Article Text

Abstract
Purpose This randomized, double-blind, placebo-controlled, parallel-group, phase II trial assessed the efficacy and safety of adagloxad simolenin (OBI-822; a Globo H epitope covalently linked to keyhole limpet hemocyanin (KLH)) with adjuvant OBI-821 in metastatic breast cancer (MBC).
Methods At 40 sites in Taiwan, USA, Korea, India, and Hong Kong, patients with MBC of any molecular subtype and ≤2 prior progressive disease events with stable/responding disease after the last anticancer regimen were randomized (2:1) to adagloxad simolenin (AS/OBI-821) or placebo, subcutaneously for nine doses with low-dose cyclophosphamide. The primary endpoint was progression-free survival (PFS). Secondary endpoints included overall survival, correlation of clinical outcome with humoral immune response and Globo H expression, and safety.
Results Of 349 patients randomized, 348 received study drug. Patients with the following breast cancer subtypes were included: hormone receptor-positive (HR+)/human epidermal growth factor receptor 2-negative (HER2–) (70.4%), triple negative (12.9%), and HER2+ (16.7%), similarly distributed between treatment arms. Median PFS was 7.6 months (95% CI: 6.5–10.9) with AS/OBI-821 (n=224) and 9.2 months (95% CI: 7.3–11.3) with placebo (n=124) (HR=0.96; 95% CI: 0.74–1.25; p=0.77), with no difference by breast cancer subtype. AS/OBI-821 recipients with anti-Globo H IgG titer ≥1:160 had significantly longer median PFS (11.1 months (95% CI: 9.3–17.6)) versus those with titers <1:160 (5.5 months (95% CI: 3.7–5.6); HR=0.52; p<0.0001) and placebo recipients (HR=0.71; p=0.03). Anti-KLH immune responses were similar at week 40 between AS/OBI-821 recipients with anti-Globo IgG titer ≥1:160 and those with anti-Globo IgG titer <1:160. The most common adverse events with AS/OBI-821 were grade 1 or 2 injection site reactions (56.7%; placebo, 8.9%) and fever (20.1%; placebo, 6.5%).
Conclusion AS/OBI-821 did not improve PFS in patients with previously treated MBC. However, humoral immune response to Globo H correlated with improved PFS in AS/OBI-821 recipients, leading the way to further marker-driven studies. Treatment was well tolerated.
NCT01516307.
- randomized trials
- oncology
- immunology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The 5-year survival rate for women with metastatic breast cancer (MBC) is 27% or less in the USA and Europe.1 2 Although MBC generally is incurable, systemic therapy can provide meaningful prolongation of survival.3 The choice of therapy is increasingly determined by biological markers predictive of response to targeted therapy.4 New molecularly targeted therapies that are well tolerated and prolong duration of response are of great importance.4
Active immunotherapy with cancer vaccines has gained considerable interest over the last two decades. Cancer vaccines harness the host immune response to tumor-associated antigens and exert antitumor effects. Several tumor-associated carbohydrate antigens (TACAs) are overexpressed in many epithelial tumors, with limited expression in normal tissues, making them promising targets for cancer immunotherapy.5–8 Central to a successful vaccine intervention is ensuring that the host mounts a robust immune response. TACAs have long been known to elicit T-cell-independent immune responses, which make them poorly immunogenic.9 10 Immunization against carbohydrate antigens conjugated to immunostimulatory molecules such as keyhole limpet hemocyanin (KLH) results in immunoglobulin M (IgM) and immunoglobulin G (IgG) humoral antibody responses.7 These antibodies are known to induce complement-dependent cytotoxicity (CDC), antibody-dependent cell-mediated cytotoxicity (ADCC), and antibody-dependent cellular phagocytosis.5 11
Globo H, a hexasaccharide (Fucα1–2Galβ1–3GalNAcβ1–3Galα1–4Galβ1–4Glc) originally isolated as a ceramide-linked glycolipid from the human breast cancer cell line MCF-7, is one of the most prevalent TACAs.12 13 Globo H is highly overexpressed in several cancers, including breast, ovarian, gastric, lung, prostate, pancreatic, endometrial, and liver.14
Globo H is an important regulator in the tumor microenvironment, promoting tumor progression through several mechanisms. Globo H ceramide present in the tumor microenvironment is taken up by tumor-infiltrating lymphocytes, leading to immunosuppression,15 and is incorporated into endothelial cells, promoting angiogenesis.16 17 These findings provide scientific rationale for targeting the Globo H antigen in cancer immunotherapy.
The specific expression of Globo H in tumor stem cells16 and its function as an immune checkpoint inhibitor16 make it an ideal target for immunotherapy. Adagloxad simolenin (OBI-822) is a Globo H epitope conjugated to the immunostimulatory carrier protein KLH (OBI-821). More specifically, OBI-822 is a glycoconjugate composed of a carbohydrate tumor antigen, Globo H, covalently linked to the carrier protein KLH, which ensures that robust T cell help elicited by the carrier protein is concentrated in the vicinity of T and B cells specific to the weak antigen to which the KLH is linked. This in turn facilitates T–B cell cooperation and results in a more vigorous immune response to the weak antigen, Globo H. When used with the potent saponin-based adjuvant QS-21, the Globo H-KLH vaccine was well tolerated in two phase I studies in patients with MBC or metastatic prostate cancer, with local skin reactions at the injected site as the predominant side effects.7 18 In these two trials, induction of significant Globo H-specific IgM and IgG antibodies against Globo H-expressing tumor cells was demonstrated and post-immunization sera from some patients exhibited complement-mediated lysis of MCF-7 cells.7 18 Clinically, among 27 patients with MBC, 15 patients enrolled without evidence of disease and 10 remain so with a median follow-up of 107.5 weeks. Of the 12 patients who began this trial with stable disease (SD), 5 still have SD and 7 had progression, with a median follow-up of 111 weeks.18 Five of 18 patients with metastatic prostate cancer had stable prostate-specific antigen slope profiles in the absence of any radiographic evidence of disease for more than 2 years.7
The primary objective of this randomized, placebo-controlled trial was to evaluate the effect of maintenance therapy with adagloxad simolenin (AS/OBI-821) on investigator-assessed progression-free survival (PFS) in women with previously treated MBC of any biologic subtype receiving low-dose cyclophosphamide. Secondary endpoints included overall survival (OS), safety, and correlation of clinical outcomes with humoral immune response and Globo H expression.
Materials and methods
This was an international, randomized, double-blind, placebo-controlled, phase II study performed at 40 sites in Taiwan (15), USA (12), Korea (10), India (2), and Hong Kong (1). All patients provided written informed consent. The trial was registered at clinicaltrials.gov.
Vaccine preparation
Globo H allyl glycoside is a hexasaccharide prepared according to the total synthesis route, previously developed by Professor SJ Danishefsky.19 The purity of Globo H allyl glycoside is ≥99%. OBI-821 is directly purified from the Quil-A, a saponin extract obtained from the tree bark of Quillaja saponaria, Molina. The purification steps involved three stages of chromatographic purification, developed by Optimer Pharmaceuticals (Jersey City, New Jersey, USA), from Quil-A to obtain the OBI-821 containing two major isomers and four other potential isomers as a mixture. Of these six isomers, four have been identified to be structurally identical to the currently marketed adjuvant, QS-21. The total purity of these six isomer mixtures is controlled at no less than 99%.
Patients
Eligible patients were women with MBC achieving SD, partial response (PR), or complete response (CR) after at least one anticancer therapy and with no more than two events of progressive disease after MBC diagnosis. Patients with estrogen receptor-positive (ER+) or progesterone receptor-positive (PR+) tumors were allowed to continue antihormonal therapy with study treatment; those completing chemotherapy and starting hormone therapy during maintenance therapy must have had SD for at least 4 weeks before study entry. Concurrent treatment with anti-human epidermal growth factor receptor 2 (HER2) therapies was prohibited. Patients had adequate organ function and an Eastern Cooperative Oncology Group (ECOG) performance status of less than or equal to 1. Exclusion criteria included more than two lines of prior anticancer therapy; chemotherapy within 4 weeks of randomization; autoimmune disease or disorder requiring treatment with systemic corticosteroids or immunosuppressive therapies; any other investigational drug; any evidence or history of central nervous system metastases; and bone-only metastases.
Randomization and study treatment
Eligible patients were randomly assigned to receive AS/OBI-821 or placebo (phosphate-buffered saline) in a 2:1 ratio via a centralized interactive web-based randomization system. Adagloxad simolenin (OBI-822) was used with OBI-821, a saponin-based adjuvant that contains the same major components as QS-21 used in the phase I trials.20
Patients were stratified according to disease status at randomization (CR or PR/SD) and hormone therapy use (yes or no), with a block size of three for each of the four combined stratification levels. Study subjects and investigators were blinded to treatment group assignment.
AS/OBI-821 (30 µg/100 µg) or placebo was administered by subcutaneous injection at weeks 1, 2, 3, 5, 9, 13, 17, 25, and 37 for a total of nine doses or until disease progression. All patients received cyclophosphamide 300 mg/m2 administered intravenously at weeks 1, 5, 9, 13, 17, 25, and 37, 3 days prior to each dose of study drug.
Study procedures
CT scan (or MRI) was performed within 3 weeks before randomization, then repeated every 8 weeks for up to 2 years or until disease progression (whichever came first), reviewed both locally and by an independent central radiology facility. Biochemical and hematologic laboratory tests were performed within 3 weeks before randomization, then repeated at weeks 3, 5, 9, 13, 17, and every 8 weeks thereafter for up to 2 years or until disease progression or early termination. Blood samples were collected for measurement of anti-Globo H IgG and IgM titers by ELISA at weeks 1, 3, 5, 9, 13, 17, 25, 33, 37, 41, and every 8 weeks thereafter for up to 2 years or until disease progression or early termination. Anti-KLH IgG titers were assessed by ELISA in blood samples obtained at week 40. Blood samples for cellular immune response were collected on the day of but prior to dosing, then at day 4, weeks 5, 13, and 41. Additional immune studies were performed to assess antisera binding ability with Globo H+ tumor cells and CDC/ADCC, and results will be published elsewhere.
Archival samples (n=244) for Globo H analysis were from the primary tumor (184/244, 75%) or from metastatic sites (60/244, 25%). Metastatic sites included lymph nodes, chest walls, lung, liver, ovary, bone, and others. Archival tumor tissue was tested for Globo H antigen by immunohistochemical (IHC) staining with anti-Globo H IgG, VK9 monoclonal antibody (provided by Memorial Sloan Kettering Cancer Center, New York, USA) as previously described.21 Globo H is a glycolipid molecule. In this study, the interval between sample collection and IHC assay ranged from 0 to 17.3 years, with median of 1.5 years. The Globo H scores of the ≤10-year-old samples were comparable with the scores of the >10-year-old samples (p=0.23). We compared Globo H expression in 18 available pairs of primary tumors versus metastatic lesions from the same patients collected more than 1 year apart. The median duration of sample collection between primary and metastatic tumors was 2.7 years (range, 1.3–11.7 years). There was no obvious correlation of Globo H expression between primary and metastatic tumors obtained at an interval of more than 1 year. Among 14 patients whose paired tumors were collected at the same time (n=10) or at 1-month to 6-month intervals (n=4), there also was no correlation of Globo H expression between primary and metastatic tumors. In all paired samples obtained from 32 patients, there was no significant correlation of Globo H expression between primary and metastatic tumors. Thus, long-term storage of paraffin-embedded tissues of up to approximately 17 years did not appear to affect the detection of Globo H expression by IHC. Based on the percentage of tumor cells with positive staining, Globo H expression was defined as negative (<1%), 1+ (1%–30%), 2+ (31%–60%), or 3+ (>60%). Adverse events (AEs) were recorded and graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events V.4.03, with relationship to study medications recorded.
Outcomes
The primary endpoint was investigator-assessed PFS, which was defined as the time from randomization to investigator-assessed progression or death, whichever came first. Secondary endpoints included OS, defined as the interval from randomization until death from any cause; magnitude and correlation of the humoral immune response (IgM and IgG against Globo H) with PFS and OS; correlation of tumor Globo H expression with study outcome; and safety. Post hoc analyses included an analysis of PFS in patients who completed all nine injections of study drug; an analysis of anti-KLH IgG levels at week 40 (when all nine injections of study drug were scheduled to have been administered) in patients who did and did not have a humoral immune response to the investigational product (retrospectively defined as an anti-Globo H IgG titer ≥1:160 and <1:160, based on the correlation of anti-Globo H IgG response with PFS); and an analysis of potential clinical factors associated with anti-Globo H IgG response (retrospectively defined as an anti-Globo H IgG titer ≥1:160).
Immune studies
Flow cytometry
Breast cancer cell line MCF-7, which expresses Globo H, was used to determine the binding ability of serum from patients. Human serum (1/10 diluted) was incubated with MCF-7 cells (2×105/100 µL) for 30 min on ice. After washing with a flow cytometry staining (FACS) buffer, cells were incubated with fluorescin isothiocynate (FITC)-goat anti-human IgG (Cat No 2040-02, Southern Biotech, Birmingham, Alabama, USA) and PE-goat anti-human IgM (Cat No 2020-09, Southern Biotech) at 2 µg/mL each, for 30 min on ice. After washing, cells were resuspended in FACS buffer to determine the per cent of fluorescent cells by flow cytometry (EC800, Sony Biotechnology, Champaign, Illinois, USA). The data were analyzed using FlowJo (Tree Star, Ashland, Oregon, USA). The preimmune serum was used to define background binding (around 10%).
Complement-dependent cytotoxicity
MCF-7 target cells (2×106) were labeled with bis(acetotoxymethyl) 2,21:61,211-terpyridine-6,611-dicarboxylate (BATDA) (1 µL, PerkinElmer, San Jose, California, USA) at 37°C for 30 min. After washing three times with Dulbecco’s Modified Eagle’s Medium (DMEM), 1% fetal calf serum (FCS), BATDA-labeled cells were seeded into 96-well plate and incubated with 1:5 diluted human serum (50 µL) at 37°C for 30 min. Rabbit serum at 1:5 dilution in DMEM was used as a source of complement (50 µL). After incubation at 37°C for 2 hours, plates were centrifuged to collect supernatants. Europium solution was incubated with the supernatants containing TDA, and fluorescence of EuTDA was determined by Victor X3. Controls included target cells only, target cells with complement but no immune serum, and target cells with lysis buffer. The percentage of cytotoxicity was calculated according to (experimental release−spontaneous release)/(total release−spontaneous release)×100%. A 1.5-fold increase in CDC activity of postimmune sera over preimmune sera was considered as positive.
Antibody-dependent cell-mediated cytotoxicity
ADCC was performed according to the protocol of ADCC reporter bioassay (Promega, Madison, Wisconsin, USA). Briefly, MCF-7 cells (1.25×104/25 µL) were placed in each well of a 96-well plate, followed by adding human serum (25 µL) and effector cells (7.5×104/25 µL). Six hours after incubation, Bio-Glo luciferase assay (Promega) reagent (75 µL) was added to each assay well, and the luminescence was determined by a plate reader. A 1.1-fold increase of postimmune sera over preimmune sera was considered as positive.
Statistical methods
Efficacy and baseline variables were evaluated in the modified intent-to-treat (mITT) population, which included all patients who received at least one injection of study drug and were analyzed according to randomized treatment. The safety population included all patients who received at least one injection of study drug and who had at least one post-dose safety assessment and were analyzed according to treatment received.
PFS and OS for each treatment group were evaluated using the Kaplan–Meier method with treatment effect and treatment comparison (HR, associated CI, and p value) estimated from the Cox proportional hazards model stratified by hormone therapy use during study treatment (yes or no) and investigator-reported baseline disease status (CR or PR/SD). The proportional hazards model was also used to assess the potential factors associated with the immune response and the post hoc analyses on PFS. Safety variables were analyzed with treatment comparison using Fisher’s exact test. All p values were based on two-sided tests with no multiple comparison adjustments. A total of 289 disease progression events or deaths were estimated to detect an HR of 0.67 with 90% power using a two-sided log-rank test at 5% level of significance. Assuming an extension of median PFS from 6 to 9 months (ie, HR 0.67), a 2-year recruitment and a 2-year follow-up period, and accounting for an 11% dropout rate, a sample size of 342 patients was required.
Results
Patients
Between January 13, 2011, and August 25, 2014, a total of 349 patients were enrolled and randomly assigned to either AS/OBI-821 (n=225) or placebo (n=124), both in combination with cyclophosphamide. One patient randomized to AS/OBI-821 did not receive study treatment and was excluded from the mITT and safety populations (figure 1). Baseline characteristics were well balanced between the treatment groups (table 1). A total of 121 (75%) of the 161 patients in the AS/OBI-821 group and 63 (75%) of the 84 patients in the placebo group with ER+ or PR+ tumors received concurrent antihormonal therapy throughout the study.

Trial profile. PFS, progression-free survival.
Patient demographics and baseline disease characteristics (modified intent-to-treat population)
The data cutoff date was November 1, 2015. Of the patients who received study treatment, 104 (46%) of 224 assigned to AS/OBI-821 and 64 (52%) of the 124 assigned to placebo received all nine scheduled study drug injections. The main reason for treatment discontinuation was disease progression (109 patients (49%) in the AS/OBI-821 group and 50 patients (40%) in the placebo group). Other causes included consent withdrawal (7 (3%) and 8 (6%), respectively), AEs (2 (<1%) and 2 (2%), respectively), non-compliance (one patient (<1%)) in the AS/OBI-821, and loss to follow-up (one patient (<1%)) in the AS/OBI-821 group).
Efficacy
At the time of this analysis, the median follow-up time for patients was 22.3 months in the AS/OBI-821 group and 21.2 months in the placebo group. A total of 159 patients (71%) in the AS/OBI-821 group experienced an investigator-assessed PFS event (all disease progression events) compared with 90 patients (73%) in the placebo group (89 disease progression events and one death). Median PFS by investigator assessment was 7.6 months (95% CI: 6.5–10.9) in the AS/OBI-821 arm and 9.2 months (95% CI: 7.3–11.3) in the placebo arm (HR=0.96; 95% CI: 0.74–1.25; p=0.77; figure 2). Exploratory analyses evaluating subgroups of patients based on stratification factors (hormone therapy use and disease status at baseline) and breast tumor subtypes (hormone receptor-positive (HR+)/HER2-negative (HER2–), triple-negative breast cancer (TNBC), HER2-positive (HER2+)) revealed no difference in PFS by treatment group within each subgroup (online supplementary figure 1).
Supplemental material

Investigator-assessed progression-free survival in patients treated with AS/OBI-821 or placebo. Kaplan–Meier estimates; modified intent-to-treat population.
At the time of the analysis for the PFS endpoint, 85 deaths were reported. These occurred in 50 patients (22.3%) in the AS/OBI-821 arm and 35 patients (28.2%) in the placebo arm. The majority of deaths were due to disease progression. The median OS had not been reached for either treatment group. Preliminary OS analysis of patients treated with AS/OBI-821 versus placebo showed an HR of 0.79 (95% CI: 0.51–1.22; p=0.29).
Correlation of anti-Globo H response with PFS
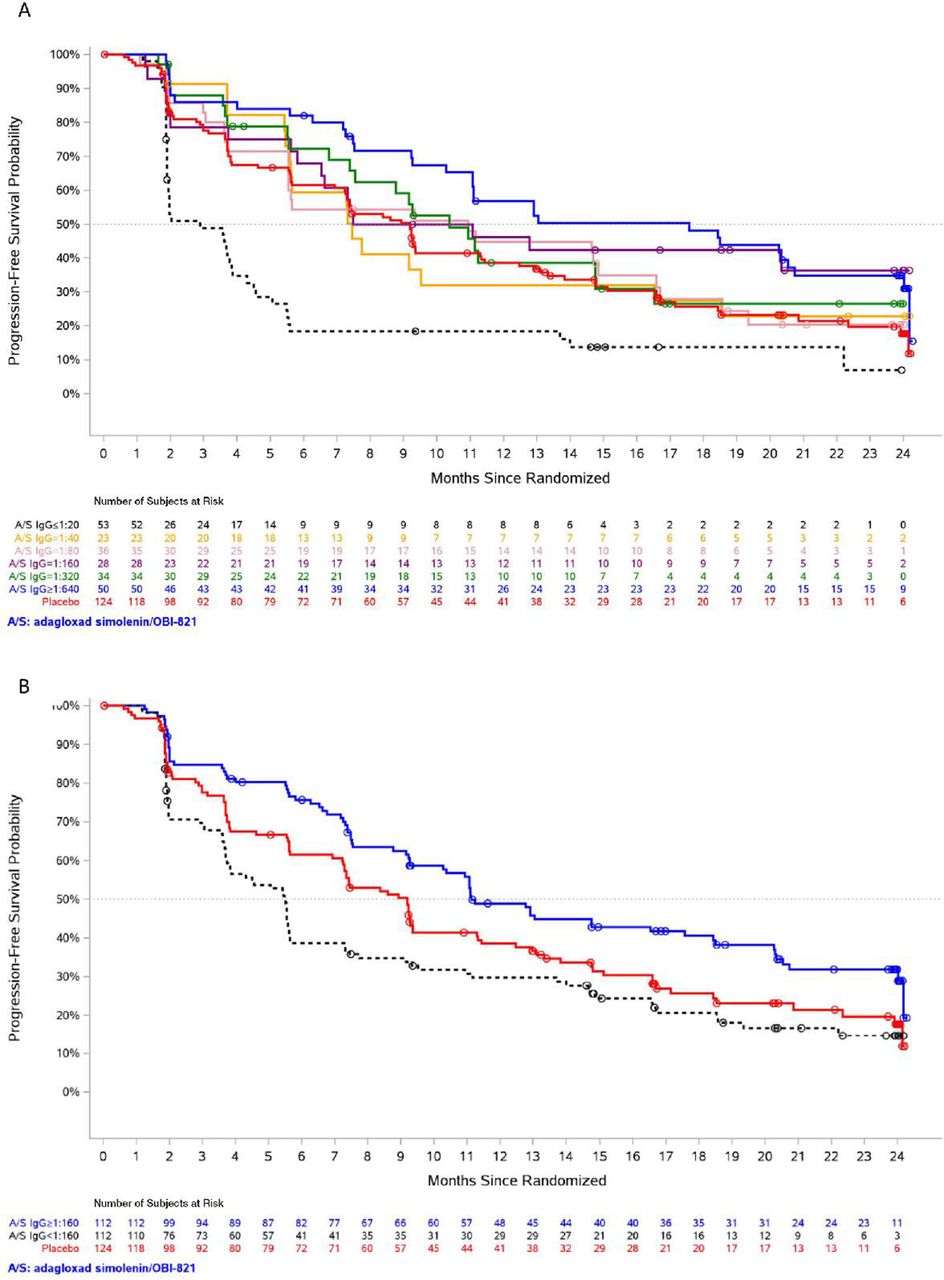
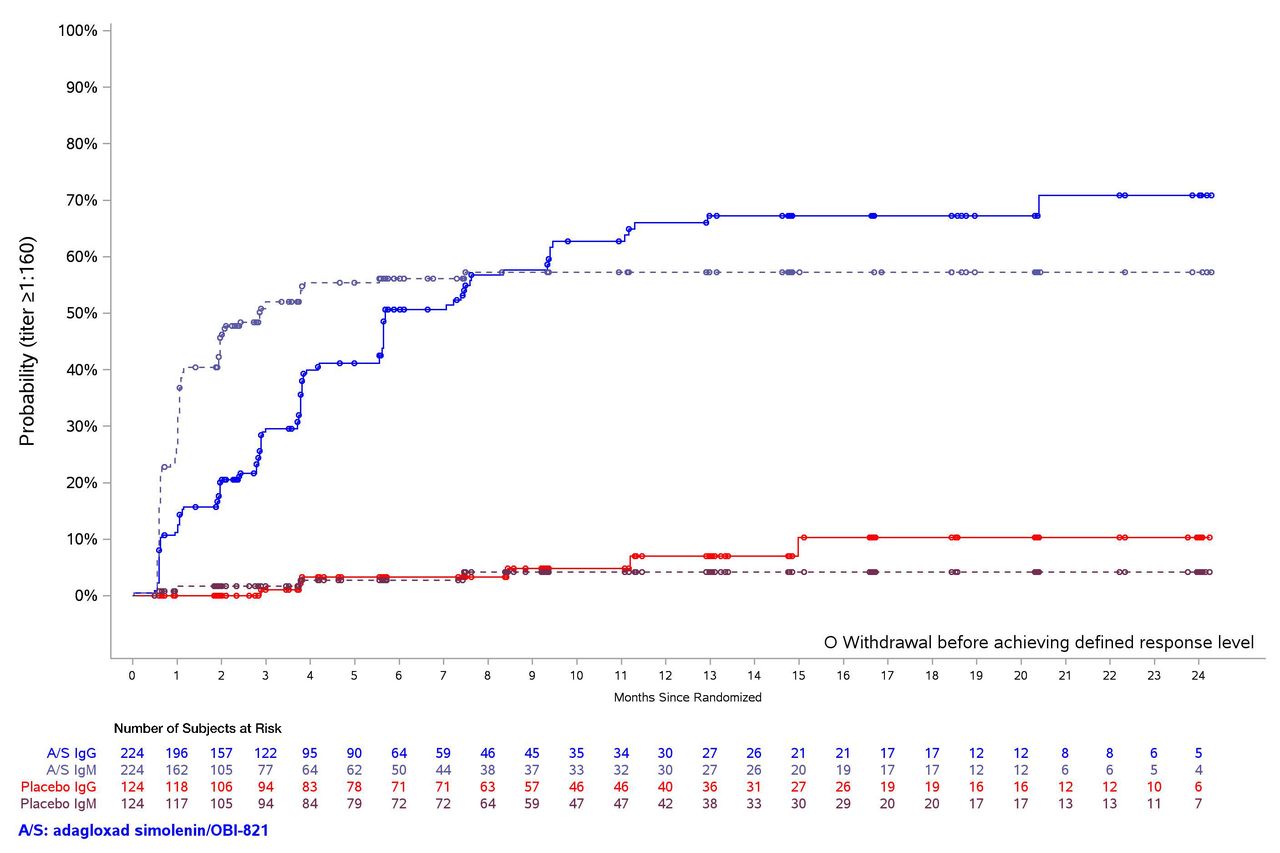
Of the 224 patients treated with AS/OBI-821, 199 (89%) generated a detectable anti-Globo H IgM (titer ≥1:20) and 182 (81%) generated a detectable anti-Globo H IgG (titer ≥1:20) at least once during the study. An evaluation of the correlation between anti-Globo H IgG antibody titer levels and PFS outcome revealed that the higher the anti-Globo H IgG antibody levels, the better the PFS outcome, and the curve with a titer level of 1:160 started showing a trend of better PFS than the placebo curve (figure 3A). Using an anti-Globo H IgG titer of 1:160 as a cutoff, patients treated with AS/OBI-821 with an IgG titer ≥1:160 at any time during study treatment (n=112) had improved median PFS (11.1 months (95% CI: 9.3–17.6)) compared with those who never achieved an IgG titer ≥1:160 (n=112) (5.5 months (95% CI: 3.7–5.6)); HR=0.52; 95% CI: 0.37–0.71; p<0.0001, and placebo-treated patients (n=124) (9.2 months (95% CI: 7.3–11.3)); HR=0.69; 95% CI: 0.50–0.94; p=0.02 (figure 3B). In general, AS/OBI-821 was immunogenic, and IgM response occurred earlier than IgG response with median time to anti-Globo H titer 1:160 of 2.9 months (95% CI: 2.0–7.5) and 5.7 months (95% CI: 5.6–9.3) for IgM and IgG, respectively (figure 4).

Progression-free survival (PFS) according to (A) anti-Globo H IgG titer level and (B) immune response. Panel A shows PFS for AS/OBI-821 recipients according to anti-Globo H IgG titer level and placebo recipients. Other than the placebo curve, each curve represents a group of patients with their maximum anti-Globo H IgG antibody titers at any time during the study reaching the specified level. These groups of patients were mutually exclusive. Panel B shows AS/OBI-821 recipients with and without an immune response and placebo recipients. AS/OBI-821-treated patients were divided into IgG (+), defined as patients with anti-Globo H IgG antibody titers ≥1:160 at any time, and IgG (-), defined as those whose anti-Globo H IgG antibody titers had never reached ≥1:160 at any time.

Cumulative IgG/IgM response based on Kaplan–Meier estimate (time to first IgG/IgM response). IgG/IgM immune response was defined as anti-Globo H IgG/IgM antibody titer ≥1:160 at any time.
In a post hoc analysis, KLH IgG levels at week 40 were available for 95 patients in the AS/OBI-821 arm and 59 patients in the placebo arm. As expected, patients who received AS/OBI-821 had a higher KLH IgG titer than those who received placebo; however, no significant differences in KLH IgG levels were observed between AS/OBI-821 recipients who had an anti-Globo H IgG titer ≥1:160 and those who had an anti-Globo H IgG titer <1:160 (online supplementary figure 2).
Supplemental material
Correlation of tumor Globo H expression with PFS
Of the 348 patients who received at least one dose of study treatment, tumor samples for Globo H antigen testing were available from 243 patients (70%); 159 in the AS/OBI-821 arm and 84 in the placebo arm (table 1). Globo H expression was evaluated and scored as 0 (AS/OBI-821, 44 vs placebo, 25), 1+ (57 vs 30), and 2+ and 3+ combined (58 vs 29) by IHC and was detected (Globo H expression 1+, 2+, or 3+) in 72% (115/159) of the AS/OBI-821-treated patients and in 70% (59/84) of the placebo-treated patients. For patients with no Globo H expression detected, the comparison for PFS between the AS/OBI-821 and placebo groups showed an HR of 0.75 (95% CI: 0.41–1.36; p=0.34). Similar analyses in the subgroups of patients with Globo H expression 1+ and with Globo H expression 2+ and 3+ combined showed HRs of 1.22 (95% CI: 0.72–2.07; p=0.46) and 0.77 (95% CI: 0.46–1.30; p=0.33), respectively. This analysis evaluating the potential correlation between percentage of Globo H-expressing cells and PFS was inconclusive.
Post hoc analyses evaluating potential factors associated with anti-Globo H IgG response
Post hoc analyses suggested that a greater percentage of patients without progressive disease events after diagnosis of metastatic disease had an anti-Globo H IgG ≥1:160 (57% (78/137)) compared with those with one or two events of progressive disease (39% (34/87)). In addition, a higher percentage of patients with CR status at the time of randomization had anti-Globo H IgG ≥1:160 (62% (18/29)) compared with those with non-CR status (PR or SD) at baseline (48% (94/195)). A higher percentage of patients with ER+ disease achieved anti-Globo H IgG ≥1:160 (53% (95/180)) compared with those with ER− disease (39% (17/44)). However, given the relatively small sample size, the significance of these associations awaits validation in future studies.
Post hoc subgroup analysis for Globo H expression and tumor subtype
Globo H expression was analyzed by breast cancer tumor subtypes (TNBC, HER2+, HR+). The percentages of patients with 0, 1+, 2+, and 3+ were not different by cancer type (online supplementary table 1).
Supplemental material
Post hoc subgroup analysis for patients completing all nine planned injections
The baseline characteristics between patients receiving all nine injections and those who received less than the nine injections were similar (online supplementary table 2). In the patients who had completed all nine injections of study drug, median PFS was 20.7 months (95% CI: 18.5−not estimable) in the AS/OBI-821 arm and 16.7 months (95% CI: 13.3−22.3) in the placebo arm (HR=0.66; 95% CI: 0.42−1.01; p=0.06) (figure 5).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Investigator-assessed progression-free survival in patients treated with nine injections of AS/OBI-821 or placebo. Kaplan–Meier estimates.
Safety
A similar incidence of all treatment-emergent adverse events (TEAEs) (98.2% vs 96.0%) and non-injection site TEAEs (95.1% vs 94.4%) occurred in the AS/OBI-821 and placebo arms, respectively (table 2). TEAEs at the injection site were more common in the AS/OBI-821 arm than in the placebo arm (77.2% vs 15.3%; p<0.0001). All injection site reactions were grade 1 or 2 in severity and transient, and the incidence decreased with successive injections. A statistically significant higher incidence of fever was reported with AS/OBI-821 (20.1%) compared with placebo (6.5%; p<0.0005). Most non-injection site TEAEs were grade 1 or 2 in severity.
Treatment-emergent adverse events (TEAEs) occurring in ≥10% of patients in any treatment group (safety population)
Serious adverse events (SAEs) were reported in 29 patients (12.9%) in the AS/OBI-821 arm and in 15 patients (12.1%) in the placebo arm. There were three serious adverse drug reactions with AS/OBI-821 (hypersensitivity in two patients and fever in one patient; all recovered without sequelae).
Deaths related to SAEs occurred in four patients in the AS/OBI-821 arm (three due to disease progression and one due to central nervous system metastases) and in no patients in the placebo arm.
Immune studies
The first 40 patients who completed all nine planned injections and developed median or greater titers of IgM or IgG anti-Globo H antibodies (≥1:160) were selected and exploratory FACS, CDC, and ADCC assays were performed on immune sera to explore tumor cell binding and potential functional impact of these vaccine-induced polyclonal antibodies. Anti-Globo H IgM antibodies bound to Globo H-expressing MCF-7 cells had a peak 3.26-fold increase at 4 weeks, which was associated with a 1.66-fold peak increase in CDC also at 4 weeks (online supplementary figure 3A). Anti-Globo H IgG antibody binding to MCF-7 cells was not observed as a mean increase over baseline (online supplementary figure 3B), although sera from 17 of 40 patients tested demonstrated increases in ADCC over baseline of between 1.1-fold and 2.6-fold (online supplementary figure 4 and online supplementary table 3).
Supplemental material
Supplemental material
Supplemental material
Discussion
AS/OBI-821 is a therapeutic cancer vaccine targeting Globo H, the most prevalent TACA for active immunotherapy. This randomized phase II study demonstrated that vaccination with AS/OBI-821 was well tolerated and immunogenic. Although the primary endpoint of improved PFS compared with placebo was not reached, in a post hoc analysis, patients receiving AS/OBI-821 who generated an anti-Globo H antibody immune response with anti-Globo H IgG titers ≥1:160 had a significantly improved PFS compared with vaccine-treated patients whose anti-Globo H IgG titers never reached 1:160 and patients in the placebo group.
The development of a humoral immune response that targets specific tumor antigens is an important step in the eradication of tumor cells.22 However, the study of vaccines as a treatment for solid tumors has been complicated by multiple factors, including unique tumor antigen expression and poor generation of immune responses.23 In previous cancer vaccine studies using a carbohydrate antigen, Theratope cancer vaccine (Biomira), containing sialyl-Tn (STn), a carbohydrate epitope found on a variety of glycoproteins, conjugated to KLH combined with the adjuvant Detox (STn-KLH) was shown to be effective in early phase studies. In 1999, two phase II trials compared the use of low-dose cyclophosphamide with and without Theratope and reported a statistically significant increase in survival among patients treated with Theratope versus patients not treated with the vaccine (median overall survival (mOS) of 19.1 vs 9.2 months, respectively).24 However, in a phase III trial with 1030 women with MBC, mOS between the treatment and control groups (23.1 vs 22.3 months, respectively) was not significantly different despite high IgG titers in patients treated with Theratope and no detectable antimucin antibodies in the control group. The authors suggested that perhaps the tumor-specific antibody response to STn did not occur in time to prevent disease progression, particularly because the patients in this study had advanced metastatic disease, and thus studying a population with earlier stage disease may be of benefit.25 However, post hoc analysis revealed that patients who received concomitant endocrine therapy and STn-KLH had a longer time to progression and OS than the control group of women who received KLH alone. Moreover, of the women who received endocrine therapy, those with a median or greater antibody response (titer >1:320 toward ovine submaxillary mucin) to the STn-KLH vaccine had significantly longer median OS than those who had a below-median antibody response.26 This observation is in line with our finding of improved PFS for AS/OBI-821 recipients who generated an anti-Globo H antibody immune response.
In this trial, anti-Globo H IgG antibodies were detected in patients immunized with AS/OPT-821, suggesting that glycopeptides containing the Globo H moiety might be presented by major histocompatibility complex class II molecules to cyclin-dependent 4 (CD4) T cells to induce class switch recombination. In our preclinical testing of the Globo H-KLH vaccine in C57BL/6 mice, both IgG and IgM anti-Globo H antibodies were induced; however, no T-cell activation in response to Globo H glycan moiety alone was observed.
Cyclophosphamide was given to enhance the immune response to the AS/OBI-821 vaccine. Low-dose cyclophosphamide reduces the suppressive function of CD4+ CD25+ regulatory T cells in experimental tumor models27 28 and patients with cancer.28 29 It is possible that cyclophosphamide combined with AS/OBI-821 reduces suppressive regulatory T cells, thereby increasing the humoral response to the vaccine.27–30 In the current trial, AS/OBI-821 led to high levels of IgM and IgG, which correlated with improved PFS.
Exploratory immune studies using sera from patients who had a humoral response supported binding of vaccine-induced IgM antibodies to Globo H-expressing MCF-7 cells with peak increases at 4 weeks, which was also associated with an increase in CDC. However, anti-Globo H IgG antibody binding to MCF-7 cells was not observed as a mean increase over baseline, although sera from 17 of 40 patients tested demonstrated fold increases in ADCC over baseline of between 1.1-fold and 2.6-fold. These data should be interpreted with caution given the exploratory nature of these studies and a representative sample that was used.
While it is possible that AS/OBI-821 benefits those patients able to generate a humoral immune response, it is important to acknowledge the possibility that the anti-Globo H immune response was simply a prognostic factor (ie, patients who were able to generate an immune response had a better prognosis). Interestingly, an exploratory post hoc analysis found that patients with and without the anti-Globo H immune response had similar anti-KLH immune responses at week 40, suggesting that the specific antigen response to Globo H may be more pertinent to PFS. These findings must be interpreted with caution due to the exploratory nature of the analyses.
In this first-in-class, randomized, phase II trial of vaccination against Globo H, a broad range of breast tumor subtypes were included (HR+/HER2–, TNBC, HER2+), likely contributing to both reduced power to detect potential impact on PFS and the inability to identify specific breast tumor subtypes that could possibly benefit from AS/OBI-821 treatment. Globo H expression has been observed in similar intensity across breast cancer tumor subtypes,16 suggesting that expression alone would not impact subtype-specific response.
The heterogeneity of the study population and the variable ability to mount an immune response may have contributed to the lack of improved PFS in the entire cohort of vaccinated patients. A post hoc analysis showed that having no event of progressive disease after a diagnosis of metastatic disease, a CR status at randomization or ER+ disease was associated with a higher probability of developing an anti-Globo H IgG ≥1:160 compared with those who had more extensive prior therapies, a non-CR status at baseline, or ER‒ disease. Although this is an exploratory post hoc analysis, a lack of extensive prior treatment has correlated with a better response to immune checkpoint inhibitors and raises the potential for combination therapy with additional checkpoint inhibitors for improved outcomes.31 32 Additional studies to evaluate tumor and patient factors associated with anti-Globo H IgG immune response are needed. In addition, the ability to generate an immune response could be enhanced by combining the vaccine with chemotherapy or immune checkpoint blockade. Further, a tumor-specific antibody response may not have occurred quickly enough to prevent disease progression in patients with more rapidly progressing disease. Although patients receiving all planned injections appeared to have a better PFS than those who stopped treatment early, this could simply be an indicator of disease biology. Collectively, these findings support studying a population with earlier stage disease.
The ability of a therapeutic vaccine to demonstrate therapeutic benefit may be in part dependent on continuous exposure to the tumor antigens in the vaccine. In this trial, patients stopped treatment after nine injections rather than at disease progression; therefore, we cannot rule out the possibility that continued vaccination might be advantageous. The relationship between Globo H antigen expression by IHC and efficacy in patients receiving AS/OBI-821 was explored in a preplanned subset analysis. The correlation of the presence of weak to strong Globo H expression with PFS was inconclusive. This analysis was based on the percentage of Globo H-positive staining tumor cells only, which may not be a sensitive enough marker. A better scoring method that takes into account the intensity of positive staining tumor cells is currently being validated (the Globo H IHC H-score).
The current study has several limitations. As discussed, it prescribed only nine injections of vaccine, irrespective of patient response. An anti-Globo H IgG titer of 1:160 was used as a threshold for humoral immune response in several analyses; however, this threshold was retrospectively chosen based on analyses, indicating that this was the value above which a PFS benefit was observed. Tumor samples were not available for further analysis of potential biomarkers of response, and the trial was not powered for an OS endpoint—which may be a more sensitive indicator of beneficial immune response.
Conclusion
Because MBC remains incurable despite available treatments, novel therapies with different mechanisms of action to stimulate the patient’s own immune system are of great interest, as reflected by numerous ongoing clinical immunotherapy trials and the recent regulatory approval of a checkpoint inhibitor for advanced breast cancer. The results of this trial provide the basis for the development of a phase III study focusing on a well-defined group of patients with less heavily pretreated and earlier stage breast cancer who are more likely to generate an effective humoral immune response to AS/OBI-821.
References
Footnotes
Contributors C-SH developed the protocol for the study, enrolled patients in the study, helped with interpretation of data, reviewed and approved the manuscript, and is the Chairman of the Publication Steering Committee. ALY developed the protocol for the study, helped with interpretation of data, directed ad hoc analysis of the tissue samples, reviewed, edited, and approved the manuscript, and is a member of the Publications Steering Committee. L-MT enrolled patients in the study and reviewed and approved the manuscript. LWCC enrolled patients in the study, reviewed and approved the manuscript, and is a member of the Publications Steering Committee. M-FH enrolled patients in the study and reviewed and approved the manuscript. SAH helped with protocol development, enrolled patients in the study, helped with interpretation of data, reviewed and approved the manuscript, and is a member of the Publications Steering Committee. RBS enrolled patients in the study, reviewed, edited, and approved the manuscript, and is a member of the Publications Steering Committee. JLM helped with protocol development, enrolled patients in the study, reviewed and approved the manuscript, and is a member of the Publications Steering Committee. H-KC enrolled patients in the study and reviewed and approved the manuscript. H-TC enrolled patients in the study and reviewed and approved the manuscript. S-CC enrolled patients in the study and reviewed and approved the manuscript. S-BK reviewed the study protocol, enrolled patients in the study, reviewed and approved the manuscript, and is a member of the Publications Steering Committee. J-TH validated the immunohistochemical (IHC) method and performed the IHC analysis for Globo H expression and reviewed and approved the manuscript. S-HU performed pathological examinations and IHC testing of Globo H expression, and reviewed and approved the manuscript. S-HL developed the statistical analysis plan and analyzed data according to the plan; reviewed, edited, and approved the manuscript. C-CC managed the clinical trial implementation, and reviewed and approved the manuscript. HSR helped with protocol development, enrolled patients in the study, interpreted data, helped with preparation and review of the manuscript, and is a member of the Publications Steering Committee. HSR, C-SH, and ALY were involved in the design of the study protocol, conduct of the study as investigators, members of the Study Steering Committee, analysis of data, and contributed to the manuscript and reviewed/edited the manuscript at every stage prior to approving for publication. All other authors contributed to review of the protocol, were investigators in the study, and were members of the Study Steering Committee. All authors contributed to the manuscript, reviewed it at every stage, and approved the manuscript for publication.
Funding The study is funded by OBI Pharma, Inc. (Taipei, Taiwan) and MOEA Grant number 100-EC-17-A-20-I1-0059 and EC-17-A-20-I1-0123.
Competing interests C-SH: Consulting fees from Amgen, AstraZeneca, Pfizer, and Roche. Contracted Research with Amgen, AstraZeneca, Eli Lilly, MSD, Novartis, Pfizer, and Roche. ALY: Member of a scientific advisory board for OBI Pharma and member of the Board of Directors for OPKO Health Corporation; has received funding for sponsored research from United Therapeutics Corporation and Cancer Prevention Pharmaceuticals. SAH: Has received grants/support from Ambrx, Amgen, Bayer, Biomarin, BI Pharma, Cascadian, Daiichi Sankyo, Dignitana, Genentech, GSK, Eli Lilly, MacroGenics, Medivation, Merrimack, Novartis, OBI Pharma, Pfizer, Pieris, PUMA Biotechnology, Roche, and Seattle Genetics. Travel support from Eli Lilly, Novartis, and OBI Pharma. RBS: Owns stock in Samumed; expert witness for PUMA Biotechnology. H-KC: Research grants from Merck, Ono, and Roche. S-BK: Institutional funding from Dongkook Pharmaceutical Co, Genzyme, Kyowa Kirin, and Novartis. S-HL: Employee of OBI Pharma. C-CC: Previously employed by OBI Pharma. Consultant to Amwise Diagnostics, MiCareo Diagnostics, and SynCore Pharmaceuticals. Independent board member of Anxo Pharmaceuticals. HR: Receives research support for clinical trials through the University of California at San Francisco from: Eisai, Daiichi Sankyo, Genentech/Roche, Eli Lilly, MacroGenics, Merck, Novartis, OBI Pharma, Odonate, Pfizer, and Plexxikon. Has received travel support for clinical trials from Amgen, Eli Lilly, Merck, Mylan, Pfizer, and PUMA Biotechnology.
Patient consent for publication Not required.
Ethics approval This study was performed in accordance with the ethical principles outlined in the Declaration of Helsinki and Good Clinical Practice guidelines, and in compliance with relevant local laws and regulations. The trial protocol was approved by the relevant institutional review boards of each study center.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. The datasets generated and/or analyzed during the current study are not publicly available due to the fact that the study is ongoing and overall survival status is still being followed.