Article Text

Abstract
Background The combination of CTLA-4 and PD-L1 inhibitors has a manageable adverse effect profile, although rare immune-related adverse events (irAE) can occur.
Case presentation We describe an autoimmune polymyositis following a partial response to combination tremelimumab and durvalumab for the treatment of recurrent lung adenocarcinoma. Radiography revealed significant reduction in all metastases; however, the patient developed progressive neuromuscular hypoventilation due to lymphocytic destruction of the diaphragmatic musculature. Serologic testing revealed a low level of de novo circulating antibodies against striated muscle fiber. Immunohistochemistry revealed type II muscle fiber atrophy with a mixed CD8+ and CD4+ lymphocyte infiltrate, indicative of inflammatory myopathy.
Conclusions This case supports the hypothesis that muscle tissue is a target for lymphocytic infiltration in immune checkpoint inhibitor-associated polymyositis. Further insights into the autoimmune mechanism of PM will hopefully contribute to the prevention and treatment of this phenomenon.
- Immune-related adverse event
- Non-small cell lung cancer
- Programmed death protein 1
- Programmed death-ligand 1
- Cytotoxic T-lymphocyte-associated-protein 4
- Immune checkpoint inhibitor
- Myasthenia gravis
- Striated muscle antibody
- MEDI4736
- AChR
- Acetylcholine receptor
- ASM
- Anti-striated muscle
- BiPAP
- Bilevel positive airway pressure
- CD
- Cluster of differentiation
- CO2
- Carbon dioxide level
- CSF
- Cerebrospinal fluid
- CT
- Computed tomography
- CTCAE
- Common toxicity criteria for adverse events
- CTLA-4
- Cytotoxic T-lymphocyte-associated protein 4
- GvHD
- Graft-versus-host disease
- H&E
- Hematoxylin and eosin
- HIER
- High pH heat induced epitope retrieval
- ICH –GCP
- International conference on harmonization good clinical practice
- IFN-γ
- Interferon gamma
- IHC
- Immunohistochemistry
- irAE
- Immune-related adverse events
- IV
- Intravenous
- IVIG
- Intravenous immunoglobulin G
- KRAS
- Kirsten rat sarcoma viral oncogene homolog
- MHC
- Major histocompatibility
- MRI
- Magnetic resonance imaging
- MuSK
- Muscle specific kinase protein
- NCT
- National clinical trials
- PBMCs
- Peripheral blood mononuclear cells
- PD-1
- Programmed cell death protein 1
- PD-L1
- Programmed death ligand 1
- Pex
- Plasma exchange
- PM
- Polymyositis
- RECIST
- Response evaluation criteria in solid tumor
- TAR DP-43
- Transactive response DNA binding protein 43 kDa
- TCR
- T cell receptor
- VGCC
- Voltage gated calcium channel
- wks
- Weeks
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Statistics from Altmetric.com
- Immune-related adverse event
- Non-small cell lung cancer
- Programmed death protein 1
- Programmed death-ligand 1
- Cytotoxic T-lymphocyte-associated-protein 4
- Immune checkpoint inhibitor
- Myasthenia gravis
- Striated muscle antibody
- MEDI4736
Background
Combination therapy with anti-cytotoxic T-lymphocyte-associated-protein 4 (CTLA-4) and anti-programmed death ligand 1 (PD-L1) monoclonal antibodies holds incredible potential for the treatment of solid tumors [1]. Despite their robust activity, these immune checkpoint inhibitors can have rare but important immune-related adverse events (irAEs). Specifically, CTLA-4 inhibitors have been associated with irAEs in most organ systems, including enterocolitis, hepatitis, and endocrinopathy [2]. Among these irAEs, there are several cases of inflammatory myopathies [3].
Polymyositis, dermatomyositis, and inclusion body myositis (IBM) are among a group of inflammatory myopathies associated with muscle weakness and inflammatory infiltrates within skeletal muscle. Polymyositis (PM) is a subacute myopathy which differs from other subgroups by perifascicular atrophy and the absence of vacuoles [4]. In animal models, PM is induced by clonal expansion of cluster of differentiation (CD) 8+ cells of specific T cell receptor (TCR) families targeting muscle tissue. High levels of interferon gamma (IFN-γ) lead to up-regulation of MHC class I in myotubes, even in areas far from sites of inflammation [5]. Perforin-dependent cytotoxicity mediated by CD8+ T cells causes muscle fiber atrophy and necrosis [6]. Diaphragmatic weakness is one of the most prominent and life-threatening consequences of autoimmune myositis [7].
Herein we describe a patient treated with a single infusion of combination anti-CTLA-4 and anti-PD-L1 antibody, and subsequently incurred a fatal destructive lymphocytic myositis involving the inspiratory muscles. We performed a retrospective analysis of this subject with the primary objective to further characterize the immunopathology of this rare adverse event.
Case presentation
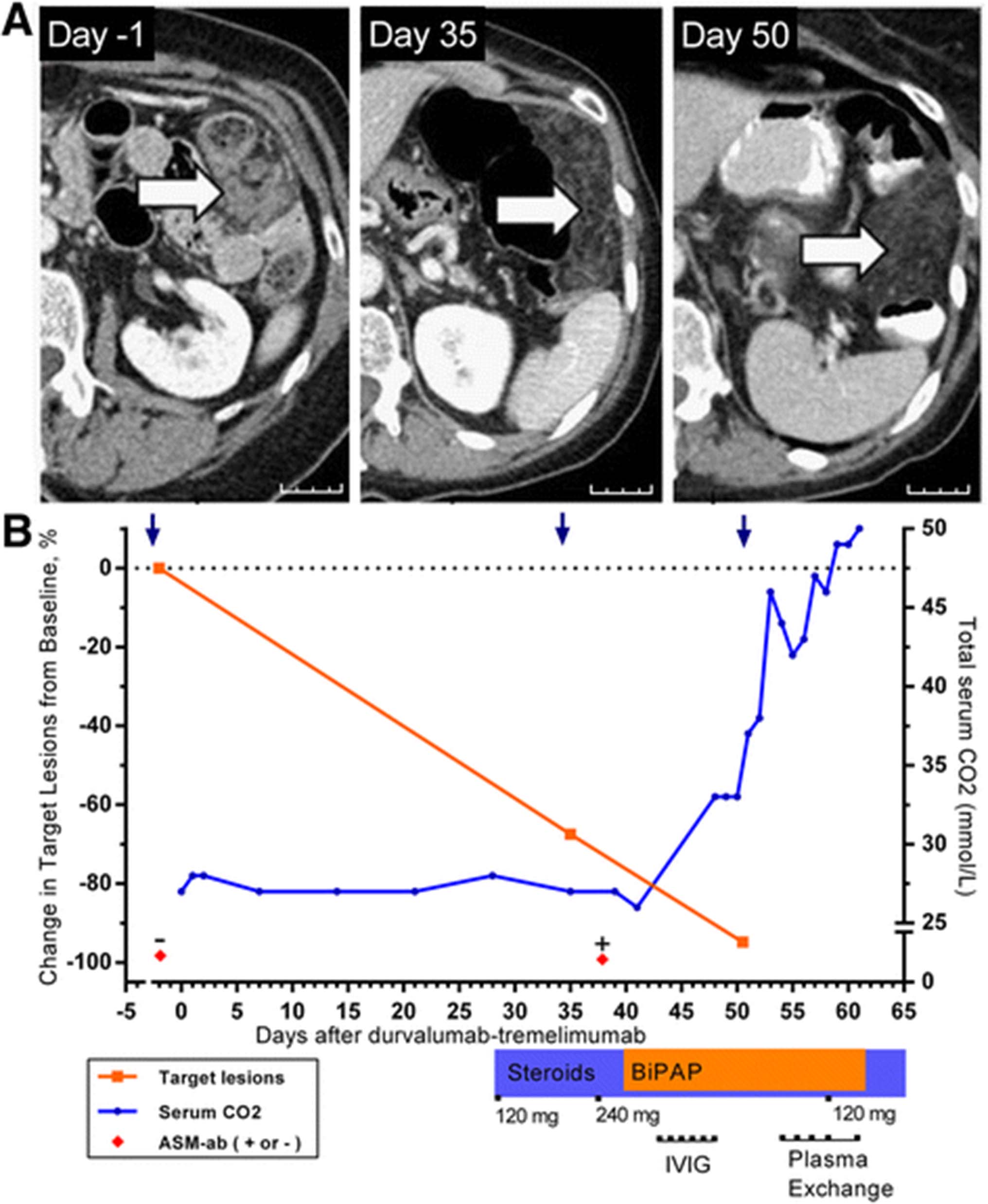
A 64-year-old female former smoker presented with lung adenocarcinoma originally treated with right pneumonectomy. Follow-up imaging four years later revealed a recurrence involving the omentum, confirmed by biopsy. Primer-extension mass spectrometry genotyping of the tumor revealed a KRAS G12C mutation, and immunohistochemistry showed no PD-L1 expression in tumor cells. She was seronegative for HIV and viral hepatitis. The patient expressed a preference for immunotherapy instead of palliative chemotherapy. She began a phase 1 clinical trial (NCT02000947) consisting of tremelimumab (1 mg/kg) and durvalumab (10 mg/kg) IV over 1 h on Day 1 [8]. At Day 28, she reported progressive dysphagia and a barium esophagram demonstrated hypomotility. Soon thereafter, she developed respiratory acidosis. Magnetic resonance imaging (MRI) was normal, and lumbar puncture revealed normal cerebrospinal fluid (CSF) cell count with negative cytology. Computed tomography (CT) scan demonstrated a significant reduction in the size of the omental metastases (Fig. 1). Further tremelimumab -durvalumab was stopped, and she was treated empirically with high-dose prednisone at 120 mg/day. Despite this, she experienced progressive neuromuscular hypoventilation requiring continuous bilevel positive airway pressure (BiPAP) ventilation, with declined forced vital capacity (0.73 L) and impaired negative inspiratory force (−41 cm H2O). Intravenous polyvalent immunoglobulin (1 g/kg, Day 42–46), plasma exchange (Days 54–61), and pyridostigmine (Day 49–65) were added, with no effect. Eventually she requested de-escalation to comfort care, and died peacefully after withdrawal of BiPAP support on Day 65.
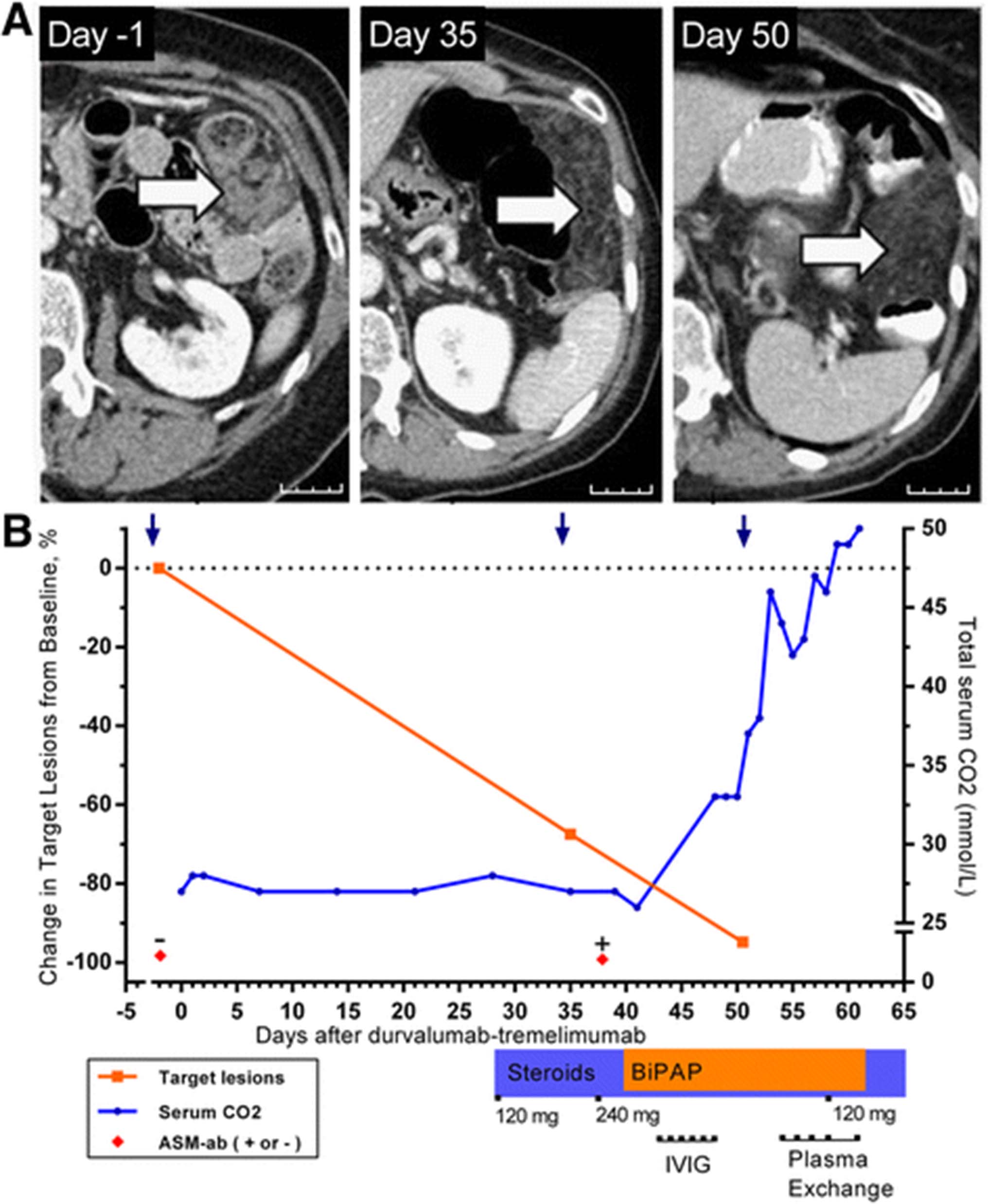
a Change in representative omental metastasis on CT scan after treatment with durvalumab- tremelimumab on Day 1. Arrows indicate omental metastasis replaced by fatty tissue. Scale bar indicates 25 mm. b Clinical course of patient until death from neuromuscular respiratory failure on Day 65. Serum CO2 retention is indicative of hypoventilation
Although the patient was initially suspected to have a drug-related myasthenia syndrome, consequent testing for acetylcholine receptor (AChR) immunoglobulin (IgG), voltage gated calcium channel (VGCC) IgG, and muscle-specific kinase protein (MuSK) IgG was negative. Anti-striated muscle (ASM) IgG was detected at a low titer of 1:40; it was not detected in archived pretreatment serum. Since the ASM IgG was only detectable at low titer, we could not conclude a diagnosis based solely upon the serology findings.
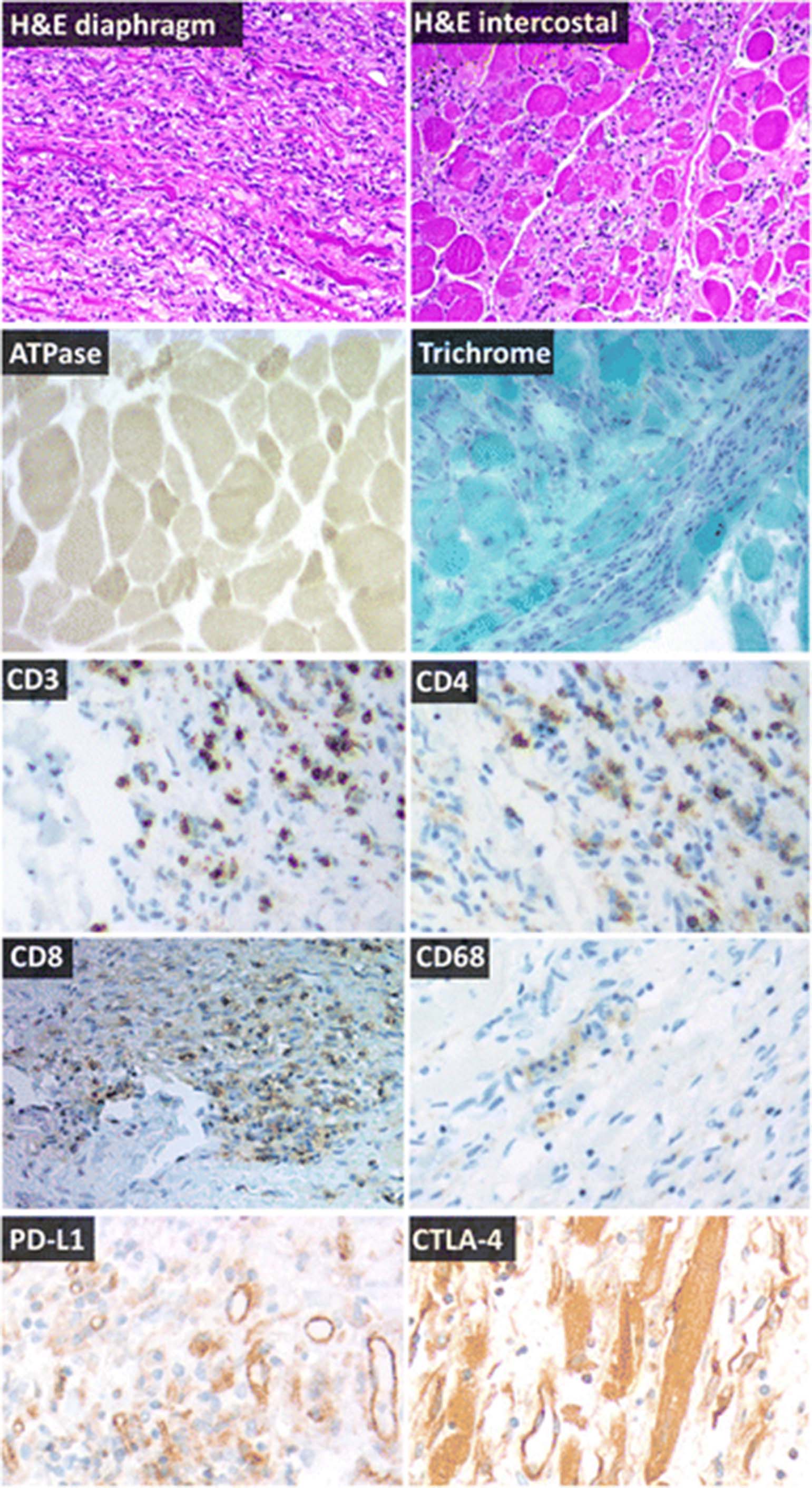
Upon autopsy, gross examination showed mild atrophy of the intercostal and diaphragm muscle. There was no evidence of interstitial lung disease. An additional file describes the methods used (Additional file 1) and controls used (Additional file 2). Microscopic examination of the inspiratory musculature showed an inflammatory mononuclear infiltrate most pronounced in the diaphragm, with only scattered preserved fibers (Fig. 2). Immunohistochemistry showed no increased lipid stores, and an attenuated mosaic pattern with type II fiber specific atrophy. Transactive response (TAR) DNA-binding protein 43 and trichrome evaluation were negative for inclusion bodies [9]. Mononuclear cells infiltrating the diaphragm and intercostal muscle consisted of a mixed phenotype of CD8+ and CD4+ lymphocytes. CD68+ macrophages were also observed in necrotic myofibers [10]. No residual metastases were identified on gross examination, indicating a complete pathological response to tremelimumab-durvalumab.
{kind=link}
{kind=link}
Representative immunohistochemistry of inspiratory muscles at autopsy, 66 days after tremelimumab-durvalumab treatment. Hematoxylin and eosin (H&E) sections show inflammatory myopathy in the diaphragm and intercostal muscles without rimmed vacuoles and without perifascicular atrophy, consistent with polymyositis. A mononuclear infiltrate is present which invades otherwise normal myofibers and completely effaces the background muscle fiber architecture in some areas. ATPase shows intense staining in small fibers compared to surrounding lighter, normal sized fibers in preserved areas of muscle, indicative of type II fiber atrophy. Trichrome shows mildly increased connective tissue, but shows no rimmed vacuoles, rods, or other inclusions. T cell co-receptor staining (CD3, CD4, CD8) revealed a mixed T-cell infiltrate which often completely effaced the myofascicular architecture. CD68 highlights necrotic myofibers scattered within the larger inflammatory infiltrate. PD-L1 expression was observed in blood vessels of dying muscle. Weak CTLA-4 expression was detected in necrotic myofibers. All images are 100× magnification
Discussion
As CTLA-4 and PD-1 axis inhibition becomes adopted for more cancer types, rare irAE presentations are becoming more common. Severe PM has been reported with monoclonal antibodies against both CTLA-4 and PD-1 (Table 1). This disease classically affects the proximal muscles and in severe cases, such as this one, is associated with dysarthria and dysphagia [11]. Although diaphragmatic PM has been previously reported [9], our case is prominent for its acute onset following immune-checkpoint inhibitor therapy.
Select cases of severe myositis associated with CTLA-4 and/or PD-1 axis inhibitors
The pathogenesis of idiopathic PM has intrinsic mechanistic overlap with the action of CTLA-4 blockade. Anti-CTLA-4 monoclonal antibody treatment increases IFN-γ production in draining lymph nodes [12], which may induce higher MHC class I expression on adjacent cells. Like the drug-related PM reported here, idiopathic PM is identified by disorganized muscle fibers of variable sizes coupled with endomysial T cell infiltrates [13]. CD8+ cells preferentially invade fibers which express MHC class I and trigger necrosis via the perforin pathway [4]. Although terminally differentiated, these CD8+ T cell infiltrates are predominantly CD28null [14]. In patients, this CD28null phenotype correlates with resistance to corticosteroid therapy [15]. Thus, aberrant B7-family receptor function appears to have a contributory role in idiopathic PM, not unlike the CTLA-4 drug-related PM described.
Targeting of muscle fiber by autoreactive T cells has been proposed as the pathogenesis of idiopathic PM [16]. Muscle-related antigens have been recognized in TCRs sequenced from idiopathic PM lesions [17], and a focused T cell repertoire is observed in these lesions [18]. Consistent with idiopathic PM, TCR sequencing of inflamed muscle in a nivolumab-related PM case revealed a clonally expanded T cell population in the muscle, as compared to either blood or tumor [19]. Like most irAEs associated with CTLA-4 or PD-1 inhibition, PM is also a recognized complication of up to 7.8% of allogeneic stem cell transplants, due to graft-versus-host disease (GvHD) [20]. It occurs after onset of hematopoietic full chimerism, and is associated with an increase in circulating CD8+ T cells. Muscle biopsy often reveals a mononuclear infiltrate of donor T cells and macrophages at endomysial sites, as in our case [21]. However, GvHD PM usually responds promptly to high-dose corticosteroids or cyclosporine [22].
The PD-1 axis is also implicated in the development of idiopathic myositis. Skeletal muscle cells normally express PD-L1, which induces T cell anergy. PD-L1 had a immunoprotective role against myositis in coculture experiments of MHC class I/II labeled myoblasts with CD4+ or CD8+ T cells [23]. Thus, PD-1 or PD-L1 monoclonal antibody may theoretically contribute to the autoimmune myositis cascade by attenuating the protection of skeletal muscle cells against autoreactive T cells [24].
The pathological findings in our case seem most indicative of PM, although a seronegative myasthenia overlap condition may also have been present. A Murine B6 model suggests that anti-CTLA-4 treatment stimulates AChR auto-antibody production and enhances the T cell response to provoke severe autoimmune myasthenia gravis [25]. Several cases of myasthenia gravis have been reported with ipilimumab [26, 27], as well as ipilimumab-nivolumab [28].
Optimal treatment of KRAS-mutant lung adenocarcinoma remains an emerging field. At present, therapy with PD-L1 axis blockade appears to be at least as effective in KRAS-mutant lung adenocarcinomas, compared to wild-type [29, 30]. Although KRAS point mutations do not appear to result in highly antigenic proteins, there has been preclinical success in inducing T-cell responses against Ras-associated epitopes [31]. In addition, TCRs reactive to the mutant KRASG12D peptide have been isolated within CD8+ TIL cultured from colon adenocarcinoma [32, 33]. Likewise, TCRs reactive to KRASG12D/G12V peptides have been isolated from immunized, HLA-specific transgenic mice [34]. Thus, adoptive cell transfer may be a viable treatment option for the proportion of KRAS-mutant patients who do not respond to PD-L1 / CTLA-4 blockade.
This study was conducted post-mortem, and is characterized by important limitations. Unfortunately, electromyography was not conducted. In addition, sufficient volumes of blood to determine the specific epitope of striated muscle protein were not collected, or determine the putative autoantigens involved. Absence of properly preserved PBMCs precluded lymphocyte reactivity testing. In addition, no blood samples suitable for creatine kinase measurement were collected. The ASM IgG was only weakly positive in our case, which is inconclusive as a standalone finding. Nonetheless, PM was unmistakable on pathologic examination.
Conclusion
PM remains a rare but important irAE associated with anti-CTLA-4 and PD-L1 combination therapy. The case reviewed in this report supports the hypothesis that muscle tissue is a target for lymphocytic infiltration in tremelimumab - durvalumab associated PM. Fatality was an unfortunate outcome in this case, perhaps tied in part to delayed recognition. In similar cases, prompt initiation of corticosteroids and additional measures have limited the severity of PM. Further insights into the autoimmune mechanism of PM will hopefully contribute to the prevention and treatment of this phenomenon.
Acknowledgments
This work has been supported in part by the Tissue Core Facility at the H. Lee Moffitt Cancer Center & Research Institute, an NCI designated Comprehensive Cancer Center (P30-CA076292). We gratefully acknowledge the patient and her family who consented for autopsy.
- AChR
- Acetylcholine receptor
- ASM
- Anti-striated muscle
- BiPAP
- Bilevel positive airway pressure
- CD
- Cluster of differentiation
- CO2
- Carbon dioxide level
- CSF
- Cerebrospinal fluid
- CT
- Computed tomography
- CTCAE
- Common toxicity criteria for adverse events
- CTLA-4
- Cytotoxic T-lymphocyte-associated protein 4
- GvHD
- Graft-versus-host disease
- H&E
- Hematoxylin and eosin
- HIER
- High pH heat induced epitope retrieval
- ICH –GCP
- International conference on harmonization good clinical practice
- IFN-γ
- Interferon gamma
- IHC
- Immunohistochemistry
- irAE
- Immune-related adverse events
- IV
- Intravenous
- IVIG
- Intravenous immunoglobulin G
- KRAS
- Kirsten rat sarcoma viral oncogene homolog
- MHC
- Major histocompatibility
- MRI
- Magnetic resonance imaging
- MuSK
- Muscle specific kinase protein
- NCT
- National clinical trials
- PBMCs
- Peripheral blood mononuclear cells
- PD-1
- Programmed cell death protein 1
- PD-L1
- Programmed death ligand 1
- Pex
- Plasma exchange
- PM
- Polymyositis
- RECIST
- Response evaluation criteria in solid tumor
- TAR DP-43
- Transactive response DNA binding protein 43 kDa
- TCR
- T cell receptor
- VGCC
- Voltage gated calcium channel
- wks
- Weeks
References
Footnotes
Funding Correlative studies were supported by 2013 Conquer Cancer Foundation Young Investigator Award (to BCC), NCI P50 CA119997 (to SJA). The funding organizations had no direct role in the preparation, review, or approval of the manuscript.
Authors’ contributions SJ collected and assembled data into a rough draft, including figures. SJA treated the patient and conceived of the study. TAR interpreted and contributed the CT scan figure. RPS and BAC carried out autopsy study and immunohistochemistry, including microscopy photographs. ASW provided specialized immunohistochemistry, including microscopy photographs. BCC designed the report, provided financial support, and revised the manuscript. All authors read and approved the final manuscript.
Competing interests The authors BCC and SJA have served as a paid consultant and/or received honoraria from AstraZeneca Pharmaceuticals. The remaining authors have no potential competing interests to disclose.
Consent for publication Written informed consent was obtained from the patient for publication of their individual details and accompanying images. The consent form is held by the authors’ institution in the patient clinical notes.
Ethics approval and consent to participate Yes, the subject described provided written informed consent. Approved by Liberty IRB; IRB00003411.
Publisher’s Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material The online version of this article (doi:10.1186/s40425-017-0258-x) contains supplementary material, which is available to authorized users.