Article Text

Abstract
Background Immune checkpoint inhibitors such as nivolumab and targeted BRAF inhibitors have dramatically altered the treatment outcomes of metastatic melanoma over the past few years. Skin toxicity is the most common adverse event (AE) related to the commonly used BRAF inhibitor vemurafenib, affecting more than 90% of patients. Vemurafenib-related severe AEs with early onset are reported in patients who were previously treated with anti-programmed cell death-1 (anti PD-1) antibodies. A prolonged administration of systemic steroids is the first-line treatment of severe or life-threatening AEs. We report the case of a woman suffering from vemurafenib-related severe, rapidly worsening Drug Rash with Eosinophilia and Systemic Symptoms (DRESS) syndrome, resolved in a few hours after single-dose administration of a combination of TNF-α antagonist infliximab with interleukin (IL)-6 receptor antagonist tocilizumab.
Case presentation A 41-year-old woman treated with single-agent nivolumab presented with a melanoma progression. Biopsy samples were revised, revealing a BRAF V600E mutation. The patient was started on vemurafenib and cobimetinib treatment only 10 days after the last administration of nivolumab. On the third day of anti-BRAF therapy, profound lymphopenia was detected, and maculopapular eruption appeared afterward. Subsequently, the clinical conditions deteriorated further, and the woman was admitted on an emergency basis with high fever, respiratory and cardiocirculatory failure, diffuse rash, generalized edema, and lymphadenopathy. Diagnosis of DRESS syndrome with overexpressed capillary leakage was made. A single dose of tocilizumab was administered with an improvement of cardiocirculatory and renal function in a few hours. Because of worsening of liver function, skin lesions and mucositis, a single dose of infliximab was prescribed, and dramatic improvement was noted over the next 24 hours. Dabrafenib and trametinib were initiated, and coinciding with washout of infliximab from the patient’s blood, the drug toxicity recurred.
Conclusion Anti-IL-6 and anti-TNF-α target treatment of very severe AEs may afford an immediate resolution of potentially life-threatening symptoms and reduce the duration and the costs of hospitalization. Maintenance of therapeutic infliximab blood concentrations permits an early switch to dabrafenib after vemurafenib-related AEs.
- oncology
- tumors
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Targeted therapy currently represents a promising therapy for malignancies, such as metastatic melanoma with the BRAF V600 mutation, that are refractory to conventional chemotherapies. Vemurafenib was licensed for the treatment of nonresectable metastatic melanoma by the Food and Drug Administration Agency in the USA in August 2011 and by the European Medicines Agency in Europe in February 2012.1 Unfortunately, the duration of BRAF inhibitor-induced responses proved too short in all treated patients because of the development of resistance. The primary resistance mechanism to BRAF inhibition is reactivation of the MAPK pathway.2 The clinical evidence of the benefit, however, led to approval in 2015 of the use of combinations vemurafenib plus cobimetinib as well as dabrafenib plus trametinib.3
Skin toxicity is the most common adverse event (AE) related to vemurafenib, affecting more than 90% of patients.4 5 Grade 3 skin toxicity is observed in a variable percentage from 15% to 40% of treated patients. In contrast, grade 4 skin toxicity is uncommon in clinical studies, with an incidence that does not exceed 1%.6 However, the rate of severe AEs occurring in patients treated with vemurafenib in real-life conditions is reported to be significantly higher.7
Vemurafenib-related severe AEs with early onset are reported in patients who were previously treated with anti-PD-1 (anti-programmed cell death-1) antibodies, especially in the preceding 4 weeks.8 9 According to preliminary evidence, the combination of BRAF/MEK-inhibitors with anti-PD-1 antibodies results in a significantly higher toxicity profile compared with current treatment protocols, with more than half of patients experiencing a grade 3–5 AE and 40% discontinuing at least one of the drugs in phase II of their ongoing clinical trial KEYNOTE-022.10
A prolonged administration of systemic steroids, after interruption of a culprit drug, is the first-line treatment of severe or life-threatening AEs. Several case reports describe the second-line successful treatment with intravenous immunoglobulin, cyclosporine, cyclophosphamide, mycophenolate mofetil, and plasmapheresis.11 The duration of clinical and biological abnormality is 35 days on average in the severe AEs with systemic involvement.7
In this manuscript, we report the case of a woman suffering from vemurafenib-related severe, rapidly worsening Drug Rash with Eosinophilia and Systemic Symptoms (DRESS) syndrome. Disease progression was stopped in a few hours after a combination of TNF-α antagonist infliximab with interleukin (IL)-6 receptor antagonist tocilizumab single-dose administration.
Case presentation
A 41-year-old woman was diagnosed with AJCC stage IB melanoma on her back (Breslow index, 4.65 mm) in June 2016 in Ukraine. At the time, she was treated only with radical resection of primary tumor. Disease progression with primary lesion recurrence ensued over the next 2 years. Breast, lung, spleen, liver, subcutaneous fat, and axillary lymph node involvements were documented when a CT scan was performed. She was treated with primary lesion debulking and axillary lymph node curettage. Subsequently, after her arrival in Italy, she began anti-PD-1 (nivolumab) and tolerated four cycles of therapy without side effects but developed new splenic, hepatic, and bone metastases. Biopsy samples were revised, and molecular testing revealed a BRAF V600E mutation. A combination of anti-BRAF and anti-MEK therapy was proposed. The patient was started on vemurafenib 960 mg two times a day and cobimetinib 60 mg once a day.
On the third day (D+3) of anti-BRAF therapy, profound lymphopenia (210/mm3) was detected. The following day (D+4) maculopapular eruption predominating on the photo-exposed areas appeared. Treatment was continued, and a topical corticosteroid was prescribed. The rash worsened over the next days (figure 1), high fever and fatigue also manifested, and 3 days later (D+7) the patient was admitted on an emergency basis with life-threatening conditions.

Highly painful confluent erythematous macules.
At admission she presented with a highly painful erythematous rash covering more than 80% of the body surface, hemorrhagic crusting on the lips (figure 2), oral, and nasal mucositis, generalized edema more prominent in the face, inguinal lymphadenopathy, fever of 39.7°C with chills, hypotension, oliguria, and shortness of breath with desaturation (SaO2 84% in room air). The examination demonstrated decreased breath sounds and dullness to percussion over the lower two-thirds of both hemithoraxes. Lung ultrasound was performed, and bilateral pleural effusion was documented. Laboratory testing demonstrated leukocytosis (16,700/mm3) with 98.7% of neutrophils, C reactive protein 145.7 mg/L (n.r.<5 mg/L), procalcitonin 4.11 µg/L (n.r.<0.5 µg/L), lactate dehydrogenase 717 U/L (n.r. <250 U/L), creatine phosphokinase 824 U/L (n.r. 25–170 U/L), serum creatinine 1.53 mg/dL (baseline value 0.70 mg/dL), alanine aminotransferase (ALT) 188 U/L and aspartate aminotransferase (AST) 193 U/L (n.r. <35 U/L), cholinesterase activity 3004 U/L (n.r. 3930–10,800 U/L), serum albumin 2.32 g/dL (n.r. 3.50–5.20 g/dL), complement C3 63 mg/dL (n.r. 90–180 mg/dL), and complement C4 6 mg/dL (n.r. 10–40 mg/dL). Blood cultures, FilmArray Respiratory Panel (RP2 plus) and Pneumonia Panel (Pneumo plus), real-time PCR for cytomegalovirus (CMV), Epstein-Barr virus (EBV), Adenovirus, herpes simplex virus (HSV), human herpes virus (HHV)-6, HHV-7, HHV-8, Parvovirus B19 were all negative.

Hemorrhagic crusting on the lips associated with oral mucositis.
Vemurafenib and cobimetinib were discontinued at once. The patient was started on a powerful intravenous saline solution with albumin, prednisone 2 mg/kg/day, broad-spectrum antibiotics, continuous furosemide infusion, and antihistamine medication. She also underwent noninvasive ventilation used high flow oxygen therapy with an AIRVO device because of increasing (up to 10 L/min) oxygen requirement.
The next day the patient’s clinical condition worsened even more: low urine output was evident in weight gain, the edema worsened leading to anasarca, renal function deteriorated, and hypotension requiring vasopressor support ensued. DRESS syndrome with overexpressed capillary leakage symptomatology was suspected. Using the RegiSCAR scoring system, our case registered a score of 7 points and was therefore classified as definite DRESS syndrome.12 Despite the mucosal involvement, a diagnosis of Stevens-Johnson syndrome was discounted because of the severity of systemic symptoms. In an attempt to interrupt capillary leakage of fluid in the interstitial space, the patient was treated with a single, 8 mg/kg, dose of tocilizumab (D+9), an IL-6 receptor antibody. Progression of body weight gain and edema was halted, and blood pressure and renal function improved in a few hours. Diuretic and vasopressor supports were discontinued, oxygen requirement was drastically reduced, and noninvasive ventilation was replaced with the conventional nasal cannula. Oxygen support was finally suspended 2 days later (D+11).
Together with the restoration of hemodynamic and respiratory functions, the liver function tests (LFTs) worsened (ALT 450 U/L, AST 339 U/L), and eosinophilia (930 cells/mm3) and thrombocytopenia appeared. Oddly, the immunoglobulin M went up to 693 mg/dL (n.r. 40–230 mg/dL). The cutaneous involvement did not have decisive improvement. Mucosal lesions also remained unchanged, making any enteral intake impossible. Three days after tocilizumab administration (D+12), the patient received a single dose (5 mg/kg) of infliximab, the TNF-α-blocking agent. Dramatic improvement of skin lesions and mucositis was noted over the next 24 hours (D+13), and the patient was discharged the next day. The hospitalization lasted only 7 days. At follow-up 1 week after discharge (D+20), the physical examination was unremarkable, no cutaneous or mucosal lesions were noted, the LFTs were normal, and the patient had resumed regular feeding. She began a rapid prednisone tapering (D+25; D+32).
Because of the benefit of BRAF inhibitors on her metastatic disease, relatively young age and good general condition, dabrafenib and trametinib were initiated 1 month after discharge without signs of drug toxicity (D+53; D+67). Two weeks after the start of dabrafenib, at the same time as washout of infliximab from the patient’s blood, high fever without other symptoms recurred (D+71). Fortunately, she could continue the dabrafenib treatment after the addition of cortisone (0.5 mg/kg) without further complications.
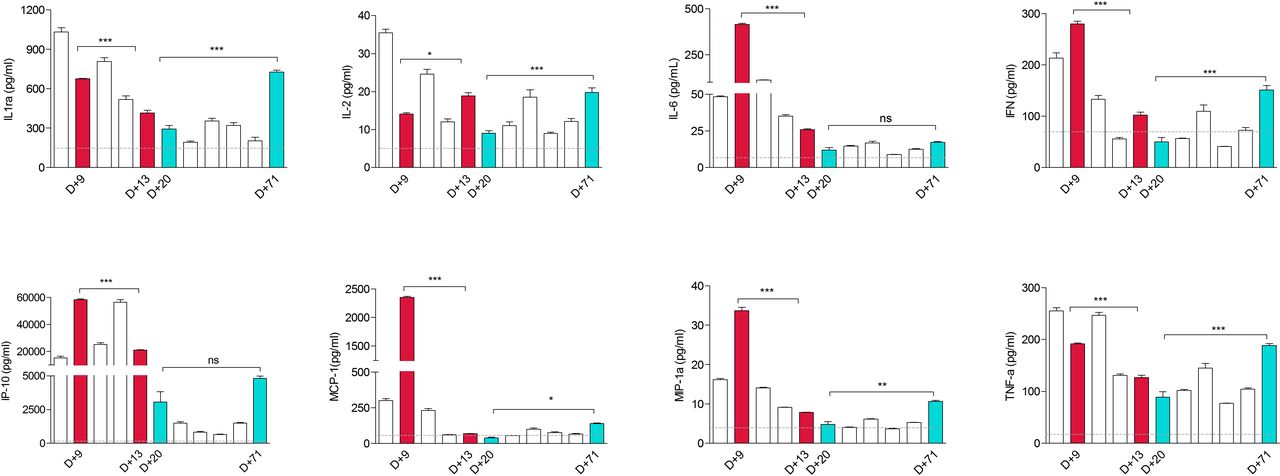
We evaluated the concentration of plasma cytokines, using inflammatory multiplexed panel, at every significant phase of this case. Of 27 proinflammatory and regulatory cytokines and chemokines evaluated, the levels of 24 molecules greatly exceeded those normal for age, while IL-12 and granulocyte-macrophage colony-stimulating factor (GM-CSF) concentrations were below the normal range, and only IL-1β values remained around the normal values. The marked increase in the concentration of cytokines was found only during the active phase of the drug-related inflammatory process for IL-1ra, IL-6, IL-10, interferon (IFN)-γ, interferon-γ inducible protein-10 (IP-10)/CXCL10, monocyte chemoattractant protein-1 (MCP-1)/CCL2, and macrophage inflammatory protein-1α (MIP-1α)/CCL3 (figure 3). Consistently high values, even during remission, have been documented for IL-5, macrophage inflammatory protein-1β (MIP-1b)/CCL4, regulated on activation, normal T cell expressed and secreted (RANTES)/CCL5, Eotaxin/CCL11, fibroblast growth factor (FGF), granulocyte colony-stimulating factor (GCSF), and vascular endothelial growth factor. Remarkably, even TNF-α values, although significantly decreased, remained permanently high despite infliximab treatment.

Cytokine profile at every point of time in the case report. Columns of serum level (pg/mL) of IL-1ra, IL-2, IL-6, IFN-γ, IP-10/CXCL10, MCP-1/CCL2, MIP-1α/CCL3, TNF-α at all times analyzed (D+7, D+9, D+11, D+12, D+13, D+20, D+25, D+32, D+53, D+67, D+71). The physiological cytokine levels in healthy subjects (HS; n=35) (≥18 years old) are represented by the dashed line. Data analyses were performed with one-way analysis of variance (ANOVA) test followed by the Bonferroni’s correction D+3 vs D+13 and D+20 vs D+71; *p<0.05, **p<0.01, ***p<0.001, NS: nonsignificant. ANOVA, analysis of variance; IP-10, inducible protein-10; MCP-10, monocyte chemoattractant protein-1; MIP-1α, macrophage inflammatory protein-1α.
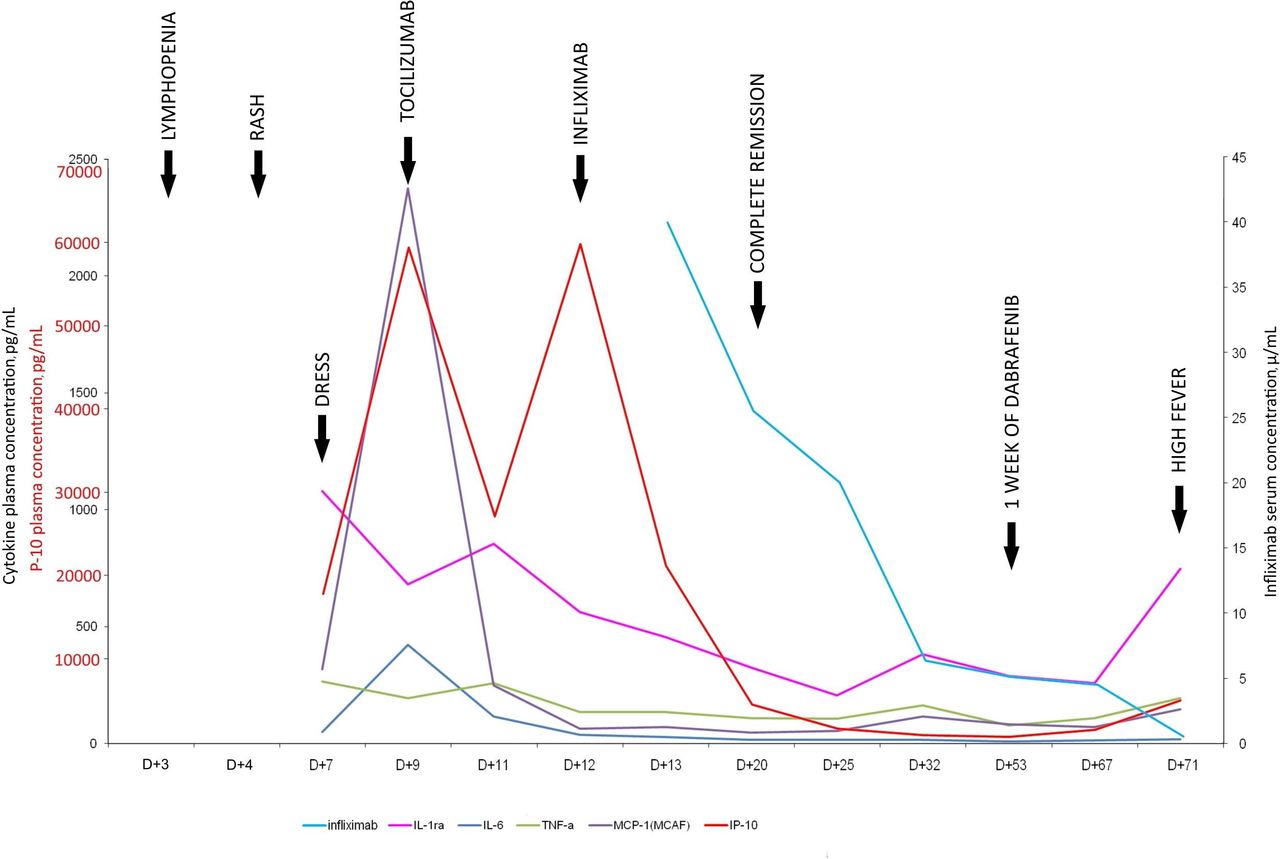
All data of cytokines and chemokines concentration are shown in online supplementary figures S1–S3. Infliximab therapeutic drug monitoring and the more significant plasma cytokine level tendencies are illustrated in figure 4.
Supplemental material
Supplemental material
Supplemental material
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Graph of the trends of cytokine plasma and infliximab serum concentration during the vemurafenib-related DRESS treatment course and at the time of dabrafenib reintroduction. D 0 (day 0) coincides with the beginning of vemurafenib treatment. Note the drop of plasma concentration of all cytokines/chemokines displayed after treatment with monoclonal antibodies. Their levels remain low until infliximab is a washout, when the cytokines start to rise, particularly the IL-1ra.
Discussion
DRESS syndrome, also known as drug-induced hypersensitivity syndrome, is a rare, potentially life-threatening rash with eosinophilia and systemic symptoms. Reported DRESS-related mortality rates are approximately 10% or higher, depending on the degree and type of organ involvement, even with proper medical management.11
Usually, the onset of DRESS syndrome is 2 months following culprit drug initiation. Our patient developed the first signs of skin toxicity on the fourth day from the start of vemurafenib-cobimetinib therapy. Some recent publications have shown that previous treatment with anti-PD1 drugs is associated with the early onset and the severity of vemurafenib-induced skin disorders, including hypersensitivity syndrome.13–15 Our patient started anti-BRAF therapy only 10 days after the last administration of nivolumab, without a sufficiently long washout period. Though the nivolumab treatment was well-tolerated, it may have triggered the immune system, leading to severe drug toxicity. The reduction in immune checkpoint inhibition caused by nivolumab may have predisposed the patient to a skin hypersensitivity reaction caused by vemurafenib. The overlapping of the two phenomena can explain this predisposition. First, vemurafenib caused marked tumor infiltration of CD8+ cytotoxic T lymphocytes. Furthermore, the presence of functional host cytotoxic T cells may have played an essential role in effecting responses to BRAF inhibitor therapy.16 Second, the immune checkpoint inhibitors strongly provoked activation of CD8+ cytotoxic T cells, which are also the key cellular mediators in drug-induced skin toxicity.17 High levels of IP-10/CXCL10 and MCP-1/CCL2 plasma concentration, which were documented in our patient only at the onset, that is, in the active phase of DRESS, confirm this process. IP-10/CXCL10 with MCP-1/CCL2 plays a significant role in CD8+ T cell recruitment and in leucocyte homing to inflamed tissues, exacerbating inflammation and causing substantial tissue damage.18
More than 90% of patients treated with vemurafenib experience AEs; 26% of them develop grade 3–4 skin toxicity.7 19 We documented a severe lymphopenia in our patient as early as 2 days after initiation of anti-BRAF treatment. The previous report of Imafuku et al suggested that lymphopenia is a useful marker of vemurafenib-induced AEs and may be used as an indicator for reduction of vemurafenib dosage to prevent the appearance of severe side effects.20 The authors demonstrated a positive correlation between the grade of lymphopenia and the severity of AEs. We found the increase of IL-1ra, in addition to profound lymphopenia, at the early onset of anti-BRAF-related AE. We have documented the high concentrations of IL-1ra both at the onset of DRESS and the manifestation of dabrafenib-related fever, before the significant increase of the other cytokines and chemokines analyzed.
Development of severe skin adverse reactions such as DRESS, Steven-Johnson syndrome or toxic epidermal necrolysis, besides indicating immediate discontinuation of vemurafenib, permanently contraindicates its use.7 For those who do not respond to immune checkpoint blockade therapy, it is equivalent to a death sentence because of the extremely severe course of metastatic malignant melanoma after vemurafenib withdrawal.21 The successful use of dabrafenib in case of vemurafenib-induced severe AEs have been reported.7 22–24 For a safe switch to dabrafenib, complete remission of vemurafenib-related toxicity symptoms is required. One month is the mean time to a full recovery with no sequelae, which is reported in the literature.13 The disease can undergo a rapid progression in 1 month. High level of immunoglobulin M, the potent inhibitor of the excessive inflammatory response25 found in our patient’s blood, confirmed the increased activity of the inflammatory process. Targeted treatment with drugs that are selective inhibitors of the production of cytokines involved in severe drug-related toxicity, such as tocilizumab, can significantly modify the clinical outcomes and allow the rapid resumption of anti-melanoma therapy. Mori et al recently demonstrated that elevated levels of IL-6 and TNF-a might predict a poor outcome in patients with cancer with severe cutaneous adverse reactions.26 Extremely high levels of IL-6 and TNF-α at the DRESS onset (70 and 20 times greater than the normal range, respectively) provide the rationale for treatment with targeted monoclonal antibodies.
However, we need to consider another important matter. Though combination BRAF and MEK inhibition extend the duration of response, most tumors develop adaptive resistance within a relatively short interval. In the first-line setting, the proportion of patients free of disease progression at 6 months is 72.3%, survival at 12 months is 76.9% and at 24 months, 53.5%.27 Recently reported in the literature is a significant increase in overall survival within the first 3 months of patients who experienced severe vemurafenib-related skin toxicity.7 The explanation for the findings is that immunomodulatory therapies and inflammation due to vemurafenib trigger the patient’s antitumor immunity, inducing the systemic release of cytokines and activation of natural killer (NK) and cytotoxic T lymphocytes. In our case, we documented an elevated plasma concentration of IL-2 at each evaluation, which proved particularly high during acute DRESS phase. IL-2 has a pleiotropic role in the maintenance of the balance between the promotion and inhibition of the immune response. This equilibrium allowed to obtain promising results from the clinical therapeutic application of IL-2 in the trial in patients with metastatic melanoma.28–30 Despite the development of new therapeutic approaches, high-dose IL-2 remains an important option for patients with melanoma and has an improved therapeutic window in the current era.31 Three chemokine proteins that were reproducibly detected in abundance in the T-cell-rich melanoma were MCP-1/CCL2, MIP-1β/CCL4, and RANTES/CCL5, while most melanoma cell lines showed expression predominantly of IL-8/CXCL8 only.32 As a result, the lack of CD8+ T cell recruitment chemokines can explain the worst outcomes of antimelanoma treatment. The most relevant chemokines for effector CD8+ T cell migration could be considered MCP-1/CCL2, MIP-1α/CCL3, MIP-1β/CCL4, RANTES/CCL5, CXCL9, and IP-10/CXCL10. Transmural migration assays document that each of these chemokines was sufficient to recruit CD8+ effector T cells primed from healthy donors in vitro.25 Our data document that at the onset of DRESS, the values of all of these chemokines is markedly elevated (CXCL9 was not analyzed). While the values of IP-10/CXCL10, MCP-1/CCL2 and MIP-1α/CCL3 return within the normal range after monoclonal antibodies are used, the levels of MIP-1β/CCL4 and RANTES/CCL5 remain persistently high, even when the DRESS symptoms disappear.
Conclusion
First-line therapy options for metastatic melanoma treatment currently include BRAF inhibitors or immune checkpoint inhibitors. The better sequence for these treatments has not yet been defined. A switch to BRAF inhibitors after immunotherapy failure must be carried out under close medical control with prompt identification of patients who develop profound lymphopenia. If profound lymphopenia is detected, the IL-1ra blood concentration determination could be useful in predicting the severity of drug-related toxicity and in taking decisions about treatment interruption. Anti-IL-6 and anti-TNF-α target treatment of very severe AEs may yield an immediate resolution of potentially life-threatening symptoms and reduce the duration and the costs of hospitalization. Maintenance of therapeutic infliximab blood concentrations for 9 weeks permits an early introduction of dabrafenib after vemurafenib-related AEs. Use of infliximab during extreme systemic inflammation such as DRESS does not reset the TNF-α levels but only lowers them. Thus, the risk of infections due to its use does not increase. The “protective” blood concentration of infliximab boosts antitumor immunity, maintaining the high levels of proinflammatory cytokines, without AEs.
Acknowledgments
We thank all the nursing and support staff of the Bone Marrow Transplant Unit of the Burlo Garofolo Pediatric Hospital for their care and attention generously given to this ‘overly mature’ patient, matching what they offer daily to their smaller patients.
References
Footnotes
Contributors NM was involved in the clinical care of the patient, in conceptualizing the study, and manuscript writing. AnM was involved in conducting translational cytokine and infliximab blood concentration studies, as well as editing relevant sections. AlM and DZ were involved in patient data collection, creating figures, and editing the manuscript. All authors contributed to revising the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval Reporting patient biomarker data presented in this manuscript was obtained from the Institutional Review Board of IRCCS Burlo Garofolo (reference no. 34\18).
Provenance and peer review Not commissioned; externally peer reviewed.