Article Text

Abstract
Immunotherapy is among the most rapidly evolving treatment strategies in oncology. The therapeutic potential of immune-checkpoint inhibitors is exemplified by the recent hail of Food and Drug Administration (FDA) approvals for their use in various malignancies. Continued efforts to enhance outcomes with immunotherapy agents have led to the formulation of advanced treatment strategies. Recent evidence from pre-clinical studies evaluating immune-checkpoint inhibitors in various cancer cell-lines has suggested that combinatorial approaches may have superior survival outcomes compared to single-agent immunotherapy regimens. Preliminary trials assessing combination therapy with anti-PD-1/PD-L1 plus anti-CTLA-4 immune-checkpoint inhibitors have documented considerable advantages in survival indices over single-agent immunotherapy. The therapeutic potential of combinatorial approaches is highlighted by the recent FDA approval of nivolumab plus ipilimumab for patients with advanced melanoma. Presently, dual-immune checkpoint inhibition with anti-programmed death receptor-1/programmed cell death receptor- ligand-1 (anti-PD-1/PD-L1) plus anti-cytotoxic T lymphocyte associated antigen-4 (anti-CTLA-4) monoclonal antibodies (MoAbs) is being evaluated for a wide range of tumor histologies. Furthermore, several ongoing clinical trials are investigating combination checkpoint inhibition in association with traditional treatment modalities such as chemotherapy, surgery, and radiation. In this review, we summarize the current landscape of combination therapy with anti-PD-1/PD-L1 plus anti-CTLA-4 MoAbs for patients with melanoma and non-small cell lung cancer (NSCLC). We present a synopsis of the prospects for expanding the indications of dual immune-checkpoint inhibition therapy to a more diverse set of tumor histologies.
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Statistics from Altmetric.com
Background
The regulation of immune responses through MoAbs is a ground-breaking therapeutic strategy in oncology. Based on substantial pre-clinical and clinical evidence, several immunotherapy agents have received approval by the FDA as standard of care treatment for various malignancies over the past two decades [1, 2]. However, with increasing experience in the use of immunotherapy agents in clinical settings, several limitations, such as treatment resistance and undesired immunogenicity, have been observed [3, 4]. Extensive efforts have been made to meet such challenges, and novel immune checkpoints are being tested and are expected to pave the way for the next generation of immunotherapy agents [5].
The fundamental goal in advancing anti-cancer immunotherapy is to improve clinical outcomes. The use of combination checkpoint inhibition is being applied to meet this goal. This approach intends to exploit the distinct mechanisms of immunomodulation of two MoAbs in a single treatment regimen. Recent evidence suggests that the combined use of an anti-CTLA-4 immune-checkpoint inhibitor with an anti-PD-1/PD-L1 MoAb may have complementary action, thus yielding a higher clinical efficacy than either agent individually [6, 7]. Comprehensive data on the efficacy of MoAb combination therapy in clinical settings is warranted in order to ascertain the true therapeutic value of this treatment strategy.
Presently, combination checkpoint inhibition is being extensively evaluated for potential clinical benefit in a large number of tumor histologies. Due to positive outcomes in preliminary trials, nivolumab (IgG4 anti-PD-1 MoAb) plus ipilimumab (fully humanized IgG1 anti-CTLA-4 MoAb) is one of the most enthusiastically investigated combined immunotherapy regimens, with over 100 clinical trials in various stages [8, 9]. Of note, nivolumab plus ipilimumab received approval for use in BRAF V600 wild-type metastatic/unresectable melanoma, making it the first combination checkpoint inhibition regimen to be approved by the FDA [9]. In addition, other PD-1/PD-L1 inhibitors plus CTLA-4 inhibitor combination checkpoint inhibition regimens that are presently in clinical trials include atezolizumab (anti-PD-L1 MoAb) plus ipilimumab, pembrolizumab (IgG4 anti-PD-1 MoAb) plus ipilimumab, and tremelimumab (IgG2 anti-CTLA-4 MoAb) plus durvalumab (Fc optimized anti-PD-L1 MoAb) [10]. The data published from these trials will be crucial to appraise the efficacy of combination immune checkpoint inhibitor regimens in varying clinical scenarios.
In this review, we describe the rationale for combined immunotherapy with PD-1/PD-L1 plus CTLA-4 checkpoint inhibitors. Building on what we have learned through studies of combination checkpoint inhibition in patients with melanoma and NSCLC, we shall also critically assess the current landscape and future prospects for the development of an ideal combination checkpoint inhibition regimen.
Role of PD-1/PD-L1 and CTLA-4 in modulation of anti-tumor T-cell activity
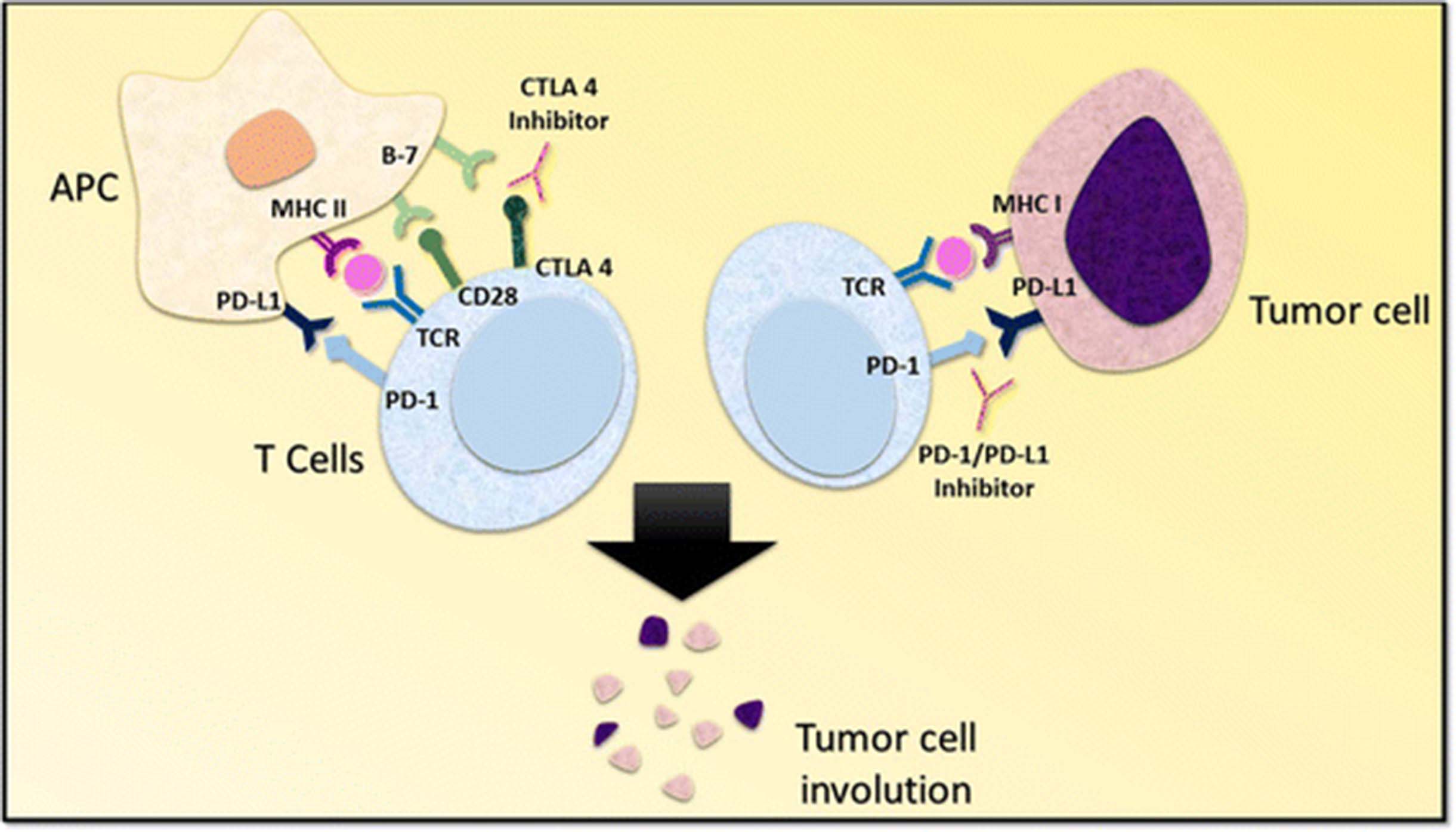
The process of T cell activation requires two signals. The primary signal comes from the binding of the T cell receptor (TCR) to the major histocompatibility complex (MHC) molecule presented by an antigen presenting cell (APC) [11]. The costimulatory signal may arise from one of several distinct T cell-APC interactions. One such pathway is the engagement of CD28 on T cells with CD80 (B7–1) or CD86 (B7–2) on APCs [11] (Fig. 1). T-cell activity can be modulated by regulating the generation of costimulatory signals through various mechanisms.

Mechanism of CTLA 4 and PD-1/PD-L1 inhibition. The activation of T cells is mediated by the interaction of T cell receptor and the CD28 receptor with class II major histocompatibility complex and B7 co-stimulatory molecule located on the antigen presenting cells. The interaction of CTLA-4 with the B7 molecule delivers an inhibitory signal, effectively checked by CTLA-4 inhibitors. On the other hand, the negative regulation of T cells resulting from PD-1/PD-L1 interaction between T cells and tumor cells is prevented by PD-1/PD-L1 inhibitors. Abbreviations: APC, antigen presenting cell; PD-1, programmed death receptor-1; PD-L1, programmed cell death receptor ligand-1; TCR, T cell receptor; MHC I, major histocompatibility complex class I; MHC II, major histocompatibility complex class II
Several signaling pathways have been implicated in the modulation of T cell activity. The CTLA-4 molecule is a homolog of CD28 and is expressed by T cells (Fig. 1) [12, 13]. The influence of CTLA-4 on T cell activity primarily occurs in the priming phase of T cell activation [14]. CTLA-4 competitively binds to B7 on APCs and inhibits the costimulatory signal that arises from the engagement of CD28 with B7, thereby diminishing the T cell immune response [13, 15–18]. The upregulation of CTLA-4 expression on CD8+ and CD4+ T cells precludes stimulatory signaling from CD28-B7 binding and TCR-MHC binding [11, 19]. On the other hand, regulatory T cells (Treg cells) exhibit constitutive expression of CTLA-4 [20]. Murine models bearing Treg cells deficient in CTLA-4 exhibited attenuated immunosuppressive activity, thus highlighting the significance of CTLA-4 in regulating immunological self-tolerance [20].
The PD-1 molecule is akin to CTLA-4. It is a member of the B7-CD28 family and is expressed by myeloid derived cells, B cells, and T cells [21, 22]. PD-1 has two corresponding ligands, PD-L1 and PD-L2 [14]. PD-L1 is expressed by a diverse set of cells including hematopoietic cells, leucocytes, parenchymal cells, and tumor cells, whereas PD-L2 is expressed by dendritic cells and macrophages [22–24]. The PD-1 receptor on T cells binds PD-L1 expressed by APCs and inhibits pro-inflammatory events such as T cell proliferation and cytokine production (Fig. 1) [14, 25]. Of note, recent evidence has suggested that PD-1/PD-L1 interactions facilitate immune escape by tumor cells [24, 26]. This phenomenon has been attributed to PD-1/PD-L1 mediated induction of anergy and apoptosis of activated T cells, tumor resistance to the cytotoxic T cell response, and differentiation of CD4+ T cells into Fox3p + CD4+ Treg cells [27–29].
An intricate knowledge of various pathways regulating T cell-APC interactions has been central to identifying the points of intervention that allow us to modulate host immune responses. The aforementioned evidence and other studies with similar outcomes prompted the development of PD-1/PD-L1 and CTLA-4 checkpoint inhibitors for potential application in anti-cancer therapy.
Preclinical rationale for combination checkpoint inhibition
Combination immunotherapy with PD-1/PD-L1 plus CTLA-4 checkpoint inhibitors has been studied in multiple cancer cell lines. In an experiment on murine preclinical models, vaccination with B16-Flt-3 ligand (Fvax) along with the use of CTLA-4 antibody promoted tumor rejection in 10% of mice with pre-implanted B16-BL6 melanoma [7]. Fvax plus PD-1 blockade exhibited tumor rejection in 25% of mice. The combined use of CTLA-4 and PD-1 checkpoint inhibitors resulted in the rejection of B16-BL6 melanoma in 50% of test animals. Upon the addition of a PD-L1 inhibitor to the above, 65% of test animals exhibited rejection of melanoma. The outcomes observed with combined PD-1 and CTLA-4 blockade were found to correlate with an increase in CD4+ effector T cell (CD4+ Teff) to Treg cell ratio and CD8+ T cell to Treg cell ratio in tumor tissue. Another significant observation was that a high percentage of T cells positive for CTLA-4 and PD-1 that would have undergone anergy remained active with combined PD-1 plus CTLA-4 blockade [7].
Similar findings were documented in another study investigating the effects of checkpoint inhibition (PD-1/PD-L1 and CTLA-4) in murine models of ovarian (ID8-VEGF) and colonic carcinoma (CT26) [30]. For ID8-VEGF, tumor regression was observed in 25% of test animals after PD-1 blockade, 25% with CTLA-4 blockade, and 37.5% with PD-L1 blockade, as compared to 50% with combined CTLA-4 plus PD-1 or PD-L1 blockade. Likewise, in mice bearing CT26, tumor regression was observed in 25% of test animals with PD-1 blockade, 50% with CTLA-4 blockade, and 33% with PD-L1 blockade, as compared to 75% (p < 0.01 for the combination to checkpoint inhibitor monotherapy comparison) with combined CTLA-4 plus PD-1 or PD-L1 blockade. Combined therapy with CTLA-4 and PD-1 blockade was associated with a greater enhancement in tumor induced lymphocyte (TIL) activity and proliferation similar to CTLA-4 or PD-1 blockade alone [30]. Combination therapy also decreased the frequency of Treg cells and functional markers of activated Treg cells such as glucocorticoid induced tumor necrosis factor receptor (GITR) [30]. This suggested that dual checkpoint inhibition simultaneously blunted the function and decreased the number of Treg cells.
In view of these and other preclinical studies, it was established that combined immune checkpoint blockade decreases suppression of the host immune system, while promoting inflammation in the tumor microenvironment. Moreover, the vast amount of preclinical data also suggested that the anti-tumor activity of combination therapy with CTLA-4 plus PD-1/PD-L1 checkpoint inhibitors may have superior outcomes compared to CTLA-4 or PD-1 monotherapy. It was thus prudent to investigate the therapeutic potential of CTLA-4 plus PD-1/PD-L1 checkpoint inhibitors in clinical settings.
Emergence of combination checkpoint inhibition
Cancer immunosurveillance has been considered one of the primary natural mechanisms of defense against aberrant cell populations [31, 32]. Immune cells recognize and eliminate transformed cells through various cellular interactions [33]. In addition, the immune system is also involved in shaping tumor immunogenicity, a phenomenon theorized as immunoediting [34]. However, it was observed that cancer cells gradually undergo immune selection that disrupts the equilibrium with immune cells, consequently generating a tumor cell population that effectively evades immune surveillance [35–38]. Furthermore, alterations in the tumor microenvironment have also been reported to mediate immune escape [39]. It was thus theorized that therapeutic agents with the ability to restore immune surveillance or prevent immune escape of tumor cell populations could potentially have a significant impact in clinical oncology.
The knowledge of various factors that influence tumorigenesis has been exploited for developing a wide range of immunotherapy agents. Immunogenic cell death inducers, immunostimulatory cytokines, pattern recognition receptor agonists (PRR agonists), and tumor targeting antibodies have benefitted cancer patients for nearly two decades [40]. Numerous immunotherapy agents have received FDA approval for use as monotherapy in a variety of tumor histologies. For instance, nivolumab has been approved for patients with melanoma, renal cell carcinoma (RCC), metastatic squamous cell carcinoma of the head and neck (SCCHN), classical Hodgkin’s lymphoma (HL) and advanced lung cancer [41–46]. Pembrolizumab, another anti-PD-1 MoAb, is approved for use in patients with SCCHN, NSCLC, and melanoma [47–49]. Likewise, atezolizumab is approved for patients with NSCLC and urothelial carcinoma [50–52]. However, any further enhancements in clinical benefit beyond checkpoint inhibitor monotherapy are still in clinical trials.
Recent clinical trial data comparing combination therapy with nivolumab and ipilimumab versus ipilimumab monotherapy in treatment naïve melanoma patients drew much attention (CheckMate 069, NCT01927419). In patients with BRAF-wild type melanoma, the investigators reported an objective response of 61% (95% CI: 49–72) as opposed to 11% (95% CI: 3–25) with combination checkpoint inhibition and ipilimumab monotherapy, respectively [53]. Furthermore, 22% of study participants receiving combination therapy exhibited a complete response, as compared to none among those receiving ipilimumab monotherapy [53]. In view of these findings, combined therapy with nivolumab and ipilimumab in melanoma patients became the first FDA approved (accelerated approval) indication for combination checkpoint inhibition. Furthermore, this study prompted comprehensive efforts to explore the application of combined immunotherapy with anti-PD-1/PD-L1 and anti-CTLA-4 MoAbs for patients with various malignancies.
Currently there are a large number of clinical trials evaluating several PD-1/PD-L1 plus CTLA-4 checkpoint inhibitor combination regimens. Positive outcomes in preliminary trials have made way for more intensive efforts to explore the full potential of combination checkpoint inhibition regimens, particularly nivolumab plus ipilimumab. It is widely anticipated that the ongoing trials will provide formidable evidence to support clinical applications of PD-1/PD-L1 plus CTLA-4 checkpoint inhibitor combination regimens for patients with a substantial variety of tumor histologies.
Methods
The details of pertinent clinical trials were gathered from clinicaltrials.gov (United States National Institute of Health) from the database available to public domain. The database was narrowed using the search queries “nivolumab” with “ipilimumab”, “pembrolizumab” with “ipilimumab”, “atezolizumab” with “ipilimumab” and “tremelimumab” with “durvalumab”. All prospective clinical trials using aforementioned immunotherapy agents as treatment intervention in NSCLC or melanoma patients were selected from the filtered results. Additionally, all phase 1 solid tumor trials aimed at providing a recommendation for the appropriate phase 2 dose of above combinations were also selected. The NCT number of each trial was used to search for published results on online databases including PubMed, American Association of Cancer Research (AACR), American Society of Clinical Oncology (ASCO) and European Society for Medical Oncology (ESMO).
Clinical trials: Current landscape
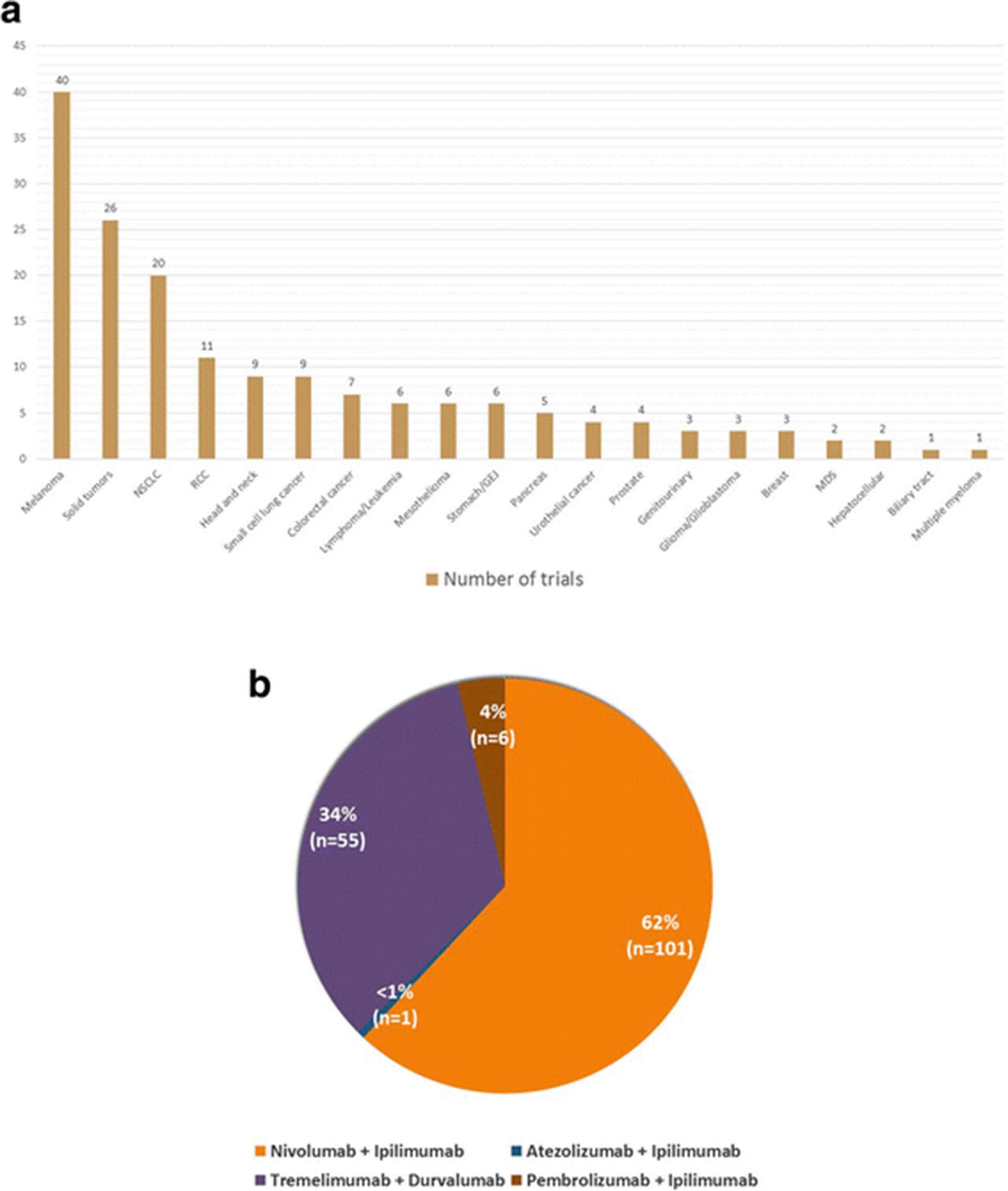
The United States National Institutes of Health lists a total of 44 ongoing clinical trials (clinicaltrials.gov) evaluating combined immunotherapy with anti-PD-1/PD-L1 plus anti-CTLA-4 MoAbs for patients with NSCLC and melanoma (Tables 1 and 2, Fig. 2a). The designated combination therapy regimens include nivolumab plus ipilimumab, pembrolizumab plus ipilimumab, atezolizumab plus ipilimumab, and tremelimumab plus durvalumab. A majority of these trials focus on survival and other treatment response indices, whereas a limited number of trials are investigating the safety profile and maximum tolerable dose (MTD) of combination therapy protocols. Furthermore, eight phase 1/phase 2 clinical trials are in the process of enrolling participants with solid tumors in order to determine recommended phase 2 doses (RP2D) for combination checkpoint inhibitor therapy with various anti-PD-1/PD-L1 and anti-CTLA-4 MoAbs. Of note, over three quarters (37 of 44 trials) of ongoing combination therapy trials for patients with NSCLC and melanoma are investigating treatment regimens that involve the application of nivolumab and ipilimumab (Fig. 2a and b).
Melanoma trials evaluating combination checkpoint inhibition with anti-CTLA-4 plus anti- PD-1/PD-L1 monoclonal antibodies
NSCLC trials evaluating combination checkpoint inhibition with anti-CTLA-4 plus anti- PD-1/PD-L1 monoclonal antibodies

Current landscape of combination immunotherapy trials for various tumor histologies. a Number of combination checkpoint inhibition trials for various tumor histologies. Abbreviations: NSCLC, non-small cell lung carcinoma; RCC, renal cell carcinoma; GEJ, gastro-esophageal junction; MDS, myelodysplastic syndrome. b Landscape of combination checkpoint inhibition agents. Legend: The figure elaborates relative number of trials for four combinations of immunotherapy agents. Nivolumab plus ipilimumab: 62% (101 trials), pembrolizumab plus ipilimumab 4% (6 trials), tremelimumab plus durvalumab 34% (55 trials) and atezolizumab plus ipilimumab < 1% (1 trial)
Combination checkpoint inhibition trials in melanoma
Massive efforts are testing dual checkpoint inhibition with anti-PD-1/PD-L1 plus anti-CTLA-4 MoAbs in patients with melanoma. Presently, there are 28 clinical trials in various phases committed to this objective (Table 1). Currently, only one trial is in the process of recruiting participants that will receive ipilimumab in combination with pembrolizumab. Approximately two-thirds of all ongoing trials (18 of 28 trials) in melanoma patients are investigating combined therapy with nivolumab plus ipilimumab.
Several distinct methodologies for the combined use of nivolumab and ipilimumab have been identified and are presently being investigated for potential clinical benefit in two trials. One trial will compare the incidence of adverse events, overall response rate (ORR), and progression free survival (PFS) with concurrent versus sequential administration of nivolumab and ipilimumab in the induction phase (NCT02905266). Another trial, CheckMate 064, will evaluate the duration of response, response rate (RR), rate of progression and the proportion of study participants that develop grade 3–5 adverse events when using nivolumab prior to ipilimumab versus ipilimumab prior to nivolumab in the induction phase (NCT01783938).
Treatment protocols in five trials involve the integrated use of nivolumab and/or ipilimumab with additional anti-cancer agents. The assessment of MTD and ORR for combined therapy with nivolumab plus ipilimumab and ACY241 (histone deacetylase {HDAC} inhibitor) will be performed in one trial (NCT02935790) [10]. Another trial will be exploring the clinical efficacy and incidence of adverse events for nivolumab plus TAK580 (pan-Raf kinase inhibitor), nivolumab and plozalizumab (chemokine receptor-2 {anti-CCR-2} MoAb), and the combined use of nivolumab plus ipilimumab and vedolizumab (anti-LPAM-1/α4β7 MoAb), each in separate arms (NCT02723006) [10]. Similarly, a different trial will evaluate the safety profile and clinical efficacy with combination dabrafenib (BRAF protein inhibitor) and/or trametinib (MEK MAPK/ERK kinase {mitogen-activated protein kinase kinase} inhibitor) in the induction phase, followed by ipilimumab and/or nivolumab (NCT01940809) [10]. This trial will also compare the outcomes of the above treatment regimens with nivolumab plus ipilimumab (NCT01940809). The SECOMBIT study will compare survival outcomes among several variations of treatment regimens composed of binimetinib (MEK1/2 inhibitor), encorafenib (Raf kinase inhibitor), nivolumab and ipilimumab (NCT02631447) [10]. Lastly, one trial will analyze response to vemurafenib (BRAF-V600 kinase inhibitor) plus cobimetinib (MAP2K1/MEK1 inhibitor) in the induction phase followed by nivolumab plus ipilimumab, versus nivolumab plus ipilimumab combination therapy alone (NCT02968303) [10].
Several additional treatment modalities with nivolumab plus ipilimumab combination therapy for melanoma is being examined in three trials. Neoadjuvant therapy with nivolumab and combined nivolumab plus ipilimumab is under evaluation in NCT02519322 and NCT02977052, respectively. A different trial will assess the use of Yttrium-90 selective internal hepatic radiation prior to induction with nivolumab plus ipilimumab (NCT02913417).
The safety and survival statistics from five clinical trials that applied combined immunotherapy with various anti-PD-1/PD-L1 plus anti-CTLA-4 MoAbs has been made available. One trial enrolled 136 patients with unresectable stage III/IV malignant melanoma in eight cohorts (NCT01024231). Each cohort received a unique regimen, differing in sequence of administration and dosing for nivolumab and ipilimumab. The doses for nivolumab were 1, 3, or 10 mg/kg whereas ipilimumab was administered at 3 or 10 mg/kg, per predefined criteria for each cohort. The study documented a considerable variation in OS among different cohorts. In one group, among 14 patients that received nivolumab 0.3 mg/kg plus ipilimumab 3 mg/kg, the 1 year OS rate was 56%, whereas among six patients receiving nivolumab 3 mg/kg plus ipilimumab 3 mg/kg the 1 year OS rate was 100% [54]. Another parameter compared in this study was median OS for concurrent and sequential administration of nivolumab and ipilimumab, which was noted to be 39.7 months and 13.0 months, respectively. The study also recorded objective response stratified on the basis of PD-L1 status. In patients with PD-L1 positive melanoma, an objective response was noted in 6 of 13 participants receiving concurrent therapy and 4 of 8 participants receiving sequential therapy. In the PD-L1 negative subgroup 9 of 22 patients responded with concurrent therapy and 1 of 13 patients receiving sequential therapy responded. Treatment related adverse events were noted in 93% (grade 3–4 adverse events: 53%) patients receiving the concurrent regimen and 73% (grade 3–4 adverse events: 18%) in the sequential therapy group [54].
The outcomes for combined therapy with nivolumab plus ipilimumab versus placebo plus ipilimumab in BRAF-wild type and BRAF-mutant unresectable/metastatic melanoma were recorded in one trial (CheckMate 069, NCT01927419). Combination therapy appeared to be effective in patients with both BRAF-wild type (objective response: 61%, 44 of 72 patients, 95%CI: 49 to 72; complete response: 22%, 16 patients) and BRAF-mutant tumors (objective response: 52%, 12 of 23 patients, 95%CI: 31 to 73; complete response: 22%, 5 patients) [53]. The placebo group, however, exhibited poor outcomes in both BRAF-wild type (objective response: 11%, 4 of 37 patients, 95%CI: 3 to 25; complete response: 0%) and BRAF mutant tumors (objective response: 10%, 1 of 10 patients, 95%CI: 0 to 45; complete response: 0%). A subgroup analysis in this study evaluated the influence of tumor PD-L1 status on clinical outcomes. Patients receiving combination therapy demonstrated no significant difference in objective response rates (PD-L1 positive: 58, 95%CI: 37–78; PD-L1 negative: 55, 95%CI: 41–69) [53].
Another trial assessing survival outcomes for combined therapy with nivolumab plus ipilimumab versus placebo in treatment naïve unresectable/metastatic melanoma reported a median PFS for nivolumab monotherapy as 6.9 months (95%CI: 4.3 to 9.5), ipilimumab monotherapy as 2.9 months (95%CI: 2.8 to 3.4), and combined therapy with ipilimumab plus nivolumab as 11.5 months (95%CI: 8.9 to 16.7) (CheckMate 067, NCT01844505) [55, 56]. The study reported an overall survival at 2 years for nivolumab plus ipilimumab combination as 64%, nivolumab monotherapy as 59% and ipilimumab monotherapy as 45%. At 3 years follow-up, these were 58, 52 and 34%, respectively. Median overall survival for ipilimumab monotherapy was recorded as 19.9 months (95%CI: 16.9–24.9), nivolumab monotherapy as 37.6 months (95%CI: 29.1 - not reached) and as not reached (95%CI 38.2 months - not reached) for combination therapy arm. The objective response with combination therapy was noted in 58% patients, 19% with ipilimumab monotherapy and 44% with nivolumab monotherapy whereas complete response was observed in 19, 5 and 16% patients, respectively [56]. This data from CheckMate 067 allowed for confirmatory approval of combined therapy with nivolumab and ipilimumab for melanoma that initially received an accelerated approval by the FDA based upon the findings of CheckMate 069 trial. In addition to the above, the CheckMate 067 study also presented data on the influence of PD-L1 status on clinical outcomes. Patients with PD-L1 positive melanoma that received either combination therapy or nivolumab monotherapy had a median PFS of 14.0 months. However, study participants with PD-L1 negative melanoma exhibited a median PFS of 5.3 months (95%CI: 2.8 to 7.1) with nivolumab monotherapy and 11.2 months (95%CI: 8.0 - not reached) with combination therapy [55]. Lastly, with regards to the safety, this trial noted treatment related grade 3–4 adverse events in 59% patients receiving nivolumab plus ipilimumab therapy, 21% of those receiving nivolumab only and 28% patients treated with ipilimumab monotherapy [56].
A different trial investigating the effects of variation in the sequence of administering different immunotherapy agents observed that the patient cohort receiving nivolumab before ipilimumab exhibited grade 3–5 treatment related adverse events (TRAE) in 50% patients, response at 25 weeks in 41% and 12 months overall survival in 76% patients (CheckMate 064, NCT01783938) [57]. In the patient cohort receiving ipilimumab prior to nivolumab, 42.8% patients had a grade 3–4 TRAE, 20% patients exhibited response at 25 weeks and 12 months overall survival was noted in 54% patients [57].
Finally, one trial investigated the safety and efficacy of combined therapy with reduced dose ipilimumab (1 mg/kg every 3 weeks for 4 doses) plus full-dose pembrolizumab (2 mg/kg every 3 weeks) in patients with advanced melanoma (KEYNOTE-029, NCT02089685) [58]. This trial documented grade 1–2 and grade 3–4 treatment related adverse events in 51% (78 of 153) and 45% (69 of 153) patients, respectively. Immune-related adverse events were reported in 60% (92 of 153) of melanoma patients, of which 27% (42 of 153) patients experienced one or more grade 3–4 immune-related adverse events. A number of study participants discontinued treatment due to treatment related adverse events. This included 14% (22 of 153) patients discontinuing both ipilimumab and pembrolizumab, 9% (14 of 153) patients stopping pembrolizumab only and 8% (12 of 153) patients that discontinued ipilimumab only. With respect to survival outcomes (median 17.0 months follow-up), the study reported a PFS at 12 months of 69% (95%CI: 60–75), objective response of 61% (93 of 153 patients, 95%CI: 53–69), complete response of 15% (23 of 153 patients), partial response of 46% (70 of 153 patients), stable disease in 18% (28 of 153 patients) and progressive disease in 19% (29 of 153 patients) [58]. These results were considerably better in terms of survival benefit and toxicity profile than combination therapy with nivolumab and ipilimumab for melanoma. Combined checkpoint inhibition with nivolumab 1 mg/kg plus ipilimumab 3 mg/kg evaluated in early phase 1 trials reported an objective response rate of 53% (9 of 17 patients, 95%CI: 28 to 77), complete response of 17% (3 of 17 patients), partial response of 35% (6 of 17 patients) and serious treatment related adverse events in 49% patients (NCT01024231) [54, 59].
Combination checkpoint inhibition trials in NSCLC
Combined immunotherapy with anti-PD-1/PD-L1 and anti-CTLA-4 MoAbs in patients with NSCLC is currently being investigated in 16 ongoing trials (Table 2). Over half (10 of 16 trials) of these trials are evaluating combination therapy with nivolumab and ipilimumab with or without other therapeutic modalities. Other combination checkpoint inhibition regimens that are being examined in patients with NSCLC include tremelimumab plus durvalumab (5 of 16 trials) and pembrolizumab plus ipilimumab (1 of 16 trials).
Presently, five ongoing trials are assessing the combined use of anti-PD-1/PD-L1 and/or anti-CTLA-4 MoAbs with various chemotherapy agents. One of the trials has defined treatment cohorts on the basis of patient tumor marker status (NCT01998126). Patients with EGFR mutant NSCLC will receive erlotinib with either nivolumab or ipilimumab and those with ALK rearranged NSCLC will be administered crizotinib with either nivolumab or ipilimumab. Another trial will compare PFS, ORR, and duration of response in patients with advanced NSCLC after administration of dasatinib (SRC-family protein-tyrosine kinase inhibitor) plus nivolumab, BMS-986016 (anti- LAG-3 {lymphocyte activation gene-3} MoAb) plus nivolumab and ipilimumab plus nivolumab (NCT02750514) [10]. Participants enrolled in CheckMate 227 will be randomized to receive nivolumab plus platinum doublet chemotherapy (carboplatin/cisplatin plus gemcitabine for squamous NSCLC and carboplatin/cisplatin plus pemetrexed for non-squamous NSCLC) or combined therapy with nivolumab plus ipilimumab (NCT02477826). Similarly, CheckMate 722 will evaluate PFS for T790 M negative, EGFR mutant NSCLC patients treated with nivolumab plus platinum doublet chemotherapy (carboplatin/cisplatin plus pemetrexed) and ipilimumab plus nivolumab combination therapy (NCT02864251). The KEYNOTE 021 trial will focus on determining the RP2D for pembrolizumab plus ipilimumab, and it has a planned survival assessment to follow (NCT02039674). This trial will also evaluate the combined use of pembrolizumab with one or more standard chemotherapy agents using pre-defined treatment protocols. These include carboplatin, pemetrexed, paclitaxel, bevacizumab, erlotinib, and gefitinib (NCT02039674).
The development of a treatment regimen that integrates immunotherapy with PD-1/PD-L1 and CTLA-4 checkpoint inhibitors with surgery and radiation has been undertaken in one trial (NCT02696993). This trial will determine the RP2D for four combination therapies in NSCLC patients with brain metastases at the time of enrollment. The treatment regimens specified by the study protocol include nivolumab plus stereotactic radiosurgery, nivolumab plus ipilimumab and whole brain radiation therapy, nivolumab plus whole brain radiation therapy, and nivolumab plus ipilimumab and stereotactic radiosurgery.
At present, data on safety and survival benefit from combined immunotherapy with PD-1/PD-L1 and CTLA-4 checkpoint inhibitors in NSCLC is available from three trials. One trial evaluated four experimental dosing schedules of combined therapy with nivolumab and ipilimumab against one monotherapy arm (nivolumab) in order to identify the regimen that delivers maximum clinical benefit with an acceptable adverse-effects profile (CheckMate 012, NCT01454102). In the patient cohort receiving ipilimumab 1 mg/kg every 6 weeks plus nivolumab 3 mg/kg every 2 weeks an ORR of 39% was observed (95%CI: 23–55), median PFS was 3.9 months (95%CI: 2.6–13.2), the 1 year OS rate was 69% (95% CI: 52–81), and grade 3–4 treatment related adverse events (TRAE) occurred in 33% of patients [60]. In another cohort, designated to receive ipilimumab 1 mg/kg every 12 weeks plus nivolumab 3 mg/kg every 2 weeks, reported grade 3–4 TRAE occurred in 37% of patients, the ORR was 47% (95%CI: 31–64), median PFS was 8.1 months (95%CI: 5.6–13.6), and the 1 year OS rate was not calculated. Alternatively, patients treated with nivolumab 3 mg/kg every 2 weeks were noted to have an ORR of 23% (95%CI: 13–37), median PFS of 3.6 months (95%CI: 2.3–6.6), a 1 year OS rate of 73% (95% CI: 59–83), and TRAE occurred in 19% of patients. The study also attempted to correlate the data for treatment response to tumor PD-L1 expression. In patients treated with nivolumab plus ipilimumab combination therapy, the ORR for tumors with PD-L1 expression ≥1% and ≥ 50% were 57 and 92%, respectively. Conversely, patients receiving nivolumab monotherapy experienced an ORR of 28 and 50% for tumors with PD-L1 expression of ≥1% and ≥ 50%, respectively. Based on the overall analysis, treatment with ipilimumab 1 mg/kg every 6 weeks plus nivolumab 3 mg/kg every 2 weeks was selected for further investigation [60]. This regimen is presently under evaluation in the CheckMate 227 trial (NCT02477826).
The KEYNOTE 021 trial evaluated the combined use of pembrolizumab and traditional chemotherapy; it noted an ORR of 52% (13 of 25 patients, 95%CI: 31 to 72) and PFS of 10 months (95%CI: 4 - not reached) in patients treated with carboplatin 6 mg/mL/min plus pembrolizumab 2 or 10 mg/kg and paclitaxel 200 mg/m2 (NCT02039674) [61]. Likewise, the ORR was 48% (12 of 25 patients, 95%CI: 28 to 69) and PFS was “not reached” (95%CI: 4 - not reached) in patients that received paclitaxel 200 mg/m2 plus pembrolizumab 2 or 10 mg/kg, carboplatin 6 mg/mL/min and bevacizumab 15 mg/kg. Another cohort of patients that were given pemetrexed 500 mg/m2 plus carboplatin 5 mg/mL/min and pembrolizumab 2 or 10 mg/kg were noted to have an ORR of 71% (17 of 24 patients, 95%CI: 49 to 87) and PFS of 10 months (95%CI: 6 to 15) [61].
A different trial assessing combination checkpoint inhibition in patients with NSCLC involved the use of various doses of tremelimumab (1, 3 or 10 mg/kg) in combination with durvalumab (3, 10, 15 or 20 mg/kg) during the dose escalation phase (NCT02000947). The objective response (investigator assessed) in the tremelimumab 1 mg/kg treatment cohort was 23% (6 of 26 patients, 95%CI: 9 to 44) [62]. Also, an objective response was noted in 22% (2 of 9 patients, 95%CI: 3 to 60) of cases with PD-L1 positive tumors and 29% (4 of 14 patients, 95%CI: 8 to 58) of cases with PD-L1 negative tumors. MTD was exceeded for treatment with tremelimumab 3 mg/kg plus durvalumab 20 mg/kg, with almost 30% (2 of 6 patients) of patients reporting DLTs [62].
Discussion
There is great enthusiasm surrounding combination immunotherapy with PD-1/PD-L1 and CTLA-4 checkpoint inhibitors. The superior outcomes with combined immunotherapy over single-agent regimens in preclinical studies, together with the approval of nivolumab plus ipilimumab combination therapy for patients with melanoma have shed light on the therapeutic potential of this concept. The possibility of expanding the spectrum of indications for combination checkpoint inhibition to a wide range of tumor histologies is being explored in several trials. Simultaneously, extensive efforts have been undertaken to optimize clinical benefit to adverse effects ratios with combination checkpoint inhibition.
Combined therapy with anti-PD-1/PD-L1 and anti-CTLA-4 MoAbs in advanced melanoma has exhibited better survival outcomes in comparison with single-agent immunotherapy (Fig. 3). CheckMate 067 reported a survival benefit with nivolumab plus ipilimumab combination therapy (median PFS: 11.5 months, objective response 58%) over monotherapy with ipilimumab (median PFS: 2.9 months, objective response 19%) and nivolumab (median PFS: 6.9 months, objective response 44%) [55, 56, 63]. It is, however, important to note that though this study met the co-primary end-point of exhibiting improved overall survival with combination therapy versus ipilimumab, it was underpowered to reflect upon the use of nivolumab and ipilimumab combination therapy over anti-PD-1 monotherapy followed by subsequent ipilimumab rescue. Another trial, CheckMate 069, recorded the hazard ratio for death or progression of disease for combined versus single-agent immunotherapy for BRAF wild-type as 0.40 (95% CI: 0.23 to 0.68, p < 0.001) and BRAF-mutant as 0.38 (95% CI: 0.15 to 1.00) melanoma patients, underscoring the survival benefit with combination checkpoint inhibition [53]. Akin to the aforementioned trials, several ongoing trials will compare single-agent immunotherapy with combination checkpoint inhibition with anti-PD-1/PD-L1 plus anti-CTLA-4 checkpoint inhibitors (NCT01940809, NCT02736123, NCT02519322, NCT02731729, NCT02374242, NCT02523313, NCT02599402, NCT02460068, NCT02750514, NCT02154490, NCT02785952, NCT02477826, NCT02352948, NCT02453282, NCT01928394, NCT02537418).

Comparison of objective response in select trials. Legend: Figure presenting a comparison of objective response in study participants, expressed in percent individuals, with different treatment regimens in CheckMate 012, NCT02000947 and CheckMate 067 trials. Abbreviations: NIVO, nivolumab; IPI, ipilimumab; DURVA, durvalumab; TREME, tremelimumab; Q(x)W, every (x) weeks; NSCLC, non-small cell lung cancer
Several studies have attempted to correlate the expression of PD-L1 and response to combination checkpoint inhibition with anti-PD-1/PD-L1 plus anti-CTLA-4 MoAbs. PD-L1 positivity has classically been defined as visualization of at least 5% of tumor cells with PD-L1 staining in a section containing a minimum of one hundred cells suitable for evaluation [53, 54, 64, 65]. NCT01024231 documented response with combination therapy regardless of tumor PD-L1 status [54]. Likewise, CheckMate 069 reported no significant variation in response to combination checkpoint inhibition based on PD-L1 status [53]. Interestingly, patients with PD-L1 positive melanoma had better objective response rates as compared to those who tested negative for PD-L1 with ipilimumab monotherapy [53]. Another trial, CheckMate 067, noted a considerable advantage in median PFS with combined ipilimumab plus nivolumab (11.2 months) as opposed to nivolumab monotherapy (5.3 months) in patients with PD-L1 negative melanoma. The median PFS for patients with PD-L1 positive tumors, however, was the same for both treatment groups (14 months) [65]. Similarly, a different trial evaluating low-dose ipilimumab plus nivolumab in NSCLC patients reported an ORR of 57% in patients with tumor PD-L1 expression ≥1 and 92% in patients with tumor PD-L1 expression ≥50% (CheckMate 012) [60]. Considering the above, it appears that a pragmatic approach for selecting the most appropriate immunotherapy regimen (monotherapy versus combination therapy) may be through a novel treatment algorithm including tumor PD-L1 status.
The incidence of treatment-related adverse events with combination checkpoint inhibition has been a matter of concern in pivotal trials. The CheckMate 069 trial, which evaluated combination therapy with nivolumab and ipilimumab (nivolumab 1 mg/kg plus ipilimumab 3 mg/kg every 3 weeks for 4 doses followed by monotherapy with nivolumab 3 mg/kg every 2 weeks) versus ipilimumab monotherapy in melanoma patients, documented treatment-associated grade 3–4 adverse events in 54% of patients receiving combination therapy as compared to 24% receiving ipilimumab monotherapy [53]. These results suggest that melanoma patients receiving combination checkpoint inhibition were much more likely to develop severe drug-related adverse events as compared to treatment with ipilimumab monotherapy. Although 68% of patients that discontinued combination therapy due to toxicity exhibited an objective response, concerns over treatment-related toxicity with combination checkpoint inhibition regimens persuade some to favor immune-checkpoint inhibitor monotherapy [53]. In order to validate these findings, the same combination therapy regimen was evaluated in the CheckMate 067 trial and compared ipilimumab monotherapy and nivolumab monotherapy in parallel arms [56]. The frequency of grade 3–4 adverse events in patients treated with combination therapy (59% patients) was higher than that recorded for patients receiving monotherapy with ipilimumab (28% patients) or nivolumab (21% patients) [56]. However, treatment related adverse events with combination therapy were described as manageable and the study concluded that this regimen was suitable for further investigation. Considering the above, it may be stated that one should be cautious in selection of combination immune checkpoint inhibition over monotherapy in elderly patients with high frailty index.
A retrospective pooled analysis conducted to study efficacy and safety of combined therapy with nivolumab and ipilimumab in patients that discontinued therapy due to adverse events presented interesting findings. Data from phase 2 and phase 3 trials for advanced melanoma evaluating nivolumab 1 mg/kg plus ipilimumab 3 mg/kg every 3 weeks followed by monotherapy with nivolumab 3 mg/kg every 2 weeks, was pooled to compare outcomes in participants who discontinued therapy due to adverse events versus those who did not [66]. After a minimum of 18 months follow-up, median PFS and objective response rate for patients that discontinued therapy during induction were found to be 8.4 months and 58.3% respectively. On the other hand, patients that did not discontinue therapy were found to have a median PFS and objective response rate of 10.8 months and 50.2%, respectively. The nearly similar efficacy outcomes in the two groups indicated that despite discontinuing the therapy, patients continued to derive benefits from the treatment [66]. In other words, shorter course of treatment exhibited outcomes comparable to those achieved with full-course combination therapy. Also, it may be argued that immune related adverse events could possibly serve as surrogate markers for patients that may benefit from immunotherapy regimens.
The use of low-dose combination checkpoint inhibition appears to be a promising approach for improving clinical benefit without significantly increasing adverse events. The CheckMate 012 trial assessed several nivolumab plus ipilimumab combination regimens as first-line therapy in NSCLC patients. The frequency of treatment-associated grade 3–4 adverse events with nivolumab 3 mg/kg every 2 weeks plus ipilimumab 1 mg/kg every 12 weeks was 37% and with nivolumab 3 mg/kg every 2 weeks plus ipilimumab 1 mg/kg every 6 weeks was 33% [60]. The frequency of treatment-related grade 3–4 adverse events with nivolumab monotherapy was 19% [60]. Low-dose combination checkpoint inhibition with nivolumab and ipilimumab had a more acceptable adverse-effects profile compared to the combination regimen evaluated in CheckMate 067 (Fig. 4). However, it may be argued that the variation in toxicity profile was secondary to, or at least in part influenced by a difference in tumor histologies. One example may be the FDA approved regimen for melanoma (4 cycles of ipilimumab 3 mg/kg plus nivolumab 1 mg/kg every 3 weeks followed by nivolumab 240 mg every 2 weeks), that exhibited an acceptable safety profile and response in recurrent small cell lung cancer but at the same time demonstrated a poor safety and efficacy profile in NSCLC, leading to abandonment of this strategy in the latter [60, 67]. Data from ongoing studies investigating low-dose combination checkpoint inhibition in a number of tumor histologies will be crucial to the validation of these findings.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of treatment related adverse events for different regimens in CheckMate 012 and CheckMate 067. Legend: The figure elaborates percent patients documented to have adverse events with different treatment regimens assessed in the CheckMate 012 and CheckMate 067 trials. Please note that some participants had more than one adverse event. No treatment associated deaths were reported till point of assessment in CheckMate 012 while 2 treatment related deaths in CheckMate 067 nivolumab group were reported > 100 days after discontinuation of therapy. Abbreviations: NIVO, nivolumab; IPI, ipilimumab; n, number of patients; X axis: treatment regimens, Y axis: percent patients relative to cohort size
Another step towards achieving the right balance of efficacy and incidence of adverse events may be to critically assess the use of common terminology criteria for adverse events (CTCAE). CTCAE are used for documenting chemotherapy associated adverse events [68]. They are instrumental to determine the appropriate dose limiting toxicity for the experimental regimen in a trial. This in-turn has a significant bearing on the recommended phase 2 dose for the novel therapeutic agent. CTCAE are, however, now being applied to immune related adverse events for novel immunotherapy regimens [69]. A phase 1 trial investigating nivolumab plus ipilimumab in melanoma patients used an asymptomatic rise in lipase as the primary dose limiting toxicity, central to informing the recommended phase 2 dose in this trial. A retrospective study analyzed the association between asymptomatic rise in lipase and amylase (grade 3 and above) with pancreatitis in 119 participants and found only 2 patients to have pancreatitis. This represented 6.3% of all patients with grade 3 and above lipase and 20% of those with grade 3 or above increase in both amylase and lipase. Thus, in simple terms, lipase did not appear to be a relevant marker for pancreatitis. This observation thus signifies the need to exercise appropriate caution when grading independent lab values using CTCAE in immunotherapy trials [69].
Existing evidence suggests that single-agent immunotherapy for tumors with high PD-L1 expression (≥50% cells positive for PD-L1 staining) can achieve far superior outcomes than chemotherapy in similar settings. In patients with NSCLC with high PD-L1 expression, pembrolizumab exhibited a response rate of 45%, PFS of 10.3 months, and a 1-year survival rate of 70% [70]. In comparison, treatment with standard of care chemotherapy had a response rate of 28%, PFS of 6 months, and 1-year survival rate of 54% (KEYNOTE 026) [70]. On the other hand, trials involving a lower cut-off value for PD-L1 positivity (≥5% cells positive for PD-L1 staining) failed to demonstrate any advantage in clinical efficacy with single-agent immunotherapy over standard chemotherapy (CheckMate 026) [71, 72]. Reflecting on the data on efficacy and overall toxicity profile of single-agent immunotherapy regimens in tumors with high PD-L1 expression, outperforming these regimens may prove to be a challenge for combination checkpoint inhibition regimens. Further data from ongoing trials will be vital to conclusively determine if single-agent immunotherapy with pembrolizumab can be replaced with a combined immunotherapy regimen.
Immunotherapy with PD-1/PD-L1 plus CTLA-4 checkpoint inhibitors for a diverse set of solid tumors is currently being investigated in 8 trials (Table 3). Half of all phase 1/phase 2 solid tumor trials are evaluating combined therapy with nivolumab and ipilimumab. Others include three trials with combined therapy with tremelimumab plus durvalumab and one trial with atezolizumab plus ipilimumab. Each of these eight trials will evaluate combination checkpoint inhibition regimens in a large number of malignancies. The data gathered from these studies will be crucial to identifying tumor histologies that would benefit most from combination checkpoint inhibition.
Phase 1 solid tumor trials investigating combined immunotherapy with anti-CTLA-4 plus anti- PD-1/PD-L1 monoclonal antibodies
Recently, the FDA approved the use of pembrolizumab for unresectable/metastatic mismatch repair deficient (dMMR) or microsatellite instability-high (MSI-H) solid tumors and colorectal cancer with progression on prior therapy. This was based upon data from KEYNOTE 012, KEYNOTE 028, KEYNOTE 164, KEYNOTE 016 and KEYNOTE 158 [73–76]. The advised regimen is pembrolizumab 10 mg/kg every 2 weeks or 200 mg every 3 weeks for up to 24 months, unacceptable toxicity or progression of disease. It is of note that this is the first time when a drug has been approved not on the basis of tumor location but a tumor biomarker.
The Dual Anti-CTLA-4 and Anti-PD-1 Blockade in Rare Tumors (DART) trial will evaluate response to combination checkpoint inhibition for a large number of rare tumors in a basket fashion (NCT02834013). In this trial, minimizing toxicity profiles without compromising clinical efficacy is the primary goal. We nominated the low-dose combination therapy with fixed-dose nivolumab and wider interval ipilimumab (nivolumab 240 mg every 2 weeks plus ipilimumab 1 mg/kg every 6 weeks) for assessment in this trial. Our treatment regimen is based on the superior toxicity profile for this regimen observed in CheckMate 012 as compared to the FDA approved combination therapy regimen (nivolumab 1 mg/kg plus ipilimumab 3 mg/kg every 3 weeks for 4 doses followed by monotherapy with nivolumab 3 mg/kg every 2 weeks) in CheckMate 069 [53, 60]. Based on the fact that no significant difference in response was recorded between PD-L1 positive and negative patients receiving combination therapy, we decided to recruit study participants irrespective of tumor PD-L1 status. Through this trial, we expect to provide critical data for expanding the application of low-dose combination therapy in rare tumors.
Recent studies have suggested that sequential administration of immune-checkpoint inhibitors targeting various pathways may benefit cancer patients exhibiting treatment resistance. A multi-center retrospective study evaluated outcomes with ipilimumab and combination therapy with nivolumab and ipilimumab in advanced melanoma patients that previously failed treatment with anti-PD-1 MoAbs [77]. Patients receiving ipilimumab monotherapy were observed to have superior disease control as compared to those receiving combination checkpoint inhibition (42% versus 33%) [77]. Of note, though this was a retrospective study, it was insufficiently powered to detect the difference. A different retrospective analysis of 10 melanoma patients that received ipilimumab after progression on anti-PD-1 therapy found that 1 of 10 patients exhibited partial remission and an additional four patients had stable disease [78]. Similar to the findings of the above and other retrospective studies, the CheckMate 064 documented a higher treatment efficacy in melanoma patients receiving nivolumab prior to ipilimumab versus those receiving ipilimumab prior to nivolumab [57]. However, superior clinical efficacy with the former regimen was associated with an inferior toxicity profile to the latter [57]. Of note, the trial involved a planned switch to reverse sequence at 12 weeks and not at progression. Therefore, it remains unclear if switching to combinatorial regimen at the time of progression is a feasible approach. The outcomes from NCT02731729 trial should perhaps be able to provide some direction on this matter.
Conclusion
Combination immunotherapy is evolving at a phenomenal pace. In light of initial success in patients with melanoma, efforts to explore the indications for combination checkpoint inhibition with anti-PD-1/PD-L1 and anti-CTLA-4 MoAbs have diversified to a large number of tumor histologies. Several treatment strategies intended for achieving better clinical efficacy and to overcome challenges such as treatment resistance and toxicity associated with the use of immunotherapy agents, are presently under investigation. Of note, the use of low-dose combination checkpoint inhibition with nivolumab and ipilimumab in NSCLC appears to be a promising approach. Alternatively, the use of nivolumab prior to ipilimumab in the induction phase for melanoma patients may be a simple but effective strategy to achieve superior outcomes. Data from ongoing trials is expected to provide vital evidence for validation of the above preliminary findings and facilitate the application of combination checkpoint inhibition on a larger scale.
Acknowledgments
All data analyzed during this study is included in this published article.
Authors’ contributions
YKC and AA gathered, analyzed and interpreted the data from various published articles. All authors read and approved the final manuscript.
Notes
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.