Article Text

Abstract
Malignant pleural effusions (MPE) are a common terminal pathway for many cancers, with an estimated United States incidence of more than 150,000 cases per year. MPE is an aggressive disease with a uniformly fatal prognosis and a life expectancy of only 3 to 12 months. The development of an effective targeted therapy represents a pressing unmet need. This commentary focuses on how cellular and humoral components condition the pleural space as a tumor-promoting, wound-healing environment. Despite an abundance of potential antigen presenting and effector cells in the pleura, their physical isolation by the mesothelial barrier, the concentration of cytokines and chemokines driving the epithelial to mesenchymal transition (EMT) and M2 /Th-2 polarization, suppress tumor-specific immune effector responses. We argue that local immune repolarization must precede either immune checkpoint or cellular therapy to successfully eradicate pleural tumor. We further hypothesize that, because of its cellular content, a repolarized pleural space will provide an effective immune environment for generation of systemic anti-tumor response.
- Malignant pleural effusion
- Immunotherapy
- Pleural infiltrating T cells (PIT)
- Tumor associated macrophages (TAM)
Albert D. Donnenberg and Vera S. Donnenberg contributed equally to this work.
- CEACAM
- Carcinoembryonic antigen-related cell adhesion molecule
- CTLA-4
- Cytotoxic T-lymphocyte-associated protein 4
- EMT
- Epithelial to mesenchymal transition
- FcR
- Fraction crystalizable receptor
- IL
- Interleukin
- iTreg
- induced regulatory T cell
- M2
- M2-type macrophage polarization
- MPE
- Malignant pleural effusion
- PD
- Programmed death
- PD-L
- Programmed death ligand
- PIT
- Pleural infiltrating T cell
- TAM
- Tumor associated macrophage
- TGF
- Transforming growth factor
- Th2
- Th2-type T-cell polarization
- TIL
- Tumor infiltrating lymphocyte
- TIM-3
- T-cell immunoglobulin and mucin-domain containing-3
- VEGF
- Vascular endothelial growth factor
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Statistics from Altmetric.com
- Malignant pleural effusion
- Immunotherapy
- Pleural infiltrating T cells (PIT)
- Tumor associated macrophages (TAM)
Albert D. Donnenberg and Vera S. Donnenberg contributed equally to this work.
Introduction
At advanced stages, metastatic cancer infiltrates thoracic lymph nodes as well as the lining of the chest cavity, known as the pleura. When this occurs, the normal cycle of fluid secretion and absorption is interrupted, resulting in fluid collection and compression of the lung. The fluid, which is composed of serous proteins, cancer cells, and lymphoid and myeloid immune cells, is termed malignant pleural effusion (MPE). Accumulation of fluid results in symptoms that range from cough to life threatening dyspnea and hypoxia, but it is the aggressive nature of the tumor to which the patient ultimately succumbs. Epithelial cancers account for about 80% of patients receiving interventions and life expectancy ranges from 3 to 12 months [1] . Despite the fact that the incidence of MPE in the United States exceeds 150,000 cases per year [2], and despite the fact that a wide range of systemic and localized therapeutic approaches have been tested, current best practice is limited to palliation by drainage [3]. It is our contention that the interactions that occur between tumor and immune cells in the confines of the pleural space make it an incubator promoting an epithelial to mesenchymal transition (EMT) and the emergence of the most aggressive drug-resistant neoplastic cells. This commentary makes the case for an intrapleural immunotherapeutic approach for patients with MPE. Our growing appreciation of the immune environment of the pleural space and of the complex interplay between tumor and immune cells suggests a more rational immunotherapeutic approach to treat this condition.
Localized immunotherapy
The concept of immune system activation in the setting of thoracic malignancy dates to the 1970’s, when investigators noted improved survival in patients with empyema after resections for lung cancer [4], justifying largely unsuccessful trials of intrapleural Baccilus Calmette-Guérin (BCG) [5] and other bacterial antigens. Direct instillation of the recombinant cytokines interferon ɣ [6], interferon α2b [7] and IL-2 [8, 9] have also been tested. Intrapleural IL-2 was well tolerated in non-small cell lung cancer (NSCLC). Further, intrapleurally administered IL-2 levels were 6000-fold higher than in the plasma [8], indicating that locally administered IL-2 (formula weight = 15.5 kDa) is sequestered in the pleural space. This is a very important observation, since other large molecule biologicals, such as antibodies can be expected to be similarly concentrated when administered directly to the pleura. Although intrapleural IL-2 cleared effusions in 28 of 31 patients studied [9], and partial responses were seen with other cytokine modalities, the median time to progression ranged from days [7] to months [8]. Thus instillation of high-dose Th1 associated cytokines was insufficient by themselves to overcome the immunosuppressive environment of the pleural space.
Therapeutic use of pleural-infiltrating T cells (PIT)
A recent clinical trial described the use of tumor infiltrating lymphocytes (TIL) derived from MPE and malignant ascites in combination with cisplatin [10]. Effusion-derived TIL provided longer progression-free survival and better quality of life than cisplatin alone. The combination of immunotherapy and chemotherapy is somewhat counterintuitive since many cytotoxic agents inhibit cell proliferation, an important aspect of adaptive immunity. However, regulatory T cells (Treg) have been shown to be more susceptible to platinum-based combination chemotherapy than conventional CD4+ T cells [11], potentially providing a release from Treg-mediated suppression of anti-tumor immunity. Effusion-derived TIL have several important advantages over TIL derived from primary tumors or biopsies of solid metastases: [1] The T-cell yield from MPE or ascites is orders of magnitude higher than from biopsies, so the number of passages required is lower, and culture time is shorter; [2] Malignant effusion pleural T cells (PIT) represent a cross-section of all TIL, whereas TIL derived from solid tumors display spatial heterogeneity and can differ with respect to function and specificity depending on the biopsy location [12]. Owing to their abundance, it may be possible to prime PIT by short term ex vivo exposure to activation signals, and reinstill them without expansion. The resulting cells would not be cytokine addicted as are conventional TIL and would not require administration of high dose IL-2 for their survival.
Immune checkpoint inhibitors in MPE
PD-L1 is expressed on malignant mesothelioma [13] and other malignancies and is therefore potentially targetable by anti-PD-L1 antibodies. T cells from NSCLC MPE display increased expression of PD-1, TIM-3, and CTLA-4, when compared with non-malignant controls [14], possibly due to high levels of TGF-β in the effusion, secreted by PD-L1+ tumor-associated M2-macrophages.
Toward efficacious localized immunotherapy therapy
It is becoming increasingly clear that both conventional and immunotherapeutic attempts have failed in MPE because the pleural space is a sequestered environment in which tumor cells and immune cells interact to the benefit of the tumor. In the pleural space, wound-healing cytokines and chemokines are concentrated, and juxtacrine interactions of tumor, macrophages and mesothelial cells are favored by their proximity. The result is the perpetuation of a wound-healing environment in which T-cell effectors are suppressed or killed, and macrophages are channeled to an M2 program that assists angiogenesis and metastasis, all culminating in the promotion of an aggressive and invasive EMT tumor phenotype.
Sequestered environment
The pleural space represents a sequestered local environment formed by mesothelial cells joined by tight junctions [15]. Protein biologics such as IL-2 remain highly concentrated when administered intrapleurally, with local concentrations thousands of times higher than that of the plasma [8]. Protein movement from the plasma to the pleura is also impeded, albeit to a lesser extent, and the pleural effusion to plasma ratio of protein concentrations is inversely related to their molecular weight [16]. This is highly relevant to systemic administration of antibody therapeutics, which predictably would not pass easily into the pleural space, abdominal cavity, or interstitial spaces [17].
The pleural secretome
The cell-free serous component of MPE contains an array of cytokines and chemokines [18]. The majority of the secreted cytokines in MPE are Th2-like and include IL-10 [19], VEGF [20] and TGFβ [21], further promoting the wound-healing milieu to the detriment of an anti-tumor effector response. Interestingly, the pleiotropic cytokine IL-6 and its soluble receptor component sIL-6Rα are among the most abundant cytokines in MPE [22]. IL-6 is produced by the tumor [23] and also by pleural mesothelial cells [24] and stromal cells [25]. IL-6 plus IL-10 upregulate PD-L1 expression in tumor cells [26]. IL-6 signal transduction is mediated through a receptor complex consisting of IL-6Rα (CD126) and IL-6Rβ (CD130). IL-6Rβ is expressed ubiquitously, but IL-6Rα expression is restricted chiefly to leukocytes and hepatocytes. In normal physiology, IL-6 mediates powerful systemic effects by trans-signaling, which occurs when IL-6 binds to soluble IL-6Rα and complexes with membrane-bound IL-6Rβ [27]. IL-6 trans-signaling has been shown to promote aggressive tumor behavior and progression in malignant ascites of ovarian cancer [28] and in breast cancer pleural effusions [23], and promotes EMT in non-small cell lung cancer [29], making it an attractive therapeutic target. Tocilizumab, a monoclonal antibody directed against IL-6Rα, is licensed for the treatment of rheumatoid arthritis, and has been used experimentally to treat cancer-associated cachexia [30] and cytokine release syndrome [31]. Intrapleural administration may have profound effects on the polarization of the pleural immune environment with minimal systemic effects.
Juxtacrine interactions
The proximity and high concentration of T cells, macrophages, mesothelial cells and tumor in the pleural space favors cell-cell contact and juxtacrine signaling. Examples include the promotion of EMT by binding of CD90 and EphA4 on the tumor to CD11b and Ephrin on macrophages, respectively [23]. Similarly, PD-L1 and PD-L2 expressed on tumor and pleural macrophages bind to PD-1 on T cells, promoting anergy, development of induced regulatory T cells (iTregs) and apoptosis [32]. Other ligands expressed on pleural tumor, such as CEACAM1 which binds to TIM-3, may interact with immune checkpoint receptors expressed on PIT. MPE, which are routinely therapeutically drained, provide a unique window into interactions that are more difficult to observe in other metastatic settings.
Conclusion
Despite continuing efforts to provide effective systemic and localized cytotoxic and immune-based therapies, there is currently no effective treatment for malignant pleural effusions. We argue that the pleural space, because of the physical barrier provided by the mesothelium, acts like a bioreactor in which carcinoma cells, TAM, PIT and stroma interact (Fig. 1). The concentration of wound-healing cytokines and chemokines and environmental polarization resulting from these multi-way feedback interactions promote EMT and aggressive tumor behavior, and thwarts anti-tumor immune effector responses by multiple distinct and probably synergistic mechanisms. The benefit of intrapleural administration is that high molecular weight biologicals are sequestered in the pleural space [8, 33] by the same mechanism that allows the accumulation of high concentrations of locally secreted cytokines. Thus, repolarizing treatment combinations that would have unacceptable dose-limiting toxicities when given systemically, may have more acceptable toxicity profiles when administered directly to the pleural space at a fraction of the systemic dose.

{kind=link}
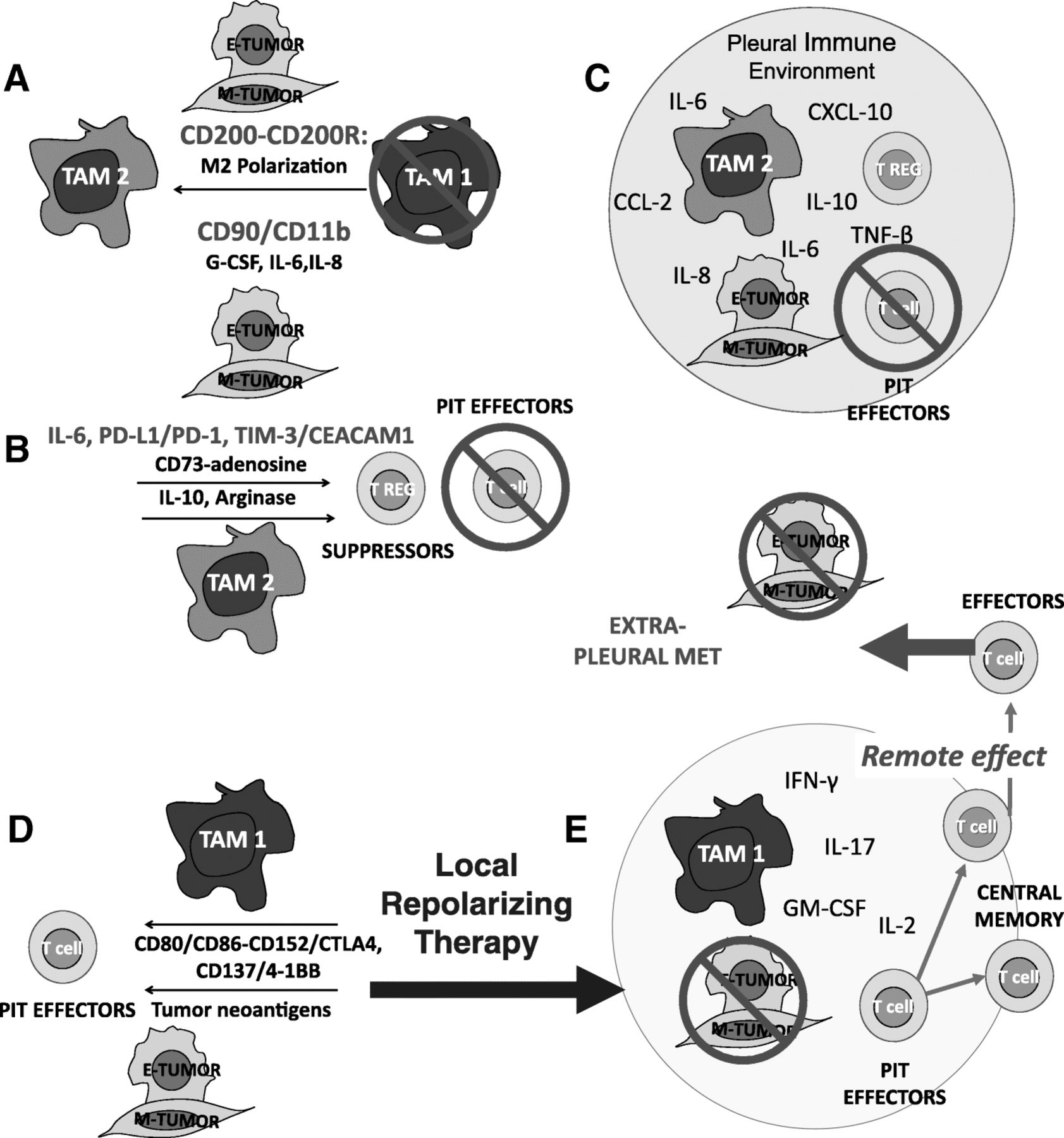
The interactions of tumor, TAM, and T-cells are highly dependent on the local immune environment. Tumors can evade an immune response, even when all of the required components are abundant and in close proximity. Panel a: Tumor effects on TAM. Tumor, particularly tumor that has undergone EMT, amplifies and maintains TAM M2-like wound healing polarization. TAM are recruited with tumor-secreted G-CSF and polarized through CD200/CD200R and CD90/CD11b interactions and tumor secreted IL-6 and IL-8. Panels b and c: Tumor and TAM polarization effects on T cells. M2 TAM polarization favors T-cell suppression through cytokines and programmed death ligand-induced apoptosis (b). The pleural space is isolated from the systemic circulation, permitting the maintenance of very high local cytokine and chemokine levels. The encircled space (Panel c) represents the isolated pleural immune environment in which potential effector cells are potently suppressed. It should be possible to repolarize the pleural immune environment with local delivery of cytokines, activation signals, antibody-based therapeutics and ex vivo activated PIT, tipping the balance in favor of the immune system. Panel d: Local repolarizing therapy results in M1 TAM polarization, providing presentation of tumor neo-antigens and costimulatory signals, culminating in the generation of tumor-specific effector T cells. Panel e: Once the immune blockade has been breached, antigen presenting cells and T cells can traffic to the draining lymph nodes where responding T cells can proliferate and differentiate. Once this has occurred, tumor specific T cells can be expected to home to other sites of metastasis
The remarkable progress of cancer immunotherapeutics over the last decade demands that we devise new methods to treat rather than palliate malignant pleural effusions. Recognizing the pleural space as a sequestered environment in which all the components required for an effective anti-tumor response are present, but conscripted into a wound-healing mode, we argue that a combination of local repolarizing therapy in combination with immune checkpoint blockade and therapeutic effector cells may be sufficient to turn a dire clinical situation to therapeutic advantage.
Acknowledgments
None.
Authors’ contributions
Albert and Vera Donnenberg contributed equally to the writing of this commentary. James Luketich and Rajeev Dhupar provided clinical insights. All authors read and approved the final manuscript.
Notes
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors consent.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
- CEACAM
- Carcinoembryonic antigen-related cell adhesion molecule
- CTLA-4
- Cytotoxic T-lymphocyte-associated protein 4
- EMT
- Epithelial to mesenchymal transition
- FcR
- Fraction crystalizable receptor
- IL
- Interleukin
- iTreg
- induced regulatory T cell
- M2
- M2-type macrophage polarization
- MPE
- Malignant pleural effusion
- PD
- Programmed death
- PD-L
- Programmed death ligand
- PIT
- Pleural infiltrating T cell
- TAM
- Tumor associated macrophage
- TGF
- Transforming growth factor
- Th2
- Th2-type T-cell polarization
- TIL
- Tumor infiltrating lymphocyte
- TIM-3
- T-cell immunoglobulin and mucin-domain containing-3
- VEGF
- Vascular endothelial growth factor
References
Footnotes
Funding This work is supported by the Thoracic Surgery Foundation for Research and Education STS Research Grant (7/2016–7/2018), BC032981, BC044784, W81XWH-12-1-0415 and BC132245_W81XWH-14-0258 from the Department of Defense, National Cancer Institute grant R21 CA191647, the Glimmer of Hope Foundation, and the David Downing Fund.
Availability of data and materials Not applicable.