Article Text

Abstract
Bispecific antibodies (bsAb) and chimeric antigen receptor (CAR) T cells allow for antibody guided recruitment of T cells against tumors. Both are successfully used for treatment of CD19 expressing leukemias, but may cause cytokine release syndrome (CRS) as a major dose-limiting side effect. For CRS prevention, steroids are recommended prior to bsAb treatment, despite their well-known lymphotoxic activity. The IL-6 receptor antibody tocilizumab is established for treatment of CRS induced by CAR T cells, but was not considered for CRS prevention in bsAb therapy. We here compared the influence of dexamethasone and tocilizumab on bsAb-mediated T cell proliferation and tumor lysis in vitro and in vivo and found that dexamethasone profoundly inhibited T cell proliferation and antitumor activity as induced by two different bsAb, particularly at low effector:target ratios, whereas tocilizumab did not affect efficacy. When we applied tocilizumab early during treatment of three patients with a newly developed PSMAxCD3 bsAb, significant CRS attenuation despite high IL-6 serum levels was observed. Thus, early IL-6 blockade may reduce the undesired sequelae of CRS upon bsAb therapy without affecting therapeutic activity, allowing in turn for safe application of effective doses.
- immunotherapy
- antibodies, neoplasm
- lymphocyte activation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Bispecific antibodies (bsAb) and chimeric antigen receptor (CAR) T cells are successful strategies for cancer immunotherapy.1 2 However, both reagent types can cause life-threatening cytokine release syndrome (CRS).1 3 In case of blinatumomab, a benchmark bsAb with CD19xCD3 specificity, this side effect limits safely applicable doses to approximately 30 µg/day resulting in serum levels <1 ng/mL1, which appears not sufficient to achieve optimal therapeutic activity. To prevent CRS, dexamethasone (16 mg) is usually applied prior to the first cycle of blinatumomab and other bsAbs.4 However, there are conflicting data as to whether this medication does affect bsAb-mediated T cell activation and tumor cell killing. Brandl et al did not report any inhibitory effect of dexamethasone on blinatumomab-mediated tumor cell lysis.5 However, a recent publication reports inhibition of bsAb-mediated T cell activation and tumor cell killing by dexamethasone during long-term stimulation.6 Moreover, steroid medication did not significantly increase the maximal tolerated dose of a CEAxCD3 bsAb in a recent clinical study.7
Meanwhile, the IL-6 receptor antibody tocilizumab is approved for treatment of severe CRS induced by CAR T cells based on several case reports8 9 and there is growing evidence supporting its efficacy in treating established bsAb-mediated CRS.10 11 When we compared the influence of dexamethasone to that of tocilizumab on bsAb-induced T cell proliferation and tumor cell lysis, we found that dexamethasone profoundly inhibited therapeutic activity, whereas tocilizumab did not. Based on these findings we used early tocilizumab treatment for prevention of CRS in three patients with prostate carcinoma treated with the newly developed PSMAxCD3 bsAb CC-1.
Methods
Cells and reagents
Blood was drawn from healthy donors . Peripheral blood mononuclear cells (PBMCs) were isolated using density gradient centrifugation with Biocoll cell separation solution (Biochrom, Berlin, Germany). The prostate carcinoma cell line LNCaP and the acute lymphatic leukemia cell line Nalm-16 were purchased from the German Collection of Microorganisms and Cell Cultures (DMSZ, Braunschweig, Germany) and were routinely tested negative for mycoplasma. PBMCs and cell lines were kept in RPMI 1640 supplemented as described earlier.12 Dexamethasone (Sigma-Aldrich) was dissolved in RPMI 1640 including 10% FCS and kept at −20°C until use. Dexamethasone (Sigma-Aldrich) was dissolved in RPMI 1640 including 10% FCS and stored at −20°C.
Antibodies and flow cytometry
The recombinant bsAb CC-1 (PSMAxCD3 specificity, online supplementary figure 1A) was generated at our institution in the IgGsc format based on the format published by Coloma and Morrison1 (Zekri et al, manuscript submitted December 2019). The PSMA and CD3 binding sites are comprised of the newly generated hybridoma-derived IgG2b antibody 10B3 and a single chain derived from the CD3 antibody UCHT-1, respectively. Fc receptor binding and complement fixation was attenuated by introducing mutations in the CH2 domain (online supplementary figure S1A).
Supplemental material
The humanized anti-IL-6 receptor antibody tocilizumab was purchased in clinical quality from Hoffmann-La Roche (Basel, Switzerland). The bispecific CD19xCD3 BiTE antibody blinatumomab (online supplementary figure S2A) was purchased from Amgen (Thousand Oaks, USA). Flourochrome-labeled antibodies against CD4, CD8, CD10, CD276 and the respective isotype control antibodies were purchased from BioLegend (San Diego, USA). CD45-AmCyan was purchased from BD Biosciences (Franklin Lakes, USA).
Supplemental material
For flow cytometry based lysis assays, 50,000 PSMA+ LNCaP cells or 100,000 CD19+ Nalm-16 cells were incubated in 96 well plates together with 32,500–1,000,000 PBMCs, bsAb at 1 µg/mL and blocking reagents (0,1 µg/mL dexamethasone or 10 µg/mL tocilizumab). After 3 days, flow cytometric analysis was performed. LNCaP cells were defined as CD45-CD276+, Nalm-16 as CD45-CD10+, and T cells as CD45+CD4+ or CD45+CD8. Absolute cell numbers were determined by the acquisition of a defined amount of compensation particles (BD Biosciences) per sample.2 Binding of antibodies to Fc receptors was blocked with Flebogamma DIF (Grifols, Barcelona, Spain) at 50 µg/mL. Data acquisition was performed using a FACSCanto II (BD Biosciences). For data analysis, FlowJo V.10 software (Tree Star, Ashland, OR) was used.
T cell proliferation assay
PBMCs from healthy donors (100,000 cells/well) and irradiated (100 Gy) target cells (E:T ratio 1:1) were seeded in triplicates in 96 well plates and incubated with bsAb (1 µg/mL). After 48 hours, cells were pulsed with 3H-methyl thymidine (0.5 µCi/well) and incubated for another 20 hours until they were harvested on filter mats. Incorporated radioactivity was determined using a liquid scintillation counter (MicroBeta2 2450 Microplate counter, PerkinElmer, Waltham, USA).
Impedance-based real-time assessment of tumor cell killing
To observe real-time killing of PSMA +tumor cells, xCELLigence assays were performed. Adherent LNCaP cells (30,000 cells/well) were seeded in a 96 well E-plate and incubated for 20 hours. After constitution of adequate cell indices (>1.5), indices were normalized to 1.0. Then, PBMCs (100,000 cells/well) and a bispecific PSMAxCD3 antibody at 1 µg/mL together with the respective blocking agents were added and cell indices were measured every 15 min to determine viability of the tumor cells.
Animal model
Animal experiments were performed in accordance with the German Animal Protection Law and after authorization by the competent authority of the state of Baden-Württemberg (Regierungspräsidium Tübingen, authorization number M9/17). Six weeks old NOD.Cg-Prkdcscid Il2rgtm1Wjl /SzJ (NSG) mice (Charles River Laboratories, Wilmington, USA) were injected subcutaneously with 1,000,000 PSMA+ LNCaP tumor cells into the flank. After formation of large palpable tumors (approximately 4 mm after 7 days), mice were injected intravenously with 5 µg dexamethasone or 200 µg tocilizumab (d1). One hour later, 10,000,000 human PBMCs were applied intraperitoneally as well as 2 µg of a PSMAxCD3 antibody CC-1 (intravenous). Treatment with the same amount of PMBC in combination with CC-1 was repeated at days 8 and 15. Tumor size was measured every 2 days and mice were euthanized if signs of sickness occurred or tumor size exceeded 14 mm.
Patients
Patients with castrate-resistant metastatic prostate carcinoma were treated with the bispecific PSMAxCD3 antibody CC-1 and tocilizumab in an individualized experimental approach. CC-1 was produced in compliance with good manufacturing process standards according to section 13 (2b) of the German Medicines Act and applied using an individual dose escalation protocol. Body temperature was monitored at least every 2 hours. For monitoring purposes, IL-6, C reactive protein (CRP) and solubIe IL-2 receptor (sIL-2R) levels were assessed daily using ELISA at the central laboratory of the University Hospital Tübingen. After the first occurrence of fever ≥38.5°C, 400 mg tocilizumab was applied. Patient samples were tested for human antihuman antibodies by ELISA at the University Hospital Tübingen. To this end, (Fab)2 fragments of CC-1 were coated as capture antibody. After blocking, serum samples of patients were added and specific binding of human antihuman antibodies to (Fab)2 fragments was detected by addition of goat-antihuman HRP-conjugated secondary antibodies.
Statistical analysis
Data are displayed as mean±SD. For statistical analysis, Graphpad V.10 was used. If not otherwise stated, Mann-Whitney U tests were used to test for statistical significance in unpaired data sets.
Results
Inhibition of T cell proliferation and tumor cell killing in vitro
Figure 1A shows T cell proliferation in cocultures of PBMC and irradiated PSMA+ tumor cells in the presence of the PSMAxCD3 bsAb CC-1. BsAb induced T cell activation and proliferation was markedly inhibited by increasing concentrations of dexamethasone but not by tocilizumab. Of note, a serum concentration of 1–5 µg/mL of tocilizumab is therapeutically highly effective.13 Serum concentrations of >0,1 µg/mL dexamethasone are easily reached after intravenous application of 16mg,14 the recommended dose for CRS prevention during blinatumomab treatment. We therefore chose this concentration of dexamethasone and compared it to 10 µg/mL of tocilizumab in experiments that assessed bsAb-mediated T cell proliferation and tumor cell killing at different E:T ratios and in several independent assay systems (figure 1B, online supplementary figure1C-D).
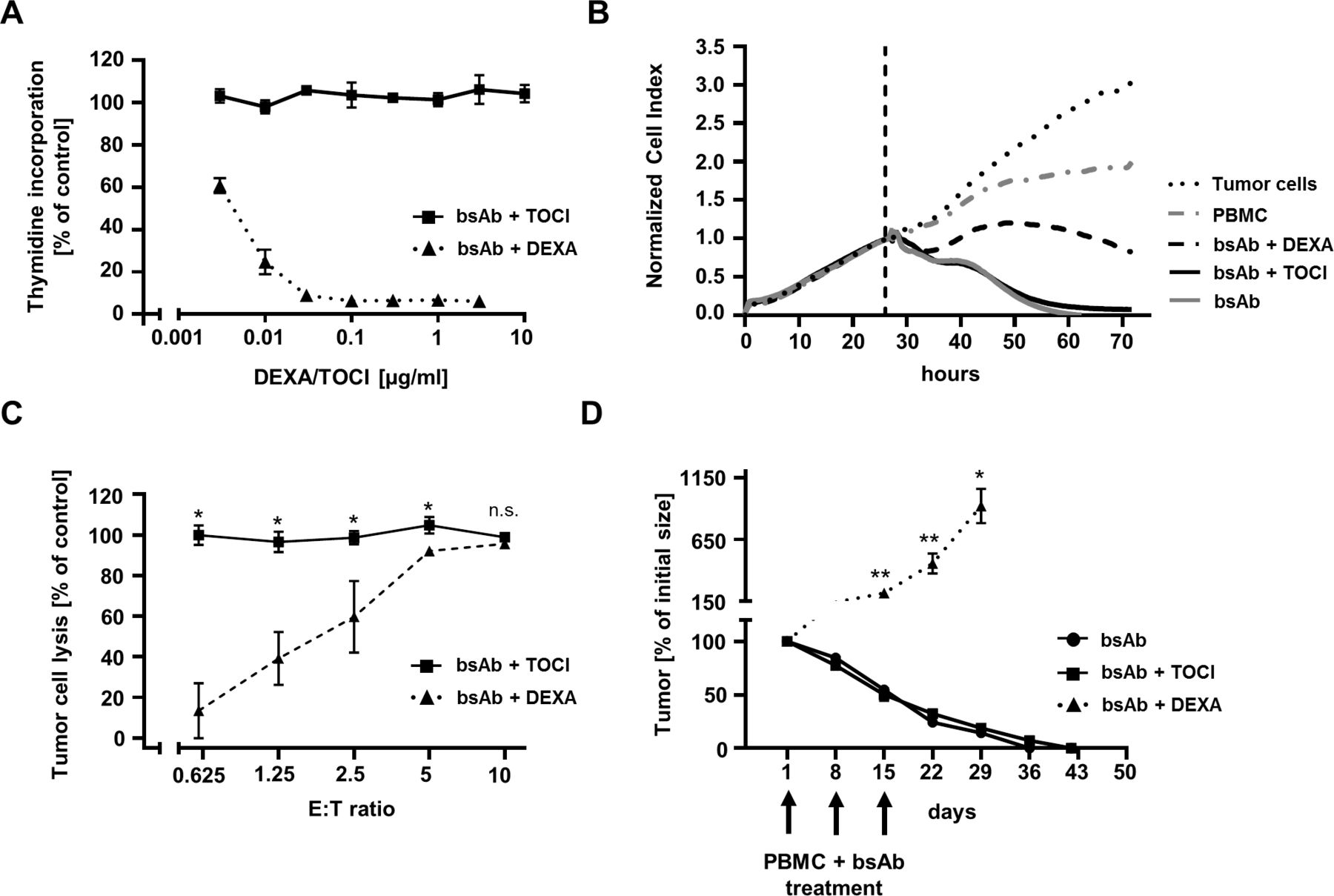
T cell proliferation and tumor cell lysis in the presence of dexamethasone or tocilizumab in vitro and in vivo. (A) PBMC of healthy donors (n=3) were incubated with the PSMAxCD3 bispecific antibody (bsAb) CC-1 (1 µg/mL) in the presence of PSMA+ LNCaP cells for 72 hours (effector:target (E:T) ratio 2:1) and additionally treated with tocilizumab (TOCI) or dexamethasone (DEXA) at the indicated concentrations. T cell proliferation was assessed by thymidine uptake assays. (B) LNCaP cells were used in xCELLigence assays. After 24 hours, cell indices were normalized and tumor cell lysis was measured after addition of PBMC of healthy donors (E:T = 3.3:1) as well as CC-1 (bsAb, 1 µg/mL) and TOCI (10 µg/mL) or DEXA (0.1 µg/mL). Cell indices were measured every 15 min and represent the amount of viable tumor cells. Representative data from three independent experiments are shown. (C) Tumor cell lysis was assessed in a flow cytometry-based assay with PBMC of healthy donors (n=4) and LNCaP cells at different E:T ratios for 72 hours in combination with CC-1 (1 µg/mL) and TOCI (10 µg/mL) or DEXA (0.1 µg/mL). (D) NSG mice (n=5 per group) with established LnCaP flank tumors were repeatedly treated with PBMC in combination with CC-1 (2 µg/mouse) (d1, d8, d15) and TOCI (200 µg/mouse) or DEXA (5 µg/mouse) (d1). Statistical analysis was done using Mann-Whitney U test. *p<0.05; **p<0.01; n.s. not significant.
Dexamethasone markedly inhibited T cell proliferation, but tumor cell killing was not suppressed at E:T ratios ≥5 (figure 1C, online supplementary figure 2C). This is in line with the findings reported by Brandl et al and Li et al.5 6 At lower ratios, however, that certainly reflect the situation at an established tumor more closely, a marked inhibition of tumor cell killing was observed.
The extent of inhibition depended on the bsAb concentration with more pronounced inhibition at lower, non-saturating concentrations (online supplementary figure 1E). In marked contrast to dexamethasone, tocilizumab inhibited neither bsAb induced T cell proliferation nor tumor cell killing.
To rule out that the observed effects were due to the chosen target antigen or bsAb format, we also performed experiments with blinatumomab (online supplementary figure 2A). Again, a marked inhibition of T cell proliferation and killing of leukemia cells by dexamethasone but not tocilizumab was observed (online supplementary figure 2C-E).
Inhibition of antitumor activity in vivo
To evaluate whether bsAb-mediated antitumor effects in vivo were affected, an established efficacy model using NSG mice with large established PSMA+ expressing tumors was used. Of note, mice of either group did not develop signs of CRS during the treatment. Establishment of CRS in a xenograft model relies on IL-6 production by monocytes15 and can only be achieved by massive tumor loads, for example, in the peritoneal cavity,16 17 which was not the case in our experiments. A single application of 5 µg dexamethasone prior to a 3-week treatment with PBMCs and the PSMAxCD3 bsAb CC-1 led to complete abolition of bsAb activity and almost unrestricted growth of established tumors. In contrast, tocilizumab did not inhibit the rapid and sustained regression of the tumors (figure 1D).
CRS prevention by early application of tocilizumab in bsAb-treated patients
Based on these results, three patients treated with the bsAb CC-1 in individual experimental approaches received tocilizumab to prevent CRS. Application of tocilizumab (400 mg) was initiated at a first fever episode of >38.5°C that occurred at IL-6 levels of 20–100 pg/mL. After tocilizumab application IL-6 levels rose to >4000 pg/mL on further dose escalation, but body temperature declined, and additional antipyretic treatment was not required (figure 2). Profound activation of T cells in the peripheral blood was demonstrated by markedly elevated sIL-2R (figure 2) and CD69 expression levels (Zekri et al, manuscript submitted December 2019). However, CRP levels did not exceed 9 mg/dL (online supplementary figure 3).
Supplemental material

{kind=link}
{kind=link}
Temperature and cytokine release of three patients treated with a bispecific antibody (bsAb) and tocilizumab (TOCI). The PSMAxCD3 bsAb CC-1 was applied to three patients on compassionate use basis in an individual dose escalation regime as indicated. The bsAb was applied as continuous infusion over 22 hours. TOCI was applied as soon as body temperature reached 38.5°C (dotted line). Serum IL-6 levels and soluble IL-2 receptor (sIL-2R) levels were determined by ELISA at the central laboratory of the University Hospital Tübingen. Temperature was measured at least every 2 hours. Each panel (A–C) represents one individual.
Major side effects did not occur in two patients receiving the target bsAb dose of 2.4 mg (figure 2A–B) (American Society for Transplantation and Cellular Therapy (ASTCT) CRS consensus grading 1).18 A third patient (figure 2C) experienced atrial fibrillation and subsequent pulmonary edema and infection at a dose of 1.2 mg (ASTCT CRS grade 3).18 After application of high dose steroids (prednisolone 500 mg), CRS symptoms resolved within days. We assume that these complications were due to the particular history of this patient including bone marrow transplantation and cryptogenic pneumonias after being diagnosed with malignant lymphoma several years ago. We detected human antihuman antibodies against (Fab)2 fragments of CC-1 that may have facilitated the elimination of tocilizumab in this patient. However, it is also likely that this patient experienced a case of at least partially tocilizumab-refractory CRS that was resolved by application of steroids. This hypothesis is supported by the rapid response to high dose steroid treatment. While steroids are needed for the treatment of severe CRS in some cases, the doses applied for this indication are much higher than the prophylactic dose used prior to bsAb treatment and thus most certainly abrogate therapeutic activity of bsAb. Notably, all patients experienced a rapid and profound (≥50%) reduction of elevated prostate specific antigen (PSA) levels (Zekri et al, manuscript submitted December 2019).
Discussion
bsAb and CAR T cells directed to the B cell antigen CD19 are currently used with considerable success for immunotherapy of B cell derived leukemias. However CRS is a major dose-limiting side effect of these functionally closely linked strategies for recruitment of T cells and its underlying mechanisms are incompletely understood.
Although CRS in CAR T cells and bsAb appears similar in regard to the clinical presentation, its pathophysiology might be different. Conclusions drawn from CAR T cell mediated CRS might not be fully transferable to bsAb treatment, since the time course of T cell expansion, availability of costimulation and cytokine release differ significantly between CAR T cells and bsAb.6 16 17 Therefore, scientific work regarding bsAb-induced CRS is urgently needed.
The application of dexamethasone is recommended before the first cycle of the bench mark bsAb blinatumomab to prevent CRS. This procedure has been confirmed by a paper that failed to detect inhibitory effects of dexamethasone on blinatumomab-mediated in vitro T cell activation and tumor cell lysis.5 In contrast, Li et al recently described inhibition of tumor cell killing by dexamethasone, both in vitro using human T cells and in vivo by using a MMTV.huHER2.FVB/n transgenic mouse model and a HER2xCD3 bsAb.6 Our data further support the observation of reduced bsAb-mediated tumor cell killing in the presence of dexamethasone in vitro and in vivo using human primary T cells. Furthermore we describe T cell proliferation as being significantly impaired by dexamethasone, which was not assessed by Li et al. In order to address the apparent contradiction of the findings by Li et al and that by Brandl et al, we identified unfavorable E:T ratios and low bsAb concentrations as factors that amplify the inhibitory properties of steroids.
In our opinion the pronounced and clear-cut inhibition of bsAb activity in vitro and in an established tumor model strongly suggests that steroids should be used with caution for the prevention of CRS, since therapeutic activity could be impaired. While steroids might not be optimally suited as comedication, it is obvious that potential CRS severely limits applicable doses of bsAb as well as CAR T cells and thus a strategy that allows for attenuation of CRS without affecting therapeutic activity is urgently needed.
In recent years it became apparent that the IL-6 receptor antibody tocilizumab is highly effective for treatment of CRS induced by CAR T cells and in the mean time it is approved for this indication based on successful application as reported in several cases.8 9 Likewise, evidence for the activity of this drug against bsAb-induced CRS is accumulating.10 11 However, preclinical data on the use of IL-6 blockade as well as on a potential interference with therapeutic activity particularly of bsAb are scarce. Singh et al showed that macrophages rather than CAR T cells are the source of IL-6 during therapy.15 This was further confirmed by more recent work.16 17 Li et al described that IL-6 or IL-6 receptor blockade does not interfere with bsAb-mediated T cell activation and tumor cell lysis.6 Our data support this observation. We further noticed no negative influence of tocilizumab on T cell proliferation at different E:T ratios as well as in a mouse model using human primary T cells.
These findings prompted us to include early concomitant application of tocilizumab during individual experimental therapeutic approaches with the newly developed PSMAxCD3 bsAb CC-1. All patients received tocilizumab early during treatment with CC-1 after the first spike of fever. Despite rising IL-6 levels, temperatures did not exceed 39°C. Several publications have established that severe CAR T cell-mediated CRS is associated with IL-6- and CRP levels of >1000 pg/mL and >16 mg/dL, respectively.18–21 In our patients, the temperature course as well as high IL-6 serum levels combined with (relatively) low CRP values suggest that IL-6 receptor blockade prevented development of higher-grade CRS. The enzyme-linked assay used by us was validated and showed only minimal variations in the presence of tocilizumab.
Neither patient showed any signs of neurotoxicity during treatment with CC-1. In the cohort 3 of the ZUMA-1 trial, patients that received tocilizumab early during application of 19.28.z CAR T cells had a reduced incidence of ≥grade 3 CRS, but a higher rate of all-grade neurotoxicity.22 However, the latter might be closely linked to the chosen target antigen, since neurotoxicity is almost absent in CAR T cell trials targeting solid tumors3 and is rarely seen with CD22 CAR T cells.23 It should be noted that ineffective CAR T cells directed against CD19+ or solid tumors cannot be denominated as safe, since the occurrence of side effects correlates with clinical efficacy. However, the clinical outcome seen with tocilizumab in a single CAR T cell trial cannot be transferred to bsAb treatment directly. Therefore, more extensive clinical studies are needed to compare steroids and tocilizumab for the treatment of bsAb-mediated CRS.
Clearly, cytokines other than IL-6 may be involved in the pathogenesis of CRS6 16 17 24 and an evaluation of the role of IL-6 blockade in the pathophysiology of CRS requires further investigation. However, we conclude that IL-6 blockade may be successfully used for the prevention of CRS induced by bsAb without impairing T cell functionality. A first-in-human clinical study including CC-1 and tocilizumab application is approved and started recruiting in Q4/2019.
Acknowledgments
The authors thank Carolin Walker, Beate Pömmerl and Janina Palm for expert technical assistance, and Reinhild Klein for performing the HAHA assay. The authors thank Markus Löffler for advice regarding statistics.
References
Footnotes
Contributors GJ, HRS and JK designed research. JK, LO and SH performed and analyzed the in vitro experiments. SM and MM performed animal experiments. JSH and JK were substantially involved in monitoring patients during treatment. H-GR and LZ contributed to experimental designs. JK, GJ and HRS wrote the manuscript. All authors read, revised and accepted the submitted manuscript.
Funding This work was supported by the German Cancer Consortium (DKTK), the Helmholtz validation fund (OPTIMAB), the Deutsche Forschungsgemeinschaft (SA1360/9-1 and SA1360/7-3), the Wilhelm Sander-Stiftung (2007.115.3), the Deutsche Krebshilfe (111828 and 70112914) and Germany’s Excellence Strategy (EXC 2180/1).
Competing interests GJ, HRS, and LZ are listed as inventors on the patent application “Novel PSMA bindingantibody and uses thereof”, EP16151281, applicant German Cancer Research Center, Heidelberg, Germany.
Patient consent for publication Not required.
Ethics approval Drawing of blood from healthy donors was approved by the ethics committee of the University Hospital Tübingen, authorization number 156/2012BO1. Patients with castrate-resistant metastatic prostate carcinoma were treated with the bispecific PSMAxCD3 antibody CC-1 (NCT04104607) and tocilizumab in an individualized experimental approach pursuant to Article 37 of the Declaration of Helsinki of the World Medical Association after providing written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Original data and materials are available from the corresponding author upon reasonable request.