Article Text

Abstract
Background PD-1 immune checkpoint blockade (ICB) improves survival versus chemotherapy in PD-L1 CPS≥1 recurrent or metastatic head and neck cancer. We evaluated the safety and efficacy of induction and concurrent CTLA4 and PD-1 ICB and IMRT in newly diagnosed HPV-OPSCC.
Methods PD-L1 CPS≥1, p16-positive + HPV RNA-Scope-positive, AJCC 8th edition T1-3N1-2 M0 or T3N0M0 OPSCC patients irrespective of smoking status received two, six-week cycles of ipilimumab (1 mg/kg) day 1 and nivolumab (3 mg/kg) on days 1, 15, and 29, and IMRT concurrent with cycle 2. IMRT was delivered in 4 weeks to pre-induction tumor volume (40-44 Gy) and one adjacent uninvolved nodal level (36 Gy). Post-induction volume was boosted to 50-66 Gy in 2 weeks. Response was evaluated by RECIST 1.1. Principal outcomes were FDG-PET complete response (PET-CR) at 6 months per Hopkins Criteria1 and progression-free survival (PFS) at 2-years. Correlatives included histological (% tumor viability)2 and molecular (plasma cfHPV clearance) responses after induction ICB.
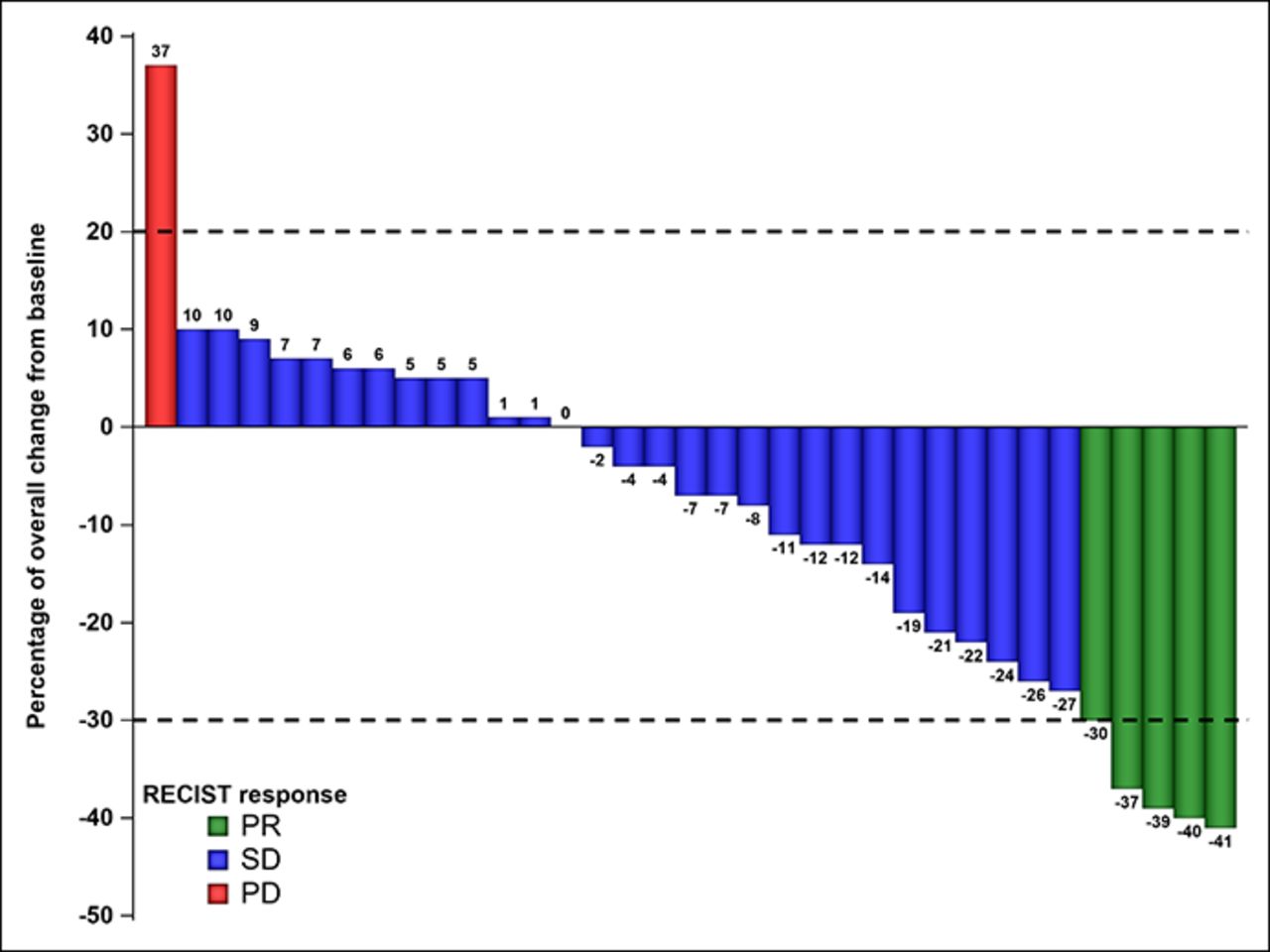
Results Treated patients (35) were male (97%), median age 64 (49-78) years with stage T1(14), T2(16), T3(5) and N0(1), N1(33), N2(1) base of tongue (18) or tonsil (17) SCC. 66% had acute grade≥3 AEs (table 1). Five discontinued ICB due to toxicity (n=3), progression (n=1), or physician decision (n=1) and received concurrent platinum (n=3) or IMRT alone (n=2). PET-CR was 90% (29 of 32 evaluable). One of 3 patients without PET-CR progressed. After median follow-up of 14.9 months, 3 patients had local progression and were treated with surgery or SBRT. All patients are alive without cancer at last follow-up. Response to induction ICB was 14% (figure 1). Among 27 evaluable patients, histological response was 0% viability in 37% and <10% viability in 48% (figure 2). 96% had pathological treatment effect ≥20% [2]. At baseline, 97% were positive and 74% quantifiable (≥16 copies/ml) by cfHPV. cfHPV clearance was 30% after induction ICB and 100% 4 weeks after IMRT. Compared to standard planning, RT volume to ≥66 Gy and ≥50 Gy was reduced by 21% (+/- 3%) and 36% (+/- 4%), and dose to ipsilateral parotid, spinal cord, larynx and esophagus was reduced by up to 50%.
Conclusions Patients with HPV-OPSCC treated with induction and concurrent CTLA4 and PD-1 ICB with dose-volume-adapted IMRT experienced a 6-month PET-CR of 90%, a 2-year PFS of 86%, and acute grade≥3 toxicity rate of 66%. Efficacy of induction ICB was supported by <10% tumor viability in 48% and cfHPV clearance in 30%.
Acknowledgements Funded by Cancer Prevention and Research Institute of Texas and Bristol-Myers-Squibb.
Trial Registration NCT03799445
References
Marcus C, et al. Head and neck PET/CT: therapy response interpretation criteria (Hopkins Criteria)-interreader reliability, accuracy, and survival outcomes. J Nucl Med 2014;55, 1411–6.
Wise-Draper, et al. Phase II Clinical Trial of neoadjuvant and Adjuvant Pembrolizumab in Resectable Local-Regionally Advanced Head and Neck Squamous Cell Carcinoma. Clin Cancer Res 2022;28, 1345–1352.
Ethics Approval The study was approved by The University of Texas MD Anderson Cancer Center Institutional Review Board, approval numbers 2018-0381 and PA19-0470. All participants gave their informed consent prior to enrollment.
Grade=3 treatment related adverse events per CTCAE V4 that occurred after dose of ICB
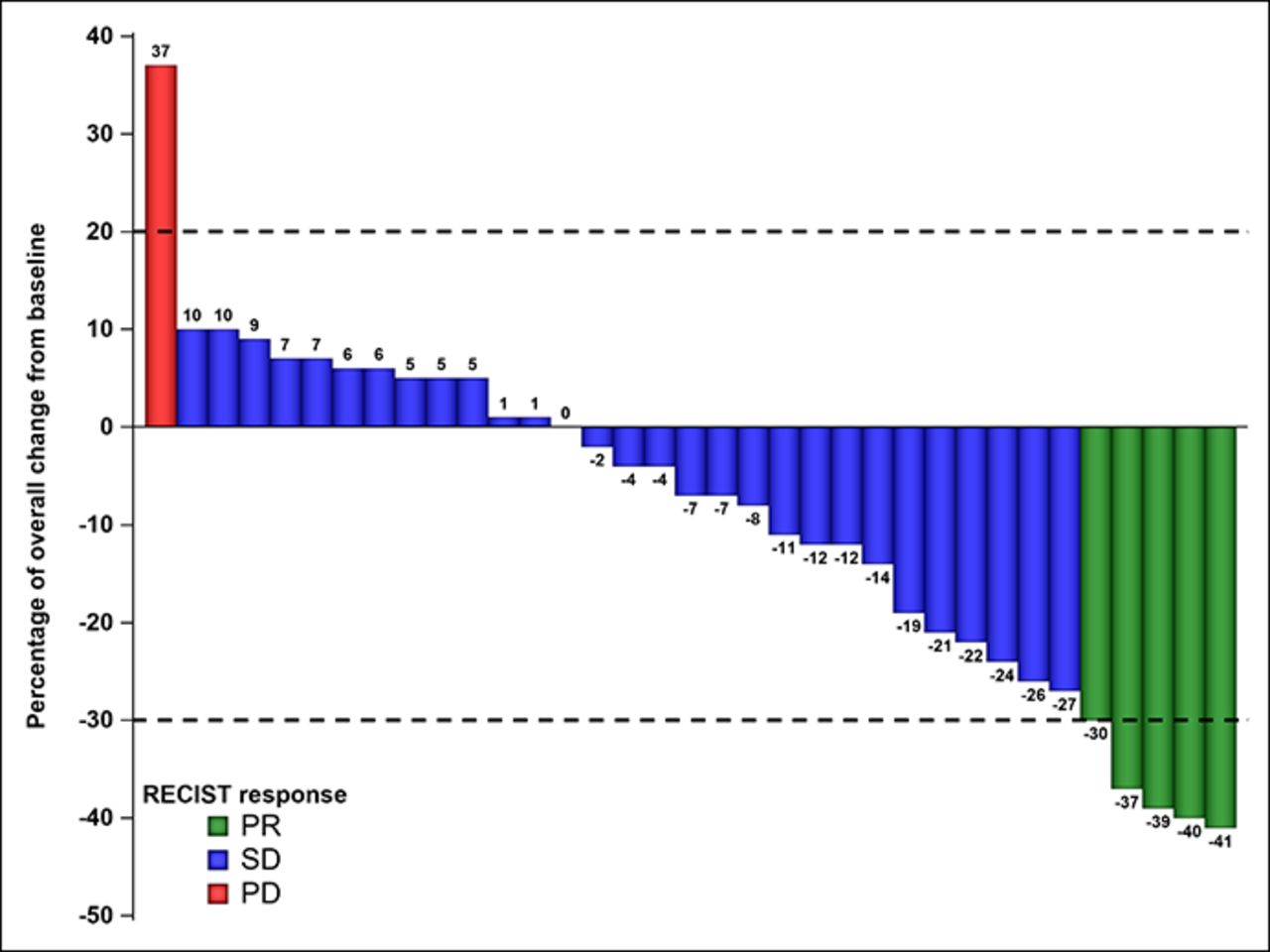
Waterfall plot of percent reduction in tumor volume by RECIST 1.1 after induction ICB

{kind=link}
{kind=link}
Waterfall plot of percent reduction in tumor viability from baseline. Percent change in tumor viability (%, y-axis) in core needle biopsy at baseline versus 3-5 weeks on induction ICB. Due to tumor viability of 90-100% at baseline, patients with =95% and =90% change in viability achieved complete (i.e., 0% viability) and major* (i.e., <10% viability) histological response, respectively. RECIST response, partial (green), stable (blue), progression (red)