Article Text

Abstract
Recent randomized phase III trials (KEYNOTE-407 and IMpower131) reported that adding anti-programmed death (ligand) 1 (anti-PD-(L)1) antibodies in combination with taxane-platinum improve the therapeutic efficacy for advanced squamous non-small-cell lung cancer (NSCLC). However, there is no head-to-head comparison of pembrolizumab (anti-PD-1) plus chemotherapy vs. atezolizumab (anti-PD-L1) plus chemotherapy. Therefore, we performed an indirect comparison to explore the optimal choice of anti-PD-(L)1 treatment for advanced squamous NSCLC in combination with chemotherapy. The clinical outcomes were overall survival (OS), progression-free survival (PFS), objective response rate (ORR) and adverse event (AE). For overall patients, pembrolizumab had significantly superior OS (hazard ratio (HR) with 95% confidence interval, 0.67, 0.47–0.94; P = 0.02) and numerically better PFS (HR, 0.79, 0.60–1.04; P = 0.10) than atezolizumab, while they had similar ORR, all cause AE and grade 3–5 AE. For PD-L1 high patients, pembrolizumab and atezolizumab showed similar OS and PFS. However, for PD-L1 low/negative patients, pembrolizumab had superior OS (HR, 0.43, 0.24–0.76; P < 0.01/ HR, 0.74, 0.40–1.38; P = 0.35) and better PFS (HR, 0.80, 0.51–1.26; P = 0.33/ HR, 0.46, 0.28–0.75; P <0.01) than atezolizumab. Our analysis raises the hypothesis that anti-PD-1 antibody therapy in combination with chemotherapy may have superior efficacy compared to anti-PD-L1 antibody combination for patients with PD-L1 low/negative advanced squamous NSCLC.
- NSCLC
- Squamous
- Anti-PD-1
- Anti-PD-L1
- Pembrolizumab
- Atezolizumab
Yaxiong Zhang and Huaqiang Zhou contributed equally to this work.
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Statistics from Altmetric.com
Yaxiong Zhang and Huaqiang Zhou contributed equally to this work.
Background
Adenocarcinoma and squamous carcinoma are two most common histological subtype of advanced non-small-cell lung cancer (NSCLC). Patients with lung adenocarcinoma whose tumor harbor specific gene mutations, such as epidermal growth factor receptor (EGFR) mutation or anaplastic lymphoma kinase (ALK) fusion, derive significant benefit from targeted agents, tyrosine kinase inhibitors (TKIs), and have better prognosis [1]. However, this advancement has not been achieved in squamous NSCLC given the lack of efficacy and there are currently no approved targeted agents for squamous NSCLC [1]. The standard treatment for advanced squamous NSCLC includes platinum-based doublet chemotherapy, such as taxane-platinum combination, which has poor efficacy [2]. Therefore, we still need to explore a better therapeutic regimen for advanced squamous NSCLC. Recently, a randomized phase III trial (KEYNOTE-407) reported that adding pembrolizumab, an anti-programmed death 1 (anti-PD-1) antibody, in combination with carboplatin plus paclitaxel/nab-paclitaxel decreases the mortality risk for advanced squamous NSCLC [3]. Meanwhile, another randomized phase III study (IMpower131) showed that combined carboplatin plus nab-paclitaxel with atezolizumab, an anti-programmed death ligand 1 (anti-PD-L1) antibody, also improved the therapeutic efficacy for those patients [4]. However, there is no head-to-head comparison of pembrolizumab plus chemotherapy vs. atezolizumab plus chemotherapy. Therefore, we performed an indirect comparison of KEYNOTE-407 and IMpower131 to explore the optimal choice of anti-PD-(L)1 treatment for advanced squamous NSCLC in combination with chemotherapy.
Methods
The clinical outcomes for our study were overall survival (OS), progression-free survival (PFS), objective response rate (ORR) and adverse event (AE). Data of OS and PFS were extracted as hazard ratio (HR) and its 95% confidence interval (CI), while data of ORR and AE were extracted as risk ratio (RR) and its 95% CI. All of above data were derived from KEYNOTE-407 and IMpower131. HR and RR represented pembrolizumab vs. atezolizumab. Based on the assumption that there is no significant treatment efficacy of carboplatin plus paclitaxel in comparison to carboplatin plus nab-paclitaxel for advanced squamous NSCLC, [5] we calculated the adjusted indirect comparison using the following formulas as previously described [6]. The log HR of the adjusted indirect comparison for arm A (pembrolizumab plus chemotherapy) vs. arm B (atezolizumab plus chemotherapy) was linked by arm C (chemotherapy), which was estimated by log HR
AB = log HR
AC − log HR
BC, and its standard error (SE) for the log HR was  . RR was evaluated similarly as above formulas. HR <1 or RR> 1 standed for pembrolizumab had longer PFS/OS or better ORR/less AE than atezolizumab incombination with chemotherapy. A statistical test with P-value≤0.05 was considered as significant.
. RR was evaluated similarly as above formulas. HR <1 or RR> 1 standed for pembrolizumab had longer PFS/OS or better ORR/less AE than atezolizumab incombination with chemotherapy. A statistical test with P-value≤0.05 was considered as significant.
Results
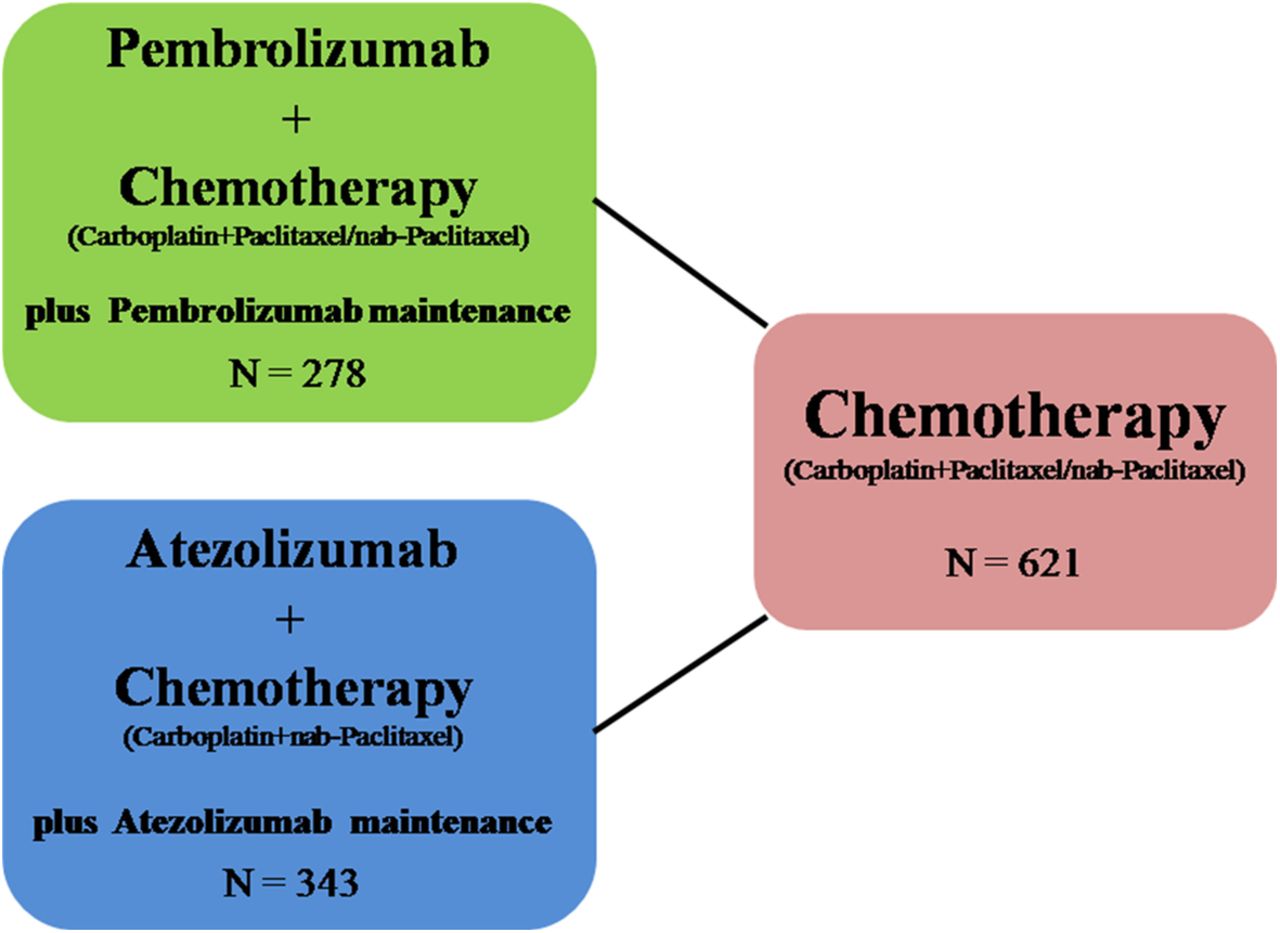
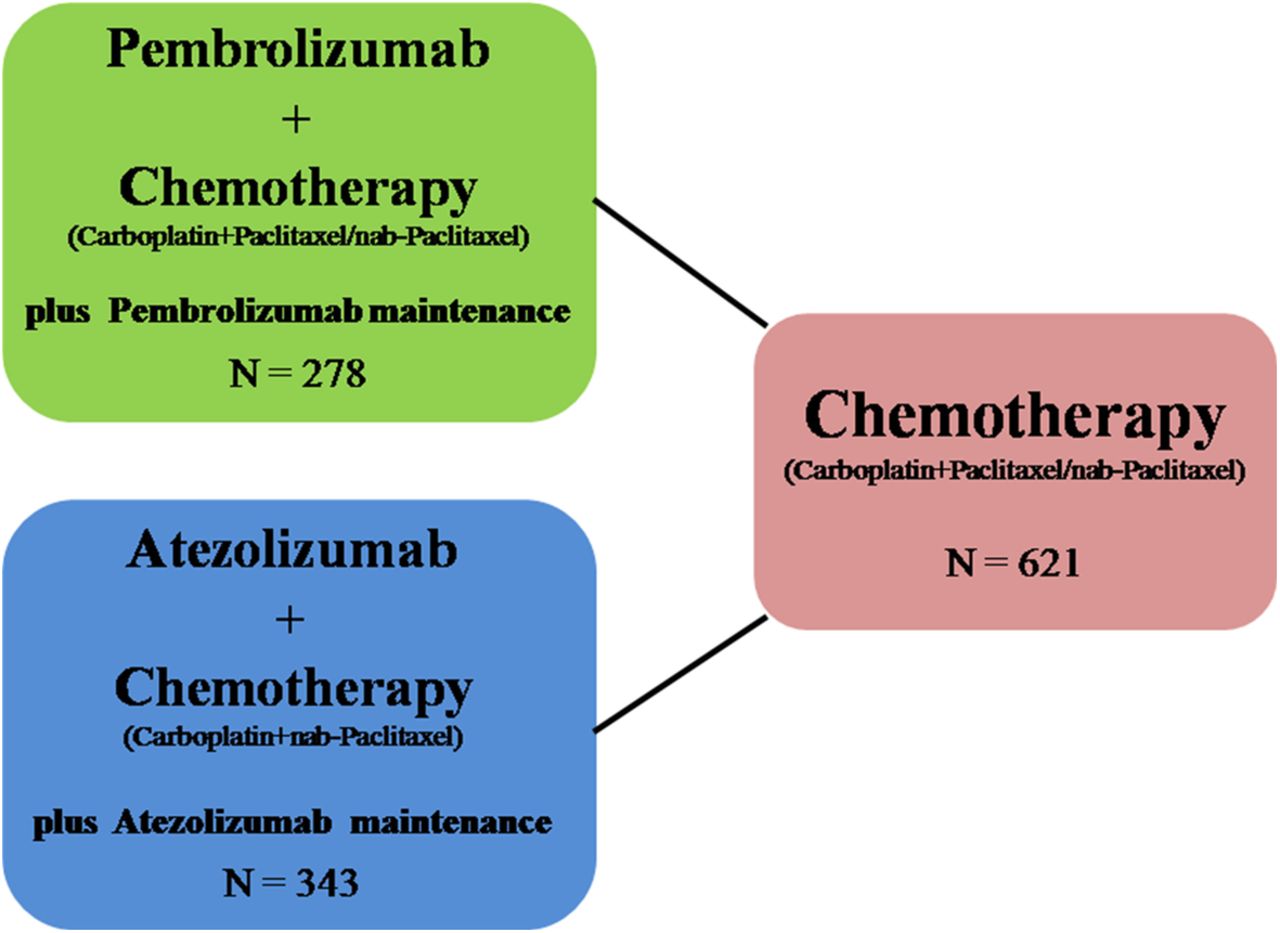
Table 1 summarized study design, baseline characteristics and available endpoints of the trials in detail. We compared therapeutic efficacy and AE between pembrolizumab (N = 278) and atezolizumab (N = 343) in combination with chemotherapy as the first-line treatment of advanced squamous NSCLC (Fig. 1). The HR, RR and CI in the result part were calculated from our analysis and not from the above trials. For overall patients, pembrolizumab had significantly superior OS (HR, 0.67; 95% CI, 0.47–0.94; P = 0.02) and numerically better PFS (HR, 0.79; 95% CI, 0.60–1.04; P = 0.10) than atezolizumab, while they had similar ORR, all cause AE and grade 3–5 AE (Table 2). For PD-L1 high patients, pembrolizumab and atezolizumab showed similar OS and PFS, while pembrolizumab had significantly superior OS (HR, 0.43; 95% CI, 0.24–0.76; P <0.01) and numerically better PFS (HR, 0.80; 95% CI, 0.51–1.26; P = 0.33) than atezolizumab for PD-L1 low patients. Furthermore, pembrolizumab showed significantly longer PFS (HR, 0.46; 95% CI, 0.28–0.75; P <0.01) compared with atezolizumab for PD-L1 negative patients (Table 2).
Baseline characteristics and available endpoints about the trials of KEYNOTE-407 and IMpower 131
{kind=link}
Diagram of the indirect comparison between pembrolizumab plus chemotherapy vs. atezolizumab plus chemotherapy for advanced squamous non-small-cell lung cancer. Solid lines between treatment regimens represented the existence of direct comparisons. N = enrolled patient number
Indirect comparison of pembrolizumab plus chemotherapy vs. atezolizumab plus chemotherapy for advanced squamous non-small-cell lung cancer
Discussion
According to this indirect comparison, we found pembrolizumab plus chemotherapy seemed to be superior in terms of OS and PFS compared to atezolizumab plus chemotherapy, most notable in PD-L1 low/negative subgroup of patients. Not surprisingly, both of pembrolizumab and atezolizumab showed similar efficacy in PD-L1 high patients. Theoretically, PD-1 antibody can bind to PD-1 protein on T cells, so it will block the binding of PD-1 to PD-L1 and PD-L2 at the same time, while PD-L1 antibody can only interact with PD-L1, so it will only block the binding of PD-1 to PD-L1. Therefore, T cells might still be inhibited by the interaction between PD-1 and PD-L2 using anti-PD-L1 treatment [7]. For PD-L1 high patients, Anti-PD-L1 and Anti-PD-1 treatment might be effective similarly, because PD-L1 expression might be dominant for those patients. However, for PD-L1 low/negative patients, the expression spectrum of immunological molecule might be complicated, such as PD-L2 expression enhancement. As a result, Anti-PD-L1 treatment might not be enough compared with Anti-PD-1 treatment for PD-L1 low/negative patients.
The major limitation of this study was the limited follow-up time for KEYNOTE-407 and IMpower131, so that we used relative variables (HR and RR) instead of absolute value (median survival time) for analyses to lower the bias. Besides, the proportion of PD-L1 high patients was slightly higher in KEYNOTE-407, while the proportion of PD-L1 negative patients was slightly higher in IMpower131, both in experimental group and control group. It might cause imbalance of the patient population which affected the comparability of this indirect comparison. Moreover, PD-L1 expression was scored by SP142 assay in IMpower131, while it was scored by 22C3 assay in KEYNOTE-407, thus might have influence on PD-L1 level evaluation. Recent studies demonstrated the percentage of PD-L1-stained tumor cells was highly comparable among 22C3, 28–8 and SP263 PD-L1 assays, while SP142 assay exhibited fewer stained tumor cells, [8, 9] which was in accordance with the proportion of PD-L1 level population in KEYNOTE-407 (higher PD-L1 high patients) and IMpower131 (higher PD-L1 negative patients). To some extent, it proved that the overall patient population between KEYNOTE-407 and IMpower131 was comparable. But it should still be cautious to interpret the subgroup analysis stratified by PD-L1 level. After all, our study was an indirect comparison analysis, which might compromise the evidence level.
Conclusions
These limitations aside, our study firstly compared pembrolizumab plus chemotherapy and atezolizumab plus chemotherapy for advanced squamous NSCLC and found the former seemed to be superior in terms of OS and PFS than the latter, especially in PD-L1 low/negative patients. Our analysis provides a hint that anti-PD-1 antibody might have superior efficacy compared to anti-PD-L1 antibody in combination with chemotherapy for patients with PD-L1 low/negative advanced squamous NSCLC. Additional studies are warranted to confirm this.
Acknowledgments
This work was supported by the National Key R&D Program of China (Grant No. 2016YFC0905500, 2016YFC0905503).
Authors’ contributions
YZ and LZ concept and design this study. YZ and HZ make the data and statistical analysis. All authors write the manuscript. All authors read and approved the final manuscript.
Notes
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.