Article Text

Abstract
Background Immune checkpoint inhibitor (ICI)-associated early cardiac adverse events (CAEs), mostly acute and fulminant myocarditis, have been well characterized and mainly occur during the first 90 days after ICI therapy initiation. ICI-associated late CAEs (occurring after the first 90 days of treatment) have not yet been described.
Methods First, we compared characteristics of a cohort involving early (defined as a CAE time to onset (TTO) of <90 days after ICI therapy initiation) and late (defined as a CAE TTO of ≥90 days after ICI therapy initiation) ICI-associated CAE consecutive cases who were referred to three French cardio-oncology units. Second, ICI-associated CAE cases were searched in VigiBase, the WHO global individual case safety report database, and early and late ICI-associated CAEs were compared.
Results In the cohort study, compared with early CAE cases (n=19, median TTO of 14 days), late ICI-associated CAE cases (n=19, median TTO of 304 days) exhibited significantly more left ventricular systolic dysfunction (LVSD) and heart failure (HF) and less frequent supraventricular arrhythmias. In VigiBase, compared with early cases (n=437, 73.3%, median TTO 21 days), the late ICI-associated CAE reports (n=159, 26.7%, median TTO 178 days) had significantly more frequent HF (21.1% vs 31.4%, respectively, p=0.01). Early and late ICI-associated CAE cases had similarly high mortality rates (40.0% vs 44.4% in the cohort and 30.0% vs 27.0% in VigiBase, respectively).
Conclusions Late CAEs could occur with ICI therapy and were mainly revealed to be HF with LVSD.
Trial registration numbers NCT03678337, NCT03882580, and NCT03492528.
- cardiology
- epidemiology
- pharmacology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Pharmacological innovations are transforming the prognoses of malignancies, which, in some cancer types, are progressively turning into chronic diseases. The question of short-term and long-term adverse events is emerging with the use of these novel therapies. The aging of the population and the subsequent burden of cardiovascular risk factors are potential predictors of heart disease-specific mortality in cancer survivors, although great variability exists among different cancers.1 2
Early cardiac adverse events (CAEs) with immune checkpoint inhibitor (ICI) therapies were recently described.3–5 ICI-associated early CAEs are rare (close to 1% of patients) but potentially life-threatening, and are mostly represented by acute and fulminant myocarditis, which is often associated with hemodynamic failure and a risk of death of up to 50%.3–6 The time to onset (TTO) is usually very short (median time to occurrence is approximately 30 days after ICI therapy initiation),5 and the accepted higher-risk time window is defined as the first 90 days after ICI therapy initiation, justifying cardiac monitoring during this period, especially in patients with risk factors (ie, ICI combination therapy).3 7 8
Recently, in our daily cardio-oncology practice, cases of late ICI-associated CAEs (≥90 days after ICI therapy initiation) have emerged with clinical presentations that appear to be different from the acute and fulminant myocarditis previously described. Therefore, we aimed to characterize and describe the presentation and clinical course of these new clinical cardiac manifestations. We used two complementary approaches: first, we performed a cohort study to describe the clinical manifestations, management, and outcomes of consecutive sporadic CAE cases referred to three French cardio-oncology units. A cut-off of 90 days was used to separate early (defined as a CAE occurrence of <90 days after ICI therapy initiation) and late (defined as a CAE occurrence of ≥90 days after ICI therapy initiation) ICI-associated CAEs; second, we searched for reports of ICI-associated CAEs in VigiBase, the WHO global individual case safety report (ICSR) database, and we compared early (<90 days) versus late (≥90 days) ICI-associated CAE cases.
Methods
Cohort study
We extracted consecutive ICI-associated CAE cases (sporadic cases) referred to three French cardio-oncology units (Caen University Hospital; Hôpital Saint Antoine, Paris; and Aix-Marseille University NORD Hospital) between March 2015 and June 2019. Late ICI-associated CAE cases were defined as a CAE occurrence of ≥90 days from ICI therapy initiation, and early ICI-associated CAEs were defined as a CAE occurrence of <90 days from ICI therapy initiation. The 90-day cut-off period was based on several recent articles and reviews of ICI-associated CAEs describing higher rates of CAEs after the first and the third infusions of ICI.3 7 8 Some of these cases were previously published.3 The patients were managed according to similar protocols. Because no specific follow-up had previously been established for patients receiving ICIs during the study period, the oncologists referred patients receiving ICIs only on the basis of their clinical suspicion of a CAE. At the time of the CAE, these patients had a standardized evaluation including clinical evaluation, ECG, transthoracic echocardiography, and measurement of the brain natriuretic peptide and troponin serum levels. An additional biological sample was collected at the time of the CAE for the patients referred to Caen University Hospital. We described the patients with late ICI-associated CAE, including the demographic characteristics, cardiovascular risk factors and cardiovascular histories. We further reported the cancer type, ICIs used, the time of onset expressed as the calendar delay and as the total number of ICI injections before toxicity, the initial cardiovascular clinical manifestations, the type of cardiomyopathy, the associated cardiovascular diagnoses and the results of the complementary investigations. Informed consent was obtained from all the living subjects. The detailed list of collected variables is available in online supplementary material 1. The presence of a left ventricular systolic dysfunction (LVSD) was based on an echocardiographic or MRI left ventricular ejection fraction (LVEF) drop of <10% and LVEF of <50%, disregarding the presence of heart failure (HF) symptoms.9
Supplemental material
VigiBase pharmacovigilance cohort descriptive analysis
VigiBase is the WHO global ICSR database. It contains more than 18 million reports from 130 countries. The database is fed with reports from healthcare professionals, pharmaceutical companies and, more recently, patients. All reports are referred to national pharmacovigilance centers within a country, which secondarily transmits them to VigiBase. The Uppsala Monitoring Centre (Uppsala, Sweden) is in charge of keeping VigiBase current by adding novel reports and removing duplicates. We used a definition of CAEs similar to that used in a recent work addressing CAEs in VigiBase.5 Details on the VigiBase search and CAE identification are available in online supplementary material 1. The request was performed from inception until January 31, 2019. The time of onset was computed as the calendar delay between the date of the most recent ICI therapy initiation and the date of the CAE onset. Reports where the TTO could not be calculated due to the lack of at least one of the dates were excluded. We classified cases as early cases when the TTO was less than 90 days and as late cases when the TTO was at least 90 days.
The definitions of the ICSR parameters are available in online supplementary material 1. Associated immune-related adverse events (irAEs) were defined according to the definitions used in a recent study in VigiBase.5
Detection of anticardiac troponin I antibody
A dot blot was specifically developed for the detection of monoclonal anticardiac troponin I in late CAE cases. Controls were chosen among patients with lung cancer treated for more than 90 days with ICI who did not experience CAE and who had at least one cardiovascular risk factor at Caen University Hospital. Three hundred and eighty nanograms of the full-length recombinant human cardiac troponin I (Sigma-Aldrich) were spotted on a nitrocellulose membrane. When dried, the membrane was incubated with a blocking buffer (phosphate-buffered saline (PBS)/1% (m:v) gelatine) for 1 hour at room temperature, then sera obtained from control or patients (1/40 dilution in PBS/0.05% (v:v) TWEEN 20/1% (w:v) bovine serum albumin) or the monoclonal anticardiac troponin I (used as a positive control at 2 ng/μL, Abcam) was added. After 1 hour at room temperature under constant shaking, the membrane was washed three times with Tris-buffered saline/0.1% (v:v) TWEEN 20 (TBS/T) and was incubated for an additional 1 hour either with a mixture of antihuman IgG and IgM (1/1000, Southern Biotech) or antimouse IgG (1/1000, Abcam) antibodies, all conjugated to horseradish peroxidase. After three washes with TBS/T, immune reactive complexes were detected as present or absent using the western lightning chemiluminescence reagent plus (Perkin Elmer).
Statistical analysis
A descriptive analysis of the cohort study was performed on the available data. Qualitative variables were expressed as median and IQR. Qualitative variables were expressed in effectives and percentages, and Agresti-Coull 95% CIs of proportion were estimated for late CAE cases. Comparative analyses were performed between early and late CAE cases in the cohort population and between VigiBase early and late CAE reports. We did not merge sporadic cases and VigiBase reports to avoid duplicates because some of our cases were declared to the pharmacovigilance centers. The non-parametric Mann-Whitney-Wilcoxon test was used with quantitative variables, and χ2 test or Fisher exact test was used when appropriate for qualitative variables. Statistical analyses were performed with R software V.3.5.3 for Windows (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was defined as a p value of <0.05.
Results
Description of late ICI-associated CAE cases (cohort study)
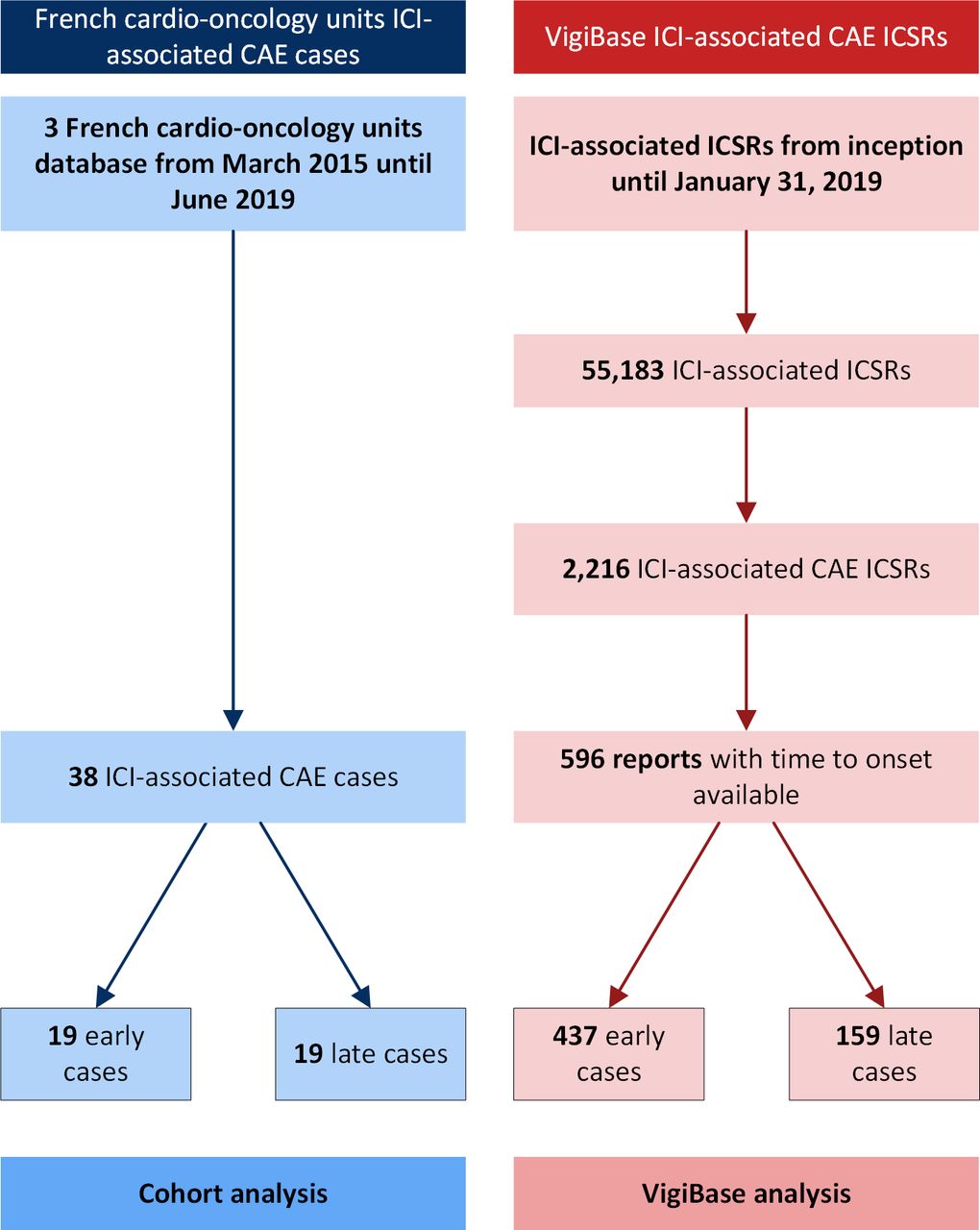
Figure 1 shows the case selection process. Nineteen late ICI-associated CAE cases were collected from our three French cardio-oncology units. Table 1 describes the late ICI-associated CAE cases. Most of the patients were men (15, 78.9%); the median age was 70 years (IQR 65–74). All the patients had cardiovascular risk factors, mostly tobacco use (13, 68.4%). A majority of the patients were treated for non-small cell lung cancer (17, 89.5%) with nivolumab monotherapy (16, 84.2%). One patient underwent a concomitant treatment with axitinib and recovered from LVSD while axitinib was continued and ICI was stopped. Thirteen patients had a prior platinum-based regimen; 3 patients had no prior treatment. No patients received myocardiotoxic drugs. Cardiovascular history was atrial fibrillation in four patients, ischemic heart disease in four patients, peripheral arterial disease in five patients, and transient ischemic stroke in one patient. Prior to the initiation of ICI therapy, 11 patients underwent an echocardiogram that was normal with an LVEF of >55% in all of them. The median TTO was 304 days (range 180–422). Patients with late CAE did not experience any early CAEs. The main clinical presentations were LVSD (14 cases, 73.7%) and symptomatic HF (9 cases, 47.4%). Late CAEs occurred on active ICI therapy in 13 patients, whereas 4 patients discontinued ICI therapy before the CAE (data missing for 2 patients). One patient presenting with HF and LVSD after 17 cycles of nivolumab had an endomyocardial biopsy. The myocardial biopsy was normal; there was no inflammatory stigmata (online supplementary figure 1). This patient had a complete LVEF recovery in 4 months with beta blockers, conversion enzyme inhibitors and ivabradine. MRI was performed in 14 patients and did not show evidence of an inflammatory process in 13 (92.9%), without late gadolinium enhancement or myocardial edema. High-dose corticosteroids were commonly used in patients with late CAE (10 patients, 52.6%). Two patients were already treated with oral corticosteroids when the CAE occurred. A second patient had improvement of his LVEF of >50% at 2 months under beta blockers and ACE inhibitor therapy. This patient was alive 10 months after the non-inflammatory LVSD diagnosis. Fatality was attributed to a cardiovascular disease in two patients (10.5%) and to malignancy in six patients (31.6%).
Supplemental material

Flowchart of case selection for the French cardio-oncology units and VigiBase. CAE, cardiac adverse event; ICI, immune checkpoint inhibitor; ICSR, individual case safety report.
Comparison of the early and late CAE cases from three cardio-oncology units
Comparison between early and late ICI-associated CAE cases (cohort study)
Figure 2 and table 1 show the comparison between early (n=19) and late (n=19) ICI-associated CAE cases from the French cardio-oncology unit database. The median TTO was 14 days (IQR 8–62) in the early CAE cases and 304 days (IQR 180–422) in the late CAE cases. Compared with the early CAE cases, the late CAE cases had significantly more cardiovascular risk factors (60% vs 100%, respectively; p=0.01), significantly higher rates of HF (5.3% vs 47.4%, respectively; p=0.01) and LVSD (36.8% vs 73.7%, respectively; p=0.049), and a significantly lower supraventricular arrhythmia rate (47.4% vs 10.5%, respectively; p=0.03). Recovery from LVSD was not different between early and late CAE cases (37.5% vs 14.3%, p=0.47). The cardiovascular-related mortality and overall mortality rates were not different between the early and late CAE cases.

{kind=link}
{kind=link}
Immune checkpoint inhibitor-associated CAE rates in early (<90 days) and late (≥90 days) cases from three French cardio-oncology unit databases (A) and in VigiBase (B). CAE, cardiac adverse event; LVSD, left ventricular systolic dysfunction; ns, not significant.
Description of the VigiBase cohort
Figure 1 shows the flow diagram of the case selection process for VigiBase. Of the 2216 reports, 596 had an available CAE TTO and were included in the analysis. There were 437 (73.3%) early ICI-associated CAE cases (any early event) and 159 (26.7%) late ICI-associated CAE cases (any late event). The median TTO was 21 days (IQR 8–44) in the early CAE cases and 177 days (IQR 128–317) in the late CAE cases. Seventeen percent of the late cases had a TTO longer than 1 year. Table 2 summarizes the characteristics of the included reports. Most of the patients were men (68.4%), and the completeness score of the selected cases was above 0.65 in 75% of the cases. The seriousness was available in all cases, and all cases were considered serious. The main drug indications were lung cancer (52.8%), melanoma (26.0%) and renal cancer (11.5%). A majority of the patients were treated with antiprogrammed death 1 (PD-1) therapy or anti-programmed death ligand 1 therapy alone (84.2%). Combination therapy with two ICIs was used in 46 (7.7%) patients. A comparison between the early and late CAE cases showed significantly higher rates of HF (21.1% vs 31.4%, respectively; p=0.012) and pericardial disorders (11.4% vs 18.2%, respectively; p=0.043) in the late CAE cases. Mortality rates were comparable between the early and late CAE cases (30.0% vs 27.0%, respectively; p=0.55).
Comparison between early (<90 days) and late (≥90 days) CAE reports collected from VigiBase until January 30, 2019
Anticardiac troponin I antibody detection in patients with late CAEs
Out of four late CAE cases, two (50%) exhibited the presence of IgG/IgM antibodies against cardiac troponin I compared with zero of four control patients (online supplementary table 1 and supplementary figure 2). One late CAE case with positive autoantibody detection had a history of silent myocardial infarction diagnosed 4 years before ICI initiation. The four control patients were treated with ICI anti-PD-1 monotherapy for more than 90 days for lung cancer and did not develop any CAE. These four control patients all had cardiovascular risk factors and were aged 62–75 years. Detection of IgG/IgM antibodies against cardiac troponin I before ICI initiation could not be performed.
Supplemental material
Supplemental material
Discussion
In this study, we described for the first time a newly phenomenon of late ICI-associated CAEs, occurring after the first 90 days previously described as the highest-risk time window for ICI-associated CAEs. The already-known and published ICI-associated CAEs are described as occurring rapidly after the initiation of ICI treatment. In a cohort study of two cardio-oncology unit databases, Escudier et al found a median TTO of 29 days for ICI-associated CAEs that were mainly represented by acute and fulminant myocarditis or takotsubo presentation.3 A recent pharmacovigilance study found similar delays in the onset of myocarditis and pericardial disorders, both associated with inflammatory process.5 Compared with these early descriptions, we described late CAEs with a median TTO of 6 months (17.0% of the late CAEs in VigiBase were diagnosed more than 1 year after ICI therapy initiation). Hence, we believe it is important for physicians to keep this risk in mind even after the accepted higher-risk time window of 90 days after ICI therapy initiation, justifying the prolongation of cardiac monitoring beyond this period.
These late ICI-associated CAE cases presented several significant differences compared with early ICI-associated CAE cases. Supraventricular arrhythmias and myocarditis were not usually observed in the late cases (10.5% for both), and conversely, late cases exhibited more HF and LVSD. The mortality rate was not significantly different between early and late ICI-associated CAE cases (40.0% vs 44.4% in the cohort analysis and 30.0% and 27.0% in the VigiBase analysis, respectively), but we observed a potential of reversibility for late LVSD cases (14.3%).
The underlying mechanism of ICI-associated late CAEs, especially the role of inflammatory processes, remains unknown. Unfortunately, endomyocardial biopsy was performed in only one of our cases (online supplementary figure 1). This myocardial biopsy did not exhibit any lymphocyte infiltration or fibrosis pleading for a non-inflammatory process. Smoldering early and acute myocarditis were previously described and were associated with minimal or absence of symptoms and less-severe evolution.10 The natural history of this entity is unclear but may parallel viral myocarditis. In case of undiagnosed smoldering myocarditis and ICI continuation, a slowly progressive evolution to LVSD seems conceivable. Prior-to-CAE corticosteroid use might also preclude early clinical manifestation of a myocarditis in late LVSD cases (two patients had corticosteroid use for another irAE before the occurrence of the CAE). This could be supported by the detection of cardiac troponin I autoantibodies in two of four late CAE cases, but one patient had a prior history of myocardial infarction, which could also be responsible for the presence of cardiac troponin I autoantibodies.11 12 Additional studies with a longitudinal follow-up of cardiac autoantibodies are needed to precisely determine the temporality between CAEs and autoantibody detection. Murine viral myocarditis models highlighted that during the chronic viral myocarditis phase, there was no longer any inflammatory cell infiltration at histology and that myocardial fibrosis was present but with a heterogeneous distribution among the myocardium and a clear predominance in the inner two-thirds of the LV free wall.13 Our case’s endomyocardial biopsy was acquired, as usual, from the right ventricular septum, which might explain the absence of fibrosis. Moreover, there are several reports that dysregulation of cardiomyocyte Ca2+ currents results in the development of LVSD and dilated cardiomyopathy.14–16 Previous experimental works have shown that PD-1-deficient mice developed autoimmune dilated cardiomyopathy with production of high-titer cardiac troponin I-specific antibodies.17 Both acute death (5 weeks of age, 14.2%) and late death (between 20 and 30 weeks of age, 46.4%) related to congestive HF were observed. Importantly, the dilated heart exhibited no apparent signs of inflammation at histology. In a follow-up work, the same group administrated cardiac troponin I specific antibodies to wild-type mice and observed the development of both acute (12 weeks of exposure) and late (35 weeks of exposure) dilated cardiomyopathy with more severe LSVD at 35 weeks.12 The underlying pathway responsible for the development of dysfunction and dilatation of the heart was attributed to an increase in voltage-dependent L-type Ca2+ current of normal cardiomyocytes. Whether immune response would be involved in the development of late ICI-associated CAEs remains uncertain.
The treatment of late ICI-associated CAEs has never been described. Seven of our 13 sporadic cases presenting with LVSD and without inflammatory signs at clinical examination, echocardiography or MRI were treated with high-dose intravenous glucocorticoids, followed by the administration of oral glucocorticoids with a progressive decrease, in addition to classical HF treatment. These seven cases represent the first cases admitted in our cardio-oncology units for late LVSD. The ignorance of such clinical presentations at this time, the delay to obtain the inflammatory status by cardiac MRI or endomyocardial biopsy (usually at least 24–48 hours in daily practice), and the fear of clinicians to be confronted with a possible fulminant myocarditis probably explain this attitude. On the basis of these seven cases, management and follow-up, the next six patients were not treated with corticosteroids, and none of them experienced fatality. Further studies are needed to determine whether this approach should be recommended for all ICI-associated late CAEs. Finally, current guidelines recommend a definitive disruption in ICI therapy in case of life-threatening or severe adverse events.18 However, we believe that the management of ICI therapy should be discussed for each individual case according to the cancer status and toxicity regression of the patient. Combined cardiological and oncological care appears to be crucial to reduce the impact of CAEs in these patients. Unfortunately, no rechallenge was performed in our late CAE cases, and therefore, to date, we cannot tell if it could be considered, even after clinical recovery.
Our study suffers from several limitations. The observational and retrospective design cannot prove the causality of the association between ICI use and late CAE occurrence. Moreover, such approach did not allow the determination of the incidence of these adverse events (ie, we do not have the denominator of ICI-treated patients in our French sites and VigiBase does not provide this information). We cannot exclude the possibility that the only endomyocardial biopsy in our sporadic case was a false negative, and of course, the lack of other biopsy represents a clear limitation to our conclusions. Unfortunately, oncology patients do not systematically undergo a cardiac evaluation before ICI therapy initiation, as illustrated in our sporadic cases. The small number of patients in our cohort may lead to biases and statistical analysis should be considered exploratory. Some cases of ICI-associated CAEs are likely not reported to VigiBase (under-reporting) and VigiBase ICSRs are incompletely reported. Thus, the TTO could not be computed for every ICSR that met the eligibility criteria. However, the completeness score of the remaining cases was rather high (>0.65 in 75% of cases). VigiBase is not designed to supply information regarding previous anticancer drugs lines. ICI being mostly prescribed in lung and melanoma malignancies at the moment of CAEs occurrence, and cardiotoxic agents not being prescribed in these cancers, we do not expect any delayed cardiotoxicity interference. It was not possible to compute the reporting OR for the late-onset reports, which would have provided additional information. The volume of reports for a specific drug could be influenced by the extent of the use of the drug or medical/healthcare community interest, which is called notoriety bias.
Conclusions
In this study, we described new clinical manifestations of ICI-associated CAEs, represented by late HF, occurring more than 90 days after ICI therapy initiation. This ICI-associated CAE spectrum completes the description of previously published early manifestations mainly related to acute and fulminant myocarditis. These cases exhibited particular clinical features and potential seriousness with a high mortality rate; therefore, we believe that physicians should be aware of this potential cardiac toxicity and that cardiac monitoring should be prolonged past the first 90 days after ICI therapy initiation.
Acknowledgments
The information presented in this study does not represent the opinion of WHO. We thank the custom searches team at the Uppsala Monitoring Centre (Uppsala, Sweden) research section, without whom this study would not have been possible.
References
Footnotes
Contributors CD, SE, JA, FRT, and JC conceived and designed the study, collected and interpreted the data, drafted the manuscript or revised it critically for important intellectual content. SA, QD, RG, JM, MS, A-FP, FC, and AAC collected and interpreted the data, revised the manuscript for critically important intellectual content. All authors gave their final approval of the manuscript submitted and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy of integrity of any part of the work are appropriately investigated and resolved.
Funding This study was funded by Centre Hospitalier et Universitaire de Caen.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The locally appointed ethics committee approved the research protocol, and informed consent to participate was obtained from all the live subjects (or their legally authorized representatives).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The datasets generated and/or analyzed during the current study are not publicly available due to the risk of individual privacy violation but are available from the corresponding author on reasonable request.