Article Text

Abstract
The pandemic caused by the novel coronavirus SARS-CoV-2 has placed an unprecedented burden on healthcare systems around the world. In patients who experience severe disease, acute respiratory distress is often accompanied by a pathological immune reaction, sometimes referred to as ‘cytokine storm’. One hallmark feature of the profound inflammatory state seen in patients with COVID-19 who succumb to pneumonia and hypoxia is marked elevation of serum cytokines, especially interferon gamma, tumor necrosis factor alpha, interleukin 17 (IL-17), interleukin 8 (IL-8) and interleukin 6 (IL-6). Initial experience from the outbreaks in Italy, China and the USA has anecdotally demonstrated improved outcomes for critically ill patients with COVID-19 with the administration of cytokine-modulatory therapies, especially anti-IL-6 agents. Although ongoing trials are investigating anti-IL-6 therapies, access to these therapies is a concern, especially as the numbers of cases worldwide continue to climb. An immunology-informed approach may help identify alternative agents to modulate the pathological inflammation seen in patients with COVID-19. Drawing on extensive experience administering these and other immune-modulating therapies, the Society for Immunotherapy of Cancer offers this perspective on potential alternatives to anti-IL-6 that may also warrant consideration for management of the systemic inflammatory response and pulmonary compromise that can be seen in patients with severe COVID-19.
- immunomodulation
- inflammation mediators
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Coronaviruses are a family of enveloped, positive sense, single-strand RNA viruses that infect mammals and birds. In humans, coronavirus infections typically cause mild respiratory disease, including seasonal colds, yet some members of the family can be highly virulent. In December 2019, a novel coronavirus, SARS-CoV-2, structurally related to the virus that causes severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), was identified in Wuhan, China. Its efficient transmission (R0 of 2.2) facilitated its spread across the globe, with the first detected case in the USA reported on January 19, 2020.1 On March 11, 2020, WHO declared the outbreak a pandemic.2
The ongoing COVID-19 outbreak is challenging every aspect of daily life, including the implementation of public health policy, the nature of social interactions, adaptation of the workforce to a ‘new normal’ and the medical research and clinical care infrastructure, including the care for oncology patients. Economic forecasts are concerning, and a global financial crisis is anticipated. Mathematical modeling based on available data shows that in the face of rapid geographical spread and a high case-fatality ratio, even the most advanced healthcare systems are very likely to be overwhelmed in the coming weeks and months.3 It will be critical to identify therapies with low barriers to rapid clinical deployment.
It is becoming apparent that in some patients, severe COVID-19 disease occurs, and is accompanied by a fulminant and damaging immune reaction, sometimes called the ‘cytokine storm’, characterized by pronounced infiltration of macrophages and monocytes into the alveolae, a pro-inflammatory T-helper 17 (Th17) response, and elevated levels of inflammatory cytokines, particularly IL-6, IL-1β, IL-8, interferon gamma (IFNγ) and tumor necrosis factor alpha (TNFα).4–7 This pro-inflammatory cytokine profile has been with poor prognosis and severe lung pathology characterized by interstitial mononuclear inflammatory infiltrates, diffuse alveolar damage, hyaline membrane formation and pulmonary edema.8–10
As the oncology community rallies behind our colleagues in intensive care, internal medicine, emergency medicine and infectious disease, the immunotherapy field is poised to offer insights into the application of immune-modulatory therapies. Modulation of IL-6, in particular, which has emerged as a potentially promising option for COVID-19-related acute respiratory distress syndrome (ARDS), is used for the treatment of some rheumatological disorders,11 and has become a mainstay in recent years in the management of cytokine release syndrome (CRS) after chimeric antigen receptor (CAR) T cell therapy for hematological malignancies.12–14 Although the cytokine levels observed in patients with COVID-19 experiencing ARDS are much lower than those seen in CRS after delivery of CAR Tcell therapies and CD3-based bispecific Tcell engagers, the cancer immunotherapy community’s experience in using the IL-6 receptor antagonists to modulate severe inflammatory pathology in the setting of CRS may prove to be useful in identifying therapies that could be of use in this setting.
Healthcare and research organizations continue to aggressively pursue development of a vaccines and effective therapeutic strategies to attenuate the burden of SAR-CoV-2 (including antimalarial, antimicrobial and directed antiviral agents as well as convalescent serum from patients who have cleared virus and recovered) and to support patients through the severe inflammatory response and pulmonary complications that can frequently occur. The aim of this analysis is to describe available strategies that could alleviate the burden on the healthcare system with a specific emphasis on therapeutics that could block or modulate the systemic inflammatory response and pulmonary complications caused by COVID-19, in particular, IL-6, IL-1 and TNFα pathways.15
Rationale for targeting IL-6
SARS-CoV-2 causes the emergent respiratory disease called COVID-19. One of the challenging aspects in management of the infection is that different presentations have been identified16:
Asymptomatic carrier state
Mild respiratory symptoms, not requiring hospitalization
Recovered and re-examined positive for SARS-CoV-2 nucleic acid after discharge
Acute respiratory disease: respiratory presentation (fever, cough, dyspnea), without radiological evidence of a parenchymal process. Additional symptoms may include myalgias, headache, sore throat, anosmia, chills, diarrhea, nausea and vomiting.
Severe respiratory disease: pneumonia, often bilateral, which can progress in severity ultimately requiring mechanical ventilation and intensive care management. While ARDS is the common feature in patients with severe disease, other manifestations have been described, such as acute cardiac injury, acute kidney injury, coagulopathy and shock.17
Lethal infection: the case-fatality rate has been reported from 0.1% to 2%, although complete epidemiological analysis is ongoing worldwide and facing the challenge of testing availability. Death is typically due to massive alveolar damage and irreversible respiratory failure.18
Almost 75% of patients with COVID-19 acute respiratory disease present with abnormal findings on chest CT scans. Ground-glass opacities are the most common finding, reported in as many as 60% of patients. Other findings include patchy infiltrates, and interstitial lung disease, although some patients present with minimal imaging abnormalities.5 7 17 19
Pathological findings resemble those seen in SARS and MERS: edema, proteinaceous exudates, focal reactive pneumocyte type II hyperplasia, patchy cellular inflammation and multinucleated giant cells.9 Notably, neutrophil infiltration is not significant.20
Elevated C reactive protein (CRP) and elevated aspartate transaminase are common in patients with COVID-19 and reports from Hubei province in China indicate that severe cases are associated with elevated levels of inflammatory markers including serum d-dimer, ferritin and lactate dehydrogenase.21 The cytokine profile of severe COVID-19 disease is characterized by elevated IL-2, IL-6, IL-7, IL-8, granulocyte-colony stimulating factor, IL-17, TNFα and other markers that indicate systemic inflammatory response,22 similar to what has been described in macrophage activation syndrome (MAS) or in hemophagocytic lymphohistiocytosis (HLH).23 24 Moreover, a retrospective multicenter study of 150 patients performed from Wuhan, China suggested that among other clinical parameters, CRP and IL-6 levels can be predictors of mortality. Among 68 patients who died, median IL-6 level was 11.4 ng/mL as opposed to 6.8 ng/mL in those 82 who survived (p<0.001).25 Additionally, an elevated neutrophil-to-leukocyte ratio was also predictive of poor prognosis.
In the USA, anticipated shortages of key resources including intensive care unit (ICU) beds and mechanical ventilators has led to the implementation of social distancing measures to avoid overloading a medical system that is not prepared to care for an overwhelming number of affected individuals.26 While a concerted effort to increase and coordinate the supply of personal protective equipment for healthcare workers as well as mechanical ventilators for patient care is clearly needed,27 a complementary approach to decrease the number of patients with severe disease, and/or decrease the time required in the ICU on a ventilator is important as well.
Based on emerging information as centers gain more experience treating SARS-CoV-2-infected patients, modulating or inhibiting the IL-6 signaling pathway to mitigate the inflammatory response related to COVID-19 is an attractive idea.15 There is a successful precedent for this strategy, as it is almost routinely considered in patients receiving T cell engaging therapies, such as CAR T cells or blinatumomab. In these contexts, IL-6 levels peak at the time of maximal T cell proliferation and patients may develop a CRS that can be quite severe and even life-threatening.14 Administration of IL-6 blocking agents such as tocilizumab and siltuximab has been shown to be effective in reversing CRS in these patients.28–30 Tocilizumab was approved by the Food and Drug Administration (FDA) for the treatment of CRS secondary to CAR T cell therapy in 2017,13 and incorporated into the risk evaluation and mitigation strategies for the approved CAR T cell therapy products, tisagenlecleucel and axicabtagene ciloleucel.
A word of caution should be exercised in extrapolating the adoptive cell transfer experience using IL-6 inhibition to COVID-19, as formal comparative analysis of the levels of pro-inflammatory cytokines in both situations has not yet been performed. Initial data from the COVID-19 pandemic indicate that cytokine levels are far lower in the context of SARS-CoV-2 infection than seen in CRS.25 31
A 21-patient observational study recently performed in China supports the use of tocilizumab to avoid rapid clinical deterioration of individuals with severe pneumonitis and pulmonary complications.32 Anecdotal cases reported in Italy33 also point that tocilizumab may be clinically active in decreasing the magnitude of the inflammatory response associated with COVID-19, with rapid improvements observed in critically ill patients, even those requiring mechanical ventilation. On March 19, 2020, the Italian Medicines Agency announced the launch of TOCIVID-19, an independent phase II study to evaluate the efficacy and safety of tocilizumab in the treatment of pneumonia during COVID-19. Accrual of 330 patients was reached within 24 hours. In the USA, a randomized, double-blind, placebo-controlled phase III clinical trial has recently been approved by the US FDA to evaluate the efficacy of tocilizumab plus standard of care in hospitalized adult patients with severe COVID-19 pneumonia (NCT04320615). A randomized, placebo-controlled phase II/III study evaluating the efficacy of low-dose and high-dose sarilumab, another IL-6-modulating therapy in hospitalized patients with COVID-19 against placebo is also ongoing (NCT04315298).
Multiple doses of tocilizumab may be necessary for maximal benefit. In the Chinese study protocol, patients received 400 mg once through an intravenous drip up to a maximum of 800 mg with an optimal dose of 8 mg/kg body weight. In cases of fever within 12 hours after the first administration, an additional dose of up to the same amount as the first would be given, with two doses as the cumulative upper limit. The protocol for the Italian trial, calls for doses comparable to those commonly used for the management of CRS, namely, 8 mg/kg (up to a maximum of 800 mg per dose), with a second administration of the same dose given after 12 hours if respiratory function has not recovered, at discretion of the investigator. In preliminary reports from Italy, meaningful effects have also been observed with the subcutaneous formulation of tocilizumab.
A key lesson learned from the experience of treating about 500 severe or critical patients in China is the necessity of starting tocilizumab therapy as soon as possible, ideally before symptoms start to rapidly deteriorate at the onset of the cytokine storm. It is critical to observe high-risk cases, patients with persistent fever, diffuse lung opacities on CT scans and elevated serum CRP and IL-6 (if cytokine measurements are available). Because the condition can quickly change from mild to severe, early intervention should be strongly considered.
While establishing new indications for an agent generally requires evaluation in a rigorous, often randomized clinical trial, the massive impact of this pandemic, and the lack of any existing standard-of-care might provide appropriate context to consider off-label use of IL-6 inhibition for severely ill patients affected by COVID-19. China’s National Health Commission has recently issued updated treatment guidelines that include the use of tocilizumab in patients with severe disease.34
The FDA is closely monitoring the medical product supply chain,35 and the demand for drugs used to treat patients with COVID-19 including but not limited to tocilizumab, could surpass the ability to manufacture these agents. Additionally, in some cases, access to tocilizumab and sarilumab is limited despite adequate supply. For example, the study protocol for sarilumab in COVID-19-related ARDS initially excluded individuals who have recently been treated with any other investigational drugs, high-dose steroids or cyclophosphamide chemotherapy—effectively preventing numerous patients with cancer and patients receiving immunotherapy from receiving this potentially lifesaving intervention—however, amended exclusion criteria may relax these requirements. Ongoing and future clinical trials should consider the unique characteristics of oncology patients in their design (including inclusion and exclusion criteria), in light of the fact that the large, immune-suppressed population of patients with cancer may be particularly susceptible to severe complications of COVID-19.36 In addition, although data are not available, it is unknown whether pulmonary manifestations of COVID-19 may be potentiated or attenuated in oncology patients being treated with immunotherapeutic approaches that themselves can have significant pulmonary toxicity, including checkpoint inhibitors and CAR T cells.
Although tocilizumab and sarilumab are presently the most well-studied anti-IL-6 agents in the COVID-19 setting, numerous agents have been developed to modulate pro-inflammatory signaling at multiple levels in the pathway. An immunology-informed approach could identify potential alternatives to tocilizumab and sarilumab, broadening the population of patients that may receive treatment to ameliorate the complications of COVID-19, and thus ‘flattening the curve’ for total patient days requiring ICU support, including mechanical ventilation.
Overview of IL-6 signaling and regulation
IL-6 is a pleiotropic cytokine with nearly ubiquitous expression in stromal and immune cells. In the airway, alveolar macrophages produce IL-6, and expression may be induced in epithelial cells by IFNγ and danger-associated molecular patterns (DAMPs).37 38 The effects of IL-6 are context-specific and may be both pro-inflammatory and anti-inflammatory. Although IL-6 is essential for both innate and adaptive immunity—patients with auto-antibodies to the cytokine or germline mutations in its downstream signaling effectors are susceptible to recurrent infections and often die prematurely due to pneumonia. In turn, uncontrolled IL-6 expression leads to profound inflammatory damage to host cells.11 39 Under homeostatic conditions, serum concentrations of IL-6 are typically lower than picograms per mL, but under conditions of severe inflammation, levels may reach up to nanograms per mL, as seen in severe CRS31 or even micrograms per mL in fatal sepsis.40
Regulation of IL-6 expression
Expression of IL-6 is regulated at multiple levels including chromatin accessibility, transcription, mRNA export, post-transcription and translation. TNFα and IL-1β also induce IL-6 expression.41 Coronavirus’ spike proteins have also been shown to directly promote IL-6 production in immune and epithelial cells. Cultured SARS-CoV-infected bronchial epithelial cells secrete IL-6,42 and murine macrophages upregulate IL-6 and TNFα through a nuclear factor-κB-dependent pathway in response to viral S protein.43
IL-6 signaling (classical and trans)
Signaling through the IL-6 receptor requires assembly at the cell membrane of a complex consisting of IL-6 bound to both the 80 kDa type 1 cytokine a-receptor subunit (IL-6R, also called CD126) and a 130 kDa signal-transducing b-receptor glycoprotein (gp130; also called CD130). This trimeric complex homodimerizes, leading to receptor activation.11 44 Expression of the membrane-bound form of IL-6R is largely restricted to hepatocytes, megakaryocytes and leukocytes,45 yet two independent pathways generate a soluble form of the receptor: cleavage by membrane metalloproteinases, primarily ADAM10 and ADAM17, as well as alternative splicing.45–47 Soluble IL-6/IL-6R receptor complex can also bind gp130, activating the downstream signaling cascade. The ubiquitous expression of gp130, which has been detected in all human tissues examined, underlies the pleiotropic effects of IL-6, and the near universal responsiveness to the cytokine across cell types. Receptor activation through the membrane-bound IL-6R versus the soluble form of IL-6R are referred to as classical and trans signaling, respectively. Generally, classical signaling contributes to regenerative and anti-inflammatory responses, whereas trans signaling is pro-inflammatory and plays a role in causing tissue damage.
Signal transduction
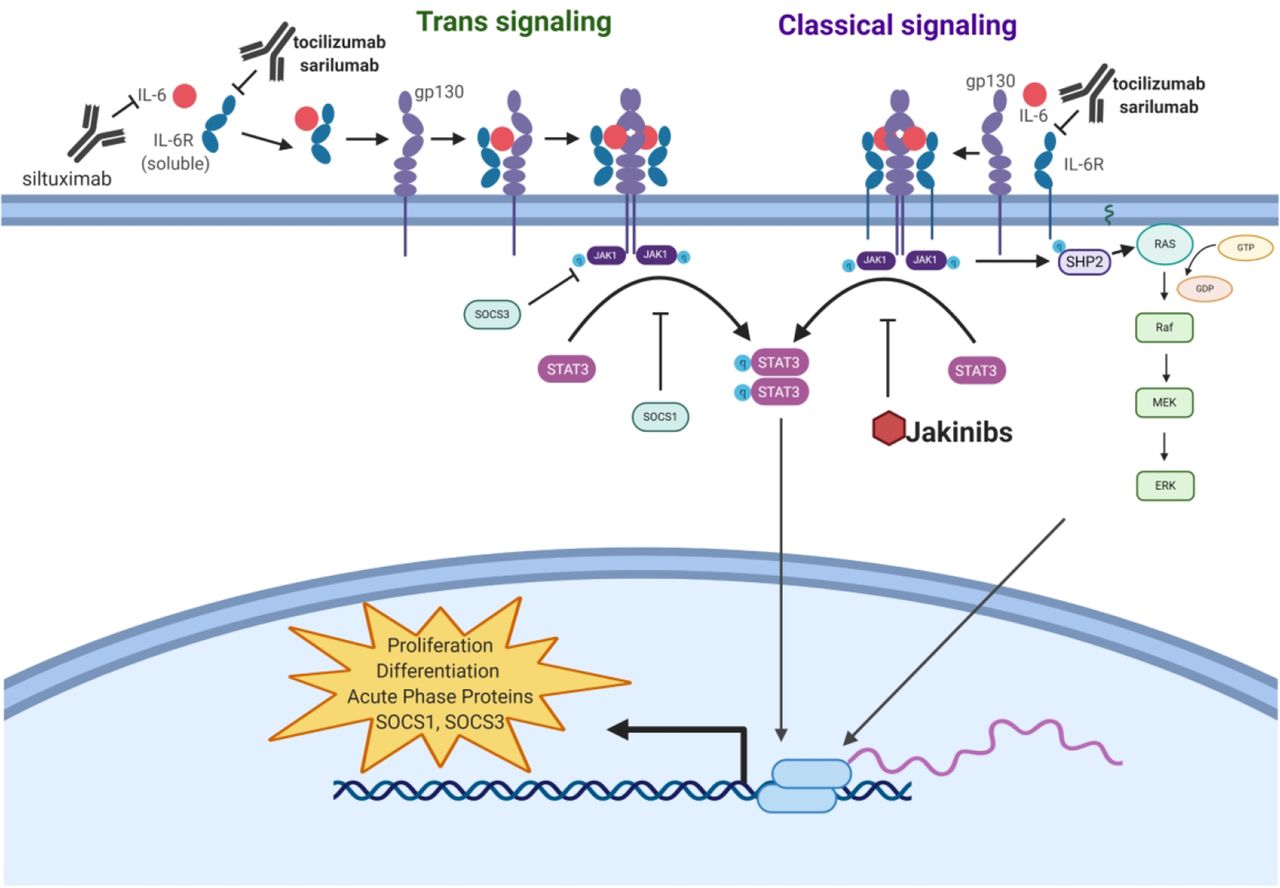
Ligand binding at the IL-6R activates multiple intracellular signaling cascades, including Janus kinase (JAK)/signal transducer and activation of transcription (STAT) pathways and the phosphatidylinositol 3-kinase (PI3K) pathway. Of potential importance in the context of COVID-19, the activation of JAK1 and STAT3 kinases by IL-6R initiates a pro-inflammatory transcriptional program associated with proliferation, differentiation, recruitment, survival and transformation in T and B cells and myeloid cells.11 44 45 An overview of IL-6 signal transduction with modes of action of approved IL-6-modulatory therapies is illustrated in figure 1.

{kind=link}
Interleukin 6 (IL-6) signaling cascade. Antibodies such as tocilizumab, sarilumab and siltuximab inhibit IL-6 signaling by antagonizing ligand-receptor engagement, whereas Jakinibs prevent the downstream signaling cascade. The intracellular domain of gp130 is constitutively associated with the Janus family tyrosine kinases JAK1 and JAK2. On homodimerization, JAKs autophosphorylate and JAK1 phosphorylates 5 tyrosine residues in the cytoplasmic tail of gp130, leading to the activation of multiple intracellular signaling cascades. Recruitment and phosphorylation of STAT3 initiates its homodimerization and nuclear trafficking, initiating a transcriptional program associated with proliferation, differentiation, recruitment, survival and transformation in T and B cells and myeloid cells. A negative feedback loop modulates activation of the IL-6-JAK/STAT cascade, as STAT3 upregulates SOCS1 and SOCS3, which directly inhibits the catalytic activity of JAK by binding to phosphorylated gp130 at tyrosine 759, and stops JAK activation through direct binding.11 Phosphorylated gp130 is also a binding site for SH2 domain tyrosine phosphatase 2 (SHP2), activating a cascade involving RAS, RAF and mitogen-activated protein kinases (MAPK), which culminates in the activation of various transcription factors involved in increasing cell growth, antibody synthesis and acute phase protein generation. JAK also phosphorylates phosphatidylinositol-4,5-bisphosphate (PIP2), which is then phosphorylated by phosphoinositide 3-kinase (PI3K) to become phosphatidylinositol-3,4,5-trisphosphate (PIP3), which then phosphorylates PkB/Akt serine/threonine kinase to modulate expression of several genes involved in cellular survival.12
Potential therapeutic strategies
IL-6 blocking agents have been developed in the recent years to treat rheumatological conditions. Tocilizumab was approved by the FDA in 2010 to treat moderately to severely active rheumatoid arthritis. While other indications followed, it was not until August 2017 that it received approval for the treatment of CAR T cell-induced CRS.
Many other agents have since been developed or are under investigation to modulate the circulating levels, receptor binding and/or biological effects of IL-6. The FDA-approved agents are listed in table 1, whereas therapies that are not yet approved, but are in later-stage clinical development are described in online supplementary table 1. Caution should be exercised in attempting to equate antireceptor and antiligand antibodies. The safety and efficacy of some of these agents that have not yet achieved regulatory approval has not been established. Furthermore, none of the agents has achieved regulatory approval for use in patients with COVID-19, although China has issued treatment guidelines recommending tocilizumab for severe SARS-CoV-2 pneumonia.
Supplemental material
Food and Drug Administration-approved agents: IL-6
As with all immune-modulatory agents, patients treated with anti-IL-6/IL-6R agents are at increased risk for infections, most commonly by opportunistic bacterial and fungal pathogens. Patients with latent tuberculosis are at risk of reactivation with IL-6 blockade. Other common side effects that may be concern in the COVID-19 setting include hypotension, decreased platelet counts, liver toxicity, risk of gastrointestinal (GI) perforation and difficulty breathing.
Interleukin-6 antagonists
Tocilizumab (Actemra®, Genentech) is an IL-6R antagonist antibody also known as atlizumab. It is indicated for the treatment of rheumatoid arthritis, giant cell arteritis, polyarticular juvenile idiopathic arthritis, systemic juvenile idiopathic arthritis and CAR-T cell-induced severe CRS.
Sarilumab (Kevzara®, Regeneron/Sanofi) is an IL-6R antagonist antibody indicated for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or intolerance to one or more disease-modifying antirheumatic drugs.
Siltuximab (Sylvant™, EUSA Pharma) is an anti-IL-6 antibody, distinct from tocilizumab and sarilumab, as it targets the soluble cytokine and not the receptor. It is indicated for the treatment of patients with Castleman’s disease. Of note, it was not studied in patients with HIV or human herpesvirus-8 (HHV-8) infections as preclinical studies showed lack of binding to virally produced IL-6. Therefore, it is only indicated in those patients who are HIV and HHV-8 negative.
Janus kinase/signal transducer and activation of transcription (JAK/STAT) inhibitors
While encouraging preliminary results have been observed with IL-6 blockade, potential constraints on the supply of IL-6/IL-6R-targeting antibodies may limit access to these drugs and the numbers of patients that can benefit. In order to expand the spectrum of patients who may access IL-6-modulatory therapies, alternative targets within the cytokine’s inflammatory signaling cascade could be considered.
IL-6 signaling takes place via two mechanisms: binding to a higher affinity membrane-bound receptor (classical) or soluble IL-6 receptor (trans).41 44 Both lead to activation of JAK/STAT signaling downstream through JAK1 and STAT3, on tyrosine phosphorylation on the gp130 receptor’s cytoplasmic tail. JAK/STAT signaling is also activated by other pro-inflammatory cytokines that are observed to be elevated in COVID-19, particularly IFNγ (although IFN signaling is primarily via STAT1). STATs also play important roles in non-canonical cell signaling pathways, including activity of non-tyrosine phosphorylated STATs, mediation of DNA methylation, regulation of cell adhesion and mitochondrial activity.48
Small molecules targeting this pathway have been successfully introduced into the clinic, and are a therapeutic option in a number of inflammatory processes,49 including graft versus host disease and HLH.50 51 In xenograft models, ruxolitinib was able to prevent CRS after CAR Tcell therapy.52 Importantly, a phase III trial is being initiated to assess ruxolitinib in combination with standard of care compared with standard of care alone in patients with severe COVID-19 pneumonia as a result of SARS-CoV-2 infection.53 Additionally, a phase II single-arm study of fedratinib is planned.
The rationale for developing these agents as an option to prevent or treat cytokine release in COVID-19 is compelling, especially given the relative ease of manufacturing small molecules at scale as compared with biologics. The safety profiles of JAK inhibitors are generally manageable and predictable including increased risk of viral infections, lower GI complications and anemia and leukopenia.54 55 Because IL-6 signaling primarily occurs through JAK1, the selectivity of JAK inhibitors should be considered before their use for COVID-19. Additionally, ‘Jakinibs’ are oral tyrosine kinase inhibitors,54 which may not be easily administered/absorbed in patients with very severe ongoing systemic inflammatory response.
Ruxolitinib (Jakavi/Jakafi®, Incyte) is an oral JAK inhibitor with selectivity for JAK1 and JAK2 indicated for treatment of intermedia-risk or high-risk myelofibrosis, polycythemia vera unresponsive or intolerant to hydroxyurea and steroid-refractory graft versus host disease in adult and pediatric patients aged 12 years and older.
Tofacitinib (Xeljanz®, Jakvinus, Pfizer) is an oral JAK inhibitor with selectivity for JAK1 and JAK3 indicated for the treatment of rheumatoid arthritis, psoriatic arthritis and ulcerative colitis. The occurrence of serious infections and lymphoid-associated malignancies have led to a current black box warning imposed by the FDA.
Baricitinib (Olumiant®, Eli-Lilly) is an oral JAK inhibitor with specificity for JAK1 and JAK2 indicated for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response to one or more TNF antagonist therapies. The occurrence of serious infections, lymphoma and thrombosis have led to a current black box warning imposed by the FDA.
Peficitinib (Smyraf®, Astellas) is an oral pan-JAK inhibitor with JAK1, JAK2, JAK3 and tyrosine kinase 2 activity approved only in Japan and indicated for the treatment of rheumatoid arthritis in patients who have inadequate response to conventional therapies.
Upadacitinib (Rinvoq™, AbbVie) is a second-generation oral JAK inhibitor with high specificity for JAK1 that is indicated for the treatment of adults with moderately to severely active rheumatoid arthritis who have had an inadequate response or intolerance to methotrexate. The occurrence of serious infections, lymphoma and thrombosis has led to a current black box warning imposed by the FDA.
Fedratanib (Inrebic®, Impact Biomedicines/Celgene) is an oral semi-selective JAK2 JAK inhibitor indicated for the treatment of adult patients with intermediate or high-risk primary or secondary (postpolycythemia vera or postessential thrombocythemia) myelofibrosis. The occurrence of serious and fatal encephalopathy, including Wernicke’s, has led to a black box warning imposed by the FDA.
Interleukin-1 inhibitors
Modulation of IL-1 signaling, especially through the IL-1β isoform, could also potentially attenuate the exuberant inflammatory response that accompanies lung pathology in COVID-19 upstream of IL-6. Although serum IL-1 has not necessarily correlated with severity of SARS-CoV-2 disease in published reports, its function as a master cytokine elicits large effects with small perturbations.56–58 IL-1 signaling orchestrates the acute phase of response to infections and has also been demonstrated to influence the differentiation of lymphocytes, particularly Th17 cells. Of the two isoforms, IL-1β is predominantly associated with pulmonary pathology in ARDS.59 60 Although data on the immunopathology underlying ARDS in COVID-19 are lacking, a pro-inflammatory Th17 signature has been observed in patients infected with SARS-CoV-261 as well as in patients with MERS-CoV.62 Additionally, IL-1 has been shown to be a key cytokine driving pro-inflammatory activity in bronchoalveolar lavage fluid of patients with acute lung injury.60
The IL-1 family of cytokines are major regulators of the acute phase response, functioning to control inflammatory reactions in response to PAMPs and DAMPs released from damaged or infected cells.57 63 Hundreds of genes are transcriptionally upregulated by IL-1 signaling, including IL-6. IL-1-modulating therapies have been FDA approved for a number of indications, primarily for auto-inflammatory diseases where the primary drivers of pathology are innate immune cells rather than the T cell and Bcell compartments.64 Three IL-1-modulating therapies have been approved by the FDA, and each agent inhibits signaling through a distinct mechanism, which may have important implications for their possible use in treating COVID-19.
Multiple mechanisms modulate IL-1 signaling, including the soluble IL-1 receptor antagonist (IL-1RA), which is secreted by immune cells, epithelial cells and adipocytes,65 and the decoy receptor IL-1RII, which exists in both membrane-bound and soluble forms and scavenges IL-1β with high affinity.66 These endogenous factors have formed the basis for several IL-1-targeting therapeutics, including anakinra (a receptor antagonist) and rilonacept (a receptor trap). Additionally, an anti-IL-1β antibody, canakinumab, has been FDA approved for a variety of auto-inflammatory diseases.
Anakinra is a recombinant form of IL-1RA that lacks glycosylation and is modified with the addition of a single methionine residue at the N-terminus. Although several randomized trials failed to demonstrate statistically significant 28-day survival benefits for IL-1R antagonist therapy for sepsis,67–69 a reanalysis showed profoundly improved outcomes among the subset of patients with disseminated intravascular coagulation and hepatobiliary dysfunction, hallmarks of secondary MAS.70 Anakinra has also proven effective and gained FDA approval for the treatment of a variety of autoinflammatory disorders including CAPS as well as rheumatoid arthritis.56 63 Anakinra is short-acting, with a plasma half-life of roughly 4–6 hours.71
Anecdotal evidence has emerged that anakinra effectively modulates late-onset, tocilizumab-refractory CRS with clinical features similar to HLH/MAS secondary to CAR T cell therapy.72 Initial experience from the Northern Italian SARS-CoV-2 outbreak, however, has indicated that anakinra monotherapy did not provide clinical benefit when administered to patients with severe ARDS.33 It is possible that multiple mechanisms need to be targeted, as cytokine profiles from patients with COVID-19 demonstrate marked elevation of multiple factors beyond IL-1, including IL-6, IL-17, TNFα and IFNγ. An ongoing clinical trial is evaluating anakinra in combination with the IFNγ inhibitor emapalumab for severe ARDS in COVID-19 (NCT04324021).
The overall safety profile of anti-IL-1 therapies is acceptable. As with any cytokine modulator, IL-1 blockade carries increased risk of bacterial infections, but after many years of clinical experience and tens of thousands of patients treated, it has become apparent that opportunistic infections are highly rare with anakinra treatment, even among people at high risk for tuberculosis reactivation. Of note, anti-IL-1 therapy is associated with a reduction in circulating neutrophil counts,58 which may be clinically significant given that a high NLR (Neutrophil to Leukocyte Ratio) is predictive of poor prognosis in COVID-19. Evidence for improved outcomes after using IL-1 modulating therapies for CRS is lacking and variable. The timing of IL-R1 antagonist administration may be critical, and limited benefit may be obtained with treatment of already-established ARDS. Targeting IL-1β directly, either by reducing its effective concentration via a receptor trap or monoclonal antibody may also be impactful.
Anakinra (Kinaret®, Sobi) is a modified, recombinant human IL-1R antagonist indicated for the treatment of adult rheumatoid arthritis and neonatal-onset multisymptom inflammatory disease.
Rilonacept (Arcalyst®, Regeneron) is a dimeric fusion protein consisting of the extracellular domains of IL-1R and IL-1RAcP, linked by the Fc portion of human anti-IL-1 IgG1 indicated for the treatment of adults and children 12 years of age and older with CAPS.
Canakinumab (Ilaris®, Novartis) is a human monoclonal anti-IL-1β antibody indicated for the treatment of periodic fever syndromes (including CAPS) and systematic juvenile idiopathic arthritis.
Tumor necrosis factor alpha inhibitors
Ligands and receptors of the tumor necrosis factor superfamily play central roles in regulation of the immune system and tissue homeostasis. Although TNF signaling is vital for antipathogen immune responses and is protective in a variety of viral infections including smallpox,73 West Nile virus74 and influenza,75 elevated levels of TNFα have been linked to pulmonary pathology in acute lung injury. Elevated TNFα is observed in both plasma and bronchoalveolar lavage fluid in patients with ARDS, and expression of the cytokine directly leads to increased endothelial permeability along with impaired alveolar fluid clearance due to downregulation of epithelial sodium channels.76 77 Elevated serum TNFα has been reported to correlate with severe disease in COVID-19,8 and the SARS-CoV S protein has been demonstrated to induce TNFα and IL-6 upregulation in murine macrophages.43
The primary sources of TNFα are stimulated monocytes, fibroblasts and endothelial cells, although macrophages, T cells, B lymphocytes, granulocytes, smooth muscle cells, eosinophils, chondrocytes, osteoblasts and mast cells all produce TNFα as well.77–79 TNFα is synthesized as a membrane-protein and cleaved by ADAM17 to release its soluble form. Both the soluble and membrane-bound forms of TNFα are active, although their affinities to TNF-family receptors varies. TNFα signaling is complex, and may involve as many as 29 different tumor necrosis factor receptor (TNFR) family members. In particular, TNFR1 is widely expressed; as is the case for IL-6 this broad-based expression gives rise to pleiotropic systemic effects.
Multiple TNFα inhibitors have been developed for the treatment of inflammatory diseases, and some have demonstrated benefit in animal models of acute lung injury and respiratory distress.80 These results have not borne out in humans, however, as anti-TNFα therapy failed to protect patients from sepsis-induced acute lung injury81 82 and did not improve outcomes for chronic obstructive pulmonary disease.83 Preliminary reports from China indicate that anti-TNFα antibody offers limited benefit for patients with SARS-CoV-2 infections with established ARDS,84 although modulating the pathway through other targets or at different timepoints may be more efficacious. In the oncology setting, the anti-TNFα antibody infliximab is commonly used for the management of immune-related adverse events secondary to immune checkpoint inhibitor therapy. Additionally, success has been reported with the use of the TNFα receptor trap etanercept for the treatment of CRS secondary to CAR T cell therapy85 and in MAS,86 but no prospective, large-scale trials have demonstrated efficacy for TNF modulation in the setting of viral cytokine storm. Adverse effects of concern for anti-TNFα therapy include dampened cell-mediated immune responses. All of the approved agents carry black box warning labels for increased risk of serious, life-threatening opportunistic bacterial and fungal infections and patients with latent tuberculosis should not receive these therapies.
Infliximab (Remicade®, Janssen) is a chimeric monoclonal anti-TNFα antibody indicated for the treatment of inflammatory bowel diseases in adults and children, rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis and plaque psoriasis.
Etanercept (Enbrel®, Amgen) is a receptor trap consisting of TNF-R2 fused to IgG1 Fc indicated for the treatment of rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis and plaque psoriasis.
Adalimumab (Humira®, AbbVie) is a human monoclonal anti-TNFα antibody indicated for the treatment of rheumatoid arthritis, ankylosing spondylitis, Crohn’s disease, psoriatic arthritis and plaque psoriasis.
Certulizumab pegol (Cimzia®, UCB) is a human monoclonal anti-TNFα antibody conjugated to a 40 kDa polyethylene glycol indicated for reducing signs and symptoms in Crohn’s disease and the treatment of rheumatoid arthritis, ankylosing spondylitis and psoriatic arthritis.
Golimumab (Simponi®, Janssen) is a human monoclonal anti-TNFα antibody indicated for the treatment of rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis and Crohn’s disease.
Interferon gamma
IFNγ is a pleiotropic cytokine that plays an essential role in multiple phases of immune and inflammatory responses. The IFN family of proteins encompasses three distinct classes, with variable direct antiviral and immune-modulatory activities.87 The IFNγ receptor is expressed on both malignant and non-malignant cell populations.88
On receptor binding, IFNγ initiates a signaling cascade through JAK1 and JAK2 activation, which leads to STAT1 homodimerization and nuclear translocation and transcriptional activation of a wide array of IFN-inducible genes through the GAS enhancer element.88 89 IFNγ has been implicated as an important downstream effector cytokine in the antitumor immune response, and in the immune response to various infectious pathogens, including viruses.90 Although protective in the context of antiviral host defense, IFNγ also has been implicated in the pathogenesis of ‘cytokine storm’ and in various autoimmune diseases.91 92 Anti-IFN therapy has been investigated in HLH, rheumatoid arthritis, multiple sclerosis, Crohn’s disease and psoriasis.91 93
Elevated serum IFNγ has been associated with severe acute respiratory distress in COVID-19.8 21 36 94 Additionally, IFNγ enhances IL-6 production in monocytes95 and an IFNγ-related cytokine storm syndrome was reported in some patients during the 2003 SARS coronavirus outbreak.96 Anti-IFN antibodies have been demonstrated to alleviate acute lung injury induced by severe H1N1 influenza infection in murine models,97 and a trial of the human monoclonal anti-IFNγ emapalumab in combination with the IL-1 receptor antagonist anakinra for COVID-19 is ongoing.98
Anti-interferon therapy is approved in the US for the treatment of primary HLH. In the pivotal trial for the approval of emapalumab for HLH, the most commonly reported adverse events included infections, hypertension, infusion reactions and fever.99
Emapalumab (Gamifant®, Sobi) a human monoclonal antibody that binds to soluble and receptor-bound forms of IFNγ and is approved for the treatment of primary HLH in patients with refractory, recurrent or progressive disease or intolerance to conventional therapy
Granulocyte macrophage-colony stimulating factor
Alveolar macrophages can play a central role in the inflammatory pathology of ARDS through the release of a wide array of bioactive factors that damage or induce cell death in the lung epithelium such as proteases, reactive oxygen species, eicosanoids, phospholipids and cytokines including IL-1, IL-6 and TNFα.77 100 One key cytokine that regulates macrophage number and function is granulocyte macrophage-colony stimulating factor (GM-CSF), a monomeric glycoprotein secreted by macrophages, T cells, mast cells, natural killer cells, endothelial cells and fibroblasts. GM-CSF is upstream of IL-6 and induces an inflammatory transcriptional program through JAK/STAT signaling.101 Inactivation of GM-CSF in CAR T cells dramatically lowers IL-6 and IL-8 secretion102 and therapeutic inhibition of GM-CSF reduces CAR T-cell-associated CRS in mouse models.103
Initial evidence from a study of 52 patients with COVID-19 reported from Wuhan, China, elevated levels of circulating GM-CSF were associated with worse clinical outcomes.18 22 Additionally, analysis of peripheral blood samples from 33 patients with COVID-19 with pneumonia found increased numbers of pathogenic Th1 cells (GM-CSF+ IFNγ+) and inflammatory monocytes (CD14+ CD16+ with high expression of IL-6) in patients admitted to the ICU as compared with non-critical patients.104 In early April 2020, several studies evaluating anti-GM-CSF antibodies for COVID-19 treatment were initiated in rapid succession, including trials of lenzilumab,105 TJM-2,106 gimsilumab107 and namilumab. One anti-GM-CSF antibody, lenzilumab, received emergency investigational new drug approval for compassionate use in patients with COVID-19. Although the safety profiles of anti-GM-CSF antibodies have been acceptable in phase I and phase II trials, it is important to note the potential for lung toxicities and pneumonia with these agents.101
Lenzilumab (Humanigen) is a human monoclonal anti-GM-CSF antibody approved for compassionate use in patients with COVID-19. A phase III trial for COVID-19 is ongoing. Lenzilumab was originally developed for the treatment of chronic myelomonocytic leukemia and has also been evaluated for inadequately controlled asthma and rheumatoid arthritis.
Namilumab (Izana Bioscience) is a human monoclonal anti-GM-CSF antibody that has been evaluated in phase II trials for plaque psoriasis and rheumatoid arthritis. It is being evaluated in a two center compassionate use study for COVID-19 by UK-based Izana Bioscience. In the rheumatoid arthritis study, a few patients experienced AEs indicative of pulmonary alveolar proteinosis, but following review all suggestive cases were given an alternative diagnosis.
Gimsilumab (Roivant) is a human monoclonal anti-GM-CSF antibody developed for rheumatoid arthritis. It has demonstrated favorable safety and tolerability with no serious adverse events reported in two phase I trials in healthy adult volunteers. Trials in patients with COVID-19 will be prioritized instead of a planned phase II study in patients with rheumatoid arthritis.
TJM-2 (I-Mab Biopharma) is a neutralizing antibody against GM-CSF that is being developed to treat cytokine storm in critically ill patients with COVID-19. It previously exhibited favorable safety, tolerability, pharmacokinetic/pharmacodynamic and immunogenicity profiles in a phase I dose-escalation study in the USA and received IND (Investigational New Drug) clearance from China’s National Medical Products Administration for a multiple-dose phase Ib study in patients with rheumatoid arthritis.
Otilimab (GSK) is a human GM-CSF inhibitory antibody that started phase III evaluation for rheumatoid arthritis in July 2019. During the phase II trials of otilimab, no serious adverse events and pulmonary toxicity, including pulmonary alveolar proteinosis, were observed.
Interleukin-17 and interleukin-23 inhibitors
IL-17 is a pro-inflammatory cytokine. It is produced by Th17 cells on stimulation with IL-23. The IL-17/IL-23 axis stimulates the secretion of cytokines know to mediate inflammation, including IL-6, and IL-6 (in the presence of TGF-β) skews naïve CD4 T cells toward the Th17 phenotype.108 IL-17/IL-23 signaling has been postulated to mediate cross-talk between the innate and the adaptive immune system.109 A characteristic Th17 signature has been noted in patients with COVID-19 ARDS,10 and modulation of IL-17 signaling through the JAK/STAT inhibitor fedratinib has been proposed, although this indication is currently speculative.61 Clinically, the use of agents that modulate this axis have been mostly used in the treatment of chronic conditions such as psoriasis109 and the most frequently observed adverse events have been nasopharyngitis, upper respiratory tract inflammation and injection site reactions.110 Although these agents have the potential to dampen IL-6 production and signaling, the use of IL-17/IL-23 modulators in conditions such as CRS has not yet been widely tested.
Secukinumab (Cosentyx®, Novartis) is a human IL-17A antagonist indicated for the treatment of moderate-to-severe plaque psoriasis, psoriatic arthritis and ankylosing spondylitis.
Ixekizumab (Taltz®, Eli-Lilly) is a humanized IL-17A antagonist indicated for the treatment of adults with moderate-to-severe plaque psoriasis.
Brodalumab (Siliq®, Valeant/LEO Pharma) is a human IL-17 receptor A antagonist indicated for the treatment of moderate-to-severe plaque psoriasis. The occurrence of suicidal ideation has led to a black box warning imposed by the FDA.
Ustekinumab (Stelara®, Janssen) is a human IL-12 and IL-23 antagonist indicated for the treatment of adult patients with moderate-to-severe plaque psoriasis, active psoriatic arthritis and moderately to severely active Crohn’s disease.
Guselkumab (Tremfya®, Janssen) is an IL-23 blocker indicated for the treatment of adult patients with moderate-to-severe plaque psoriasis.
Tidrakizumab-asmn (Ilumya™, Sun Pharma Global) is an IL-23 antagonist indicated for adults with moderate-to-severe plaque psoriasis.
Risankizumab-rzaa (Skyrizi™, AbbVie) is an IL-23 antagonist indicated for the treatment of plaque psoriasis
Conclusion
The COVID-19 pandemic caused by SARS-CoV-2 highlights an urgent need for all healthcare stakeholders including government organizations, academic centers, community centers, philanthropic organizations, advocates, pharmaceutical and biotechnology industries to develop a coordinated and flexible approach to increase the availability of resources.
Modulation/inhibition of the severe inflammatory state in patients with COVID-19, characterized by elaboration of various inflammatory mediators, including IL-6, is a potentially important strategy to treat and/or limit severe COVID-19 pulmonary complications, including ARDS. If successful across the broader population of patients with COVID-19, strategies such as anti-IL-6-directed therapy could reduce the needs for ICU support and mechanical ventilation, and ultimately decrease mortality.
Randomized phase III trials are currently evaluating the efficacy of anti-IL-6-directed agents, including tocilizumab and sarilumab, as well as the JAK/STAT inhibitor ruxolitinib, and will provide definitive data regarding the use of these agents in patients with COVID-19. As described here, other anti-IL-6 agents, including small molecule inhibitors of IL-6 signaling, and other anticytokine inhibitors may warrant investigation, particularly in the setting of overwhelming demand for agents to modulate the inflammatory state in patients with COVID-19. Ongoing studies are also investigating other strategies, such as the use of eculizumab (a monoclonal antibody that targets complement protein C5, approved for paroxysmal nocturnal hemoglobinuria), or some TLR7-8 inhibitors such as M5049. In all likelihood, a combinatorial approach encompassing antivirals such as remdesivir and potentially cytokine-modulatory therapies may be needed to successfully treat the infection with SARS-CoV-2 and the full spectrum of associated complications.
The US FDA has announced a new program, CTAP (Coronavirus Treatment Acceleration Program), to expedite drug development for COVID-19. While this is encouraging news and the appropriate way to proceed from a drug development perspective, the healthcare community and, more importantly, the affected patients, need effective treatments without delay, especially as the numbers of cases in the USA and several countries around the world continue to grow exponentially. Consideration also should be given to focus efforts on rapidly expanding the ability of clinicians and clinical investigators to access investigational anti-IL-6 agents, in particular for those agents where phase II and/or phase II studies have been completed, and acceptable safety has been demonstrated. Use of cytokine-modulatory agents during these extreme circumstances may additionally warrant consideration, and definitive prospective randomized trials also should be conducted with all due haste.
Acknowledgments
The authors would like to thank the SITC staff for their contributions including Sam Million-Weaver, PhD for medical writing and editorial support and Angela Kilbert for project management and assistance. The authors would also like to thank the society for supporting the manuscript development.
References
Footnotes
Twitter @Farnaldez3, @Vincenzo Montesarchio
Contributors JMW and BAF conceptualized the paper, served as authors on the paper, provided guidance in the development and reviewed and provided substantial comment on the content. FIA and SMW wrote the paper based on a review of the published literature and guidance from the other authors. FIA sourced the content of the supplemental table and SMW made the figure. PAA, CGD, BF, SJO'D, WJU and JSW provided substantial contributions to the content as well as reviewed and edited drafts. All authors read and approved the final version of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PAA: Consultant/Advisory Role: Bristol-Myers Squibb, Roche-Genentech, Merck Sharp & Dohme, Array, Novartis, Merck Serono, Pierre Fabre, Incyte, NewLink Genetics, Genmab, Medimmune, AstraZeneca, Syndax, SunPharma, Sanofi, Idera, Ultimovacs, Sandoz, Immunocore, 4SC, Alkermes, Italfarmaco, Nektar; Research Funds: Bristol-Myers Squibb, Roche-Genentech, Array; Travel support: MSD. FIA: Employee: Macrogenics, Inc. CGD: Consultant Fees: Agenus, AstraZeneca, Dendreon, Eli Lilly, Janssen, Merck, Pierre Fabre, Roche/Genetech; Ownership Interests: Compugen, Harpoon, Kleo; Patents/Royalties: AstraZeneca, Bristol-Myers Squibb, Janssen; Research Funding: Aduro Biotech, Bristol-Myers Squibb, Janssen. BAF: Co-Founder/Stock: UbiVac; Consulting/Research Support: Macrogenics, OncoSec, Shimadzu, Viralytics (Merck); Consulting (II-ON)/Research Support: Bristol-Myers Squibb; Consulting/Stock: PrimeVax; Research Support: NanoString, Quanterix; SAB: Argos, Bayer, CellDex, UltiVue; SAB/Institutional Research Support: AstraZeneca (MedImmunne); SAB/Research Support: Akoya BioScience (Perkin Elmer), Definiens. SJO: Advisory Board: Biothera, Bristol-Myers Squibb, BionTech, Exicure, Immunsys, Merck; Consultant: Agenus, Biothera, Immunsys; Grants/Research Support: Agenus, Amgen, Biothera, BMS, Exicure, Genocea, Incyte Merck, Ultimovacs, Viralytics; Speakers Bureau: Bristol-Myers Squibb. WJU: Advisory Board: MedImmune, Bristol-Myers Squibb; Research Support/Contracted Work: Bristol-Myers Squibb; Research Support: MedImmune. JMW: Consulting Fees: Western Oncolytics; Shareholder: MacroGenics, Inc. JSW: Consulting: Merck, Genentech, AstraZeneca, GSK, Novartis, Nektar, Medivation, Celldex, Incyte and EMD Serono; Advisory Board: Bristol-Myers Squibb, Celldex, CytoMx, Incyte, Biond, Protean, CV6 and Sellas; Equity: CytoMx, Biond and Altor; Patent/IP: Moffitt Cancer Center IPILIMUMAB biomarker, BioDesix PD-1 biomarker.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.