Article Text

Abstract
Background The efficacy of immune checkpoint inhibitors (ICI) in metastatic melanoma is well established. However, there are limited data regarding their efficacy in in-transit melanoma (ITM). This study assessed the efficacy of ICI in patients with ITM.
Methods A retrospective review of patients with ITM commenced on an ICI between March 2013 and February 2018 at three tertiary centers in Australia. Patients were excluded if they had previous or synchronous distant metastases. Overall response rate (ORR), progression-free survival (PFS) and overall survival (OS) were based on a composite of radiological and clinical assessments.
Results Fifty-four patients were included: 27 (50%) female; median age 75 (range 26–94); 12 (22%) stage IIIB, 40 (74%) stage IIIC and 2 (4%) stage IIID; 10 (19%) BRAF mutant. Forty (74%) received single-agent anti-PD-1 (pembrolizumab or nivolumab), 8 (15%) single agent anti-CTLA-4 (ipilimumab), 5 (9%) combination anti-PD-1/anti-CTLA-4 (ipilimumab and nivolumab or pembrolizumab) and 1 (2%) combination anti-PD-L1 (atezolizumab) and MEK inhibitor (cobimetinib). The median follow-up was 15 months (2–46).
ORR to ICI was 54%: 14 (26%) complete responses; 15 (28%) partial responses; 9 (17%) stable disease; 16 (30%) progressive disease. Thirteen (46%) responders had only one ITM lesion. ORR was 58% for single-agent anti-PD-1, 38% for single-agent anti-CTLA4 and 40% for anti-PD-1/anti-CTLA-4. The median PFS was 11.7 months (6.6-not reached). 1-year and 2-year PFS were 48% and 39%, respectively,. Fourteen progressed locoregionally and 11 progressed distantly. The median OS was not reached. 1-year and 2-year OS were 85% and 63%, respectively. No clinicopathological features were associated with ORR.
Conclusions and relevance ICI produce objective responses in ITM and should be considered in patients with unresectable ITM or disease recurrence.
- oncology
- surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background and rationale
The advent of immune checkpoint inhibitors (ICI) and BRAF and MEK inhibitors has transformed the treatment landscape and prognosis of patients with metastatic melanoma. In seminal studies, pembrolizumab resulted in a 5-year overall survival (OS) of 34% and the combination of ipilimumab and nivolumab produced a 4-year OS rate of 53%.1 2 In-transit melanoma (ITM) is defined by the presence of metastases in the superficial lymphatic system more than 2 cm from the primary lesion but not beyond the regional lymph node basin. Patients with locoregional disease and ITM alone are not well represented in landmark studies.
The natural history of ITM is variable; some tumors have limited systemic metastatic potential and present with multiple locoregional recurrences over years while others rapidly develop distant metastases. Although the 5-year OS for patients with ITM exceeds that of patients with distant metastatic disease (83%, 69% and 32% for stage IIIB, IIIC and IIID disease), a significant percentage of ITM patients experience morbidity from their disease and may eventually develop distant metastases.3 4 Surgical excision has been the mainstay of treatment for ITM. However, there is limited evidence to guide therapy when ITM is either clinically or technically unresectable. Locoregional approaches including topical therapies, intralesional injections, radiotherapy, laser ablation and isolated limb infusion or perfusion (ILI) have demonstrated efficacy.5 Intralesional injections with PV-10 (Rose Bengal) or talimogene laherparepvec (T-VEC) produce durable responses, with complete response (CR) rates of 26% and 16%, respectively, in patients with stage IIIB–IV disease.6 7 Similarly, ILI has demonstrated a CR rate of 38% with a median duration of response of 13 months.8 However, responses in these studies should be interpreted with care as majority of were small single arm studies or case series.
Systemic therapies are increasingly used in unresectable stage III melanoma including patients with ITM. ICIs have the potential to alter the natural history of ITM by preventing the development of further locoregional or distant metastases while limiting the morbidity associated with certain locoregional therapies. However, limited data exist ICI efficacy for ITM. Registration studies of ICI for metastatic melanoma did not prespecify ITM as a subgroup for analysis. These patients were included in the patient group with unresectable stage III disease which accounted for less than 10% of patients enrolled.1 2 9–11 Where this subgroup was analyzed retrospectively, conclusions were limited due to small patient numbers.1 2 9–11 The aim of this study was to confirm the response to ICI in patients with only ITM.
Methods
We conducted a retrospective review of patients with of ITM treated with ICI across three tertiary hospitals in Australia, following individual institutional ethics committee approval. Patients with local recurrence or satellites alone were not included, but patients with satellites together with other ITM were included. Patients were excluded if they had previous or synchronous metastatic disease. Data regarding patient demographics, clinicopathological staging at diagnosis and at commencement of ICI and prior regional therapies were collected from the medical record.
Overall response rate (ORR) was defined as CR plus partial response (PR) based on a composite of radiological and clinical assessments. PR was defined as clinical disease reduction of at least 50%. ITMs are often non-evaluable by response evaluation criteria in solid tumors (RECIST). Progression-free survival (PFS) was measured from ICI commencement to radiological or clinical progression or death. OS was measured from ICI commencement to death. PFS and OS were estimated using the Kaplan-Meier method and survival distributions were compared using a log-rank test.
The association between ORR and potential clinical and pathological factors were assessed using Fisher’s exact test (two sided) if nominal variables (ulceration, BRAF status, previous intralesional/ILI therapy), Exact Cochran-Armitage Trend test (one sided) if ordinal variables (number of lesions, stage at commencement) and Wilcoxon test (two sided) if continuous variables (first disease free interval, ITM disease-free interval). Analyzes were carried out using SAS (V.9.4; SAS Institute).
Results
Fifty-four patients received ICI for unresectable ITM between March 2013 and February 2018. Baseline characteristics are shown in table 1; 10 patients (19%) had BRAF mutant melanoma, 11 (20%) patients received ICI as first-line treatment for their ITM, 6 (11%) had prior ILI treatment and 17 (31%) had prior intralesional therapies (T-VEC: 2 (4%) or PV-10: 15 (28%)). Forty patients (74%) received single-agent PD-1 inhibitor (pembrolizumab or nivolumab), eight (15%) single-agent anti-CTLA-4 (ipilimumab), five (9%) combination anti-PD-1/anti-CTLA-4 (ipilimumab and nivolumab or pembrolizumab) and one (2%) combination anti-PDL-1(atezolizumab) and MEK inhibitor (cobimetinib). Other treatment modalities were used in combination with ICI in some instances: three (6%) patient received radiotherapy, one (2%) patient had intralesional injection and one (2%) patient had topical therapy.
Baseline characteristics stratified by ICI
The ORR to ICI was 54%: 14 (26%) CR; 15 (28%) PR; 9 (17%) stable disease (SD); 16 (30%) progressive disease (PD). The ORR was 58% for single agent anti PD-1, 38% for single-agent anti-CTLA-4 and 40% for anti-PD-1/anti-CTLA-4 (table 2). Ulceration, BRAF status, number of lesions, prior treatments (ILI or intralesional injection) and stage also had no significant association with ORR.
Overall response to immune checkpoint-inhibitors in patients with in-transit melanoma metastases
The median duration of follow-up was 15.1 months (95% CI 2 to 46). Twenty-five patients progressed (48%): 14 (56%) progressed locoregionally and 11 (44%) developed distant metastases. The median PFS was 11.7 months (6.3-not reached). One-year and 2-year PFS were 48% (95% CI 33% to 61%) and 39% (95% CI 23% to 55%), respectively (figure 1). Further 2-year PFS for anti PD-1, anti-CTLA-4 and anti-PD-1/anti-CTLA-4 was 30%, 50% and 80%, respectively.
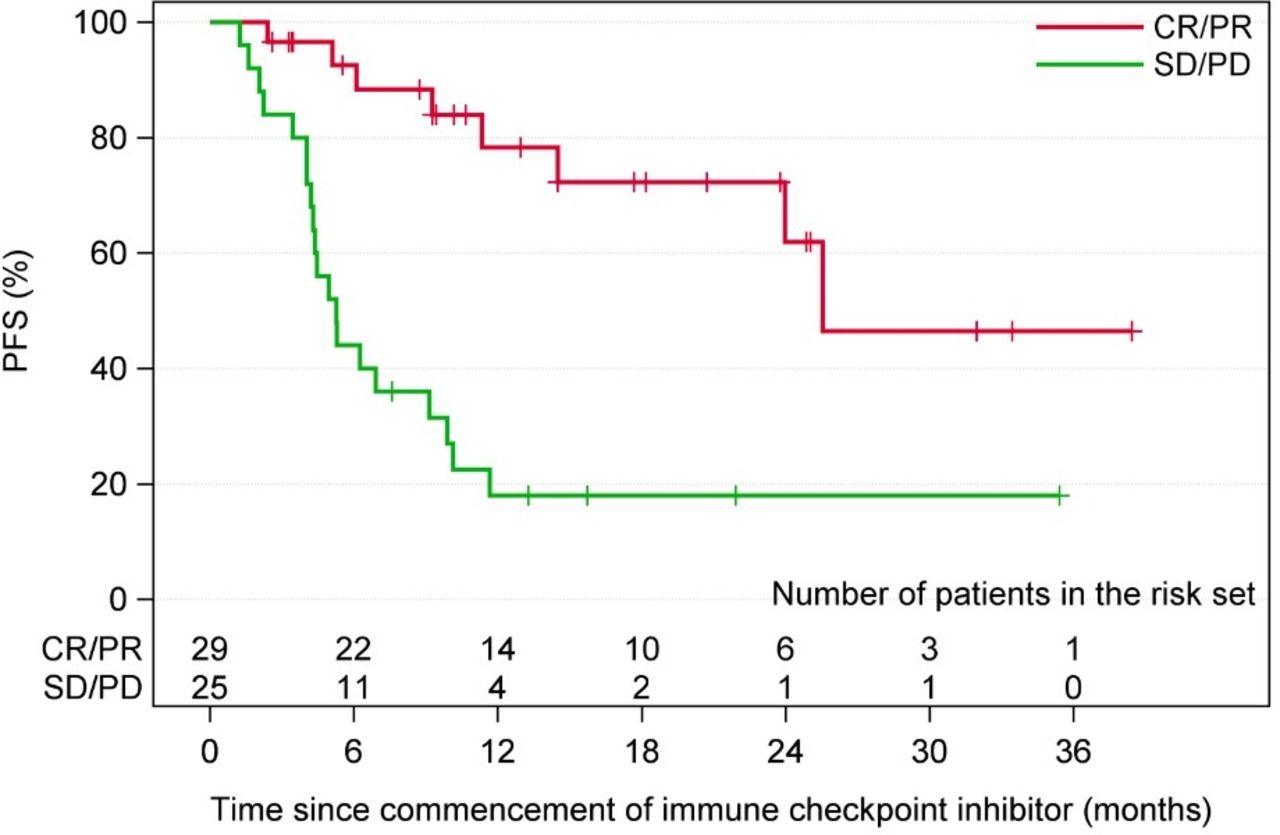
{kind=link}
CR, complete response; PD, progressive disease; PFS, progression free survival; PR, partial response; SD, stable disease.
The median OS was not reached, three (6%) patients died. One-year and 2-year OS rate were 85% (95% CI 71% to 93) and 63% (95% CI 43% to 77%), respectively. At 2 years, the OS for patients with an overall response was 85% (95% CI 50% to 96%) compared with 40% (95% CI 16% to 64%) in those who did not.
Discussion
This study demonstrates that single agent and combination ICI produces durable responses in ITM similar to rates seen in patients with stage IV melanoma. The 2-year PFS of 39% and 2-year OS of 63% are consistent with landmark survival data from registration studies for ICI in unresectable stage III and stage IV melanoma (pembrolizumab resulted in a 5-year OS of 34% study and ipilimumab/nivolumab a 4-year OS rate of 53%).1 2 9–11 Objective measurements of responses are challenging in the ITM population as the majority of patients have disease which is non-evaluable by RECIST. Thus, this study relied on subjective clinician assessed responses as well as radiological responses, a significant limitation. The lower than expected response rate in the anti-PD-1/anti-CTLA-4 group may be due to the small sample size and higher relative disease burden.
While ICI is clearly an effective treatment for ITM, there is minimal data to guide how ICI could be optimally integrated with other commonly used locoregional therapies for ITM. For patients with slowly progressing, isolated or low volume ITM, surgical resection remains a standard of care, however, for patients with rapidly progressive disease the selection of locoregional therapies, ICI or a combination of both is unclear. A phase 1b/2 study evaluating the combination of PV-10 and pembrolizumab in 23 patients with stage IIIB–IV M1c melanoma demonstrated a CR rate of 77%.12 Further, a phase II study of 18 patients with stage IIIB–IV melanoma (previous treatment not reported) examined the efficacy of ILI in combination with ipilimumab. This study demonstrated a CR rate of 65% and a 1-year PFS of 57%.13 Therefore, combinations of locoregional therapy and ICI may produce higher ORR and more durable responses than either treatment in isolation and warrants further examination in larger studies; such as MASTERKEY-265 comparing pembrolizumab with or without T-VEC (NCT02263508). In our retrospective analysis, prior treatment with ILI or intralesional injections was not associated with higher response rates to subsequent ICI therapy.
Conclusion
This multi-institutional study provides the largest evidence base of durable responses to ICI in patients with ITM, demonstrating this to be an effective treatment in patients with with unresectable ITM or disease recurrence despite locoregional therapies. Prospective studies specifically targeting this unique population are needed to confirm the efficacy of ICI and to determine optimal sequencing of treatment and potential locoregional combinations.
Acknowledgments
Melanoma Research Victoria, Queensland Melanoma Project, Melanoma Institute Australia.
Footnotes
Twitter @julialaikwon, @davidgyorki
ENT and JL-K contributed equally.
Correction notice Since the online publication of this article, the authors noticed that the middle initial for author ‘Georgina V Long’ was missing. This has been corrected.
Contributors ENT: Conceptualization, data collection and curation, project administration, writing—original draft. JL-K: Conceptualization, writing—original draft. MAR: data collection and curation, writing—review and editing. LN: statistical analysis. JB: data collection and curation. TR: data collection and curation. VA: writing—review and editing. GA-Y: writing—review and editing. GL: writing—review and editing. GAM: writing—review and editing. SS: writing—review and editing. RS: Conceptualization, supervision, data collection and curation, writing—review and editing. EW: writing— review and editing. AM: Conceptualization, supervision, data collection and curation, writing—review and editing. MS: writing—review and editing. DEG: Conceptualization, project administration, resources, supervision, writing—review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests VA—Advisory Boards: BMS, MSD, Merck, Novartis, Roche, Pierre Fabre. Travel Support: BMS, Onco-sec. Speakers Fee: BMS, MSD, Merck, Novartis, Roche. GL—consultant advisor to Aduro, Amgen, Array pharmaceutical, BMS, MSD, Novartis, Roche, Pierre-Fabre. SS—consultant advisor to Astra Zeneca, MSD, Novartis, BMS, Amgen, Roche and Janssen. RS—Advisory board MSD, Novartis and speaking honoraria BMS. AM—consultant advisor to BMS, MSD, Novartis, Roche, Pierre-Fabre. DEG—advisory board and received honoraria from Amgen and from Provectus.
Patient consent for publication Not required.
Ethics approval Individual institutional ethics committee approval was obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. The datasets generated during and/or analysed during the current study are not publicly available due to patient confidentiality but are available from the corresponding author on reasonable request.