Article Text

Abstract
Background Response rates to single agent immune checkpoint blockade in unselected pretreated HER2−negative metastatic breast cancer (MBC) are low. However, they may be augmented when combined with chemotherapy.
Methods We conducted a single-arm, phase II study of patients with triple negative (TN) or hormone receptor-positive endocrine-refractory (HR+) MBC who were candidates for capecitabine. Patients were treated with pembrolizumab 200 mg intravenously day 1 and capecitabine 1000 mg/m2 by mouth twice daily on days 1–14 of a 21-day cycle. The primary end point was median progression-free survival (mPFS) compared with historic controls and secondary end points were overall response rate (ORR), safety and tolerability. The study had 80% power to detect a 2-month improvement in mPFS with the addition of pembrolizumab over historic controls treated with capecitabine alone.
Results Thirty patients, 16 TN and 14 HR+ MBC, were enrolled from 2017 to 2018. Patients had a median age of 51 years and received a median of 1 (range 0–6) prior lines of therapy for MBC. Of 29 evaluable patients, the mPFS was 4.0 (95% CI 2.0 to 6.4) months and was not significantly longer than historic controls of 3 months. The median overall survival was 15.4 (95% CI 8.2 to 20.3) months. The ORR was 14% (n=4), stable disease (SD) was 41% (n=12) and clinical benefit rate (CBR=partial response+SD>6 months) was 28% (n=8). The ORR and CBR were not significantly different between disease subtypes (ORR 13% and 14%, CBR 25% and 29% for TN and HR+, respectively). The 1-year PFS rate was 20.7% and three patients have ongoing responses. The most common adverse events were low grade and consistent with those seen in MBC patients receiving capecitabine, including hand-foot syndrome, gastrointestinal symptoms, fatigue and cytopenias. Toxicities at least possibly from pembrolizumab included grade 3 or 4 liver test abnormalities (7%), rash (7%) and diarrhea (3%), as well as grade 5 hepatic failure in a patient with liver metastases.
Conclusions Compared with historical controls, pembrolizumab with capecitabine did not improve PFS in this biomarker unselected, pretreated cohort. However, some patients had prolonged disease control.
Trial registration number NCT03044730.
- immunology
- oncology
- breast neoplasms
- programmed cell death 1 receptor
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Patients with hormone receptor-positive (HR+) HER2−negative (HER2−) endocrine-refractory and triple negative (TN) metastatic breast cancer (MBC) are treated with sequential chemotherapy.1 2 The median overall survival (mOS) with first-line chemotherapy in HER2− MBC is <2 years, indicating a large unmet need for novel therapeutic approaches.3 4 Capecitabine is often used as an early line of chemotherapy based on its efficacy, toxicity profile without significant cumulative toxicity and oral administration.5
Studies of pembrolizumab monotherapy, an antiprogrammed death (PD)-1 immune checkpoint inhibitor (ICI), have demonstrated improved overall response rates (ORR), progression-free survival (PFS) and OS with some patients having durable disease control in several malignancies.6 7 ICI monotherapy in metastatic breast cancer (MBC) has generally had low response rates.8–14 In previously treated TN MBC, ORR range from 5% to 10% in unselected patients, but reaches up to 25% in biomarker selected patients. In HR+, HER2− endocrine-refractory MBC, that is, programmed death-ligand 1 (PD-L1)-positive ORR was 12%.12 Some long-term responses have been seen in both cohorts. Response rates are higher in earlier lines of therapy, potentially related to less iatrogenic immunosuppression and lower tumor burden.13 15
Combination chemo-immunotherapy has demonstrated safety and tolerability with improved ORR, PFS and OS in other malignancies.16 In a landmark study, the addition of anti-PD-L1 blockade with atezolizumab to chemotherapy (nab-paclitaxel) for first-line therapy in TN MBC resulted in improved PFS and OS in the PD-L1-positive cohort.15 Chemo-immunotherapy may have additive or even synergistic effects, with chemotherapy potentially producing neoantigens and disrupting mechanisms of tumor immune evasion (disrupting T-regulatory cell and myeloid-derived suppressor cell activity and promoting tumor cell recognition).17 Data from studies of capecitabine and anti-PD-1 agents support the safety of the combination.18 19
The significant unmet need to improve outcomes, the low response rates to ICI monotherapy, the use of capecitabine as a standard early chemotherapy in MBC when patients are likely less immunosuppressed and the tolerability of chemo-immunotherapy in other trials provide the rationale for this phase II study of pembrolizumab and capecitabine in HR+ HER2− endocrine-refractory or TN MBC.
Patients and methods
Patients
Patients with HR+HER2− endocrine-refractory or TN MBC were included in this trial. Patients with HR+ HER2− disease must have had progression on one or more lines of endocrine therapy. Patients were >18 years, had an Eastern Cooperative Oncology Group performance status of 0–2 and adequate organ function. Those with active central nervous system disease, prior capecitabine, a history of autoimmune disease, active pneumonitis or prior severe pneumonitis requiring steroids or gastrointestinal disease that may impair capecitabine absorption were excluded.
Trial design and procedures
This was an open-label, single-arm, phase II study conducted at Northwestern University. After initial screening, patients were treated with pembrolizumab 200 mg intravenously day 1 of a 21-day cycle and capecitabine 1000 mg/m2 by mouth twice daily days 1–14 of a 21-day cycle. Toxicities were assessed after each cycle and response assessment by tumor imaging occurred every three cycles. Treatment continued until disease progression, unacceptable toxicity, withdrawal from the study, failure to adhere to recommendations or death. Treatment beyond radiographic progression was permitted with consent of patient in cases of no clinically significant change, no change in performance status or no rapid change or threat to vital organs.
The primary end point of PFS compared with historic controls and secondary end point of ORR were assessed by RECIST V.1.1 in the entire patient population and by subgroup (HR+ HER2− hormone-refractory and TN). A secondary end point of safety and tolerability was evaluated for all patients who received the study therapy by assessing adverse events using the Common Terminology Criteria for Adverse Events V.4.03. ORR and PFS by immune-RECIST (i-RECIST) was evaluated as an exploratory end point. Additionally, clinical benefit rate (CBR) defined as partial response (PR) and stable disease (SD) for > 6 months was assessed.
When tumor tissue was available from within 2 months prior to registration, a blinded external laboratory and pathologist assessed PD-L1 expression by immunohistochemistry (IHC) using the Merck 22C3 antibody, reported as a percentage 0%–100%. PD-L1 positivity was defined as an IHC score >1+ for >1% of tumor cells. The modified proportion score of overall per cent cells expressing PD-L1 including lymphocytes and tumor cells, excluding staining of the surrounding stroma, was also evaluated. Tumor infiltrating lymphocytes (TILs) were assessed by H&E stain and scored on a scale of 0–3, with scores of 2 or 3 being considered high. Additionally, pathologists reported the presence of a stromal interface by a qualitative assessment of whether there was a distinct pattern of PD-L1 membrane stained cells within the stroma bordering tumors nests at low power and the majority of stained cells appear as macrophages at high power.
Statistical approach
The trial was designed to detect a clinically significant increase in PFS by 2 months from historic controls of 3 months in patients with prior therapy to 5 months.20–22 With 27 evaluable patients, there was an 80% power to detect this difference with a one-tailed z-test at p<0.05. Categorical variables were compared between groups via Fisher’s exact test and continuous variables were compared between groups via the Wilcoxon rank-sum test. Survival was compared using the log rank test.
Results
From May 2017 to March 2018, 30 patients were enrolled at Northwestern University (table 1). One patient in the TN cohort was taken off study after one cycle because of failure to comply with capecitabine dosing recommendations and was not evaluable for the primary end point of PFS or for response. All patients were analyzed for safety and toxicity end points. The median age was 51 years. All patients with HR+ endocrine-refractory and 88% of patients with TN MBC had visceral disease. Patients had a median of one line of prior systemic therapy for metastatic disease (range 0–6), with a median of two lines (range 0–4) in the HR+ endocrine-refractory and one line (range 0–6) in the TN cohorts. This was the first line of systemic therapy for MBC for five TN and one HR+ patients, all of whom had received prior therapy for early stage disease. The study therapy was the second line of therapy for 11 patients, third line for 5 patients, fourth line for 5 patients and fifth or greater line for 3 patients.
Baseline characteristics
Patients received a median of five cycles of therapy. A dose reduction of capecitabine was required in 43% (n=13) of patients, of whom three patients required two dose-level reductions. The most common reason for dose reduction was hand-foot syndrome. Pembrolizumab was interrupted for toxicity in 23% of patients. Therapy was stopped for progressive disease for 80% (n=24), toxicity for 10% (n=3), physician discretion 3% (n=1; for physician-determined clinical progression not meeting RECIST V.1.1 criteria for PD), and non-compliance 3% (n=1). One patient remains on trial.
Adverse events of any grade that occurred in at least one-third of patients that were at least possibly therapy-related were gastrointestinal (elevation in liver enzymes, nausea, diarrhea), fatigue, headache, hand-foot syndrome, pain in extremity, hematological (anemia, leukopenia, lymphopenia), hyperglycemia and hypoalbuminemia (table 2). Grade 3 or higher adverse events occurring in at least 10% of patients were an elevation in alkaline phosphatase, hand-foot syndrome, anemia and lymphopenia. One patient with HR+ endocrine-refractory MBC, liver metastases at enrollment and preserved hepatic function had rapid disease progression and liver failure after two cycles. The patient received high-dose steroids and supportive care but died shortly after.
Treatment-related toxicities
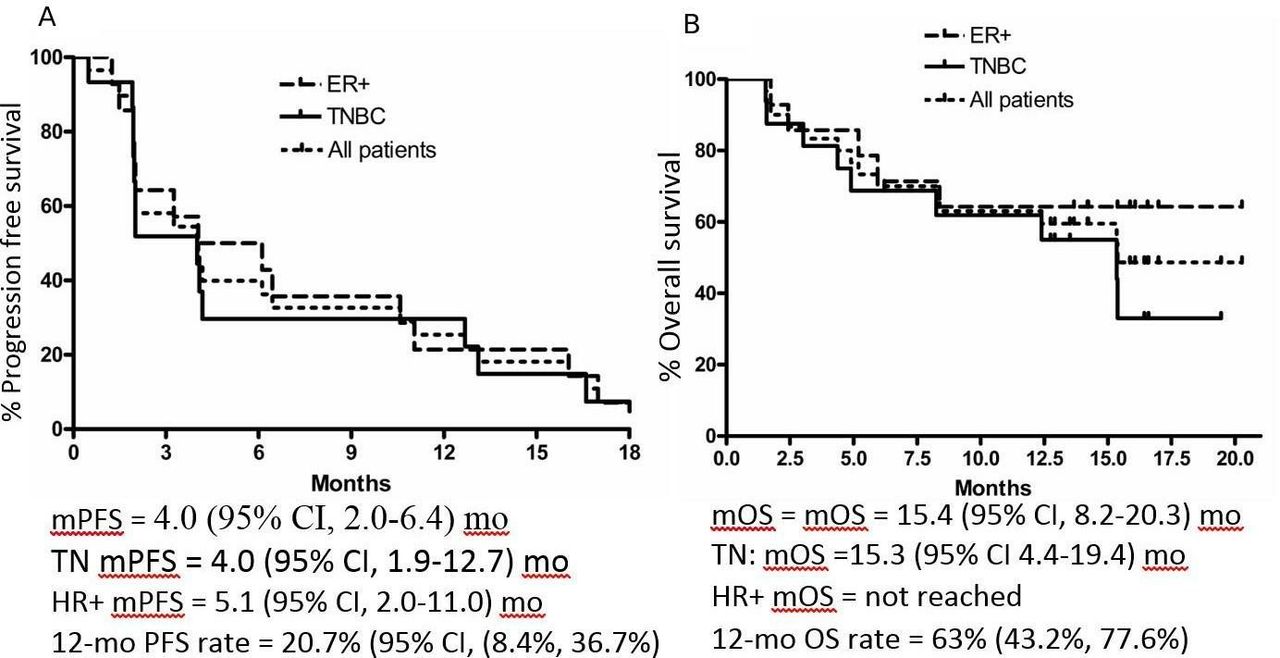
The median PFS (figure 1) was 4.0 (95% CI 2.0 to 6.4) months, which did meet the prespecified threshold of a clinically meaningful 2-month increase in PFS and was not significantly longer than historic controls of 3 months. The median PFS was similar in the HR+ endocrine-refractory and TN cohorts, 5.1 (95% CI 2.0 to 11.0) months and 4.0 (95% CI 1.9 to 12.7) months, respectively, log-rank p value=0.77. Notably, 20.7% of patients were without progression at 1 year (95% CI 8.4% to 36.7%). The median OS was 15.4 (95% CI 8.2, 20.3) months, with 63% of patients alive at 12 months (95% CI 43.2% to 77.6%). The median OS was not reached in the HR+ endocrine-refractory group and was 15.3 (95% CI 4.4 to 19.4) months in the TN group.

(A) Progression-free (PFS) and (B) overall survival (OS) in all patients and by breast cancer subtype. ER+, endocrine-refractory-positive; HR+, hormonereceptor-positive endocrine-refractory; TNBC, triple negative breast cancer.
The objective response rate (table 3, figure 2) was 14% and not significantly different between the TN and endocrine-refractory HR+ cohorts (p=0.99). Similarly, the CBR (PR+SD >6 months) was not significantly different between subgroups and was 28% in the entire cohort. Evaluation of response by i-RECIST criteria showed no differences in response rates. There were no cases of pseudoprogression and no complete responses. Among the 17 patients for whom this was the first or second line of therapy for metastatic disease, no partial or complete responses were seen, although 18% derived clinical benefit with >6 months of SD.

{kind=link}
{kind=link}
Response to capecitabine and pembrolizumab by RECIST V.1.1 criteria. HR+, hormonereceptor-positive endocrine-refractory; TN, triple negative.
Response rate
Half of patients had evaluation of tissue from a metastatic site for expression of PD-L1 and immune infiltrate (TN n=5, HR+ n=10, table 4). Tissue samples were obtained within 2 months of starting therapy and were from liver (n=7, 47%), lung (n=2, 13%), skin (n=2, 13%) and adrenal, bladder and breast (n=1 for each category, 7%). Sixty per cent of samples were PD-L1 negative (IHC score 0 for tumor cells), 70% and 40% were PD-L1 negative in HR+ endocrine-refractory and TN cohorts, respectively. TIL scores were 7%, 47%, 27%, 20% for scores 0, 1, 2 and 3, respectively. PD-L1 positivity or high TILs did not correlate with response to therapy.
Tissue immune correlatives
The median change in lymphocyte count from day 1 of treatment to day 1 of the last cycle on study was a decrease by 0.1 lymphocyte/μL. Lymphopenia was present at baseline in 52% of patients and at end of treatment in 67% of patients. There was no statistically significant difference in rate of lymphopenia in responders compared with non-responders (table 5).
Immune correlatives and clinical benefit rate based on (A) metastatic tissue sample and (B) absolute lymphocyte count
Eight patients had clinical benefit (four PR, four SD >6 months) of whom six patients remained on therapy without progression for longer than 1 year (three TN, three HR+ endocrine-refractory disease). However, one HR+ patient had only 9% expression of the estrogen receptor and 3% of the progesterone receptor. Among these patients with clinical benefit, the median lines of prior chemotherapy for metastatic disease was 1 (range 0–2). Three had a correlative tissue sample (one TN, two HR+). These patients had a PD-L1 tumor proportion score (% of tumor cells with PD-L1 IHC >1+) of 0%, 0% and 3%, and TIL scores (scale 0–3) of 2, 1 and 1 (table 4).
Discussion
Pembrolizumab with capecitabine did not improve PFS compared with historic controls in this biomarker unselected cohort that consisted of patients with prior systemic therapy. This finding is consistent with the limited efficacy of anti-PD-(L)1 monotherapy in unselected, pretreated MBC.9 11 Despite the lack of selection, 20% of patients had disease control beyond 1 year of therapy and 28% derived clinical benefit with the combination therapy.
In addition to subtype and prior therapies, PD-L1 and TILs for those with available tissue and lymphocyte count were considered in an exploratory analysis as potential biomarkers for enhanced response to therapy. Prior studies have demonstrated PD-L1 on TILs can predict for immunotherapy benefit in metastatic TNBC and studies in PD-L1-positive patients with breast cancer have higher response rates than in unselected patients.8 15 High TILs have also been associated with better clinical outcomes in metastatic TNBC.23 Lymphocyte count was explored as it may be a surrogate for immune response and may reflect degree of immunosuppression from prior therapy.24 25
No factor clearly correlated with clinical benefit including subtype (HR+ HER2− endocrine-refractory vs TN), lines of prior therapy for metastatic disease, PD-L1 status, TIL level or lymphocyte count; however, this subgroup analysis was limited by a modest patient cohort size. Future studies with larger patient cohorts and randomized designs should continue to explore potential predictors of response to identify the smaller subset of patients who may benefit from a combined chemotherapy and immunotherapy approach.
Several studies have demonstrated promising findings for chemo-immunotherapy in TNBC. Most notably, the IMpassion130 study demonstrated atezolizumab and nab-paclitaxel improved OS compared with chemotherapy alone when given as a first-line therapy in a cohort with PD-L1-positive lymphocytes >1% and TN MBC.15 This combination of capecitabine with pembrolizumab in TNBC was evaluated in a recently reported phase II study that included 14 patients in the capecitabine arm and demonstrated a 12-week ORR of 43% and mPFS of 5.6 months. The higher response rate may be related to its use in earlier lines of therapy (first-line for 79% of patients). Of note, the ORR, CBR, PFS and OS numerically favored the capecitabine-pembrolizumab cohort over the paclitaxel-pembrolizumab group.26 Additional data from early stage breast cancer studies also demonstrate the promise of chemo-immunotherapy in TNBC. The I-SPY 2 phase II trial of neoadjuvant chemotherapy with paclitaxel and pembrolizumab followed by doxorubicin and cyclophosphamide showed improvement in the estimated pathologic complete response (pCR) rate from 22.3% to 62.4% in the TN cohort.27 The KEYNOTE-522 study was a large randomized phase III trial that demonstrated the addition of neoadjuvant and adjuvant pembrolizumab to a chemotherapy regimen of a taxane+carboplatin followed by an anthracycline+cyclophosphamide with adjuvant pembrolizumab improved the pCR rate from 51.2% to 64.8%.28 Results from the phase III IMpassion132 trial evaluating atezolizomib with several chemotherapies including capecitabine as first-line therapy for TN MBC will contribute to our understanding of the use of chemo-immunotherapy in metastatic TNBC.29
For HR+ endocrine-refractory MBC, there is more limited data for chemo-immunotherapy. One phase II study of eribulin and pembrolizumab compared with pembrolizumab alone demonstrated no improvement in PFS.30 The I-SPY 2 phase II trial showed improvement in the estimated pCR rate among patients with previously untreated HR+ HER2− early stage breast cancer from 13.6% to 34.2%.27 Additionally, several ongoing trials are evaluating chemo-immunotherapy in HER2− MBC (eg, NCT02752685, UMIN000030242, NCT03371017).
Most toxicities were low grade and consistent with those expected with capecitabine monotherapy in MBC. This included elevation of liver tests, cytopenias (including lymphopenia of any grade occurring in 53% of patients), skin rash and fatigue. However, higher grade toxicities were also observed. There was one death from hepatic failure and rapid disease progression. It remains unclear whether this death was a result of rapid disease progression as can be seen in patients with MBC and liver metastases, immune-related hepatitis, a change in the character and pace of disease related to immunotherapy or a combination of these potential causes. Such an acceleration in the disease with ICI has been described in other malignancies as hyperprogressive disease, although the exact definition and relationship with immunotherapy has not been established.31–33 Future studies of immunotherapy in MBC with liver metastases should include careful monitoring of liver function and may provide added insight about whether hyperprogression is a true phenomenon observed in breast cancer.
Despite the lack of improvement in mPFS, the tolerability of the combination and noting a subset of patients with clinical benefit in the context of growing data supporting chemo-immunotherapy in MBC warrants further exploration of the combination in a more selected population (earlier line of therapy with more rigorous evaluation for predictive biomarkers). Future studies of chemo-immunotherapy in MBC are needed to identify clinical, pathological and molecular predictors of response and toxicity to identify subgroups more likely to benefit from the addition of ICI to chemotherapy.
Conclusions
Compared with historical controls, pembrolizumab with capecitabine did not demonstrate a statistically significant improvement in PFS in a biomarker unselected, pretreated cohort. However, some patients had prolonged disease control, including patients with HR+ HER2 MBC. Future studies of chemo-immunotherapy should select for factors likely to augment benefit, such as earlier lines of therapy and predictive biomarkers.
References
Footnotes
Contributors Conception and design: SJ, AR and WG. Provision of patients: LF, WG, MC, VN, DT and CAS-M. Collection and assembly of data, data analysis and interpretation: all authors. Manuscript writing: ANS and IH. Manuscript approval: all authors.
Funding This study was funded by Merck.
Competing interests No, there are no competing interests.
Patient consent for publication Not required.
Ethics approval The study was reviewed and approved by the Northwestern University IRB, STU00203215. All procedures were conducted in accordance with the Good Clinical Practice and the Declaration of Helsinki. All patients signed consent prior to any study-related procedures.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.