Article Text

Abstract
Background Aviscumine, a recombinant plant protein, is an immune modulator that induces ribotoxic stress at the 28S ribosomal RNA subunit. In this way cytokine release and T-cell responses are enhanced. This phase II trial was conducted to test the efficacy and safety of aviscumine in patients with systemically pre-treated metastatic melanoma stage IV.
Methods A total of 32 patients with progressive stage IV melanoma after failure of standard therapy were enrolled onto a single-arm, multi-centre, open-label, phase II trial. All patients had an ECOG performance status of 0 or 1. Patients received 350 ng aviscumine twice weekly by subcutaneous injection until progression. The primary end points were progression-free survival (PFS) and overall survival (OS). Safety was assessed as adverse events (AEs). Tumor response was assessed every eight weeks and survival of patients was followed up to one year after the end of therapy. Thirty one patients (intent-to-treat population (ITT)) were assessed for efficacy; safety was assessed in the whole population.
Results One patient achieved a partial response (PR) and 10 patients showed stable disease/no change (SD). The median progression-free survival (mPFS) was 63 days (95% CI 57–85) and median overall survival (mOS) was 335 days (95% CI 210–604). In total 210 treatment-emergent adverse events were recorded. Grade 1 or 2 AEs occurred in 72% of patients and were mostly application-site effects such as pruritus Grade 3–4 treatment-emergent drug-related adverse events occurred in 9% of patients.
Conclusion These results suggest that aviscumine may have a clinical impact in patients with previously treated metastatic melanoma and provide rationale for further clinical evaluation of this agent. In the light of effective new immune checkpoint blockers it might be a candidate for combinations with these agents.
Trial registration ClinicalTrials.gov: NCT00658437
- Aviscumine
- Cancer immunotherapy
- CY-503
- Metastatic melanoma stage IV
- Phase II trial
- Ribosome-inactivating protein
Statistics from Altmetric.com
- Aviscumine
- Cancer immunotherapy
- CY-503
- Metastatic melanoma stage IV
- Phase II trial
- Ribosome-inactivating protein
Background
Cutaneous malignant melanoma causes a small number of skin cancers but leads to nearly 80% of skin cancer deaths [1]. Annually, there are worldwide around 160,000 new cases of malignant melanoma with 41,000 deaths and it has the fastest rising incidence of all skin cancers among men and the second-fastest among women — which is predicted to continue [2]. Prognosis for patients with stage IV metastatic melanoma is poor [3]. In a meta-analysis of 42 phase II trials, median survival was only 6.2 months, with a 1-year survival rate of 25.5% regardless of treatment regimen [4].
Dacarbazine (DTIC), the only chemotherapeutic agent approved in the US and in Europe for the treatment of metastatic melanoma, is associated with a response rate of 5–12% and a median overall survival of 5.6 to 9.1 months after the initiation of therapy [5]–[11].
Given the known immunogenicity of melanoma [12]–[14] many studies have evaluated the combination of chemotherapy with immunotherapy, particularly regimens containing interferon alfa and interleukin-2 (IL-2) [15]. These biochemotherapeutic approaches increase response rates but could not improve survival [16]–[18]. Also mono-immunotherapy with high dose IL-2 has never been shown to significantly prolong survival in phase III trials in patients with advanced stage IV melanoma [19],[20]. In addition, IL-2 treatment-related toxicity is severe and often requires inpatient intensive care [21]–[23].
However, monotherapy with ipilimumab, a fully human monoclonal antibody (IgG1) that blocks CTLA-4 to promote antitumor immunity, has shown meaningful clinical activity including an improvement of overall survival in patients with metastatic melanoma in phase II and III studies [11],[24]–[27].
Approximately 40 to 60% of cutaneous melanomas carry mutations in BRAF that lead to constitutive activation of downstream signalling through the MAPK pathway [28],[29]. Therefore, treatment with selective BRAF and MEK inhibitors is restricted to patients with mutation-positive melanomas. Recently a phase III randomized clinical trial comparing vemurafenib, a potent inhibitor of mutated BRAF [30], with DTIC in patients with previously untreated, metastatic melanoma with a BRAF V600 mutation has shown improved rates of overall and progression-free survival for vemurafenib [31]. Moreover, a phase III randomized clinical trial of previously untreated BRAF V600E mutated melanoma patients compared dabrafenib to dacarbazine and demonstrated improvements in RR (50 vs. 6%) and PFS (5.1 vs. 2.7 months) [32]. Treatment of a similar patient population with the MEK inhibitor trametinib in those who had not previously received a BRAF inhibitor resulted in a median overall survival of 14.2 months and estimated 1-year survival of 59% [33].
Aviscumine, a recombinant plant protein, is a class II ribosome-inactivating protein. The drug preferentially and specifically binds to cell-surface structures containing CD75s (α2,6 sialolactosamine) [34]–[36]. CD75s structures are over-expressed in solid tumour cells [37],[38], in immune cells (e.g. granulocytes, monocytes/macrophages, B-cells) and in endothelial cells as well as in epithelial cells [39]–[43]. Binding enables internalisation of the drug and subsequent selective cleavage of the N-glycosidic bond of the adenine-4324 residue in the eukaryotic 28S ribosomal RNA, thus inducing catalytic inactivation of the ribosomes and inhibition of protein synthesis (“ribotoxic stress”) [44]. The “ribotoxic stress” induces T-cell responses, activation of natural killer cells, and antigen-presenting cells (APCs) (e.g. monocytes/macrophages, dendritic cells), and stimulation of cytokine release [45],[46]. IL-1β and IFN-γ seem to be the most relevant cytokines. The disease stabilisation in patients with advanced cancer observed in a phase I trial was associated with an increase of plasma levels of IL-1β and IFN-γ [47].
Here we report results from a single-arm, multi-centre, open-label, phase II trial to investigate the efficacy and safety of subcutaneously administered aviscumine (CY-503) monotherapy in patients with unresectable stage IV metastatic melanoma after failure of one or more previous anti-neoplastic therapies.
Results
Between April 2008 and May 2009 32 pretreated patients with confirmed metastatic melanoma (stage IV) were included in the study. Baseline characteristics are shown in Table 1. Characteristics of patients, which are known to be prognostic in stage IV melanoma patients (age, sex, stage, and LDH), were well balanced. For efficacy analyses, 31 patients met the eligibility criteria and were evaluated as the ITT population.
Demographic and clinical characteristics of patients at baseline
The mean duration of treatment was 104.7 (SD 98.0) days. Patients received a mean of 6.2 (range 1–8) injections per cycle and 25.6 injections (range 1–127) overall. The most frequent reason for discontinuation of therapy was disease progression. 10 patients (32.3%) had stable disease during the study, one patient showed partial response. The disease control rate (DCR) was 35.5% (11 of 31 patients) (Table 2). Median PFS was 63 days (95% CI 57–85).
Overall response and disease control rates (ITT population)
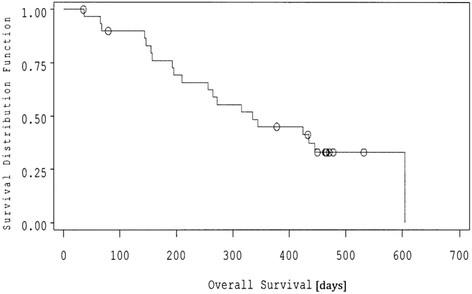
Kaplan-Meier analysis of OS was conducted. The observed mOS was 335 days (95% CI 210–604) (Figure 1). Using a benchmark analysis according to Korn [4] the predicted mOS was 256 days (95% CI 155–378). The predicted 1-year survival rate was 33.1% (95% CI 16.5-49.7) (historical 1-year OS) [4] in comparison to the observed 1-year survival rate of 45.0% (95% CI 29.8–60.2). The hazard ratio for death was 0.75 (95% CI 0.42-1.36), indicating a possible survival benefit in this study.
{kind=link}
Kaplan–Meier estimates of overall survival by ITT population О censored numbers.
mOS data and 1-year-survival rates were analysed among patient subgroups (Table 3). There was no difference in mOS and 1-year survival rates between ECOG 0 and ECOG 1 subgroups or in the pretreatment groups. However, females showed a tendency to better 1-year survival (53.3%) as compared to males (36.4%). Patients showing disease control exhibited mOS of 14.3 months and a 1-year survival rate of 72.7% (Table 3). Interestingly, patients with an induced injection site reaction showed a longer survival (mOS: 445 days, 95% CI: 335–604) compared to patients without induced injection site reactions (mOS: 155 days, 95% CI: 67–210).
Survival by subgroup in ITT population
The safety population (32 patients) included all patients who had undergone randomization and who had received any amount of study drug. In total 210 AEs were recorded between the first dose and 30 days after the last dose of aviscumine. All 32 patients experienced at least one AE. The most frequent AEs were application-site effects in 23 (72%) patients. Fifty eight (27.6%) AEs in 24 patients were deemed probably, possibly or certainly related to the study drug. Of these, most were NCI CTCAE grade 1 or grade 2; 8 (13.8%) were grade 3–4 events (Table 4).
Drug-related adverse events (n = 58) for safety population (n = 32)
Twelve SAEs occurred in five (16%) of 32 patients. Two patients died from dyspnoea and tachyarrhythmia, respectively, but these events were not deemed to be related to the study drug. The other three patients had thrombocytopenia, cerebral ischaemia (both CTCAE grade 4), chest pain (CTCAE grade 3) and atrial fibrillation, dehydration, pneumonia, venous thrombosis, urinary tract infection and urosepsis (all CTCAE grade 3).
IgG and IgM anti-aviscumine antibody data were available for 29 patients. All except two patients developed IgG anti-aviscumine antibodies of different strength during the trial. One additional patient had an anti-aviscumine IgG antibody titer at baseline. The titers were in the range 11 – 1,690 μg/mL. Furthermore most of the patients with IgG antibody titer showed also an IgM titer. A correlation between anti-aviscumine antibody titers and PFS and OS, respectively, could not be detected (Cox regression analysis for PFS and OS, respectively: p > 0.05).
Discussion
Aviscumine treatment at a dose of 350 ng resulted in a median overall survival of 11 months and a 1-year survival rate of 45% in patients with unresectable metastatic malignant stage IV melanoma who had undergone previous treatment. The 1-year survival rate regarded as a key benchmark for comparing efficacy of novel therapeutics versus historical data is notably higher than the predicted value of 33.1% [4]. More than 70% of the patients had M1c disease indicating the presence of visceral metastasis, and more than 50% had elevated lactate dehydrogenase levels, both of which are associated with very poor survival [4],[48].
The hazard ratio for death is 0.75 (95% CI 0.42-1.36) indicating a possible survival benefit in the aviscumine study compared with historical data of Korn et al. [4]. Also the median overall survival in our study (11 months) compares favorably with 8.4 months from a historical survival curve [4]. Nevertheless we have to state that the numbers enrolled are small.
In a phase II trial of sorafenib with temsirolimus (arm a) or tipifarnib (arm b) in untreated metastatic melanoma patients the median OS was 7 months in both treatment arms, while the number of patients achieving an objective response was seen in 4.7% and 2.6%, respectively [49]. Ipilimumab (3 mg/kg), an anti-CTLA4 antibody, showed a 1-year survival rate of 39.3% and a median OS of 8.7 months in a phase II trial with 50% M1c patients [26].
In recent randomized, phase III trials involving patients with unresectable stage III or IV melanoma who had received previous treatment, 1-year survival rates were reported to be 22% to 38% with various treatment regimens [50],[51]. The median overall survival in these studies ranged from 5.9 to 9.7 months. Neither these nor other randomized, controlled trials had shown a significant improvement in overall survival.
However, ipilimumab was shown in two phase III, randomized, controlled trials to increase the survival in patients with unresectable metastatic melanoma (stage III and IV) as compared with a peptide vaccine from 6.4 to 10.0 months [27] or with DTIC from 9.1 to 11.2 months [11]. Compared with the vaccine the 1-year survival rate was 45.6%, but there was only a modest effect on rates of response and progression-free survival [27]. The use of ipilimumab combined with DTIC in patients with unresectable metastatic melanoma (stage III and IV) has also been associated with improved rates of survival over DTIC alone [11]. The 1-year survival rate in the first-line treated ipilimumab/DTIC arm was 47.3% and in the first-line placebo plus DTIC arm was 36.3% [11].
In the context of published clinical experience with comparable patient populations, the 1-year overall survival rate of 62% and a median overall survival of 16.8 months associated with nivolumab, an immune checkpoint blocker of the anti-PD-1 antibody type, are particularly important [52].
Clinical activity of aviscumine was observed in all subgroups of patients, including patients with stage M1c disease. It was also seen both in ECOG 0 or in ECOG 1 patients. The median overall survival was 10.8 months vs. 11.0 months and the 1-year survival rate was 44% vs. 47% . This finding is interesting due to the known association between performance status and overall survival and the inclusion of the performance status as an important prognostic factor for stage IV melanoma patients [4],[53]. The predicted 1-year overall survival rate for patients with visceral disease (M1b and M1c) was 23.8% [4] in comparison to 42.3% in this study.
The median progression-free survival was 63 days and was not different to standard therapy. Also Hodi reported only a modest effect on rates of response and progression-free survival for the immunotherapeutic ipilimumab [27]. Regarding the immunotherapeutic approaches it is discussed that conventional definition of disease progression incompletely reflects the survival benefit [54],[55].
Overall, 35.5% of the patients treated with aviscumine met the criteria for a confirmed disease control (SD, PR), whereby most patients had SD. The high rate of SD may be viewed as an indicator of a meaningful therapeutic effect. Disease control due to SD is characteristic for immunotherapeutics and other biologics in cancer [54]. For example in a recent phase II combination trial of dendritic cell vaccination, interleukin-2 and metronomic cyclophosphamide the median OS was 9.4 months, while none of the patients achieved an objective response, but 57% of the patients achieved stable disease (SD) [56].
The confirmed DCR in our study is slightly higher than the DCR of 28.5% and 33.2% in the ipilimumab phase III trials [11],[27]. Even in the EORTC phase I trial of aviscumine to treat solid malignant tumors, twice weekly subcutaneous injections up to 10 ng/kg body weight showed a disease control rate of 31%, lasting from 11.3 to 35.7 weeks [47].
Patients receiving aviscumine reported only 8 drug-related adverse events grade 3 or 4. These were cerebral ischaemia, dyspnoea, hyperglycaemia, leukopenia, neutropenia, pruritus, thrombocytopenia and venous thrombosis. The majority of drug-related adverse events (application site reactions, grade 1 or 2) were immune-related and consistent with the proposed mechanism of action of aviscumine. The patient with cerebral ischaemia started into the trial with known leukopenia and thrombocytopenia due to previous chemotherapy.
Subcutaneous injection of aviscumine induced anti-aviscumine antibodies. The induction of these antibodies did not have any influence on the outcome parameters disease control rate and survival. Although the mechanism underlying the activity of aviscumine is not fully understood, it is known that the drug induces a strong immune response via pleiotropic mechanisms due to activation either of the innate or the adaptive immune system [45],[46].
In conclusion, the relatively high DCR and relatively long OS in patients with unresectable metastatic melanoma (stage IV), the good tolerability of 350 ng aviscumine per injection after failure of dacarbazine or other previous therapies suggest that larger, randomized, controlled clinical trials also as treatment combinations considering the immune-related response criteria (irRC) [54] are now warranted.
Conclusions
Aviscumine treatment at a dose of 350 ng (twice-weekly subcutaneously injected) resulted in clinical activity in patients with unresectable metastatic malignant stage IV melanoma who had undergone previous treatment. These results provide rationale for further clinical evaluation of this agent. In the light of effective new immune checkpoint blockers it might be a candidate for combinations with these agents.
Methods
Patients
Patients had to be at least 18 years old, with histologically confirmed stage IV melanoma with unresectable metastases and one or more measurable lesions. All patients had received at least one prior line of anti-neoplastic therapy. They had Eastern Cooperative Oncology Group (ECOG) performance status 0 or 1, LDH ≤2.5 ULN, serum creatinine levels ≤1.5 mg/dL, absolute neutrophil count ≥1.5 × 109/L, platelet count ≥100 × 109/L, and life expectancy ≥3 months. Patients had measurable disease according to Response Evaluation Criteria In Solid Tumors (RECIST) guidelines [57]. Exclusion criteria included pretreatment with mistletoe extracts, CNS metastasis, and ocular or mucosal melanoma.
Study design
The study was conducted at 4 centres in Germany between April 2008 and May 2010. Patients received twice-weekly subcutaneous injections of 350 ng aviscumine in 1 mL solution in the thigh or abdomen. Injections were done on the same 2 days of each week (4 weeks = 1 cycle), at least 3 days apart (e.g., Monday and Thursday, Tuesday and Friday).
Blood for analysis of anti-aviscumine antibodies was taken at baseline, at the end of every cycle and at the end of therapy. Anti-aviscumine antibodies (IgG and IgM) were measured with an ELISA using monoclonal anti-aviscumine antibody clone 36 (mouse, Cytavis BioPharma) and aviscumine bound to the titer plate. Detection was performed with anti-human IgG-POD and anti-human IgM-POD (both goat, Sigma-Aldrich) and colour reaction with TMB (Dako). Quantification of antibodies was performed in relation to standards: human IgG (Sigma-Aldrich), human IgM (Millipore).
Treatment was scheduled to continue without pause until disease progression (increase ≥20% in the sum of the longest diameters of the target lesions and/or new lesions) or a withdrawal criterion occurred. Withdrawal criteria were as follows: pregnancy or decision to become pregnant; toxic effects potentially related to the study drug that required discontinuation (≥grade 3 hypersensitivity and haematological or non-haematological reactions confirmed after 48 h); and other contraindication events (eg. illnesses or complications).
Supportive care and treatment of AEs were left to the investigator’s discretion. Corticosteroids, immunostimulating substances and/or monoclonal antibodies were not allowed except for in life-threatening situations, when corticosteroids and colony-stimulating factors could be used. Antiemetics could be used if appropriate. Other anticancer agents were not allowed.
The study was carried out in compliance with current Good Clinical Practice, Ethics Committee recommendations, informed consent regulations, the Declaration of Helsinki [58] and with the laws and regulations of Germany. Approval was received from the local ethics committee and from the German health authority before recruitment started. All patients gave their written informed consent.
Study outcomes
The primary end points were overall survival (OS) and progression-free survival (PFS). OS was defined as time elapsed from random assignment to death from any cause. PFS was defined as time elapsed from random assignment to disease progression, or death, or start of new antitumor therapy. Up to 10 measurable lesions were assessed at baseline and every 8 weeks (2 cycles) according to RECIST guidelines. Independent evaluation of tumor images was performed by Institut f. Diagnostische u. Interventionelle Radiologie, Universitätsklinikum Frankfurt/M., Germany.
Secondary outcomes included disease control (complete remission (CR), partial remission (PR) or stable disease/no change (SD)), safety (defined by the occurrence and severity of AEs), and anti-aviscumine antibodies in blood serum.
Safety and tolerability assessment included observed AEs, clinical laboratory tests, physical examinations, and vital sign assessments. MedRA (version 14.0) approved descriptions and assigned grades according to the Common Toxicity Criteria of the National Cancer Institute (NCI CTCAE version 3.0) were used. AEs were classified as treatment-related or unrelated according to investigator judgement. If an AE occurred more than once, it was counted only once and given the maximum CTCAE grade.
Statistical analysis
Determination of sample size
Determination of sample size was based on PFS of 3 months. The proportion of patients with stage IV malignant melanoma showing PFS of at least 3 months under DTIC-based chemotherapy is 20%. Only for the purpose of sample size planning, the value was increased to 40% and it was deemed that treatment would be unsuccessful if PFS at 3 months is ≤15%. Therefore, it was estimated that 29 eligible patients would be required to reach 80% statistical power with α = 0.05. 32 patients should be recruited to allow for 10% dropout of non-evaluable patients. Simon's two-stage design was employed [59]. If 3-month PFS is over the success threshold (≤15%) in the first 13 recruited patients the trial will be continued.
Efficacy analysis
31 patients met the eligibility criteria (ITT population) and were included in the primary efficacy analysis. The survival of patients was followed for up to 12 months.
OS and PFS were estimated by constructing Kaplan-Meier curves. Patients lost to follow-up or not progressed at time of analysis were censored. Median overall survival (mOS) and median progression-free survival (mPFS) were deduced from the Kaplan-Meier curves. The 1-y survival rates were estimated from the individual survival data of the patients.
The immunological response in respect to the analysis of anti-aviscumine antibodies was examined using descriptive analysis.
Safety analysis
All patients who had received one or more dose of study treatment were included in the safety and tolerability analysis (safety population; n = 32). Treatment-emergent adverse events (AEs) were classified and graded using National Cancer Institute Terminology Criteria for Adverse Events version 3.0. AEs were also classified according to MedRA (version 14.0).
Variability estimates are expressed as standard deviation (SD) or 95% confidence intervals (CI). Categorical variables are expressed as absolute values and percentages. Survival was estimated with the Kaplan–Meier product limit estimator, and median (95% CI) survival times are reported. OS and PFS were calculated from randomization until the occurrence of the pertinent event or last observation. The information of death due to melanoma without documented progressive disease also qualified for PFS event. Cox’s regression models were calculated for PFS and OS, with adjustment for following subgroups: ECOG performance status (0, 1), grade (no visceral, visceral), sex (male, female), age (≤60 years, >60 years), number of previous treatments (<2, ≥2), and patients with disease control (non-progressive, progressive). Survival data were compared with predicted values calculated for each individual subject based on the prognostic variables included in the meta-analysis of Korn et al.[4] using the group of trials that excluded brain metastases. Survival analyses were made in the intention-to-treat (ITT) population and safety was assessed in all patients. Fisher’s exact test was used to calculate two-sided significance values, with p < 0.05 deemed significant.
This study has not been previously presented in full or in part elsewhere.
Acknowledgments
The authors thank Beate Volkmer of Division of Molecular Cellbiology, Dermatology Center, Buxtehude, Germany for measuring the anti-aviscumine antibodies, Jennifer Schmitz and Michael Bulitta, CRMB, Rheinbach, Germany for data analysis. Manuscript writing assistance was provided by Kathryn Senior of Freelance Copy, London, UK.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
![[40425_2014_27_MOESM1_ESM.gif]](https://jitc.bmj.com/content/jitc/2/1/27/DC1/embed/media-1.gif?download=true){kind=link}
References
Footnotes
Competing interests Funding for the study was provided by CYTAVIS BioPharma GmbH, Hamburg, Germany.
Authors’ contributions HL, KW, PM, RG, UT participated in the study conception and design. PM was the principal investigator. FS, KK, RG, TW, UT were investigators. VJ carried out the independent evaluation of tumor images. HL, KW, UT drafted the manuscript. The approval of the manuscript was done by FS, HL, KK, KW, PM, RG, TW, UT, VJ. All authors approved and read the final manuscript.
Electronic supplementary material The online version of this article (doi:10.1186/s40425-014-0027-z) contains supplementary material, which is available to authorized users.