Article Text

Abstract
Background Talimogene laherparepvec is an oncolytic immunotherapy approved in the US, Europe, Australia and Switzerland. We report the final planned analysis of OPTiM, a randomized open-label phase III trial in patients with unresectable stage IIIB–IVM1c melanoma.
Methods Patients were randomized 2:1 to receive intratumoral talimogene laherparepvec or subcutaneous recombinant GM-CSF. In addition to overall survival (OS), durable response rate (DRR), objective response rate (ORR), complete responses (CR), and safety are also reported. All final analyses are considered to be descriptive and treatment responses were assessed by the investigators.
Results Of 436 patients in the intent-to-treat population, 295 were allocated to talimogene laherparepvec and 141 to GM-CSF. Median follow-up in the final OS analysis was 49 months. Median OS was 23.3 months (95% confidence interval [CI], 19.5–29.6) and 18.9 months (95% CI, 16.0–23.7) in the talimogene laherparepvec and GM-CSF arms, respectively (unstratified hazard ratio, 0.79; 95% CI, 0.62–1.00; p = 0.0494 [descriptive]). DRR was 19.0 and 1.4% (unadjusted odds ratio, 16.6; 95% CI, 4.0–69.2; p < 0.0001); ORR was 31.5 and 6.4%. Fifty (16.9%) and 1 (0.7%) patient in the talimogene laherparepvec and GM-CSF arms, respectively, achieved CR. In talimogene laherparepvec-treated patients, median time to CR was 8.6 months; median CR duration was not reached. Among patients with a CR, 88.5% were estimated to survive at a 5-year landmark analysis. Talimogene laherparepvec efficacy was more pronounced in stage IIIB–IVM1a melanoma as already described in the primary analysis. The safety reporting was consistent with the primary OPTiM analysis.
Conclusions In this final planned OPTiM analysis, talimogene laherparepvec continued to result in improved longer-term efficacy versus GM-CSF and remained well tolerated. The final analysis also confirms that talimogene laherparepvec was associated with durable CRs that were associated with prolonged survival.
Trial registration ClinicalTrials.gov identifier: NCT00769704.
- Efficacy
- Final analysis
- Melanoma
- Overall survival
- Talimogene laherparepvec
- AE
- Adverse event
- AJCC
- American Joint Committee on Cancer
- CI
- Confidence interval
- CR
- Complete response
- CTCAE
- Common Terminology Criteria for Adverse Events
- DCR
- Disease control rate
- DR
- Durable response
- DRR
- Durable response rate
- ECOG
- Eastern Cooperative Oncology Group
- GM-CSF
- Granulocyte-macrophage colony-stimulating factor
- HR
- Hazard ratio
- ITT
- Intent-to-treat
- OR
- Odds ratio
- ORR
- Objective response rate
- OS
- Overall survival
- PR
- Partial response
- RFS
- Recurrence-free survival
- TFI
- Treatment-free interval
- T-VEC
- Talimogene laherparepvec
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Statistics from Altmetric.com
Background
Talimogene laherparepvec (T-VEC), a first-in-class viral oncolytic immunotherapy [1], was approved in the United States in 2015 for the local treatment of unresectable, cutaneous, subcutaneous and nodal lesions in patients with melanoma recurrent after initial surgery [2], based on data from OPTiM, a randomized phase III open-label trial [3–5]. Intratumoral T-VEC significantly improved durable response rate (DRR) versus subcutaneous GM-CSF; achieving a durable response (DR; response lasting ≥6 months) was associated with clinical benefits such as overall survival (OS) and quality of life [3]. In the primary analysis of OS (secondary endpoint performed after 290 deaths; median follow-up 44 months), T-VEC showed a numerically reduced risk of death versus GM-CSF (median OS 18.9 vs. 23.3 months; hazard ratio [HR] 0.79; 95% confidence interval [CI], 0.62–1.00; P = 0.051) [4]. Exploratory analyses of OPTiM revealed that the benefit of T-VEC versus GM-CSF (in terms of DRR, objective response rate [ORR] and OS) was more pronounced in patients with stage IIIB–IVM1a disease than in later-stage metastatic disease [4, 5]. A tolerable safety profile for T-VEC, with a low rate of grade 3/4 adverse events (AEs), was also observed [4]. In Europe, T-VEC was approved in 2015 for unresectable, regionally or distantly metastatic (stage IIIB–IVM1a) melanoma with no bone, brain, lung or other visceral disease [6].
Here we report the final planned analysis of OS in the OPTiM trial performed 3 years after the last patient was randomized. Findings are described for the overall intent-to-treat (ITT) population as well as in patients with early metastatic disease (stage IIIB–IVM1a melanoma) included in the European label. Final analyses of objective response, including exploratory analyses of complete responders, are also discussed.
Methods
Patients
Eligibility criteria for the OPTiM trial have been described previously [4]. Eligible patients were ≥ 18 years old and had histologically confirmed, unresectable, bidimensionally measurable stage IIIB/C/IV melanoma according to the 7th edition AJCC staging system [7] with ≥1 cutaneous, subcutaneous or nodal lesions that was suitable for direct or ultrasound-guided injection. Other inclusion criteria included an Eastern Cooperative Oncology Group (ECOG) performance status of ≤1; serum lactate dehydrogenase ≤1.5 × upper limit of normal; ≤3 visceral lesions (excluding lung or nodal lesions associated with visceral organs) with none > 3 cm; and adequate organ function. Further details are provided in the Additional file 1.
Study design and treatment
OPTiM (ClinicalTrials.gov NCT00769704) enrolled subjects at 64 sites in the United States, the United Kingdom, Canada, and South Africa between 2009 and 2011. Patients were randomized in a 2:1 ratio to receive intratumoral T-VEC (at the approved dose [6]) or subcutaneous recombinant GM-CSF [4] (see Additional file 1). Treatment continued for 6 months regardless of the occurrence of progressive disease (unless alternative therapy was clinically indicated). After 6 months, treatment was continued until clinically relevant disease progression, intolerability, consent withdrawal, complete remission, lack of response by 12 months or (T-VEC arm only) disappearance of injectable lesions. Patients with stable or responding disease at 12 months could continue treatment for 6 additional months. Data cut-off for this final analysis of OPTiM was 5 September 2014.
Assessments and endpoints
Efficacy
Efficacy assessments reported here include analysis of DRR, ORR, disease control rate (DCR) and OS using the final OPTiM data set.
Clinical response was evaluated using the modified World Health Organization criteria [8], as previously described [4]. For the primary OPTiM analysis, patients with an ORR (complete response [CR] or partial response [PR]) per investigator were evaluated by a blinded endpoint-assessment committee [5]. After the primary analysis, only response assessments per investigator were collected (and are reported herein). DRR was defined as the rate of CR or PR lasting continuously for ≥6 months and onset within ≤12 months of randomization. DCR was the proportion of patients with CR, PR or stable disease.
An analysis of complete responders in the T-VEC arm was conducted, including the time to achieve CR, the duration of CR once achieved and factors predictive of CR. Analyses also evaluated associations between CR and OS, CR and recurrence-free survival (RFS; date of CR to the date of recurrence, death due to disease progression, or initiation of new anti-melanoma therapy after achieving CR) and CR and treatment-free interval (TFI, time from the last dose of study therapy to first dose of subsequent therapy or censoring in the absence thereof at end of follow-up).
OS was defined as the time from random assignment to death from any cause. Subgroup analyses were performed to investigate the relative effects of treatment on OS according to key covariates, including age, sex, disease stage, tumor burden, ECOG performance status, and line of therapy.
Safety
Safety was evaluated from enrollment up to the data cut-off for the final analysis using National Cancer Institute Common Terminology Criteria for AEs (CTCAE) version 3.0.
Statistical analyses
Sample size was determined as described previously [4]. All efficacy analyses reported here are descriptive, as multiple comparisons were not controlled for. Final analysis of DRR was conducted using a 2-sided unadjusted Fisher exact test. Univariate and multivariate analyses (including a logistic regression model) were conducted to identify independent factors associated with achieving CR. The final descriptive analysis of OS was planned to occur 3 years after the last randomization in OPTiM, and used an unadjusted log-rank test and a Cox proportional hazard model to estimate the unstratified HR for treatment effect. Five-year survival in the T-VEC arm was estimated using the Kaplan-Meier method. Exploratory subgroup analyses of OS by key covariates was carried out using the Gail and Simon quantitative interaction test. Full details of the statistical analyses can be found in the Additional file 1.
Results
Patients
Of the 436 patients in the ITT population, 295 (68%) were allocated to receive T-VEC and 141 (32%) to GM-CSF. Baseline characteristics, which have been previously reported [4], were generally well balanced between treatment arms (see Additional file 1). Median (range) duration of treatment was 23.1 weeks (0.1–176.7) in the T-VEC arm and 10.0 weeks (0.6–120.0) in the GM-CSF arm. Median follow-up (time from random assignment to analysis) in the final analysis of OS was 49 months.
Efficacy in the final OPTiM analysis dataset
Intent-to treat population (stage IIIB–IVM1c melanoma)
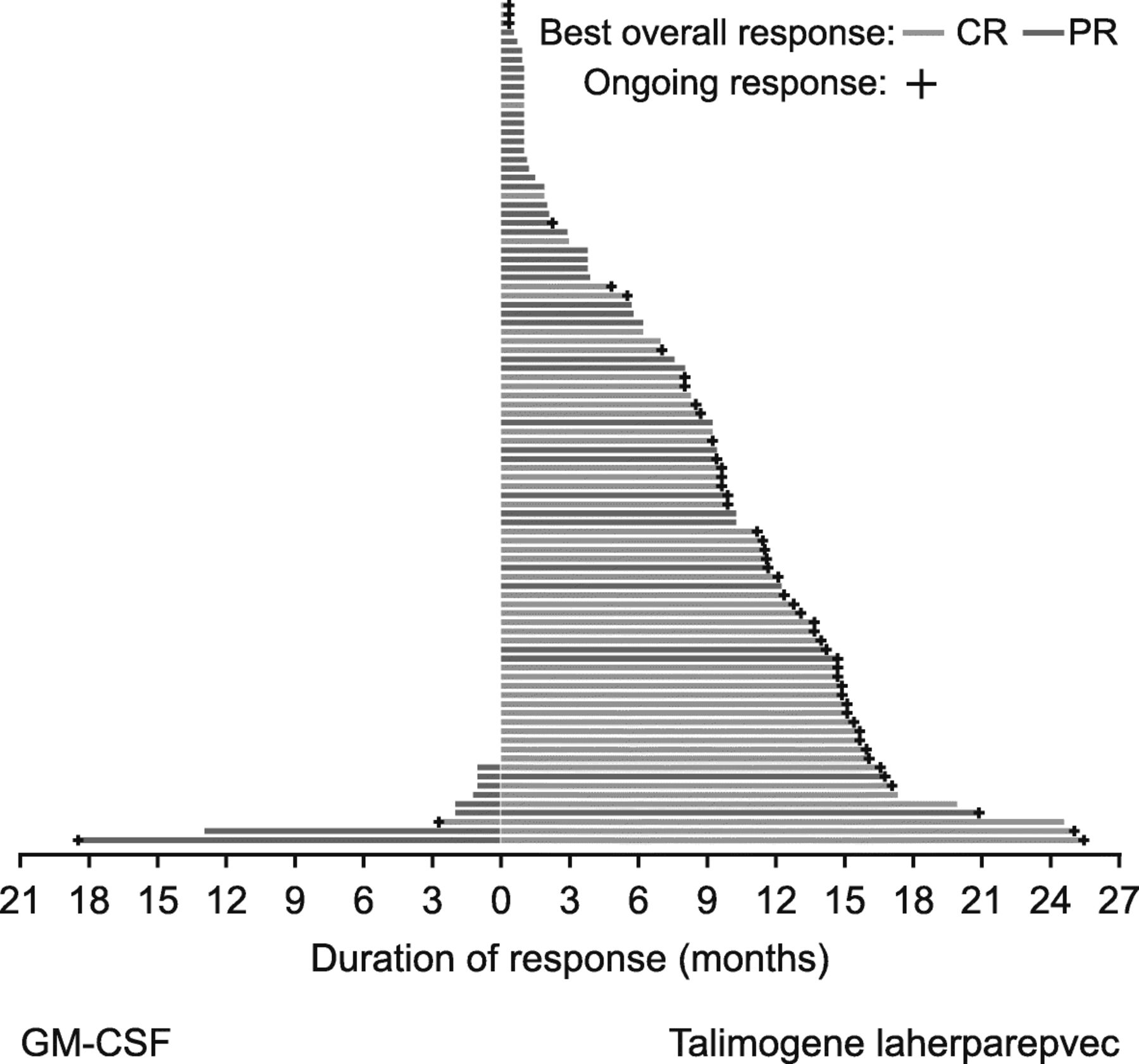
DRR was higher with T-VEC than GM-CSF: 57 (19.3%) and 2 (1.4%) patients, respectively, experienced a durable response per investigator assessment (unadjusted odds ratio, 16.6; 95% CI, 4.0–69.2; p < 0.0001). ORR was also higher with T-VEC (31.5%; 95% CI, 26.3–37.2) than GM-CSF (6.4%; 95% CI, 3.0–11.8; Table 1). Overall, 50 (16.9%) and 1 (0.7%) patients in the T-VEC and GM-CSF arms, respectively, achieved CR, while 43 (14.6%) and 8 (5.7%) achieved PR (Table 1). Figure 1 illustrates response duration. The DCR was 76.3% versus 56.7% with T-VEC and GM-CSF, respectively (Table 1).
Efficacy outcomes in final analysis data set of OPTiM
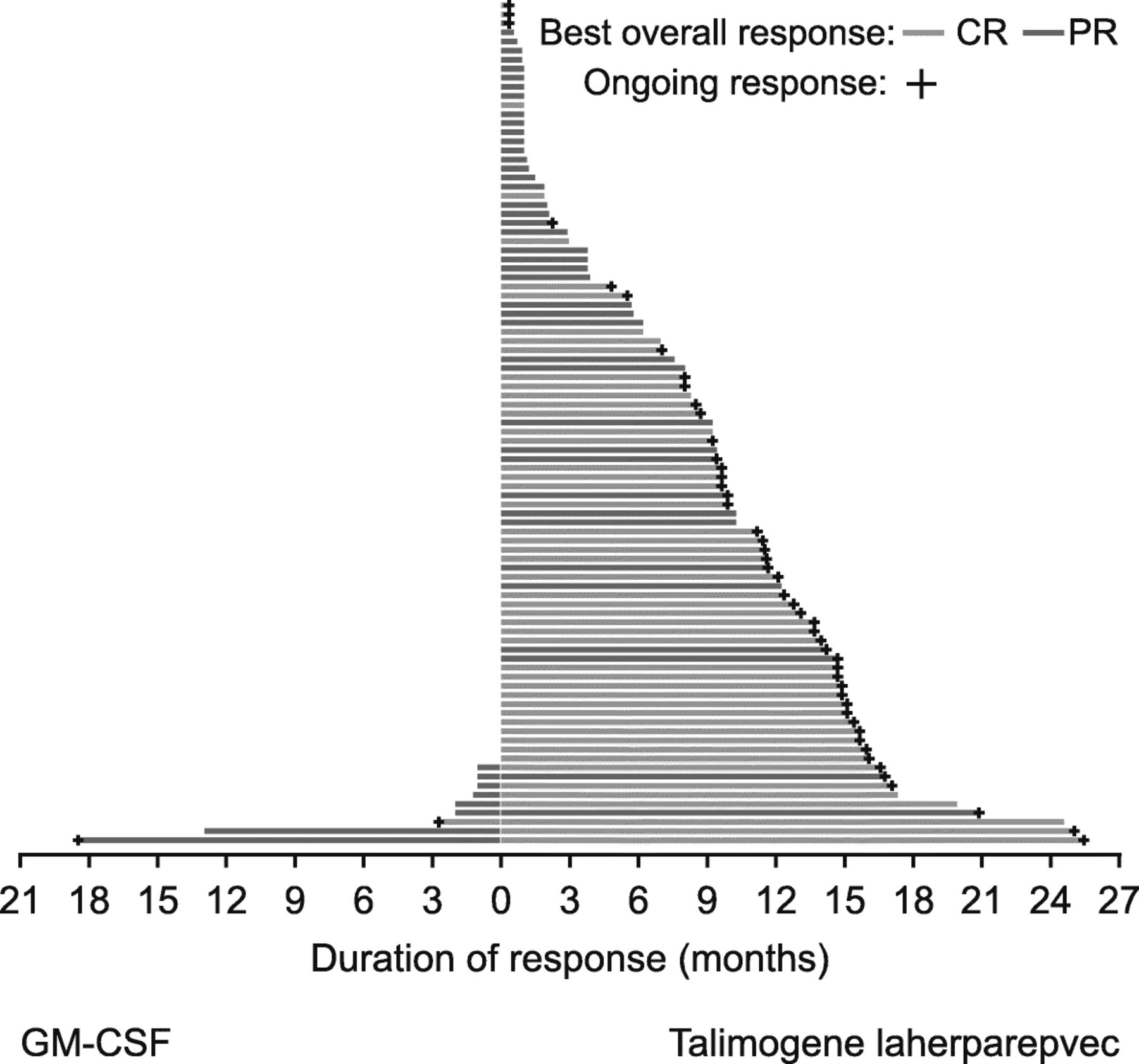
Duration of response for all patients with response per investigator assessment. Duration of response is defined as the longest individual period from entering response (PR or CR) to the first documented evidence of the patient no longer meeting the criteria for being in response or death, whichever is earlier. CR, complete response; GM-CSF, granulocyte-macrophage colony-stimulating factor; PR, partial response
Median time to CR in T-VEC-treated patients was 8.6 months (range, 2.1–42.3; Fig. 2a). Eighteen months after CR was achieved, the probability of remaining in CR was 78% (Fig. 2b). Compared with patients not achieving a CR before a landmark time of 9 months, achieving a CR was associated with an improvement in OS (Fig. 2c) and TFI (Fig. 2d). Among patients with a CR, median OS was not reached, with 88.5% (74–95) estimated to survive at a landmark analysis of 5 years. Overall, 72% of patients who achieved a CR were free from recurrence of melanoma 3 years after achieving a CR (Fig. 2e). Table 2 summarises baseline demographics and disease characteristics in T-VEC-treated patients achieving CR. Following adjustment for potential confounding factors using multivariate analysis, achievement of CR with T-VEC was significantly associated with an earlier stage of metastatic disease (Stage IIIB-IVM1a) and a baseline tumor burden of < 14.5 cm2 (Fig. 2f).

Analyses of CR in stage IIIB–IVM1c melanoma. a Time to achieve CR in patients treated with talimogene laherparepvec; b Duration of CR in patients treated with talimogene laherparepvec; c Kaplan-Meier plot of OS in patients who achieved a CR versus patients who did not achieve a CR prior to a landmark time of 9 months; d Kaplan-Meier plot of TFI in patients who achieved a CR versus patients who did not achieve a CR prior to a landmark time of 9 months; e RFS after achieving a CR with talimogene laherparepvec; f Factors associated with achieving CR with talimogene laherparepvecf. aCR duration was defined as the interval from the initial date of CR to the first response of non-CR. Ongoing CRs were censored at the date with a CR. The longest interval was utilized due to multiple CR intervals. Median follow-up for CR duration = 7 months (range < 1 to 20 months). bFor landmark analyses, OS was calculated from the landmark time of 9 months after randomization to death. Unadjusted hazard ratios and log-rank P-values are shown. cTFI was defined as the interval from the last dose of study therapy and the first dose of systemic therapy categorized as chemotherapy/targeted agent or immunotherapy. The TFI analysis was limited to treated patients with tumor assessments ≥9 months. Unadjusted hazard ratios (HR) and log-rank P-values are shown. dRFS after achieving a CR was calculated from date of CR to date of recurrence, death due to disease progression, or start of new anti-melanoma therapy. Median follow-up for RFS = 31 months (range 1 to 53 months). e14.5 cm2 was the median tumor burden. fPatients treated with talimogene laherparepvec who achieved CR (n = 50) versus those who did not (n = 245) using logistic regression models. AJCC, American Joint Committee on Cancer; CI, confidence interval; CR, complete response; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; ITT, intent-to-treat; NE, not evaluable; OR, odds ratio; OS, overall survival; RFS, recurrence-free survival; TFI, treatment-free interval
Characteristics of patients treated with talimogene laherparepvec in OPTiM by complete response and partial response (per investigator assessment)a
After five more months of follow-up versus the primary analysis of OS [4], one additional survival event occurred. Median OS was 23.3 months (95% CI, 19.5–29.6) with T-VEC and 18.9 months (95% CI, 16.0–23.7) with GM-CSF (Fig. 3a). Reduction in the risk of death was 21% with T-VEC versus GM-CSF (unstratified HR, 0.79 [95% CI, 0.62–1.00]; P = 0.0494 [descriptive]). Estimated 5-year survival in the T-VEC arm was 33.4% (Table 1). Subgroup analyses that were performed to investigate the relative effects of treatment across several key covariates for OS are shown in Fig. 3e. When the 18 patients who did not receive allocated treatment were excluded (T-VEC arm, n = 4; GM-CSF arm, n = 14), median OS in the final analysis dataset was 24.5 versus 18.9 months for T-VEC versus GM-CSF (HR, 0.78; P = 0.0439 [descriptive]; Fig. 3f).

{kind=link}
{kind=link}
{kind=link}
Final planned analyses of OS. a Final OS in the intent-to-treat population; b Final OS in patients with stage IIIB/C melanoma; c Final OS in patients with stage IIIB-IVM1a melanoma; d Final OS in patients with stage IVM1b/c melanoma; e Exploratory subgroup analyses of final OS (intent-to-treat population); and f Final OS in the treatment-received population (all randomized patients excluding those who did not receive allocated treatment; n = 4 in the talimogene laherparepvec arm; n = 14 in the GM-CSF arm). a P-values are descriptive and represent the statistical significance of the treatment difference within the subgroup from log-rank test unless otherwise stated (*P < 0.05). CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; GM-CSF, granulocyte-macrophage colony-stimulating factor; HR, hazard ratio; NE, not estimable; OS, overall survival; T-VEC, talimogene laherparepvec
According to an ad-hoc sensitivity analysis for OS accounting for subsequent systemic anti-cancer treatment (including ipilimumab, vemurafenib, dabrafenib, trametinib or an anti-PD-1), there was a 27% reduction in the risk of death for T-VEC versus GM-CSF (unadjusted HR, 0.73; 95% Cl, 0.59–0.92; P = 0.0069 [descriptive]).
Stage IIIB–IVM1a disease
Effects of T-VEC on DRR, ORR, CR and DCR were more pronounced in stage IIIB–IVM1a melanoma (28.8% DRR, 46.0% ORR and 79.1% DCR) than in more advanced disease (Table 1). Overall, 46/50 (92%) CRs occurred in stage IIIB–IVM1a melanoma (Tables 1 and 2). In T-VEC-treated patients, the CR rate in stage IIIB–IVM1a disease was 28.2% (46/163) and the median time to CR was 8.5 months (range, 2.1–42.3).
Effects of T-VEC on OS were particularly pronounced versus GM-CSF among patients with stage IIIB/C (HR, 0.48, P < 0.05 [descriptive]; Fig. 3b) and stage IIIB–IVM1a disease (HR, 0.56; 95% CI, 0.40–0.79; P < 0.001 [descriptive]; Fig. 3c) versus the ITT population including in stage IVM1b/c disease (Fig. 3d). Estimated 5-year survival with T-VEC was 48.9% (95% CI, 40.6–56.7) in stage IIIB–IVM1a melanoma versus 15.1% (95% CI, 9.3–22.2) in stage IVM1b/c disease.
Safety
The most common AEs were fatigue, chills, pyrexia, nausea and influenza-like illness (Additional file 1: Table S1). The incidence of these was highest during the first 3 cycles and subsequently decreased (Additional file 1: Figure S1). Most AEs lasted 2–4 days. Treatment-related grade 3/4 AEs occurred in 33 (11.3%) T-VEC-treated patients and 6 (4.7%) GM-CSF-treated patients. The only grade 3/4 AE occurring in ≥2% of T-VEC-treated patients was cellulitis (2.1%) (Additional file 1: Table S1).
Immune-related AEs were reported in 24/295 T-VEC-treated patients. Vitiligo was the most frequently reported immune-related AE, occurring in 18 (6.2%) T-VEC-treated patients (and one (0.8%) GM-CSF-treated patient). All vitiligo events were grade 1/2. Median time to vitiligo onset in the T-VEC arm was 22 weeks (interquartile range, 9–36). No grade 4 immune-related AEs were reported. Four grade 3 immune-related AEs were observed: glomerulonephritis/renal failure (patient with history of partial nephrectomy due to renal cell carcinoma and streptococcal injection site cellulitis), lupus vasculitis, pneumonitis (patient with a history of ulcerative colitis) and psoriasis (patient with psoriasis history).
The Additional file 1 provides further safety information.
Discussion
OPTiM was the first phase 3 trial to demonstrate a clinical benefit with an oncolytic immunotherapy in any cancer and the largest randomized controlled trial investigating a therapeutic in unresectable stage IIIB/C melanoma. Following the previously reported analysis of the primary endpoint of DRR [4], patients continued follow-up so that a planned final analysis of OS could be performed 3 years after randomization, as reported here. With 49 months of follow-up, median OS for T-VEC and GM-CSF was in line with the primary analysis [4], and was 4.4 months longer in patients receiving T-VEC than GM-CSF (reduction in the relative risk of death versus GM-CSF: 21%; P = 0.0494) [4]. Overall, estimated 5-year survival for the T-VEC arm was 33.4%. In accordance with the primary OPTiM analysis [4], the effects of T-VEC on OS were more pronounced in patients with early metastatic melanoma (stage IIIB–IVM1a), with an estimated 5-year survival of 48.9%.
The final OPTiM data set was further analysed in the 17% of patients treated with T-VEC who achieved a CR. Once achieved, CRs were durable; the median duration was not reached over a median follow-up period of more than 4 years. Additionally, median OS in these patients was not reached and approximately 90% were estimated to be alive at 5 years. Similar to T-VEC, prolonged CR duration (once achieved) and association with survival has been reported in checkpoint inhibitor (CPI) trials [9, 10]. Our analyses showed that early metastatic melanoma (stage IIIB–IVM1a) and lower tumor burden (< 14.5 cm2) were independent predictors of achieving a CR. These findings indicate that earlier commencement of an effective treatment is important for resolution of melanoma and, in turn, long-term survival. Recent analyses also demonstrated that less advanced disease and lower tumor burden are associated with achieving a CR with CPIs [9, 10]. The median time to achieve CR among T-VEC-treated patients was 8.6 months. Prior analyses showed that almost half of patients responding to T-VEC monotherapy exhibit progression prior to the response [5, 11]. Although progression prior to response prolongs the time it takes to achieve a response, it does not impact the duration of a response once achieved [11]. Hence, if there are injectable lesion(s) remaining, T-VEC should be continued for ≥6 months unless the patient is not benefitting from treatment or another treatment is required.
As previously demonstrated [4] and confirmed here, T-VEC exhibits a tolerable safety profile with a low rate of grade 3/4 AEs. The incidence of treatment-related grade 3/4 AEs with T-VEC in OPTiM was similar to that reported for anti-programmed cell death protein-1/ligand 1 monotherapy [12–16] and lower than that observed with anti-cytotoxic T-lymphocyte-associated protein-4 monotherapy [14, 17]. However, T-VEC is not associated with the same pattern of serious immune-related AEs reported with CPI therapy, such as thyroid dysfunction, hypophysitis, adrenal insufficiency and autoimmune hepatitis [16, 18–20]. It can take months to see an improvement in these AEs and some may never resolve [16, 18–20].
Interest in the use of T-VEC combined with systemic immunotherapy has arisen due its favorable safety profile, proven efficacy as monotherapy, and potentially complementary mode of action, with an ability to activate a CD8 + -dependent systemic immune response [21]. To date, T-VEC combined with CPIs in melanoma has shown improved efficacy versus CPIs alone without notable additional safety concerns [22–25]. A phase III trial of T-VEC/placebo plus pembrolizumab is underway in unresectable stage IIIB–IVM1c melanoma (MASTERKEY 265; NCT02263508).
Even if the final OS analysis was planned, a limitation is that all final subgroup analyses were descriptive, and some were post-hoc and exploratory. Additionally, after the primary OPTiM analysis, only response assessments per investigator were collected. In contrast, in the primary analysis of OPTiM, the investigator-reported ORRs (CR + PR) were independently evaluated by a blinded endpoint-assessment committee. Nevertheless, the final analyses presented here provide important new practical insights into the use of T-VEC in patients with unresectable stage III–IV melanoma.
In conclusion, as well as demonstrating a longer-term effect on survival, this analysis confirms that T-VEC resulted in high CR rates, most notably in patients with early metastatic melanoma (stage IIIB–IVM1a). Once achieved, CRs were durable and associated with prolonged survival. The favorable clinical outcomes observed in some patients treated with T-VEC, along with its good safety profile, support continued efforts to further define its future role in melanoma as a combination partner with immunotherapy.
Funding
This trial was initially funded by BioVex, who were subsequently acquired by Amgen Inc. during the OPTiM trial. The funder was involved in the design of the trial and collection, analysis, and interpretation of data and with the development of the manuscript.
Acknowledgments
We thank all patients and investigators involved in the study (as well as the members of the adjudication, independent data monitoring, and publication steering committee). Medical writing support (including development of a draft outline and subsequent drafts in consultation with the authors, assembling tables and figures, collating author comments, copyediting, fact checking and referencing) was provided by Louise Niven, DPhil and Alice Wareham, PhD, at Aspire Scientific (Bollington, UK), and funded by Amgen Inc.
Authors’ contributions
RHIA: Data collection, data interpretation, reviewed and revised drafts of the manuscript and approved the final draft. FC: Data collection, data interpretation, reviewed and revised drafts of the manuscript and approved the final draft. KJH: Data collection, data interpretation, reviewed and revised drafts of the manuscript and approved the final draft. MRM: Data collection, data interpretation, reviewed and revised drafts of the manuscript and approved the final draft. GD: Data analysis, data interpretation, reviewed and revised drafts of the manuscript and approved the final draft. KӦ: Data analysis, data interpretation, reviewed and revised drafts of the manuscript and approved the final draft. HLK: Data collection, data interpretation, reviewed and revised drafts of the manuscript and approved the final draft.
Notes
Ethics approval and consent to participate
Study procedures were approved by the institutional review boards or ethics committees for each participating site, and all patients provided written informed consent.
Consent for publication
Not applicable.
Competing interests
Andtbacka RHI – is an employee of Birdie Pharmaceuticals and has received fees for consultation or other remuneration from Amgen and Merck; Collichio F – her institution is receiving research support from Amgen, Novartis, and Merck; Harrington K – has received consulting or advisory fees from Amgen, AstraZeneca, BMS, Merck, and Pfizer; his institution has received research grants from AstraZeneca and MSD; has served on speaker bureaus for Amgen, AstraZeneca, BMS, Merck, and MSD; Middleton M – has acted as a consultant for Amgen, AstraZeneca, Bristol-Myers Squibb, Eisai, GlaxoSmithKline, Immunocore, Lilly, Merck, Millennium, Novartis, Physiomics, Rigontec, and Roche; his institution has received research grants from Abbvie, Amgen, AstraZeneca, Bristol-Myers Squibb, Clovis, Eisai, GlaxoSmithKline, Immunocore, Merck, Millennium, Novartis, Pfizer, Rigontec, Roche, and Vertex; Downey G – former employee of Amgen; Ӧhrling K – employee and stock holder of Amgen; Kaufman HL – is an employee of Replimune, Inc. and has served on advisory board for SapVax.
- AE
- Adverse event
- AJCC
- American Joint Committee on Cancer
- CI
- Confidence interval
- CR
- Complete response
- CTCAE
- Common Terminology Criteria for Adverse Events
- DCR
- Disease control rate
- DR
- Durable response
- DRR
- Durable response rate
- ECOG
- Eastern Cooperative Oncology Group
- GM-CSF
- Granulocyte-macrophage colony-stimulating factor
- HR
- Hazard ratio
- ITT
- Intent-to-treat
- OR
- Odds ratio
- ORR
- Objective response rate
- OS
- Overall survival
- PR
- Partial response
- RFS
- Recurrence-free survival
- TFI
- Treatment-free interval
- T-VEC
- Talimogene laherparepvec
References
Footnotes
Data sharing statement There is a plan to share data. This may include de-identified individual patient data for variables necessary to address the specific research question in an approved data-sharing request; also related data dictionaries, study protocol, statistical analysis plan, informed consent form, and/or clinical study report. Data sharing requests relating to data in this manuscript will be considered after the publication date and 1) this product and indication (or other new use) have been granted marketing authorization in both the US and Europe, or 2) clinical development discontinues and the data will not be submitted to regulatory authorities. There is no end date for eligibility to submit a data sharing request for these data. Qualified researchers may submit a request containing the research objectives, the Amgen product(s) and Amgen study/studies in scope, endpoints/outcomes of interest, statistical analysis plan, data requirements, publication plan, and qualifications of the researcher(s). In general, Amgen does not grant external requests for individual patient data for the purpose of re-evaluating safety and efficacy issues already addressed in the product labeling. A committee of internal advisors reviews requests. If not approved, a Data Sharing Independent Review Panel will arbitrate and make the final decision. Upon approval, information necessary to address the research question will be provided under the terms of a data sharing agreement. This may include anonymized individual patient data and/or available supporting documents, containing fragments of analysis code where provided in analysis specifications. Further details are available at the following: http://www.amgen.com/datasharing.
Electronic supplementary material The online version of this article (10.1186/s40425-019-0623-z) contains supplementary material, which is available to authorized users.