Article Text

Abstract
Background The clinical response to immune checkpoint inhibitors (ICIs) in only part of the treated patients, in conjunction with the potentially serious side effects associated with this type of therapy, has emphasized the need to identify biomarkers to select patients who may benefit from ICI treatment. The aim of our study was to test human leukocyte antigen (HLA) class I and II expression in melanoma metastases as potential biomarkers of response to ipilimumab and survival in patients with metastatic melanoma, since these molecules play a crucial role in the interactions of malignant cells with host’s immune system.
Materials and methods HLA class I and II antigen expression level in pretreatment surgical tissue samples (50 lymph node and 35 cutaneous or subcutaneous metastases) from 30 patients was analyzed by immunohistochemical staining with monoclonal antibodies. Expression levels were correlated to intratumoral density of lymphocytes expressing cluster of differentiation (CD)8, CD45RO, CD4, forkhead box P3 (FOXP3) and/or programmed cell death protein 1 (PD-1), to clinical response to treatment, and to patients’ survival.
Results HLA class I antigen expression level in lymph node metastases, but not in cutaneous or subcutaneous metastases was significantly correlated to density of CD8+ and CD45RO+ T cells and of lymphocytes expressing PD-1, as well as to clinical response and to patients’ survival.
Conclusions Our results corroborate the role of HLA class I expression level (alone or in combination with T-cell density values) as a predictive biomarker of response to ipilimumab in patients with melanoma. In addition, our results show that this association is influenced by the anatomic site of the metastasis used to measure the HLA class I antigen expression level.
- HLA
- immunology
- oncology
- tumors
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Immunotherapy with monoclonal antibodies (mAbs) targeting immune checkpoints has been shown to induce durable clinical responses in an increasing number of cancer types. However, only a percentage (between about 10% and 40% depending on tumor type when used as monotherapy) of the treated patients benefits from this therapy.1 Its efficacy will be greatly increased by the identification of biomarkers able to predict clinical response to therapy and by the development of strategies to counteract resistance mechanisms to immune checkpoint inhibitors (ICIs).2 3 The available evidence strongly suggests that ICI-based therapy is effective in patients bearing tumors with high mutational burden (therefore containing a large number of potential neoantigens), and showing high immunological activity (immune cell infiltration, immune response-related gene expression).1 3 4
Effective antitumor immune response is dependent on the recognition of tumor antigens by antigen-specific T lymphocytes in the context of human leukocyte antigen (HLA) class I molecules. To this end, expression of a fully functional HLA class I antigen processing machinery (APM) by tumor cells is crucial for the recognition and destruction of tumor cells by cognate cluster of differentiation (CD)8+ T cells. Defects in HLA class I APM component expression have been reported to be associated with disease progression and poor prognosis in several cancer types.5 6 Moreover, functional HLA class I APM is expected to be crucial for the success of T-cell-based immunotherapies. Mutation or loss of heterozygosity of β2-microglobulin (β2M), an essential component of the HLA class I complex, was identified as a mechanism of primary and acquired resistance to cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) and programmed cell death protein 1 (PD-1) inhibitors7–9 as well as other types of T-cell-based immunotherapies.10 However, structural mutations leading to defective HLA class I APM component expression and/or function have a frequency of less than 10%.6 Defects of HLA class I APM component expression are most frequently caused by epigenetic mechanisms.6 11 Nevertheless, the association of HLA class I protein expression with response to ICI therapy1 has been investigated only to a limited extent,12 and only two studies have addressed the association between HLA class II antigen expression on tumor cells and response to ICI.12 13
In a recent study we examined infiltration of 11 immune cell types in pretreatment surgical samples of patients with metastatic melanoma treated with ipilimumab. We found a positive association between immune cell density in lymph node metastases and response to ICI therapy for several cell types, including CD4+ and CD8+ T lymphocytes, forkhead box P3 (FOXP3+) cells, CD20+ B lymphocytes, NKp46+ NK (natural killer) cells, and cells expressing the activation markers CD134 or CD137.14 The aim of the present study was to analyze HLA class I and class II expression in the set of samples we had previously analyzed for immune cell infiltration, to correlate it with T-cell infiltration and to assess its value as a biomarker of clinical response to ipilimumab therapy and survival in patients with metastatic melanoma.
Materials and methods
Tumor samples
Archived paraffin blocks of pretreatment surgical tissue samples (50 lymph node and 35 cutaneous/subcutaneous metastases) were collected from 30 patients with metastatic melanoma who received ipilimumab treatment between 2010 and 2014. The clinical characteristics of this patient cohort, previously used to assess the predictive value of tumor-infiltrating immune cells, have been described in detail elsewhere.14 Eighteen patients received ipilimumab treatment in the Expanded Access Program, three patients after drug commercialization, and nine patients participated in the CA-184-169 trial. Sample collection was restricted to metastases surgically removed within 1 year before ipilimumab treatment to reduce potential changes in immune status during the time elapsed between surgery and ipilimumab therapy.
Monoclonal antibodies
The mouse mAb HCA2, recognizing β2M-free HLA-A (excluding HLA-A24), HLA-B7301 and HLA-G heavy chains, mAb HC10, recognizing β2M-free HLA-A3, HLA-A10, HLA-A28, HLA-A29, HLA-A30, HLA-A31, HLA-A32, HLA-A33, HLA-B (excluding HLA-B5702, HLA-B5804 and HLA-B73) and HLA-C heavy chains, β2M-specific mAb NAMB1 and mAb LGII-612.14 recognizing the β chains of HLA-DR, DQ, DP antigens were developed and characterized as described.15–17 The mAb EMR8-5, recognizing an epitope expressed by HLA-A, B, and C heavy chains, was purchased from Abcam.
Immunohistochemical staining and evaluation
Tissue sections were stained with mAbs, using standard methodology previously described.14 Staining was detected using the SS One-Step Polymer-HRP IHC Detection System (BioGenex) and 3-amino-9-ethylcarbazole (Vector Laboratories). Sections were counterstained with hematoxylin. Staining with HLA class I subunit-specific mAbs was scored as 0, 1, and 2 when the percentage of stained melanoma cells was <25%, 25%–75%, and >75%, respectively, based on the criteria established by the 12th International Histocompatibility Workshop (1996). In the case of HLA-DR, DQ, DP, the percentage of the area displaying positive tumor cell staining was determined in the metastases. For patients with more than one metastasis available, the average scores were calculated for each marker. Evaluation was done independently by two investigators who were blinded to the clinical information, and the mean value of their separate scores was used for the analysis. The proportion of patients with high HLA class I expression on melanoma cells was also calculated, using cut-off values based on the median of each marker in the whole patient cohort, with minor adjustment for better discriminating power in the case of NAMB1 (scores of 1.5 for the epitopes recognized by mAbs HCA2 and HC10, 1.9 for EMR8-5, and 1.2 for NAMB1). Cut-off values of 1% and 10% were used for the epitope recognized by mAb LGII-612.14.
Statistical analysis
Associations between the proportion of patients with high HLA expression and response to ipilimumab were calculated using the χ2 test. Correlation of HLA expression levels with immune cell infiltration was evaluated using the Pearson test; immune cell density values (cell number/mm2) have been derived from our previous study.14 To assess intrapatient heterogeneity, coefficient of variation was calculated [CV=(SD/mean)×100]. Analysis of survival, evaluated from start of ipilimumab treatment, was performed by the Kaplan-Meier method, using the generalized Wilcoxon test. Cox regression analyses were performed using mean HLA expression scores and other clinicopathological variables. Statistics were calculated using the BMDP Statistical Software Package.
Results
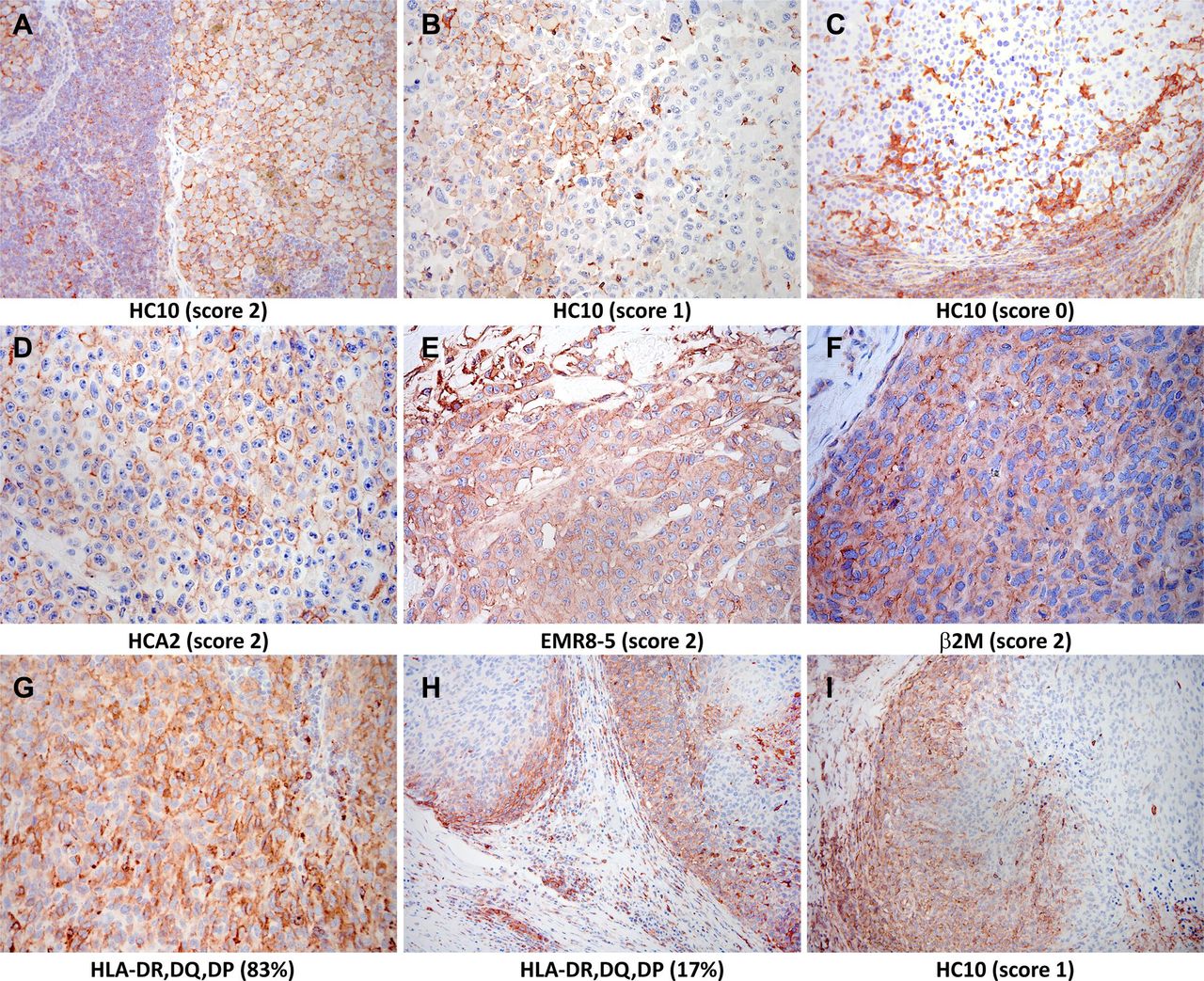
Surgically removed lymph node and cutaneous/subcutaneous melanoma metastases were analyzed for HLA expression. There was no difference between lymph node and cutaneous/subcutaneous metastases in HLA class I expression scores obtained by staining with mAb HCA2 (mean±SD, 1.3±0.8 vs 1.3±0.7), HC10 (1.3±0.7 vs 1.2±0.8), EMR8-5 (1.5±0.7 vs 1.6±0.6), or NAMB1 (1.2±0.8 vs 1.1±0.7). In the case of HLA class II expression, with the exception of one patient whose lymph node metastases showed high percentage of stained melanoma cells (43% on average, range 3%–86%; figure 1G), the majority (62%) of metastases were not stained by mAb LGII-612.14, irrespective of anatomic site. At least 1% of melanoma cells were stained by mAb LGII-612.14 in 41% of nodal and in 34% of cutaneous/subcutaneous metastases, while more than 10% of cells were stained in 16% and 6%, respectively. In many cases showing heterogeneous staining for HLA class I or class II, higher labeling was observed in tumor cells in the proximity of inflammatory cells at the margin of the metastases; this finding is consistent with locally induced HLA expression (figure 1H,I). In the 18 patients with more than one metastasis analyzed (median of 4 (range 2–9) metastases), the average CVs indicating intrapatient heterogeneity were 32.8%, 42.0%, 29.9%, 41.1%, and 37.3% for staining by mAbs HCA2, HC10, EMR8-5, NAMB1, and LGII-612.14, respectively.
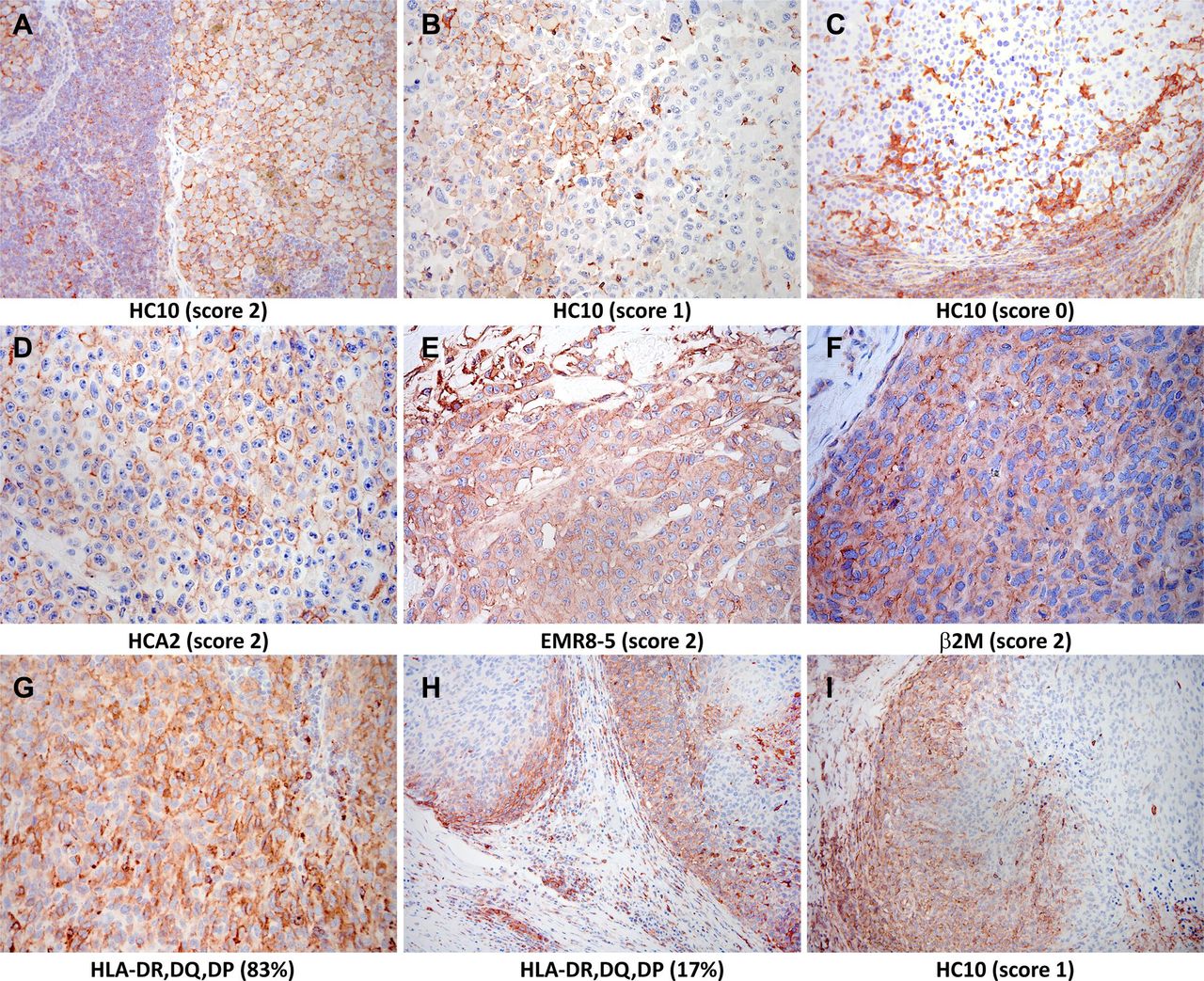
Immunohistochemical staining of melanoma metastases with human leukocyte antigen-specific monoclonal antibodies (mAbs) (3-amino-9-ethylcarbazole, red). Staining with (A–C) mAb HC10 (scores 2, 1, and 0, respectively); (D) mAb HCA2 (score 2); (E) mAb EMR8-5 (score 2); (F) mAb NAMB1 (score 2); (G) mAb LGII-612.14 (evaluated as 83% expression); and (H, I) heterogeneous staining with mAb LGII-612.14 (H) and mAb HC10 (I) detected mainly in tumor cells at the margin of the metastases. β2M, β2-microglobulin.
HLA class I and class II expression levels in lymph node metastases showed positive correlation with intratumoral density of CD8+ and CD45RO+ T cells (table 1), but not with that of CD4+ or FOXP3+ cells (not shown). Furthermore, HLA expression was significantly correlated with the density of lymphocytes expressing PD-1 (table 1). On the other hand, in subcutaneous/cutaneous metastases HLA class I expression level was not correlated with the extent of T-cell infiltration, while HLA class II expression was correlated with CD8+, CD45RO+, and PD-1+ cell density (table 1).
Correlation between tumor cell HLA antigen expression scores and T-cell density in melanoma metastases
Patients were divided into two groups according to the clinical response to ipilimumab therapy: “responders,” including 11 patients displaying complete or partial response, or stable disease for more than 6 months, and “non-responders,” including 19 patients with disease progression or stable disease for ≤6 months. The proportion of patients with high mean tumor cell HLA class I scores in lymph node metastases was significantly higher in “responders” compared with “non-responders,” when results of staining with mAb EMR8-5 were analyzed. A similar difference was observed for the results obtained with mAb HC10 and NAMB1, although the difference did not reach the level of statistical significance (table 2). The metastases from the three patients with complete and from the one with partial response displayed high reactivity with mAb HC10. In contrast, the frequency of metastases with high reactivity with mAb HC10 was significantly lower in patients with stable or progressive disease; high staining was found in only 6 of the 15 patients. Similar results were obtained with mAb EMR8-5, although the difference was not statistically significant (table 2). No differences in HLA class I expression were found between “responders” and “non-responders” when cutaneous/subcutaneous metastases were analyzed (table 2). Analysis of the reactivity pattern of the metastases with the four HLA class I subunit-specific mAbs showed that the number of metastases strongly stained by most of the mAbs tested was higher in the cohort of patients with complete or partial response compared with those with stable or progressive disease following ipilimumab treatment. This difference was observed when lymph node metastases and cutaneous/subcutaneous metastases were analyzed as individual groups or as a whole group. In contrast, HLA class II expression showed no association with treatment response in any of the patient groups studied. Evaluation of HLA class I or class II scores in combination with density values of CD8+ or CD45RO+ T cells did not increase the predictive effect of CD8+ or CD45RO+ T-cell density alone, described in our previous paper.14
Relationship of treatment response with proportion of patients with high mean tumor cell HLA class I scores in metastases (χ2 test)
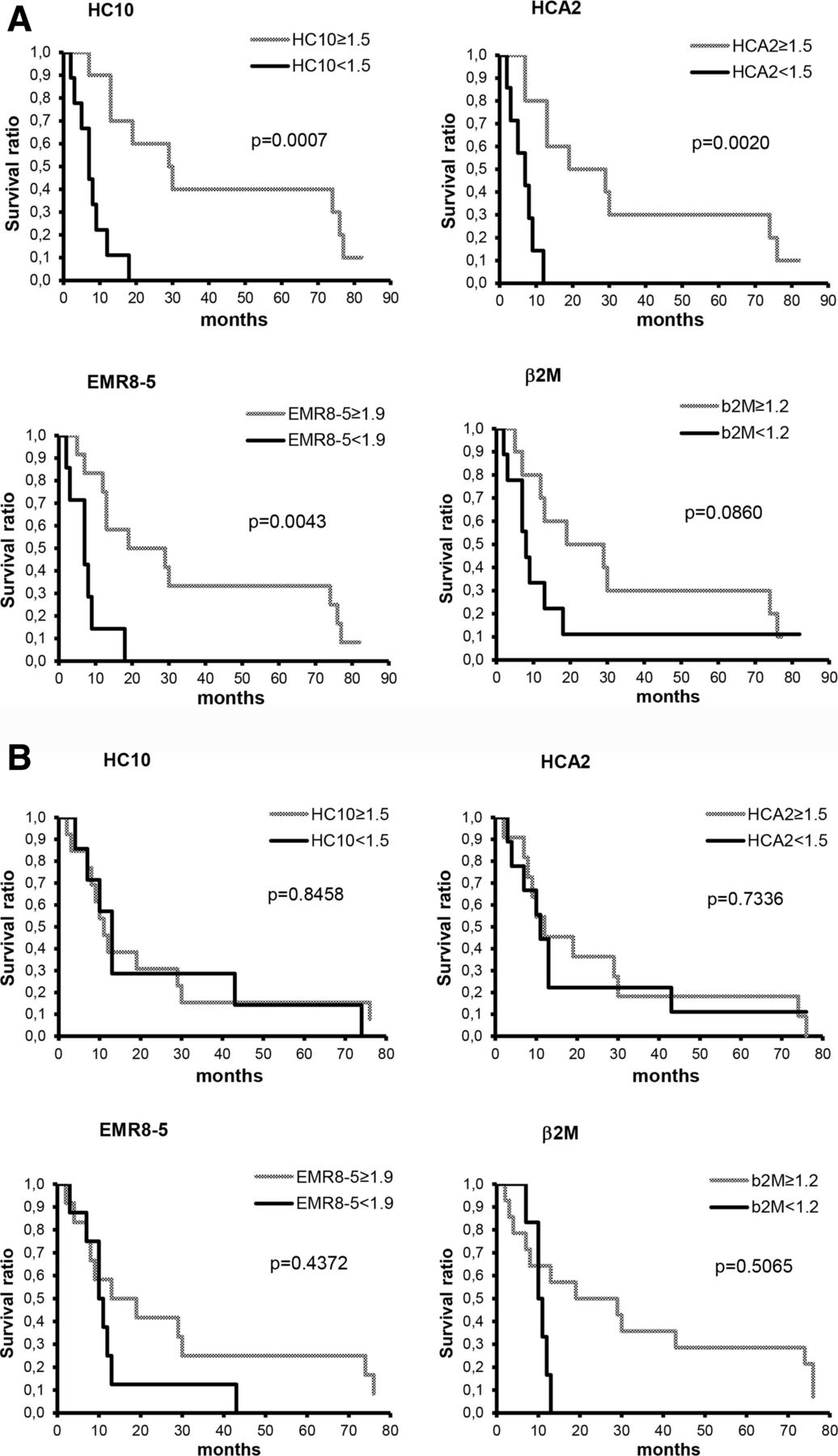
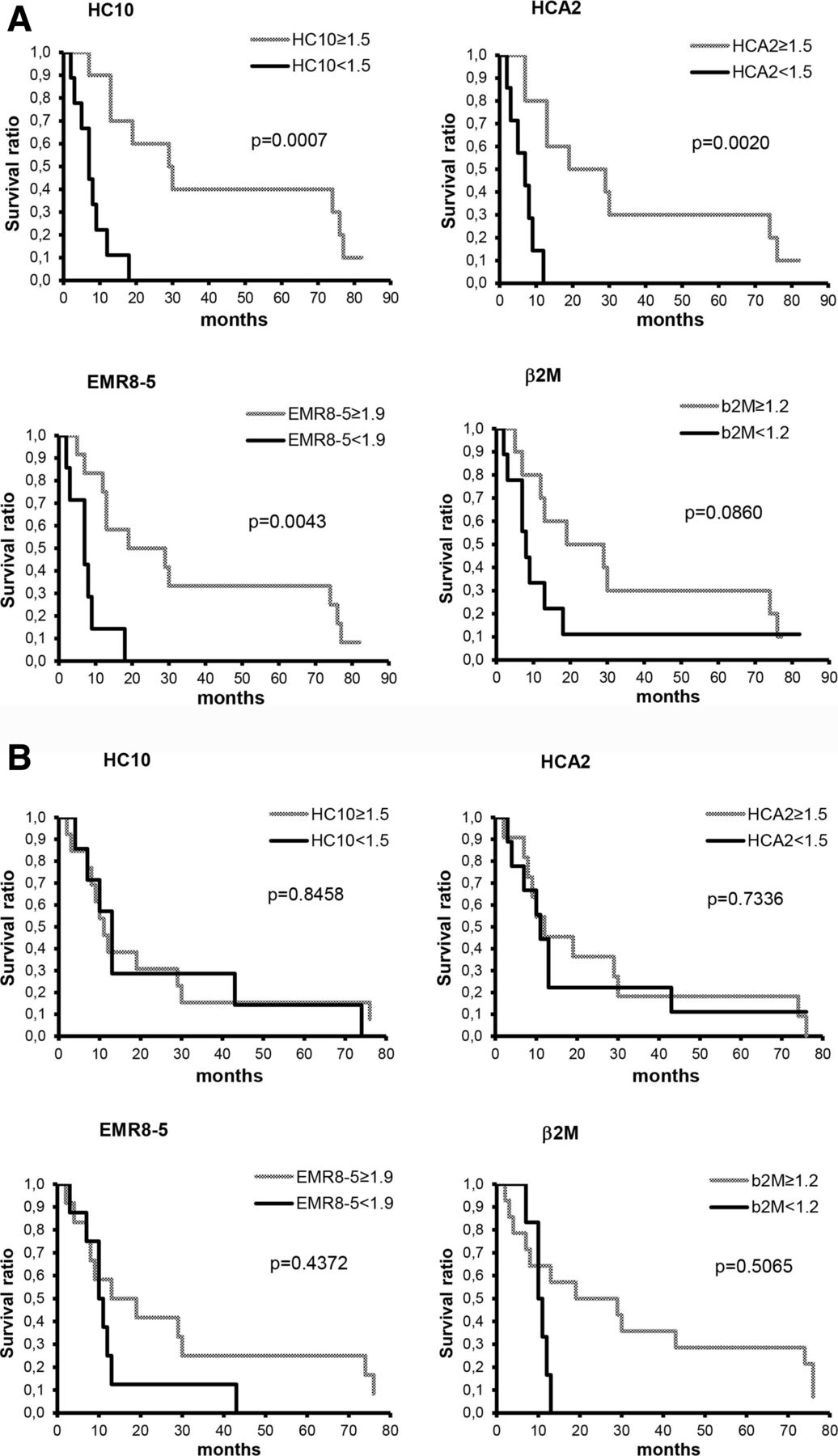
Overall survival by Kaplan-Meier curve was significantly associated with HLA class I expression level in lymph node metastases but not with that in cutaneous/subcutaneous metastases (figure 2). Prognostic correlates of HLA class I expression scores evaluated as continuous variables, together with patients’ age and gender, Eastern Cooperative Oncology Group (ECOG) status, lactate dehydrogenase (LDH) level, number of organs involved and disease stage, were also analyzed using Cox’s proportional hazards model. In univariate analysis evaluating lymph node metastatic cases, scores obtained with mAb HCA2 (p=0.0456) and with mAb HC10 (p=0.0210), besides ECOG status (p=0.0009) and LDH (p=0.0227) were significantly associated with overall survival. In multivariate analysis, only ECOG status was significantly (p=0.001) associated with survival. When evaluated in cutaneous/subcutaneous or in all metastases analyzed, HLA class I expression was not significantly associated with survival in either univariate or multivariate analysis; in the latter groups only LDH level was an independent biomarker of survival (p=0.001 and p=0.000, respectively). When the combined score obtained with the four HLA class I subunit-specific mAbs was included in the analysis instead of the scores obtained with each mAb, a concordant high expression in the lymph node metastases of the majority of the epitopes analyzed was significantly (p=0.0017) associated with survival in univariate, but not in multivariate analysis. The same association was found when the patients were analyzed as a whole group (p=0.0240). In contrast, HLA class II expression was not significantly associated with survival either in univariate or in multivariate analysis. Evaluation of HLA class I scores in combination with CD8+ or CD45RO+ cell density values in lymph node metastases using univariate Cox regression analysis revealed that high HLA class I expression combined with high T-cell density was associated with markedly better survival compared with all other cases analyzed together (p=0.0001, p=0.0021, p=0.0033, p=0.0002, p=0.0053, and p=0.0012 in the case of CD45RO/HC10, CD45RO/HCA2, CD45RO/EMR8-5, CD8/HC10, CD8/HCA2, and CD8/EMR8-5, respectively). High CD45RO/HC10 combination proved to be a significant independent predictor of good prognosis in multivariate analysis (p=0.000). In the case of cutaneous/subcutaneous metastases, CD45RO/EMR8-5 and CD45RO/NAMB1 combinations proved to be significant factors (both p=0.0128) in univariate but not in multivariate analysis.
{kind=link}
{kind=link}
Kaplan-Meier curves of overall survival for patients with melanoma subdivided according to staining with human leukocyte antigen class I-specific monoclonal antibodies in lymph node (A) and cutaneous/subcutaneous metastases (B).
Discussion
The efficacy of ICI-based therapies in only a proportion of treated patients has been a major stimulus to search for biomarkers which could identify patients likely to benefit from this therapy. A number of variables have been tested. Among them, programmed death ligand 1 (PD-L1) expression in tumors has been approved by Food and Drug Administration as a companion diagnostic marker to select patients to be treated with PD-1/PD-L1 inhibitors.18 Moreover, emerging data indicate the importance of tumor-derived and host-derived factors involved in antitumor immune reactions, such as neoantigen expression level, systemic and local immune activity, in influencing the clinical efficacy of ICIs.1 3 4 However, limited attention has been paid to the value of HLA class I expression level on tumor cells as a biomarker to predict clinical responses to ICI-based therapy. This is surprising in light of the crucial role played by HLA class I antigens in the presentation of tumor antigen-derived peptides to cognate cytotoxic T cells unleashed by ICI and the relatively high frequency of defects in HLA class I expression by tumor cells.5 6 11
The paucity of information in the literature about the role of HLA class I defects in the clinical response to ICI-based therapy has prompted us to investigate the association between HLA class I expression in metastases and clinical responses in a cohort of patients treated with ipilimumab. To the best of our knowledge, this association had been investigated only by Rodig et al.12 Their study and ours share some similarities, but display also some differences. Both studies used the mAb EMR8-5 recognizing an epitope shared by the gene products of HLA-A, B, and C loci. Both have reached the conclusion that HLA class I expression level in metastases is significantly associated with clinical response to ipilimumab. In addition, our study which has used also HLA class I subunit-specific mAbs suggests that the expression level of HLA-B and C antigens may play a more important role than that of HLA-A antigens in the clinical response to anti-CTLA-4 mAb therapy. Provided that this difference is not caused by the distinct characteristics of the two mAbs used to measure the expression level of the gene products of HLA-A and of HLA-B and C loci, it may reflect the different characteristics of the tumor antigens presented by HLA-A antigens and by HLA-B and C antigens including but not limited to their range of specificity and to their immunogenicity.
An additional difference between our study and that of Rodig et al 12 is that in the latter study biopsy samples obtained from metastases in several distinct anatomic sites were included. In contrast, we evaluated whole tumor sections (generally representing larger portions of the tumors compared with biopsies), from surgical samples of several metastases per patient when available, to reduce the confounding effect of heterogeneous expression of HLA antigens. Moreover, we analyzed only metastatic samples derived from two anatomic sites, lymph nodes and cutaneous/subcutaneous tissues. Our study has shown that HLA class I expression level in lymph node metastases, but not that in cutaneous/subcutaneous ones, is associated with clinical response and survival of patients treated with ipilimumab. Tumor cell expression of HLA class II did not show correlation with outcome of ipilimumab therapy, similarly to earlier studies where melanoma-specific HLA class II expression predicted response to anti-PD-1, but not to anti-CTLA-4 treatment.12 13
Our data are compatible with the possibility that epigenetic changes induced by the tumor microenvironment in HLA class I antigen expression on melanoma cells have a major impact on its role as a biomarker of clinical response to ICI-based therapy. In our previous investigation on the same patient cohort,14 we found more pronounced effect of immune cell infiltration in nodal versus cutaneous/subcutaneous metastases on the outcome of ipilimumab therapy. Likewise, in the present study response to ipilimumab and survival were significantly associated with HLA class I expression, only when lymph node metastases were analyzed. Also, HLA class I expression level in lymph node metastases, but not in cutaneous or subcutaneous ones was significantly correlated to T-cell density. These results suggest different biology of metastases of lymph nodes versus non-lymphoid organs, presumably due to the distinct immune milieu. Tissue-specific differences in the tumor microenvironment may influence growth and progression of tumors as well as their therapeutic sensitivity.19–21 Variation in immune cell infiltration and antigen expression according to metastatic site has been reported in melanoma and other tumor types.20–23 Immunotherapy biomarker studies, however, generally do not take into consideration anatomic site when selecting lesions for the investigations, although it could reduce variability of the results.24
An interesting finding of our study was that analyzing tumor cell HLA class I expression in combination with CD8+ or CD45RO+ T-cell density values showed higher potency to predict survival in comparison with either HLA scores or T-cell density values alone (described here and in our previous report14). It calls attention to the usefulness of multiple immunohistochemistry (IHC) assays, which was proved the strongest predictor of checkpoint blockade efficacy in the case of PD-1/PD-L1 inhibitors according to a recent meta-analysis.25
Our study has some limitations, mainly because of its retrospective nature. Furthermore, the number of cases that could be included in the analysis was limited by the availability of sufficient surgical samples due to the relatively strict criteria we applied for sample selection (including only metastases removed within 1 year before ipilimumab therapy). On the other hand, a strength of our analysis is that it was performed on whole sections from surgical samples of more than one metastasis in most of the patients. This approach reduces the impact of intralesional and interlesional heterogeneity which has been described for HLA expression level and immune cell infiltration in melanoma and other tumor types.21 If additional studies with a larger number of metastases corroborate our initial observation that analysis of metastases from different anatomic sites may yield different results, it will be important to take into account this variable when correlating HLA class I APM component expression with clinical response to ICI.
Acknowledgments
The authors thank Katalin Derecskei and Miklós Kónya (National Institute of Oncology, Budapest) for their excellent technical assistance and István Gaudi (National Korányi Institute of TB and Pulmonology) for contribution to statistical analysis.
References
Footnotes
Presented at Part of this work was presented as a poster at the 32nd Annual Meeting of the Society for Immunotherapy of Cancer, November 8–12, 2017, National Harbor, Maryland (SITC 2017).
Contributors AL and SF conceived the study; AM, EP, TB and AL performed IHC evaluation; GL, JO, AV, ZL and GE contributed to sample collection and patient data management; SF supervised the project; AL and SF wrote the manuscript.
Funding The study was supported by the National Research, Development and Innovation Office grants NKFI K105132, K116295, ANN 128524, and GINOP_2.3.2-15-2016-00020 and by National Institutes of Health grants CA219603 and DE028172.
Competing interests TB has received speaker honoraria and financial support for attending symposia from Bristol-Myers Squibb, MSD Sharp & Dohme (MSD), Novartis, and Roche. GL is on the advisory board and has received honoraria for speaking at conferences as well as financial support for educational programs from Bristol-Myers Squibb, GlaxoSmithKline, MSD, Novartis, and Roche. JO has acted as a speaker of symposia and consultant for Bristol-Myers Squibb, MSD, Novartis and Roche. ZL has received speaker honoraria from Bristol-Myers Squibb, MSD, Novartis, and Roche. GE has received speaker honoraria from Bristol-Myers Squibb, MSD, and Roche. SF has received a research grant from Merck.
Patient consent for publication Not required.
Ethics approval The study followed the Declaration of Helsinki and was approved by the Scientific and Ethical Committee of Medical Research Council, Hungary (2506-3/2017/EKU). Informed consents from patients were not required by the board in case of retrospective studies where it is not possible to obtain consents from the majority of patients as in this case where most patients were deceased at the time of the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
↵Note added in proof: a recent paper (Such L et al: Targeting the innate immunoreceptor RIG-I overcomes melanoma-intrinsic resistance to T cell immunotherapy, J Clin Invest, in press) demonstrated an association between HLA-I APM gene downregulation at the transcriptional level and ICB resistance in patients with melanoma.