Article Text

Abstract
Background Recently, anti-CD38 monoclonal antibody (Mab) therapy has become a focus of attention as an additional/alternative option for many hematological neoplasms including T-cell acute lymphoblastic leukemia (T-ALL). It has been shown that antitumor efficacy of anti-CD38-Mab depends on the level of CD38 expression on tumor cells. Reports on CD38 expression in T-ALL are scarce, and data on the effect of cytotoxic chemotherapy on CD38 expression are limited to very few samples. Moreover, it lacks entirely in refractory disease and in adult T-ALL. We report the flow cytometric evaluation of CD38 expression in T-ALL blasts at diagnosis and the effect of cytotoxic chemotherapy on its expression in measurable residual disease (MRD), refractory disease (MRD≥5%), and relapsed disease in a large cohort of T-ALL.
Methods The study included 347 samples (188 diagnostic, 100 MRD, 24 refractory and 35 relapse samples) from 196 (children: 85; adolescents/adults: 111) patients with T-ALL. CD38-positive blasts percentages (CD38-PBPs) and expression-intensity (mean fluorescent intensity, CD38-MFI) were studied using multicolor flow cytometry (MFC). MFC-based MRD was performed at the end-of-induction (EOI-MRD, day 30–35) and end-of-consolidation (EOC-MRD, day 78–85) subsequent follow-up (SFU-MRD) points.
Results Patients were classified into early thymic precursor subtype of T-ALL (ETPALL, 54/188, 28.7%), and non-ETPALL (134/188, 71.3%). Of 188, EOI-MRD assessment was available in 152, EOC-MRD was available in 96 and SFU-MRD was available in 14 patients. CD38 was found positive in 97.9% (184/188) of diagnostic, 88.7% (110/124) MRD (including 24-refractory) and 82.9% (29/35) relapsed samples. Median (95% CI) of CD38-PBPs/MFI in diagnostic, MRD, refractory, and relapsed T-ALL samples were, respectively, 85.9% (82.10%–89.91%)/4.2 (3.88–4.47), 74.0% (58.87%–83.88%)/4.6 (3.67–6.81), 79.6% (65.25%–96.11%)/4.6 (3.33–8.47) and 85.2% (74.48%–93.01%)/5.6 (4.14–8.99). No significant difference was noted in CD38 expression between pediatric versus adult and patients with ETPALL versus non-ETPALL. No change was observed in CD38-MFI between diagnostic versus MRD and diagnostic versus relapsed paired samples. However, we noticed a mild drop in the CD38-PBPs in MRD samples compared with the diagnostic samples (p=0.016).
Conclusion We report an in-depth analysis of CD38 expression in a large cohort of T-ALL at diagnosis, during chemotherapy, and at relapse. Our data demonstrated that CD38 is robustly expressed in T-ALL blasts with a little effect of cytotoxic chemotherapy making it a potentially effective target for antiCD38-Mab therapy.
- translational medical research
- receptors, antigen
- immunotherapy
- hematologic neoplasms
- antigens, neoplasm
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- translational medical research
- receptors, antigen
- immunotherapy
- hematologic neoplasms
- antigens, neoplasm
Background
T-cell acute lymphoblastic leukemia (T-ALL) is a genetically heterogeneous aggressive hematological malignancy of precursor T-cells that accounts for 10%–15% of pediatric and 20%–25% of adult patients with ALL.1 2 Despite advancements in therapeutic strategies in ALL, the clinical outcome of T-ALL remains inferior to B-cell lymphoblastic leukemia (B-ALL).2–4 Unlike the refractory/relapsed B-ALL, it is challenging to treat the patients with refractory/relapsed T-ALL, especially after allogeneic hematopoietic stem cell transplant.5–7 Further, the early thymic precursor subtype of T-ALL (ETPALL), which accounts for 10%–15% of T-ALL, has been shown to have a poorer clinical outcome in adult patients.2 4 6 8 9 Unfortunately, since the approval of nelarabine, no new agent has been approved for T-ALL and efforts are undergoing for evaluating the newer agents.6
An exciting recent achievement of modern cancer therapy is the targeted immunotherapy which has broadened the spectrum of therapeutic options for various malignancies, and monoclonal antibody (Mab) therapy is one of them. Mab specifically binds to a target molecule (epitope) expressed on the surface of cancer cells. In the last few years, daratumumab, a Mab against CD38, has been shown to be the most successful agent for the treatment of multiple myeloma (MM, a plasma cell malignancy with high levels of surface CD38 expression) and has gained rapid approval for the same.10–13 It is also being considered as an exciting option for other hematological neoplasms expressing CD38.14 CD38, a transmembrane glycoprotein and an ectoenzyme, is expressed in a variety of hematopoietic cells like plasma cells, myeloid/B-cells progenitor cells, monocytes, germinal center lymphocytes, natural killer (NK) cells, dendritic cells, and so on.15 It is variably expressed in many hematological neoplasms such as B-ALL, acute myeloid leukemia, Burkitt lymphoma, chronic lymphocytic leukemia, MM, and so on,14 15 which makes anti-CD38 Mab therapy as a potential therapeutic option in these malignancies. In early 2018, our bone marrow (BM) transplant unit has demonstrated the potential use of daratumumab in a patient with T-ALL with post-transplant refractory disease who remains disease-free for the last two and a half years.7 More recent preclinical studies of anti-CD38 therapy in T-ALL have also demonstrated promising results making it a potential therapeutic agent for future clinical trials.16–18 Hence, anti-CD38 Mab therapy is being considered as an exciting potential therapeutic option for high-risk T-ALL.
The mechanism of action of anti-CD38 Mab-like daratumumab involves Fc-dependent immunological reactions like complement-dependent cytotoxicity, antibody-dependent cell-mediated cytotoxicity, antibody-dependent cellular phagocytosis, and so on.13 These mechanisms are also dependent on the levels of target antigen on tumor cells.19–22 In 2016, Nijhof et al have shown that the low levels of CD38 expression can affect the antitumor effect of daratumumab therapy in multiple myeloma.23 Interestingly, it has been also demonstrated that CD38 expression can be upregulated using drugs like all-trans retinoic acid and Panobinostat which can improve the antitumor efficacy of anti-CD38 Mab therapy.24 25 Therefore, the data on expression levels of CD38 in a tumor of interest is a pre-requisite for considering CD38 targeted therapy. Data on the expression level of CD38 in leukemic blasts of T-ALL are scarce and limited to the recently published small series of (21 and 8) patients.14 17 Moreover, the data on CD38 expression levels in leukemic blasts from the refractory T-ALL lack entirely. In view of the recent focus on the potential role of anti-CD38 Mab therapy in T-ALL, we have performed an in-depth study on the CD38 expression in leukemic blasts at diagnosis, in measurable residual disease (MRD), refractory disease, and relapsed disease in a large cohort of patients with T-ALL .
Patients and methods
We studied CD38 expression levels in childhood as well as adolescent and adult patients with T-ALL treated at Tata Memorial Centre, India, between October 2017 and December 2019. The study was approved by the Hospital Ethics Committee. The diagnosis of T-ALL was established based on the morphology, cytochemistry (myeloperoxidase) and flow cytometric immunophenotyping (online supplementary table S1) in accordance to WHO 2016 guidelines.26 Patients were classified into two groups based on the immunophenotype at diagnosis that is, ETPALL27 and non-ETPALL. Pediatric patients were treated with MCP841 protocol28 29 and adolescent/adult patients were treated with BFM90 protocol.30 31 Treatment response was monitored at the end of induction (EOI) and subsequent time points for complete remission on BM aspirate morphological examination and MRD assessment.
Supplemental material
Multicolor flow cytometric (MFC) immunophenotyping
Acute leukemia diagnosis
BM or peripheral blood samples were processed for 10–11 color MFC immunophenotyping using bulk lyse and stain method as described elsewhere.32 In brief, the cell suspension was prepared by bulk erythrocyte lysing with ammonium chloride-based lysing reagent (0.15 M NH4Cl, 1.0 g KHCO3, 37 mg EDTA, and 1 L distilled water). After lysis and wash step, cells were resuspended in phosphate-buffered saline with 5% bovine serum albumin. The cell count was adjusted to get a final concentration of 2×106 cells in 80 µL and stained for immunophenotyping using 10–11 color antibody panels. The panel included an anti-CD38 antibody (clone, LS198-4-3; fluorochrome, APC-Alexa750, Beckman Coulter, Indianapolis, IN, USA). The details of clones and fluorochrome combinations are mentioned in online supplementary table S1. Followed by surface staining, the cells were fixed and permeabilized using FIX & PERM Cell Fixation & Cell Permeabilization Kit (ThermoFisher Scientific) and staining for intracellular (ic) antibodies like icCD3, icCD79a and icMPO was performed. The cells were either acquired within 4 hours of staining or fixed with 0.5% paraformaldehyde and acquired within 24 hours of fixation. Samples were acquired on a three laser 13-color Cytoflex instrument (Beckman Coulter, BC) and approximately, 100 000 to 200 000 events per tube were collected. The instrument calibration, quality control, and voltage and compensation were performed as per the manufacturer's instructions.
MRD and follow-up monitoring
MFC-based MRD was performed on BM aspirate samples at the EOI (day 30–35) and the end-of-consolidation (EOC-MRD, day 78–85). BM samples for MRD assessment were processed by bulk red cell lysis protocol described elsewhere33 using an 11-antibody, 10-color panel. In brief, the cell suspension was prepared by bulk erythrocyte lysing with ammonium chloride-based lysing reagent, and the cells were stained with the 11-antibody 10-color T-ALL MRD panel (online supplementary table S2). The MRD analysis approach was adopted from the methodology described by Wood.34 The primary MFC-MRD panel included the antibodies against surface CD3, icCD3, CD4, CD5, CD7, CD8, CD16, CD34, CD38, CD45, and CD56. An additional panel of antibodies against CD1a, CD2, CD11b, CD13, CD33, CD117 and TdT (online supplementary table S2) was used in selected challenging samples based on the knowledge of diagnostic immunophenotype. The cells were acquired on the Navios instrument (Beckman Coulter, Miami, FL, USA). Instrument set-up and daily quality controls were performed as per the manufacturers' recommendations. The limit of detection for MRD assay was established at a cluster of 40 events in 1.5 million cells (ie, 0.003%) and lower limit of quantitation at a cluster of 100 events in 1.5 million cells (ie, 0.006%). The median number of events acquired was 1 538 935 (range, 823 148 to 5 632 547 events) and we acquired ≥1.5 million cells in 63% of MRD samples. Flow cytometry data analysis was performed using predefined template-based strategy using Kaluza software V.1.3 (Beckman Coulter) as demonstrated in online supplementary figures S1A–C.
CD38 expression study
CD38 expression levels were studied in leukemic cells of T-ALL, mature granulocytes, NK cells, monocytes, and plasma cells. Gating strategies for T-ALL blasts were based on weak CD45 versus low side scatter characteristics (SSC), CD34 positive and/or CD7 strong positive expression with weak/negative surface CD3 (online supplementary figure S1A–C). Gating strategies for lymphocytes, monocytes, granulocytes were based on CD45 versus SSC and specific markers like CD13 and CD16 for mature granulocytes, CD13+HLA-DR+ for monocytes, CD7 and CD56 for NK cells and CD38-bright/CD19-positive for plasma cells. CD38 was never included in the gating strategy for any population except for plasma cells. Mean fluorescence intensity (MFI) of CD38 was determined as the geometric mean of its expression using Kaluza software, V.2.1. (Beckman Coulter). The expression levels of CD38 in T-ALL blasts were calculated as a normalized MFI (nMFI) score as described elsewhere.32 In brief, mature granulocytes were taken as a negative reference population and the median of it was assigned an nMFI score of ‘0’. Plasma cells were taken as a positive reference population and their median was assigned an nMFI score of ‘10’. MFI range between the negative and positive reference population was divided equally on a linear scale from ‘0 to 10’ (online supplementary figure S2). CD38-positive cell percentages (CD38-PBPs) were defined above the cut-off of the background of unstained cells acquired with each sample (online supplementary figure S1A; xiv, xv, xvi). The heterogeneous versus homogenous expression pattern of CD38 was studied using the coefficient of variation of immunofluorescence (CVIF).
Statistical analysis
Statistical significance of the difference between the PBPs, MFI, and CVIF of CD38 expression between leukemic blasts from different groups of T-ALL was determined using the Mann-Whitney U test. These statistical tests were performed using MedCalc Statistical Software V.14.8.1 (MedCalc Software, Ostend, Belgium) and figures were prepared in GraphPad Prism V.6.
Results
The study included 347 samples (188 diagnostic, 124 MRD and 35 relapse samples; refer to figure 1) from 196 patients (85 children with age <15 years; and 111 adolescents and adults with age ≥15 years) with an overall median age of 15 years (range, 1 to 53 years). Out of 196, 188 patients were newly diagnosed and 8 patients had samples only at relapse. Characteristics of the newly diagnosed patients (n=188) with T-ALL are described in table 1. Patients were immunophenotypically classified as ETPALL (54/188, 28.7%), and non-ETPALL (134/188, 71.3%). Of 188 new patients with T-ALL, EOI-MRD assessment was available in 152, EOC-MRD was available in 96 and subsequent follow-up (SFU)-MRD was available in 14 patients. EOI-MRD was measurable (≥0.01%) in 90 (59.2%) samples including 24/152 (15.8%) patients who were not in morphological remission (blasts>5%) and were categorized as ‘refractory’ disease. EOC-MRD assessment was available mostly in patients with EOI-MRD positive status (96/152) and was detectable (≥0.01%) in 30/96 (31.25%) samples. Of 14 SFU-MRD samples, MRD was detectable in 4/14 (28.57%) samples. Thus, we included 124 MRD samples including 24 with refractory disease. We also included 35 samples with medullary relapse (27, in 188 new T-ALL and 8, only relapses).
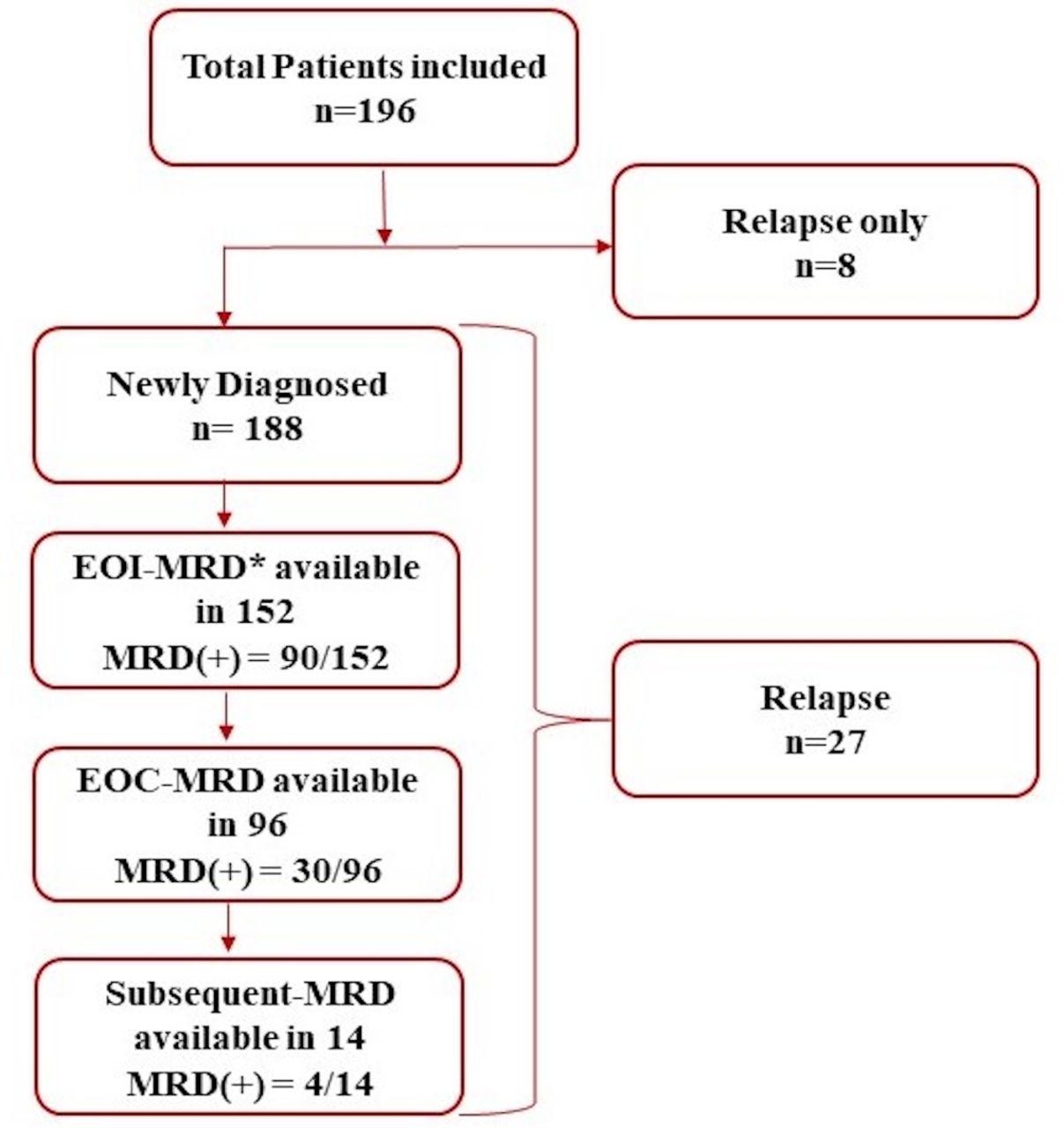
Distribution of patients with T-ALL and samples included in the study. *Included MRD samples with >5% blasts, that is, refractory disease. EOC-MRD, end of consolidation MRD; EOI-MRD, end of induction MRD; MRD, measurable residual disease; T-ALL, T-cell acute lymphoblastic leukemia.
Characteristics of newly diagnosed patients with T-ALL (n=188)
CD38 expression in diagnostic, MRD, refractory and relapse samples
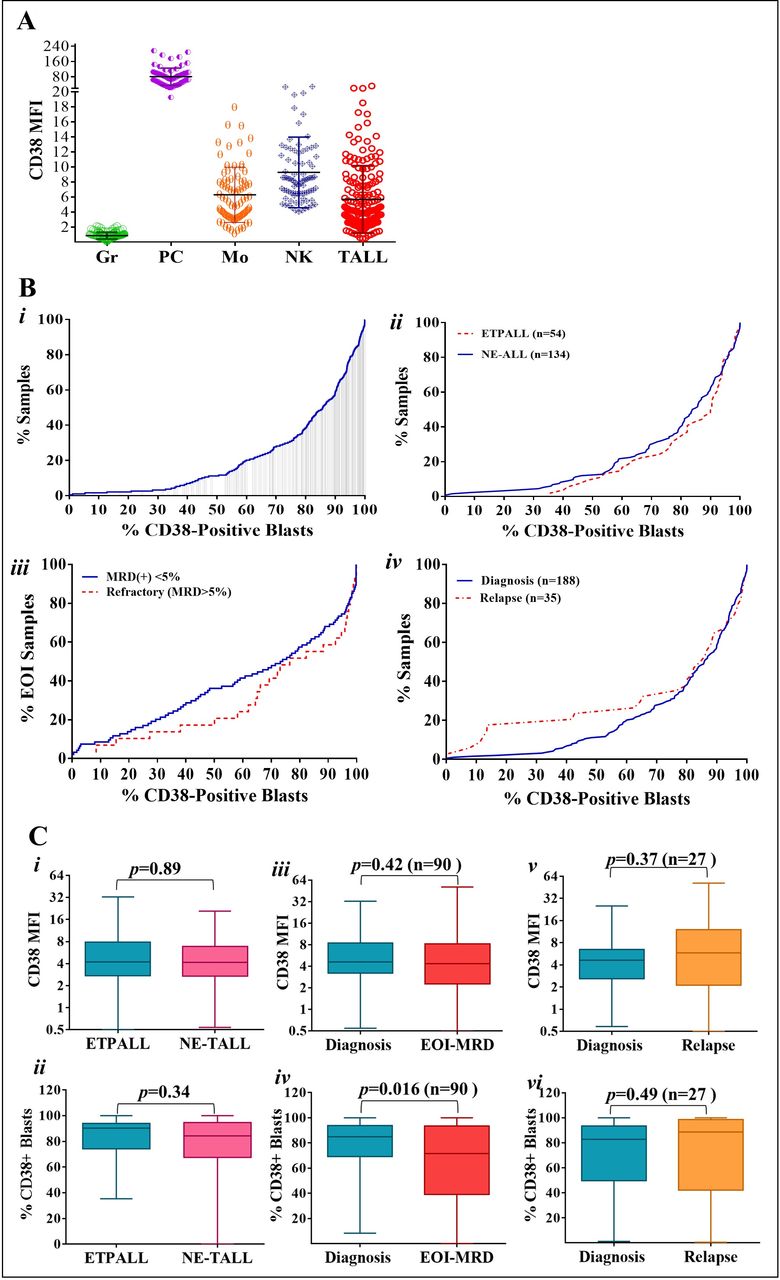
CD38-PBPs, expression levels (MFI), and patterns (CVIF) were studied in leukemic blasts from diagnostic, MRD, refractory and relapsed samples. The details are given in table 1 and shown in figure 2A. Using the conventional cut-off of ≥20% of total blasts, CD38 was found positive in 97.9% (184/188) of diagnostic, 88.7% (110/124) MRD (including refractory) samples and 82.9% (29/35) relapsed samples. The cumulative frequency of CD38-PBP in all diagnostic, ETPALL and non-ETPALL, MRD, refractory and relapsed samples has been demonstrated in figure 2B. Median (range) of CD38-PBP in diagnostic, MRD, refractory, and relapsed samples were 85.9% (0.2%–100%), 74.0% (0.4%–100%), 79.6% (8.3%–100%), and 85.2% (0.6%–100%), respectively (table 1). We further evaluated the differences in the CD38-PBP between various groups of samples. We did not find a significant difference in CD38-PBP between pediatric versus adults (p value=0.18), male versus female (p value=0.97), and ETPALL versus non-ETPALL (p value=0.34) diagnostic samples (figure 2C–i, ii).
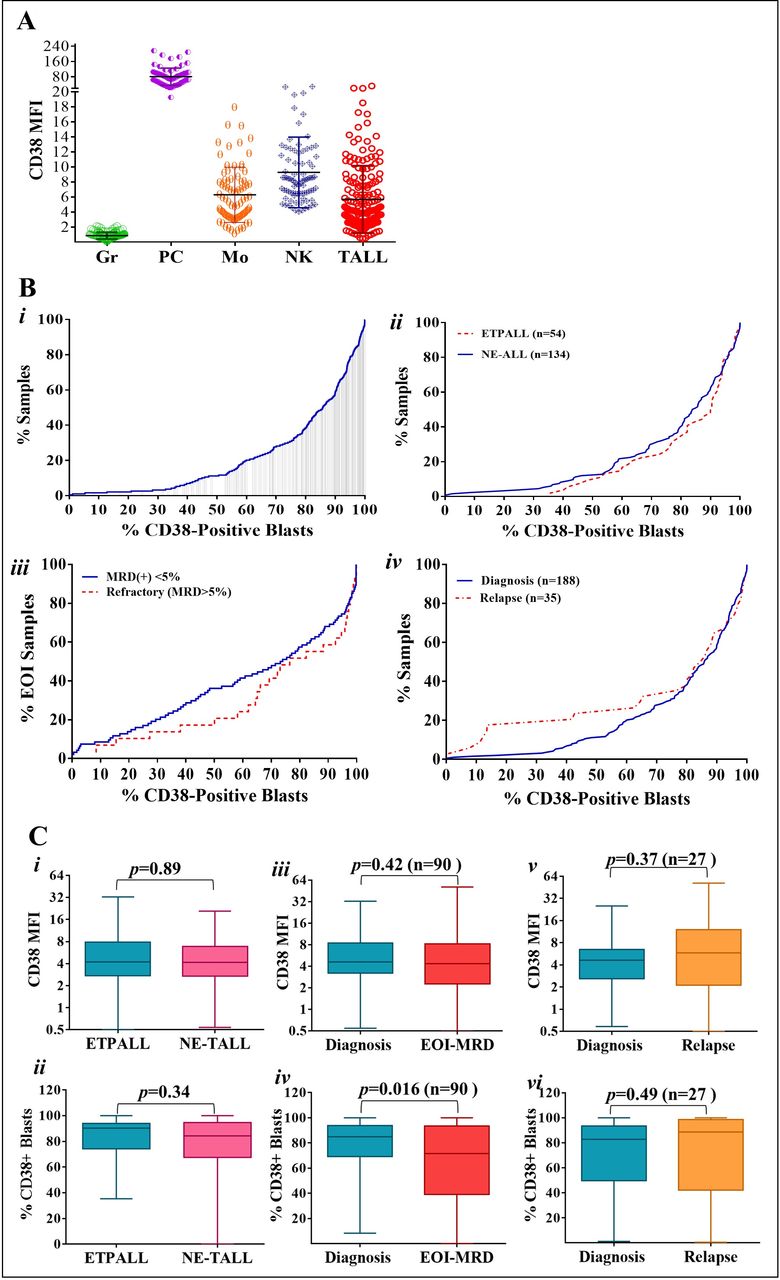
(A) CD38 expression levels using CD38-MFI in mature Gr, PC, Mo, NK cells and T-ALL leukemic blasts from diagnostic samples (n=188). The central black line indicates mean MFI value for each group. (B) The cumulative frequency (CF) of CD38-PBPs in samples from different groups of patients with T-ALL: (i) diagnostic samples (n=188), (ii) ETPALL (red dotted line; n=54) and patients with non-ETPALL (blue solid line, n=134) (iii) end-of-inductionmeasurable residual disease (EOI-MRD <5%) samples (blue solid line, n=188)and refractory samples (EOI-MRD >5%) (red dotted line, n=35) and (iv) diagnostic samples (blue solidline, n=188) and relapse samples (red dotted line, n=35) and end-of-inductionmeasurable residual disease (EOI-MRD <5%) samples (blue solid line, n=188)and refractory samples (EOI-MRD >5%) (red dotted line, n=35). (C) (i and ii) The BW plot have demonstrated no difference in CD38 expression levels (CD38-MFI) and CD38-PBPs in leukemic blasts between diagnostic samples from patients with ETPALL (n=54) and non-ETPALL (n=134, Mann-Whitney U test, p=0.89 and p=0.34, respectively). (iii) The BW plot has demonstrated the stable CD38-expression levels (CD38-MFI, p=0.42) but (iv) reduced CD38-PBPs in leukemic blasts following induction therapy (EOI) in MRD samples from 90 paired samples (p=0.016). However, it is notable that the median CD38-PBP was still higher than 60% samples in most of the samples. (v and vi) The BW plots have demonstrated the negligible effect of cytotoxic chemotherapy on CD38-MFI and CD38-PBPs in leukemic blasts from patients with relapsed T-ALL in 27 paired samples. BW plot, box and whisker plots; EOI, end of induction; ETPALL, early thymic precursor subtype of T-ALL; Gr, granulocytes; MFI, mean fluorescence intensity; Mo, monocytes; MRD, measurable residual disease; NE, non-ETPALL; NK cells, natural killer cells; PBPs, positive blasts percentages; PCs, plasma cells; T-ALL, T-cell acute lymphoblastic leukemia.
CD38 expression levels (determined as MFI) of mature granulocytes (negative reference control), monocytes, NK cells and plasma cells (positive reference control), varied between 0.02 and 2.15 (median 0.86), 1.2–18 (median 5.41), 1.8 to 16 (median 5.2), and 19.26–216.3 (median 73.7), respectively (figure 2A). The median (range) of CD38-MFI of blasts in diagnostic (n=188), MRD (n=100), refractory (n=24), and relapsed (n=35) T-ALL samples were 4.2 (0.46–32.4), 4.6 (0.4%–50.7%), 4.6 (0.63–26.6), and 5.6 (0.2–51.4), respectively (table 1). Based on the nMFI score (online supplementary figure S2), we categorized the level of CD38 expression as negative (2.7%), dim-to-negative (8%), dim (56%), moderate (27.7%) and bright (5.7%) expressions. Further, we have determined the variability in CD38 expression pattern in T-ALL blasts as CVIF. The median (95% CI) CVIF of CD38 in diagnosis, MRD, refractory and relapse samples was, respectively, 62.8 (59.32–65.55), 66.4 (62.28–72.38), 65.0 (50.22–90.73), and 61.8 (58.43–68.02, table 2A, B and figure 3). This data indicated that the CD38 expression pattern was homogenous in a majority of samples. However, some degree of heterogeneous expression was also observed in MRD and refractory samples compared with the diagnostic and relapsed samples.
CD38 PBPs, expression levels (MFI) and pattern (CVIF) in T-ALL at diagnosis, MRD and relapse samples
nMFI-based CD38 expression levels in diagnostic, MRD, refractory and relapsed samples

The box and whisker plot demonstrated a pattern of CD38 expression (heterogeneous or homogenous) using a CVIF in leukemic blasts. CVIF, coefficient of immunofluorescence; Diag, diagnostic samples; MRD, measurable residual disease; Rf, refractory disease; RLP, relapsed disease.
Effect of chemotherapy
The effect of chemotherapy on CD38 expression was studied by evaluating the difference between CD38-MFI and CD38-PBP in diagnostic versus EOI-MRD paired samples (n=90 including 24 refractory samples) and diagnostic versus relapsed paired samples (n=27, figure 1C, iii–vi). Our data did not demonstrate any significant changes in the CD38-MFI between diagnostic versus MRD paired samples (n=90; p value=0.42) and diagnostic versus relapsed paired samples (n=27; p value=0.37). The kinetics of CD38 expression from diagnostic samples to subsequent follow-up time points after initiation of therapy is shown in figure 4A. For considering CD38 as a therapeutic target, not only the expression level but CD38-negative blast percentage is also vital information. Hence, we also studied the post-therapy kinetics of CD38-PBP in leukemic blasts. There was no significant difference between CD38-PBP in diagnostic versus relapsed paired samples (p value=0.69), however, MRD samples showed a significant reduction in CD38-PBP compared with the diagnostic samples (median, 84.8% vs 71.6%; p value=0.016). Notably, although CD38-PBPs were reduced in MRD samples, 88.7% of samples had >20% CD38 positive blasts (95% CI, 59.5% to 82.2%). We have demonstrated the variation in CD38-PBP at different time points during the course of disease, that is at diagnosis, EOI-MRD, EOC-MRD, subsequent follow-up MRD and relapse in figure 4B. The results indicated that with some degree of variation, CD38-PBPs were maintained above 20% of blasts throughout the course of disease in the majority of patients.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) The figure demonstrated the postchemotherapy variation in the CD38-PBPs and (B) CD38-MFI at different time points in paired T-ALL samples. D, diagnostic samples; MFI, mean fluorescence intensity; MRD, measurable residual disease; PBPs, positive blast percentages; PR, post relapse; RLP, relapsed disease; T-ALL, T-cell acute lymphoblastic leukemia.
Discussion
The success story of daratumumab in multiple myeloma (MM) has attracted major interest in its potential utility for the treatment of other hematological neoplasms expressing CD38 antigen on tumor cells including T-ALL.7 15 35–38 Several studies have shown that the levels of target antigen can affect the antitumor efficacy of Mab therapy including daratumumab therapy.19–21 23 Since daratumumab is being considered as a potential therapeutic option for T-ALL, the data on the levels and patterns of CD38 expression in T-ALL leukemic blasts and its subtypes like ETPALL are urgently required. However, studies reporting the expression levels of CD38 in T-ALL at diagnosis and kinetics of its expression during the course of chemotherapy and at relapse are sparse and limited to a very small number of patients.8 17 18 Moreover, there is no report highlighting CD38 expression pattern in adult patients. We studied the expression of CD38 in a large cohort of T-ALL that included pediatric (85 children<15 years of age) as well as adult (111 adolescents and adults) patients. The study was performed in T-ALL leukemic samples at diagnosis, refractory disease, MRD assessment, and relapse. CD38 expression was evaluated for the percentages of leukemic cells positive for CD38, levels of CD38 expression (antigen density) with MFI and pattern of its expression (homogenous or heterogeneous) with CVIF.
The level of CD38 expression (MFI) on T-ALL blasts was not as strong as plasma cells but was of intermediate-level, that is closer to that of monocytes and NK cells (figure 2A). The CD38 expression in T-ALL was found predominantly between dim to intermediate levels. No difference was noted between the levels of CD38 expression between pediatric and adult patients as well as ETPALL and non-ETPALL. These findings are closely comparable to the recently published findings by Bride et al in a series of 21 pediatric patients.17 Using the conventional cut-off of 20% positive expression, CD38 was positive in almost all (>97%) of patients with T-ALL with median CD38-PBP of 85.9%. There was no significant difference between CD38-PBP in samples from pediatric versus adult, male versus female and patients with ETPALL versus non-ETPALL. These findings were similar to those reported by Bras et al and Naik et al in the recently published series of 8 and 12 cases of T-lymphoblastic lymphoma, respectively.14 16 Thus, we confirmed that CD38 was positive in the majority of leukemic blasts from newly diagnosed patients with T-ALL in a large cohort. Furthermore, our data demonstrated that the expression pattern of CD38 was prominently homogeneous with CVIF ranging between 61.8 and 66.4.
Anti-CD38 Mab therapy has been shown effective in combination with chemotherapy in newly diagnosed as well as in refractory or relapsed MM.10–12 39 Hence, we also evaluated the effect of cytotoxic chemotherapy (MCP841 in children and BFM90 in adults) on CD38 expression in residual tumor cells in refractory and MRD samples. The levels of CD38 expression (CD38-MFI), as well as the pattern of CD38 (CVIF), did not show any significant shift between paired diagnostic and EOI samples. These findings are in line with recently published data by Bride et al and Naik et al.16 17 Naik et al also demonstrated similar findings in acute myeloid leukemia (AML) samples.16 These findings highlighted the post cytotoxic chemotherapy stability in the expression levels of CD38 in the leukemic blasts of T-ALL. However, in our data, we also noted a mild reduction in the CD38-PBP in MRD samples (p=0.016) indicating induction therapy might have some effect on CD38-PBP, and a potential mechanism of daratumumab resistance in these patients. Nevertheless, the CD38-PBP was still sufficiently high (median 74%) in most of the MRD samples (>20% of blasts in 88.7% of MRD samples). To the best of our knowledge, this finding has not been reported in any of the earlier published studies. Although the percentage of CD38 positive blasts demonstrated a mild drop, we did not observe significant downregulation in the CD38 expression levels (CD38-MFI) in leukemic blasts from diagnostic to postinduction MRD samples. Similar findings were noted in refractory samples too. These findings highlighted the stability in the expression of CD38 in leukemic blasts even after the initiation of chemotherapy. Our data also included 35 samples from patients with relapsed T-ALL. Out of 35 patients, diagnostic and relapsed paired samples were available in 29 patients. We did not find any significant difference in the CD38-PBP, MFI and CVIF levels between the diagnostic and relapsed paired samples indicating consistent expression of CD38 in T-ALL blasts.
To summarize, we have demonstrated the details of CD38 positive percentages, levels, and patterns in leukemic blasts from a large cohort of patients with T-ALL. To the best of our knowledge, this is the first report on CD38 expression in adult patients. Our data showed that CD38 is uniformly expressed in the leukemic blasts of T-ALL across all groups of samples including ETPALL. We have also shown that cytotoxic chemotherapy has little effect on the expression of CD38 as demonstrated at various time points during the course of therapy. Thus, we conclude that the CD38 expression in leukemic blasts of T-ALL is robust and stable, making it a potentially effective target for anti-CD38-Mab therapy in patients with high-risk T-ALL.
References
Footnotes
Contributors PRT designed and performed the study, performed the data analysis, interpreted the data, statistical analysis and wrote the paper. PGS, HS, GC, NCP, SG, and DP performed the study and interpreted the data. TK, SG, YB, and ND performed the quality control of study and processed the samples. HS and TK performed the study and collected the data; GN, SB, NK, MS, BB, and HJ recruited patients, and performed clinical analyses. All authors contributed to the manuscript writing and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests No, there are no competing interests.
Patient consent for publication Not required.
Ethics approval This study has been approved by the Institutional Ethical Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. Most of the data are given in the manuscript and supplementary files. Raw data files are available with the corresponding author and will be shared on request.