Article Text

Abstract
Background For patients with advanced non-small cell lung carcinoma (NSCLC), immune checkpoint inhibitor (ICPI) and chemotherapy (chemo) ICPI represent two distinct first-line standard-of-care regimens without clear and established biomarkers to inform the optimal choice for individual patients. Here, we examined the complementary roles of tumor mutational burden (TMB) and programmed death ligand-1 (PD-L1) immunohistochemistry (IHC) to inform first-line therapy using a large real-world (rw) data set.
Materials and methods The study included patients with NSCLC from an rw de-identified clinico-genomic database. All patients underwent genomic testing using Foundation Medicine’s tissue comprehensive genomic profiling assay and PD-L1 IHC assay scored for tumor cell staining (TS).
Results Of 2165 patients included in the analysis, 150 exhibited durable benefit from first-line ICPI regimens (these patients were enriched for PD-L1 TS ≥50, non-squamous histology, and TMB ≥20 mutations/megabase (muts/Mb)). Comparing low TMB (<10 muts/Mb), high TMB (10–19 muts/Mb), and very high TMB (≥20 muts/Mb) receiving ICPI alone, we observed a stepwise increase in median rwPFS (real world-progression free survival) (6.5, 7.5, 17.2 months) and rwOS (real world-overall survival) (10.1, 11.8, 26.9 months) as TMB increased. In the low PD-L1 (TS <50%) cohort, TMB <20 muts/Mb showed a more favorable rwPFS (HR: 0.56 (95% CI: 0.40 to 0.79)) and rwOS (HR 0.74 (95% CI: 0.58 to 0.96)) on chemoICPI when compared with ICPI alone while the point estimate in rwPFS favored monoICPI in the TMB ≥20 muts/Mb cohort, the CI is wide and does not reach statistical significance (HR: 1.68 (95% CI: 0.52 to 5.48)).
Conclusion This study provides evidence that higher TMB cut-offs, such as 20 muts/Mb, can identify patients with prolonged benefit from ICPI. TMB ≥20 muts/Mb is a potential biomarker that may identify patients in whom an ICPI without chemo could be considered, even in the setting of lower PD-L1 levels. Prospective validation of these findings could increase access to chemo-sparing regimens for the first-line treatment of advanced NSCLC.
- Immunotherapy
- Tumor Biomarkers
- Lung Neoplasms
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study have been originated by Flatiron Health and Foundation Medicine. These de-identified data may be made available upon request and are subject to a license agreement with Flatiron Health and Foundation Medicine; interested researchers should contact <cgdb-fmi@flatiron.com> and <dataaccess@flatiron.com> to determine licensing terms.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
A need for biomarkers that can help predict outcomes in patients with non-small cell lung cancer (NSCLC) treated with an immune checkpoint inhibitor (ICPI) alone versus in combination with chemotherapy (chemoICPI) in the first-line (1L) setting currently exists. In June 2022, Ricciuti et al published their work describing higher real world-progression free survival (rwPFS) and real world-overall survival in a very high tumor mutational burden (TMB) cohort when compared with patients in the TMB low cohort. This current study examines whether TMB has a role in predicting outcomes on ICPI alone versus chemoICPI in 1L patients with NSCLC when using a very high TMB cut-off of 20 mutations/megabase (muts/Mb).
WHAT THIS STUDY ADDS
In this study, we examined 2165 patients with NSCLC from a real-world clinico-genomic database and discovered that in the low programmed death ligand-1 (PD-L1) cohort, the patients with TMB <20 muts/Mb showed a more favorable rwPFS on chemoICPI when compared with ICPI alone while rwPFS was not observed to increase when adding chemotherapy onto ICPI in the TMB ≥20 muts/Mb group.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study suggests that TMB ≥20 muts/Mb is potentially a biomarker that may identify patients in whom an ICPI without chemotherapy could be considered, even in the setting of lower PD-L1 levels, and should be further studied in future clinical studies.
Introduction
Immune checkpoint inhibitors (ICPI) have revolutionized cancer therapeutics through enhancing survival and increased quality of life for patients with cancer.1 Programmed cell death protein-1/programmed death ligand-1 (PD-1/PD-L1) inhibitors are a type of ICPI that have been particularly efficacious in multiple solid tumor types including non-small cell lung cancer (NSCLC).2 In first-line (1L) NSCLC, the US Food and Drug Administration (FDA) has approved single agent pembrolizumab in patients whose tumors are positive for PD-L1 expression based on the KEYNOTE-042 trial.3 In addition, based on the KEYNOTE-189 and KEYNOTE-407 trials, pembrolizumab plus chemotherapy was approved as a 1L treatment in NSCLC without an accompanying companion diagnostic (CDx).4 Despite being approved as a CDx for pembrolizumab in 1L NSCLC, PD-L1 expression remains an imperfect biomarker to consistently predict benefit from ICPI,5 6 resulting in conflicting 1L standard-of-care regimens.
In 2020, another ICPI biomarker, tumor mutational burden (TMB), was approved by the FDA as a pan-solid tumor CDx for patients with unresectable or metastatic tumor that have progressed following prior treatment using a TMB cut-off of ≥10 mutations/megabase (muts/Mb).7 Unlike PD-L1 immunohistochemistry (IHC) which identifies tumors that express PD-L1, high TMB identifies tumors with a high neoantigen load, which in turn are more likely to appear foreign to the immune system, a prerequisite for ICPI benefit. The pan-solid tumor approval was based on the KEYNOTE-158 trial that showed an overall response rate of 29% and high duration of response (57% of patients with ≥12 months response) in nine different tumor types.8 Despite the approval of TMB in the 2L+ (≥second line) setting, the clinical value of TMB in the 1L NSCLC setting is less clear.
Because of the exposure to carcinogens in tobacco, NSCLC has one of the highest median TMB values among solid tumors,9 10 an observation that encouraged the development of TMB as a predictive biomarker for ICPI.11 12 Early studies linked high TMB with clinical efficacy in pembrolizumab13 and nivolumab14-treated NSCLC and paved the way for subsequent trials such as CheckMate-568 that established TMB of 10 muts/Mb as a cut-off for prospective NSCLC trials.15 However, inconsistent performance of TMB as a predictive biomarker for overall survival (OS) in subsequent trials has cast doubt about its reliability and hampered its wide adoption.16 17 CheckMate-227 compared nivolumab plus ipilimumab versus chemotherapy using TMB as a co-primary endpoint biomarker with a cut-off of ≥10 muts/Mb. The study showed improved response rate and progression-free survival favoring high TMB but no significant difference in OS between high and low TMB cohorts. Analysis of OS in CheckMate-227 was complicated by the favorable prognostic effect of high TMB on OS in chemotherapy treated patients, possibly due to switching to ICPI after progression on chemotherapy.18 Interestingly, such a favorable prognostic effect of TMB in the chemotherapy-treated groups (OS of 16.7 vs 12.4 months in high vs low TMB) has not been seen with other ICPIs.
Subsequent trials suggested that the predictive value of TMB in ICPI-treated NSCLC was highly influenced by whether ICPI was used as monotherapy or in combination with platinum-doublet chemotherapy. In a retrospective analysis of whole exome sequencing (WES)-based TMB in second-line KEYNOTE-010 and frontline KEYNOTE-042, higher TMB evaluated as a continuous variable was associated with improved clinical outcome in PD-L1 positive patients with NSCLC treated with pembrolizumab monotherapy compared with chemotherapy.19 In contrast, addition of platinum doublet to pembrolizumab in KN-21,KN-189 and KN-407 nullified the predictive value of high TMB in predicting response to ICPI.20–22 Finally, several large meta-analyses documented improved OS in patients with TMB-high NSCLC treated with ICPI.23–25 In sum, the clinical evidence positively supports TMB as a clinically valid biomarker, although without clearly defined utility in NSCLC. In addition, although many of the studies used TMB cut-off of ≥10 muts/Mb, higher cut-offs have been explored and emerging evidence of favorable outcome and durable benefit in patients with TMB ≥20 muts/Mb are being explored.25 26 Herein, we examined the clinical value of using both TMB and PD-L1 IHC for selecting 1L treatment in patients with NSCLC using a large real-world data set.
Materials and methods
Patient selection
The study comprised patients with confirmed diagnosis of NSCLC included in the nationwide US-based Flatiron Health (FH)-Foundation Medicine (FMI) de-identified clinico-genomic database (CGDB) between January 2011 and December 2021. All patients underwent genomic testing using FMI’s comprehensive genomic profiling (CGP) assays and one of the widely commercially available PD-L1 IHC assay. De-identified clinical data originated from approximately 280 US cancer clinics (~800 sites of care). Retrospective longitudinal clinical data were derived from electronic health records (EHR), comprizing patient-level structured and unstructured data, curated via technology-enabled abstraction of clinical notes and radiology/pathology reports, which were linked to genomic data derived from FMI testing by de-identified, deterministic matching.27 Clinical data included demographics, clinical and laboratory features, timing of treatment exposure, and survival.
Patient records were included in this study if they received a 1L single-agent anti-PD-1/PD-L1 therapy or anti-PD-1/PD-L1 plus chemotherapy and had TMB and PD-L1 assessed via a tissue specimen collected before the start of 1L therapy. Patients must have additionally tested negative for EGFR mutations, and ALK/ROS1/RET rearrangements via FoundationOne/FoundationOneCDx (F1/F1CDx). Patients who were diagnosed with advanced NSCLC greater than 90 days prior to their first structured activity within the FH network or who received their FMI report greater than 60 days after their last FH structured activity date were excluded to enable accurate enumeration of line numbers and to exclude patients who left the FH network prior to CGP.
Institutional Review Board approval of the study protocol was obtained prior to study conduct and included a waiver of informed consent.
CGP
CGP was performed on hybridization-captured, adaptor ligation-based libraries using DNA extracted from formalin fixed paraffin embedded tumor in a Clinical Laboratory Improvement Amendments-certified and College of American Pathologists-accredited laboratory (Foundation Medicine, Cambridge, Massachusetts, USA). The samples were sequenced for up to 406 cancer-related genes and select gene rearrangements.28 TMB was determined on up to 1.24 Mb of sequenced DNA.29 Our primary analyses dichotomized TMB at 10 muts/Mb, in accordance with the CDx definition for pembrolizumab.7 In light of emerging evidence of favorable outcome and durable benefit among patients defined by a higher cut-off, we also explored the higher cut-off of 20 muts/Mb to align with Ricciuti et al.26
DAKO PD-L1 IHC assays
All cases included in this study must also have been tested with a commercially available PD-L1 IHC assay (ie, DAKO 22C3, DAKO 28–8, VENTANA SP142, or VENTANA SP263) in addition to the CGP. The tumor cell staining (TS) score where # PD-L1 positive tumor cells / (total # of PD-L1 positive+PD-L1 negative tumor cells) was determined.
Outcomes
Real-world overall survival (rwOS) was calculated from start of ICPI treatment regimen to death from any cause, and patients with no record of mortality were right censored at the date of last clinic visit or structured activity. Because patients cannot enter the database until a CGP report is delivered, OS risk intervals were left truncated to the date of CGP report to account for immortal time.30 31 FH database mortality information is a composite derived from three sources: documents within the EHR, Social Security Death Index, and a commercial death data set mining data from obituaries and funeral homes. This mortality information has been externally validated in comparison to the National Death Index.32 Real-world progression free survival (rwPFS) was calculated from start of treatment to the first progression date >14 days after treatment start or to death. Real-world progression events were abstracted from patient charts using a clinician-anchored approach supported by radiology report data, as previously described.33 Patients were censored at their last clinic note date if no progression or death was observed. Median rwPFS and rwOS values were estimated in months with 95% CIs.
Statistical analysis and interpretations
Differences in time-to-event outcomes were assessed with the log-rank test and Cox proportional hazard (PH) models. Χ2 tests (or Fisher’s exact test) and Wilcoxon rank-sum tests were used to assess differences between groups of categorical and continuous variables, respectively.
Multivariable Cox PH models were fitted on rwPFS and rwOS to estimate the adjusted HR and its significance for certain analyses. Features included in the Cox model include TMB status, PD-L1 status, age at treatment start, Eastern Cooperative Oncology Group Performance Status Scale (ECOG) (0~1, 2+, and unknown), sites of metastasis, history of smoking, disease histology, stage at initial diagnosis, STK11 mutation status, and therapy class.
For analyses comparing outcomes between chemoICPI versus ICPI cohorts, covariate imbalance was first addressed using inverse probability of treatment weights targeting the average treatment effect. Features used in propensity models were: ECOG (0~1, 2+, and unknown), age at therapy start, PD-L1 status and/or TMB status, histology, stage at diagnosis (stage IV vs not), sites of metastasis, and history of smoking. Standardized mean difference was used to assess balance, and within 10% considered acceptable.34 R V.4.1.3 software was used for all statistical analyses.
Results
Patient cohort
A total of 17,020 unique patients with NSCLC were in the CGDB cohort and 12,146 patients had line of therapy information (figure 1). Of the 12,146 patients, 3127 received ICPI or chemoICPI in the 1L setting. After excluding patients without PD-L1 IHC results, with specimens collected after ICPI regimen therapy start, and with EGFR mutations or ALK/ROS1/RET rearrangements, a total of 2165 patients were included in the analysis. Of these, 846 patients received ICPI and 1319 received chemoICPI. When comparing characteristics between patients receiving ICPI versus the chemoICPI, we observed that the ICPI group was more often older, self-reported white race, woman, had higher ECOG performance scores, earlier stage at diagnosis, had tumors with squamous cell histology, higher TMB score, and PD-L1 TS ≥50% when compared with the chemoICPI group (online supplemental table 1). In addition, we examined the patient characteristics of the TMB <10, TMB 10–19, and TMB ≥20 subgroups (table 1). Here, we observed that the patient age at advanced diagnosis, and use of chemoICPI trended lower as the TMB values increased. Also, the distribution of PD-L1 IHC clone and ICPI regimens are shown in online supplemental table 2. As expected, we observed a stepwise increase in rwPFS and rwOS as the PD-L1 IHC score increased in this 1L NSCLC cohort (online supplemental figure 1,2).
Supplemental material
Patient characteristics of the TMB subgroups

Consolidated Standards of Reporting Trials diagram of study. A total of 17,020 unique patients with NSCLC were in the CGDB cohort and 12,146 patients had line of therapy information. Of the 12,146 patients, 3127 received ICPI or chemoICPI in the first line. After excluding the patient without a PD-L1 IHC result, with specimen collected after ICPI therapy start, and with EGFR mutations or ALK/ROS1/RET rearrangements, a total of 2165 patients were included in the analysis. Of these 846 patients received ICPI and 1319 received chemoICPI. chemoICPI, ICPI with chemotherapy; CGDB, clinico-genomic database; ICPI, immune checkpoint inhibitors; IHC, immunohistochemistry; NSCLC, non-small cell lung cancer; PD-L1, programmed death ligand-1; TMB, tumor mutational burden.
Characteristics of patients with durable benefit
We first explored characteristics of patients who achieved durable benefit on an ICPI regimen defined as being progression-free and without treatment change for 24 months. Of the 2165 patients, 945 patients where the progression time was uncertain were censored and 1 patient switched to a new line within 2 years and was excluded. Of the remaining patients, 150 had durable benefit (rwPFS >24 months) and 1040 were without durable benefit. Those with durable benefit had significantly higher TMB, PD-L1 expression, and were more likely to have tumors with non-squamous histology (table 2). Importantly, the prevalence of TMB ≥20 mut/Mb was 25.3% (38/150) in the durable responder group compared with 8.5% (88/1040) in the non-durable responder group while the prevalence of TMB 10–19 was similar (29.3% (44/150) vs 28.1 (292/1040), respectively).
Patient characteristics of durable responders (PFS >24 months) and non-durable responders (PFS <24 months)
High TMB and ICPI outcomes in 1L NSCLC
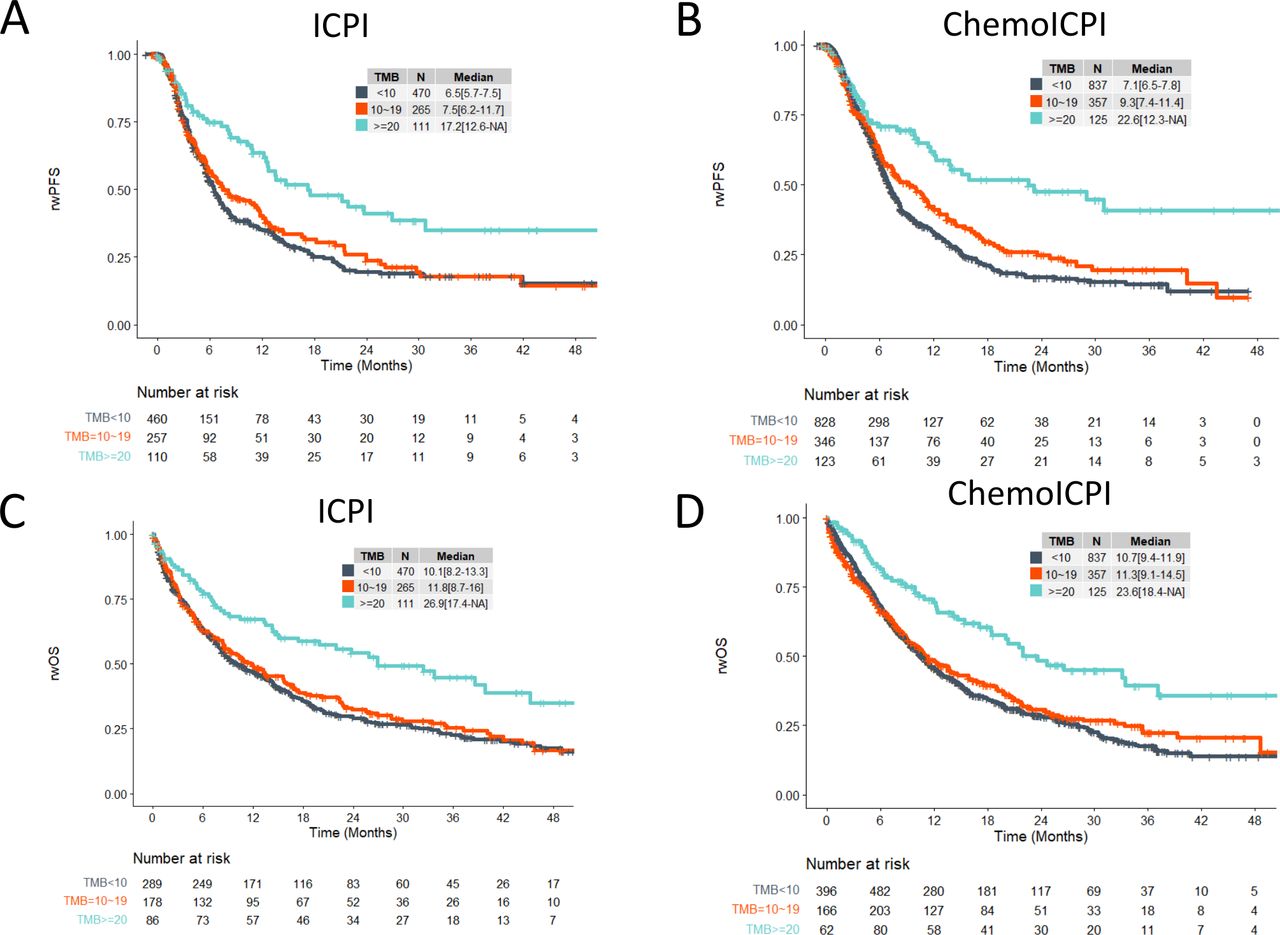
High TMB (≥10) was associated with an increased rwPFS (median: 11.3 vs 6.5 months; HR: 0.76 (95% CI: 0.63 to 0.93); p<0.01) and rwOS (median: 15.1 vs 10.1 months; HR: 0.8 (95% CI: 0.67 to 0.96); p<0.05) in the ICPI cohort and an increase in the rwPFS (median: 11.3 vs 7.1 months; HR: 0.73 (95% CI: 0.62 to 0.86); p<0.001) and rwOS (median: 13.7 vs 10.7 months; HR: 0.79 (95% CI: 0.68 to 0.92); p<0.01) of the chemoICPI group (online supplemental figure 3A-D). The association of TMB with ICPI outcomes was further amplified when we examined the TMB <10, TMB 10–19, and the TMB ≥20 groups. Here, we observed a significant increase of rwPFS (median: 17.2 vs 6.5 months, HR: 0.53 (95% CI: 0.38 to 0.72), p<0.001) and rwOS (median: 26.9 vs 10.1 months, HR: 0.54 (95% CI: 0.40 to 0.73), p<0.001) in the ICPI group and an increase of rwPFS (median: 22.6 vs 7.1 months, HR: 0.48 (95% CI: 0.36 to 0.65), p<0.001) and rwOS (median: 23.6 vs 10.7 months, HR: 0.52 (95% CI: 0.39 to 0.70), p<0.001) in the chemoICPI group when comparing the TMB ≥20 group to the TMB <10 group (figure 2A–D).

First-line patients with non-small cell lung cancer with TMB ≥20 mutations/Mb exhibited higher rwPFS and rwOS when compared with patients with TMB <20 mutations/Mb when treated with ICPI-regimens. Unweighted Kaplan-Meier plots of rwPFS (A and B) and rwOS (C and D) for patients who were treated with ICPI (A and C) or chemoICPI (B and D). Outcomes are stratified by TMB <10 (black), TMB 10–19 (orange), and TMB ≥20 (blue). chemoICPI, ICPI with chemotherapy; ICPI, immune checkpoint inhibitors; Mb, megabase; rwOS, real-world overall survival; rwPFS, real-world progression free survival; TMB, tumor mutational burden.
Clinical value of TMB+PD-L1 IHC in 1L NSCLC
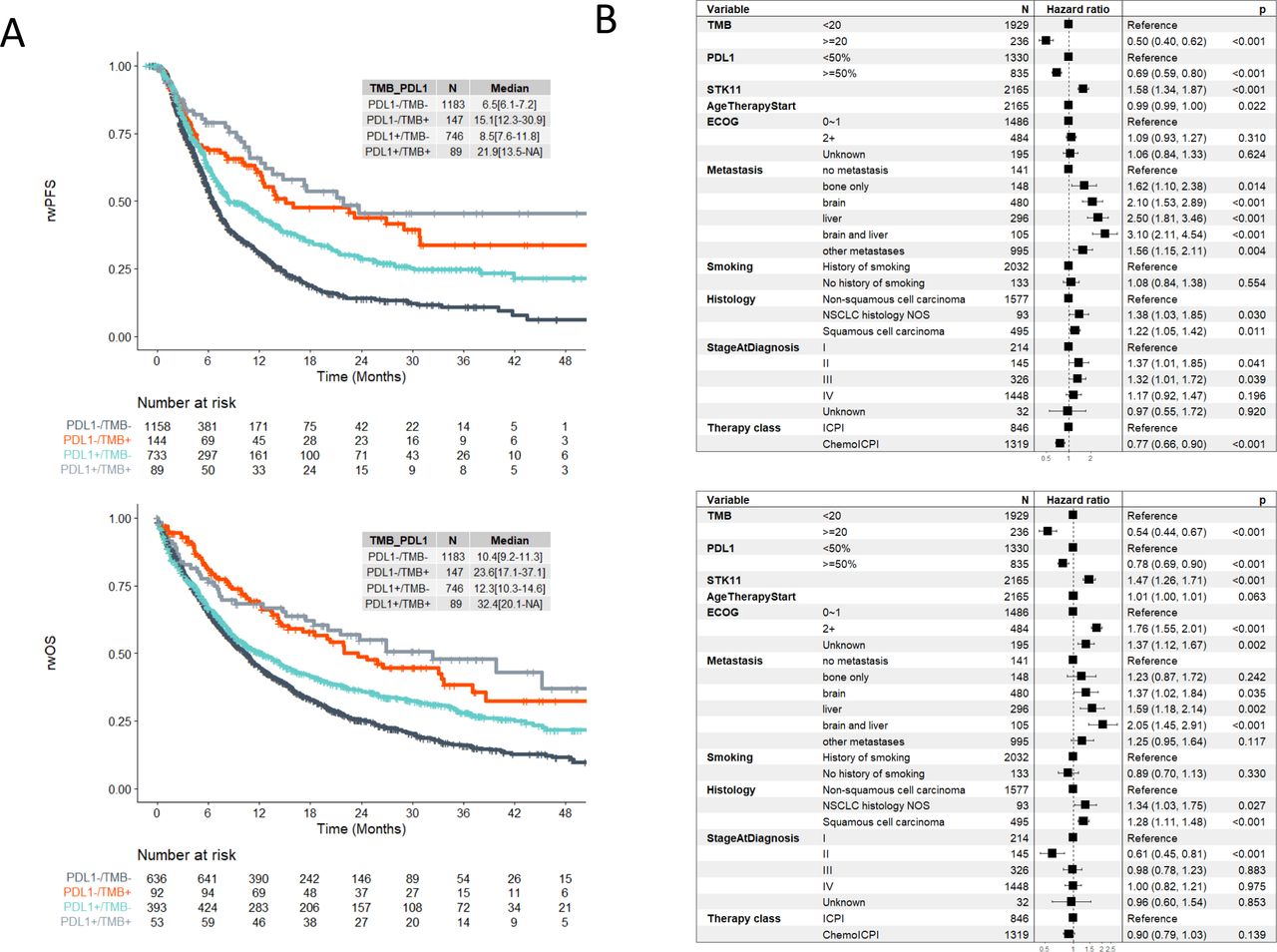
Using TMB ≥10 and PD-L1 TS ≥1% cut-offs, we observed that the rwPFS (median 11.7 vs 5.9 months) and rwOS (16.1 vs 10.3 months) was increased in the double biomarker positive cohort versus the double negative biomarker cohort when we examined 1L patients with NSCLC treated with ICPI containing regimens (online supplemental figure 4). Similar trends were observed when examining ICPI and chemoICPI cohorts separately (online supplemental figure 5). Importantly, using TMB ≥20 and PD-L1 TS ≥50% cut-offs, we saw a higher magnitude of difference in the rwPFS (median: 21.9 vs 6.5 months) and rwOS (median 32.4 months vs 10.4 months) between the double biomarker positive cohort versus the double negative biomarker cohort (figure 3). Similar trends were observed when examining the ICPI and chemoICPI groups separately (online supplemental figure 6).

Using a TMB ≥20 and PD-L1 TS ≥50 cut-off, we observed that PD-L1 immunohistochemistry and TMB are two independent and complementary biomarkers for predicting durable benefit to ICPI-regimens. (A) Kaplan-Meier plots of rwPFS (upper) and rwOS (lower) for patients who were treated with ICPI-containing regimens. Outcomes are stratified by TMB and PD-L1 levels: PD-L1 TS <50% and TMB <20 (black), PD-L1 TS ≥50% and TMB <20 (green), PD-L1 TS <50% and TMB ≥20 (orange), PD-L1 TS ≥50% and TMB ≥20 (gray). (B) Results from multivariate Cox proportional hazard model detecting associations between clinical or genomic features and rwPFS (upper) or rwOS (lower). chemoICPI, ICPI with chemotherapy; ECOG, Eastern Cooperative Oncology Group Performance Status Scale; ICPI, immune checkpoint inhibitors; NOS, not otherwise specified; NSCLC, non-small cell lung cancer; PD-L1, programmed death ligand-1; rwOS, real-world overall survival; rwPFS, real-world progression free survival; TMB, tumor mutational burden; TS, tumor staining.
Between-treatment subgroup analyses by PD-L1 or TMB
Lastly, we examined the between-treatment subgroup (1L ICPI and chemoICPI) analyses by PD-L1 or TMB. Here, we observed the trends for the estimates of the HRs when comparing rwPFS on chemoICPI versus ICPI as follows: PD-L1 TS <1% (HR: 0.43 (95% CI: 0.29 to 0.65)), PD-L1 TS=1–49% (HR: 0.65 (95% CI: 0.43 to 0.99)), and PD-L1 TS ≥50% (HR: 0.90 (95% CI: 0.71 to 1.15)) (online supplemental figure 7, with covariate balance plots in online supplemental figure 10). For TMB, we observed the trends for the estimates of the HRs when comparing rwPFS on chemoICPI versus ICPI as follows: TMB <10 (HR: 0.73 (95% CI: 0.55 to 0.96)), TMB 10–19 hour:0.60 (95% CI: 0.43 to 0.82), and TMB ≥20 (HR: 0.81 (95% CI: 0.42 to 1.55)) (online supplemental figure 7, with covariate balance plots in online supplemental figure 10). For rwOS, no trend is observed likely due to later lines of therapy that the patients received which can affect rwOS (online supplemental figure 7, with covariate balance plots in online supplemental figure 10). In sum, HR estimates favor chemoICPI across all subgroups, but precision is limited for the TMB >20 group.
Between-treatment subgroup analyses by both PD-L1 and TMB
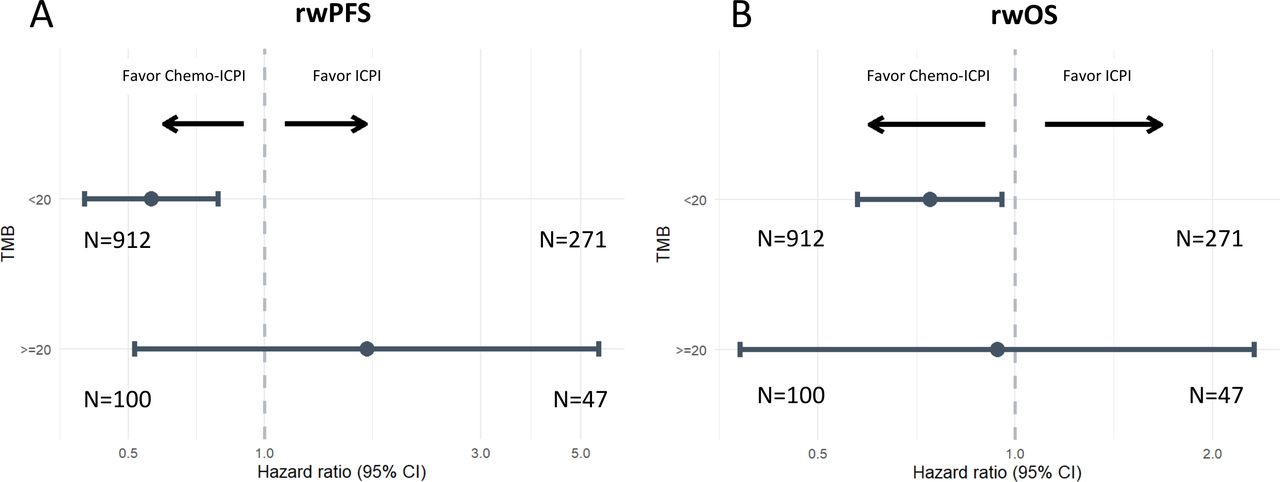
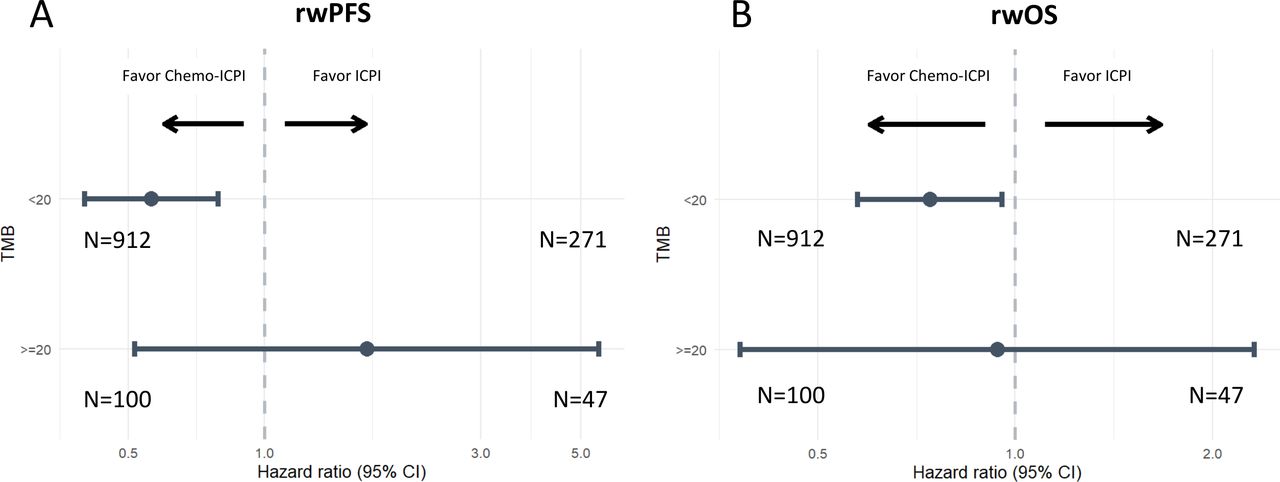
We further investigated this cohort by examining the PD-L1 TS <50% and PD-L1 TS ≥50% cohorts separately. Here, we observed trends for the estimates of the HR in the PD-L1 TS <50% cohort when comparing chemoICPI versus ICPI as follows: TMB <20 (rwPFS (HR: 0.56 (95% CI: 0.40 to 0.79))) and rwOS (HR: 0.74 (95% CI: 0.58 to 0.96)); TMB ≥20 (rwPFS (HR: 1.68 (95% CI: 0.52 to 5.48))) and rwOS (HR: 0.94 (95% CI: 0.38 to 2.32))(figure 4, online supplemental figures 8,9, with covariate balance plots in online supplemental figure 10). In the PD-L1 TS ≥50% cohort, the trends when comparing chemoICPI and ICPI were as follows: TMB <20 (rwPFS (HR: 0.93 (95% CI: 0.73 to 1.19))) and rwOS (HR: 1.05 (95% CI: 0.84 to 1.32)) and TMB ≥20 (rwPFS (HR: 0.94 (95% CI: 0.31 to 2.91))) and rwOS (HR: 1.42 (95% CI: 0.49 to 4.11)) (online supplemental figures 8 with covariate balance plots in online supplemental figure 10).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Between-treatment subgroup analyses by both PD-L1 (TS <50%) and TMB (<20 and ≥20). (A) rwPFS and (B) rwOS estimates of the HR in the PD-L1 TS <50% cohort when comparing chemoICPI versus ICPI and stratified by TMB <20 and ≥20. Multivariable Cox proportional hazard models were fitted on rwPFS and rwOS to estimate the adjusted HR and its significance. Features included in the Cox model included age at treatment start, ECOG (0~1, 2+, and unknown), sites of metastasis, history of smoking, disease histology, stage at initial diagnosis, and therapy class. Covariate imbalance between patients receiving ICPI and chemoICPI was adjusted using inverse probability of treatment weighting. chemoICPI, ICPI with chemotherapy; ECOG, Eastern Cooperative Oncology Group Performance Status Scale; ICPI, immune checkpoint inhibitors; PD-L1, programmed death ligand-1; rwOS, real-world overall survival; rwPFS, real-world progression free survival; TMB, tumor mutational burden; TS, tumor staining.
Discussion
In this study, we showed that TMB and PD-L1 expression are independent biomarkers for 1L NSCLC in patients treated with ICPI regimens. Specifically, when we examined rwPFS and rwOS we saw that both the single biomarker high (TMB or PD-L1 high) groups had better and more favorable outcomes than the double biomarker low group (TMB and PD-L1 low). Even more importantly, we observed a striking increase in rwPFS and rwOS in the double biomarker high group when compared with the double biomarker low group. This data suggests that in addition to TMB and PD-L1 expression being independent biomarkers to predict outcomes to ICPI containing regimens, the combined positivity of both biomarkers predicts the strongest response to ICPI containing regimens. Mechanistically, we hypothesize that the double biomarker high act similarly to the two ‘hit’ hypothesis by representing tumors that are more likely to evade immune attack (through PD-L1 expression) and are more susceptible to the effects of ICPI (evidenced by higher levels of TMB) leading to a more pronounced response to ICPI. The data here suggest that in addition to PD-L1, TMB testing with a validated assay may add meaningful information for the physician as they plan treatment for patients in their care.
As an independent biomarker, we saw that TMB was highly prognostic for 1L NSCLC in both the ICPI and chemoICPI groups. This was exemplified by a significant increase in rwPFS and rwOS in the TMB ≥10 muts/Mb group when compared with the TMB <10 muts/Mb group in the ICPI cohort. The same trends were seen in the chemoICPI group. While TMB was approved as a CDx in patients with cancer progression following previous treatment, new real-world evidence has been shown predictive value of TMB in the 1L setting in several tumor types such as urothelial carcinoma35 and other TMB ≥10 muts/Mb solid tumors at later lines of therapy.36 At the time of this study, the current and most widely used TMB cut-off is 10 muts/Mb. However, emerging evidence suggests that a higher cut-off can better select patients who are far more likely to be exceptional responders to ICPI. For example, in a pooled cohort of 1552 patients with NSCLC, Ricciuti et al, observed higher rwPFS and rwOS in the TMB high (defined as TMB ≥19 muts/Mb) cohort when compared with patients the TMB low cohort (defined as TMB <19 muts/Mb) (11.4 vs 2.8 months and 36.1 vs 12.4 months, respectively).26 In this study, we explored a higher cut-off of 20 muts/Mb and saw that in both the ICPI and chemoICPI group, the TMB ≥20 group responded exceedingly well to ICPI containing therapy and is enriched for durable responders (rwPFS ≥24 months). In totality, these real-world data suggest that TMB is a highly prognostic biomarker for ICPI containing regimens in 1L NSCLC when using TMB ≥20 muts/Mb as the TMB cut-off for 1L patients with NSCLC.
Lastly, we explored the predictive value of TMB and PD-L1 for ICPI versus chemoICPI. Here, we observed that PD-L1 TS ≥50% might identify populations that could potentially receive minimal additional benefit from chemo, while patients who have both PD-L1 TS <50% and TMB <20 appear to have more favorable outcomes including chemo with ICPI. What is less clear is whether patients with PD-L1 TS <50 and TMB ≥20 perform better on a chemo-sparing ICPI, a question that should be further answered definitively in future clinical trials. Of note, despite the low PD-L1, this group had favorable outcomes on ICPI alone (median rwPFS 12.6 months and median rwOS 21.9 months) (online supplemental figure 9) when compared with the real-world outcomes of the broader high PD-L1 (TS ≥50%, without TMB substratification) group treated with ICPI alone (median rwPFS 10.7 months and median rwOS 14.5 months) (online supplemental figure 2). Reviewing the 2165 patients with CGP and PD-L1 testing studied in this paper, PD-L1 testing identified that 39% of the patients are potential candidates for ICPI alone based on PD-L1 TS ≥50. Seven per cent of the patients in this cohort have low PD-L1 with TMB ≥20 and while the absolute HR suggested more favorable rwPFS in patients receiving ICPI alone, the CI is wide, likely due to the relatively small subcohort, and conclusive interpretation is difficult and should be further evaluated in clinical studies. In the remaining 55% of the patients, chemoICPI might be favored, though other emerging biomarkers may be useful for identifying ICPI without chemo among this population. Importantly, to the best of our knowledge, no completed clinical trials have evaluated ICPI versus chemoICPI using TMB as a biomarker. Of note, while the KN-189 and KN-40737 studies did not show evidence that TMB has predictive value for a different clinical decision point (chemoICPI vs chemo alone) in patients with NSCLC, these studies used a 175 mut/exome WES TMB cut-off (equivalent to a 10 muts/Mb cut-off) in their analysis. Our data, along with Ricciuti et al data,26 showcases that a 20 muts/Mb cut-off could be a more clinically meaningful cut-off to study for NSCLC in various clinical decision scenarios. The question of patient selection for ICPI monotherapy versus ICPI plus chemotherapy in treatment-naïve NSCLC is currently being evaluated in two ongoing phase III trials, INSIGNA (NCT03793179) for patients with PD-L1 ≥1% and PERSEE (NCT04547504) for those with PD-L1 ≥50% and represents studies where investigators could explore the very high TMB (≥20) cut-off. Lastly, our finding that PD-L1 1–49% correlates with better response to chemoICPI as opposed to ICPI alone is consistent with previous FDA pooled analysis.38 39
One of the main limitations of this study is that all patients were tested with the F1/F1CDx assay. While the general trends of the results in the study are applicable to other assays, the TMB scores from other assays are not equivalent to assays like F1/F1CDx that have sufficient panel coverage and have undergone requisite algorithmic and analytical validation to estimate TMB from a panel.40 As a result, conclusions derived from this study are applicable to the assays evaluated herein. In addition, the clinical data from CGDB were derived from the EHR and data not documented in the EHR may be incomplete or missing, particularly for events occurring outside of the FH network. rwPFS was abstracted from the EHR and are limited by clinician interpretation and documentation. A Response Evaluation Criteria in Solid Tumors (RECIST)-based approach to assessment of progression was impractical due to missing data (clinicians are unlikely to employ the same level of quantitative rigor needed to objectively and consistently apply RECIST in their routine care of patients), but the clinician-anchored approach used to abstract progression events from the EHR has been shown to be replicate associations with and serve as a pragmatic alternative to RECIST-based progression.41 Furthermore, compared with clinical trials, there is greater variation between patients in a real-world analysis with respect to follow-up intervals, that is, the time points at which progression can be assessed. Lastly, selection bias is likely also present due to all patients in this study having received CGP.
Conclusions
In this study, we showed with a large real-world cohort of patients that TMB adds additional prognostic value to 1L patients with NSCLC in addition to PD-L1 and suggests a potential role for testing TMB along with PD-L1 to impact treatment selection contingent on validation by future studies. In addition, we presented real-world evidence of higher TMB cut-offs such as 20 muts/Mb identifying patients with prolonged benefit and should be further explored in clinical studies. Lastly, we observed that high PD-L1 and/or very high TMB could potentially identify populations that may not need the addition of chemotherapy, while patients who have both low PD-L1 and TMB <20 are likely to benefit from chemo added to ICPI. These results could be further validated in future trials, or in prospective–retrospective analyses of existing, completed studies.42
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study have been originated by Flatiron Health and Foundation Medicine. These de-identified data may be made available upon request and are subject to a license agreement with Flatiron Health and Foundation Medicine; interested researchers should contact <cgdb-fmi@flatiron.com> and <dataaccess@flatiron.com> to determine licensing terms.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @RyonGraf, @cyclokar
Contributors Conception/design: RSPH, AS, GRO. Provision of study material or patients: RSPH, JS. Collection and/or assembly of data: GL, LZ. Data analysis and interpretation: All authors. Manuscript writing: All authors. Final approval of the manuscript: All authors. Guarantor: RSPH.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests RSPH, GL, AS, RG, LZ, KM, JSR, KT, and GRO are employees of Foundation Medicine, a wholly owned subsidiary of Roche and these employees have equity interest in Roche. DC is an employee/paid consultant for AbbVie, Adaptimmune, Agenus, Amgen, Ariad, AstraZeneca, Biocept, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, EMD Serono, Foundation Medicine, Genentech/Roche, Gritstone, Guardant Health, Inovio, Merck, MSD, Novartis, Palobiofarma, Pfizer, prIME Oncology, and Takeda, and reports receiving commercial research grants from Bristol Myers Squibb. JSR has consulting/advisory board AstraZeneca, Curadev, Daiichi-Sankyo, Jazz Pharmaceuticals, Medtronic, Pharma Mar. DS reports receiving research funding from AstraZeneca, Genentech/Roche, Novartis, Celgene, Bristol Myers Squibb, Pfizer, Boehringer Ingelheim, AbbVie, Foundation Medicine, GlaxoSmithKline, Eli Lilly, Merck, Nektar, Takeda, Amgen, University of Texas Southwestern Medical Center–Simmons Cancer Center, G1 Therapeutics, Neon Therapeutics, Celldex, Clovis Oncology, Daiichi Sankyo, EMD Serono, Astellas Pharma, GRAIL, Transgene, Aeglea Therapeutics, Tesaro, Ipsen, Janssen, BIND Therapeutics, Eisai, and ImClone Systems; and consulting, advisory, and/or speakers’ bureau fees from AstraZeneca, Genentech/Roche, Novartis, Celgene, Bristol Myers Squibb, Pfizer, Boehringer Ingelheim, AbbVie, Foundation Medicine, GlaxoSmithKline, Eli Lilly, Merck, Moderna, Nektar, Takeda, Amgen, TRM Oncology, Precision Oncology, Evelo Therapeutics, Illumina, Pharmamar, EMD Serono, Aptitude Health, Dracen Pharmaceuticals, Iksuda Therapeutics, Molecular Templates, Seattle Genetics, TRIPTYCH Health Partners, and Intellisphere.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.