant immunosuppressive therapies (especially in patients with pre-existing autoimmune diseases), and management of glucocorticoid-refractory irAEs are arising. However, no controlled trials have thus far defined the strategies for the effective management of specific irAE, and international guidelines are primarily based on retrospective cohorts, case series, and case reports; especially guidelines for treating glucocorticoid-dependent or -refractory cases are mainly based on expert opinions.8 9 33 In our study, increasing levels of IL-6 were observed in all patients due to blockade of the IL-6 receptors while levels of IL-8, IL-17, CRP, and YKL-40 decreased in responding patients. We noticed a patient with glucocorticoid-refractory colitis, treated with infliximab twice with minimal efficacy, achieved complete remission of symptoms after tocilizumab treatment. This response was paralleled by a decrease of a high circulating level of IL-17 before treatment, suggesting that cytokine levels are potential biomarkers in patients with irAEs refractory to standard treatment options. Early intervention with an immunosuppressive agent is reported to lead to more favorable outcomes.34 Furthermore, adding a glucocorticoid-sparing therapy, especially in long-term irAEs, may dampen the risk of glucocorticoid-induced AEs. Currently, infliximab and vedolizumab are the preferred second-line and third-line treatment options for ICI-induced colitis.35 36 However, ustekinumab (anti-IL-23/12), tofacitinib (a JAK inhibitor), and fecal microbiota transplantation may be effective for the treatment of refractory colitis.37–39 Loperamide ‘as needed’ was allowed in this study; however, it is debated if loperamide should be withdrawn in severe colitis to prevent a potential risk of toxic colon dilatation.40 41 In addition, CMV infection should be excluded in glucocorticoid-refractory cases, as we did in this study.42
Glucocorticoids are the first choice of therapy for rheumatologic AEs triggered by ICIs and usually long-term administration is required. No specific biological disease-modifying antirheumatic drugs have shown superiority, and treatment with TNF-inhibitors may require repeated administration with unknown influence on the antitumor response.43 However, concomitant treatment with ICIs and TNF-inhibitors is being studied (NCT03293784).44 The antitumor effect of tocilizumab was not an endpoint in this study. However, we observed cancer disease control in majority of included patients at 24 weeks. Thus, despite the small population size, tocilizumab did not seem to affect negatively the anticancer responses induced by ICIs; similar to previous reports.23 45 Clinical trials of tocilizumab (NCT04940299, NCT04258150, NCT04375228, and NCT04691817) on anticancer responses and irAEs are ongoing.
The limitations of this study were the lack of a control group and the small population size. Thus, we cannot exclude that the observed reduction of symptoms was related to the natural course of irAEs, delayed biological effect of ICI treatment, or intra-articular glucocorticoids and other supportive agents being used. However, few data on these subjects are available making this study important as a first starter. We may also have selected patients with favorable outcomes because patients had to go through a 14-day long screening period if shifted from glucocorticoids. Also, low statistical power may increase the risk of spurious findings. We included a broad spectrum of ICI regimens and cancer types, which may have skewed outcomes. The variable duration of symptoms up to inclusion suggested a heterogeneous cohort, limiting the generalizability of results. Moreover, irAEs may be caused by several relatively unknown mechanisms, and some may like to respond better to treatment than others. The strengths of this study were its prospective study design and extensive multidisciplinary workup. In addition, we supplied measurements of circulating cytokines and YKL-40. Larger comprehensive cohorts, including controls testing tocilizumab or alternative strategies for irAEs are needed. Still, a central concern is the sparsity of data related to safety and efficacy of treating irAEs with glucocorticoids and immunosuppressive drugs, including their effects on anticancer responses. However, whether immunosuppression related to tocilizumab is more acceptable than glucocorticoids is unknown. The CTCAE grading of irAEs should also be more specific and include imaging, endoscopy, and histopathology results. In addition, many patients treated with ICIs experience multiorgan toxicity.9 Therefore, a guide to multidisciplinary team building and management would be an oncological imperative of essential value. Future studies incorporating blood-based biomarkers in irAEs, as well as selecting other steroid-sparing agents are warranted. Finally, moving anti-IL-6 agents to first-line therapy for the management of the new-onset irAEs should be studied from a cost-effective perspective as it would have significant implications.
Conclusions
Tocilizumab showed promising clinical efficacy and a manageable safety profile in 16 of 19 (84%, 95% CI 60 to 97%) patients experiencing ICI-induced colitis and/or arthritis. Half of the patients successfully continued ICIs concomitant with tocilizumab. Future prospective studies of organ-specific irAEs managed with glucocorticoids as a standard approach and experimental therapies, including randomization, are warranted to refine treatment guidelines.
Supplemental material
Supplemental material
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Danish Ethics Committee (approval number H-20022758), the Danish Medicines Agency (EudraCT no. 2018-002595-41). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank all patients, their caregivers, and all the health partners at Herlev and Gentofte Hospital. The authors would like to thank the Department of Oncology, Herlev and Gentofte Hospital for their tremendous support and for providing drugs. Many thanks to the biomedical laboratory scientists Charlotte Falk, Sarah Damsbo Jensen, and Vibeke H. Holm for handling blood and stool sampling. The nurse Heidi Lind Kristensen is acknowledged for data registration. We thank statistician Kasper Madsen, for his support with statistical analyses and Christina Sylvester-Hvid for for support. We thank Editage for English language editing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conception/design: IMC, DLN, JJ. Provision of study materials or patients: RBH, OHN, SJ, LBR, JWB, PV, JJ, MKB, RHLE, IMC. Collection and/or assembly of data: all authors. Data analysis and interpretation: all authors. Manuscript writing: RBH, IMC. Final approval of manuscript: all authors. IMC is responsible for the overall content as the guarantor.
Funding This trial was supported by the Department of Oncology, Copenhagen University Hospital - Herlev and Gentofte, and the Danish Health Agency 'Empowering cancer immunotherapy in Denmark,' Grant No. DHA 4-1612-236/8. Bristol Myers Squibb (BMS) has provided financial support for translational analyses, BMS study ID CA209-8M8.
Competing interests All authors completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. RBH received speaking honoraria from BPNO. P. Vilmann reported a consulting relationship with MediGlobe GmbH, Grassau. JJ reported receiving research funding and hotel/airfare reimbursement to attend global health meetings from Roche, BMS, and Celgene. MKB reported receiving hotel/airfare reimbursement to attend global health meetings from Pfizer. RHLE received research funding from BMS and advisory relationship with Amgen. IMS has been principal investigator in BMS-supported trials and received honoraria from BMS for speaking and serving on an advisory board. IMC reported receiving research funding and hotel/airfare reimbursement to attend global health meetings from Roche, BMS, Celgene, Genis, and advisory relationship with Amgen. OHN, LBR, ST, SJ, and DLN had no disclosures.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.