Article Text

Abstract
Background A synergy between radiotherapy and anti-cytotoxic-T-lymphocyte-associated antigen 4 (anti-CTLA-4) monoclonal antibody has been demonstrated preclinically. The Mel-Ipi-Rx phase 1 study aimed to determine the maximum tolerated dose (MTD) and safety profile of radiotherapy combined with ipilimumab in patients with metastatic melanoma.
Patients and methods A 3+3 dose escalation design was used with 9, 15, 18 and 24 Gy dose of radiotherapy at week 4 combined with 10 mg/kg ipilimumab every 3 weeks for four doses. Patients with evidence of clinical benefit at week 12 were eligible for maintenance with ipilimumab 10 mg/kg every 12 weeks starting at week 24 until severe toxicity or disease progression. The database lock occurred on April 30, 2019. Tumor growth rate of irradiated lesions and non-irradiated lesions were analyzed to assess the systemic immunologic antitumor response. Blood immune monitoring was performed before and during treatment to determine if radiotherapy could modify ipilimumab pharmacodynamics.
Results 19 patients received ipilimumab between August 2011 and July 2015. Nine patients received the four doses of ipilimumab. All patients received the combined radiotherapy. Grade 3 adverse events occurred in nine patients, the most common being colitis and hepatitis. No drug-related death occurred. Dose limiting toxicity occurred in two of six patients in the cohort receiving 15 Gy. The MTD was 9 Gy. Two patients had complete response, three had partial response response and seven had stable disease, giving an objective response rate of 31% and a clinical benefit rate of 75% at week 24. The median duration of follow-up was 5.8 years (Q1=4.5; Q3=6.8). The median overall survival (95% CI) was estimated at 0.9 years (0.5–2). The median progression-free survival (PFS) (95% CI) was 0.4 (0.2–1.4). Radiotherapy combined with ipilimumab was associated with increased CD4+ and CD8+ICOS+ T cells. Increased CD8+ was significantly associated with PFS.
Conclusion When combined with ipilimumab at 10 mg/kg, the MTD of radiotherapy was 9 Gy. This combination of ipilimumab and radiotherapy appears to be associated with antitumor activity. Increased CD8+ was significantly associated with PFS. Thus, immune biomarkers may be useful for early response evaluation.
Trial registration number NCT01557114.
- radiotherapy
- radioimmunotherapy
- CTLA-4 antigen
- melanoma
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Immunotherapy using immune checkpoint inhibition has revolutionized the management of patients with advanced stage melanoma and is an emerging approach for many other cancers.1 The first immune checkpoint inhibitor that was developed was ipilimumab.2 Ipilimumab targets the cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) and significantly improves the overall survival in patients with metastatic melanoma.2 3 However, the objective response rate (ORR) and the disease control rates (proportion of patients with a partial response (PR) or complete response (CR) or stable disease (SD)) are relatively low (10.9% and 28.5%, respectively).3 As such, increased interest has been drawn to enhance the induction of systemic immune responses of ipilimumab by combining it with radiotherapy.4–6 One of the rationale put forward to combine these therapies is that ipilimumab is able to deplete T-regulatory cells (Treg cells) through antibody-dependent cell cytotoxicity and, consequently, increases the CD8 T cell to Treg ratio, whereas radiotherapy promotes the diversity of the T-cell receptor (TCR) repertoire of intratumoral T cells.7–10 When combined, ipilimumab promotes the expansion of T cells, while radiation enhances the TCR repertoire of the expanded peripheral clones.4 Ipilimumab at a dose of 3 mg/kg is approved in several countries for the treatment of unresectable or metastatic melanoma. In a recent prospective phase 1 study, 35 patients were treated with ipilimumab 3 mg/kg combined with concurrent or sequential stereotactic ablative radiotherapy.11 Dose limiting toxicities (DLTs) and grade 3 toxicities were reported in 6% and 34% of patients, respectively. PR and clinical benefit were reported in 10% and 23% of patients, respectively. However, few clinical studies were conducted to assess the efficacy of ipilimumab 10 mg/kg combined with radiotherapy,11–15 although overall survival was significantly improved with the ipilimumab 10 mg/kg monotherapy compared with the 3 mg/kg dose.2 Here, we present the phase 1 ‘Mel Ipi Rx’ study investigating the safety and efficacy of ipilimumab 10 mg/kg combined with radiotherapy in patients with metastatic melanoma. Although the treatment landscape of patients with advanced melanoma has changed since this study was initiated, the increased survival benefit of ipilimumab 10 mg/kg compared with 3 mg/kg suggests that the clinical utility of ipilimumab in refractory patients with high unmet medical need could warrant further assessment. The primary objective of this study was to determine the maximum tolerated dose (MTD), DLT and the recommended phase 2 dose (RPTD) of radiotherapy administered in combination with ipilimumab at a dose of 10 mg/kg in patients with metastatic melanoma. The secondary objectives were to determine the adverse event (AE) profiles, to describe the preliminary antitumor activity following escalating doses of radiation combined to ipilimumab using the immune-related response criteria (irRC) and to evaluate the overall survival in patients treated with this combination. The exploratory objectives were to evaluate the systemic immunologic antitumor response and factors influencing this response.
Methods
Patients
Eligible patients had unresectable locally advanced or metastatic melanoma with at least one measurable metastasis accessible to radiotherapy. Subcutaneous nodules and lymph nodes were considered as targets for irradiation. Tumor lesions located within vital organs or gastrointestinal tract were not considered as target for radiotherapy. All patients had measurable and non-measurable disease evaluable according to irRC. Patients were ≥18 years of age, were able to give written informed consent, had Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 1 and had normal renal and liver functions on blood tests. Patients were excluded if they had one of the following criteria: (1) suspected or known central nervous system tumors including brain metastasis, (2) any other malignancy with a disease-free for less than 5 years, (3) an autoimmune disease, (4) a history of prior treatment with ipilimumab, (5) prior radiotherapy within the same body area or (6) radiotherapy in fields containing flat bones (volume >35%). If chemotherapy or immunotherapy were previously used, a wash-out period of 2 weeks at least was required before the first administration of ipilimumab.
Study design
This phase I, 3+3 dose escalation study evaluated the MTD of radiotherapy in combination with ipilimumab in patients with unresectable locally advanced or metastatic malignant melanoma. Eligible patients received ipilimumab at 10 mg/kg at weeks 1, 4, 7 and 10 for a total of four doses, at 3-week intervals (online supplementary figure S1). Patients without progressive disease (PD) who tolerated the treatment continued ipilimumab dosing in 12-week intervals until progression or withdrawal of consent. Radiotherapy was delivered on week 4 (on Monday, Tuesday and Friday), at the time of the second cycle of ipilimumab, on measurable, superficial lesions including subcutaneous nodules and lymph nodes. Radiotherapy was delivered using >4 MV photons or electrons with standard field encompassing. Maximal field had to be at least 5×5 cm but not be more than 10×10 cm maximal dimensions on a lesion. Millimetric margins were used to take into account microscopic spreading and patient movements (clinical and planning target volumes of 5 mm). Dose escalation of ionizing radiation was planned in cohorts of three to six patients depending on the occurrence of DLTs during the first combination treatment cycle. A hypofractionated radiation regimen (higher doses per fraction) was used. Dose escalation was used with total doses of 9, 15, 18 and 24 Grays (Gy) administered in three fractions every Monday, Wednesday and Friday and planned in cohorts of three to six patients depending on the occurrence of DLTs from week 4 to week 10. A minimum deadline of 48 hours between two radiotherapy sessions had to be respected. If necessary, the radiotherapy could be put back to Tuesday-Thursday-Saturday. Given the small size of the radiation field, and the fact that irradiated lesions were superficial, vital organs and gastrointestinal tract were not involved in the irradiated field.
Supplemental material
Toxicities were evaluated according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0. DLT observation period ranged from week 4 to 10. Any toxicity before the start of radiotherapy was not considered as a DLT but as a toxicity from ipilimumab alone. The DLT was defined by the appearance of at least one of the following study combination-related event within 6 weeks: (1) grade 4 vomiting, diarrhea or gastrointestinal bleeding; (2) grade 3 or 4 non-hematologic toxicity (excluding grade 3 nausea, vomiting, diarrhea and transient fever); or (3) grade 3 or 4 radiation dermatitis (except if return to grade ≤2 within 2 weeks). If none of the first three subjects in a given dosing cohort had experienced DLT, dose escalation was realized. If one of the first three subjects in a given dosing cohort had experienced DLT, an additional three subjects were enrolled to that dose level before further escalation was considered. A dose escalation was realized if none of these additional three subjects had experienced DLT. If two of the first three subjects in a given dosing cohort had experienced DLT, dose escalation was stopped. Dose escalation was continued until one-third or more of the subjects at a particular dose level experienced DLT or up to the fourth cohort. This was considered the maximum administered dose (MAD). The MTD was defined as the highest dose at which less than one-third of the subjects experienced DLT. The RPTD was defined as the MTD or the dose that was considered to give the optimal clinical and/or immunological results. Tumor assessments consisting of CT scans and assessment of skin lesions were performed at weeks 12, 24 and every 12 weeks thereafter until the patient withdrew from the study or entered the follow-up phase. MRI or CT scan of the brain had to be realized when clinically indicated. Evidence of PD was confirmed by a second assessment performed 4–6 weeks later. Definitions of lesions were based on irRC. Measurable lesions were defined as lesions that could be accurately measured in two perpendicular diameters, with at least one diameter ≥20 mm and the other dimension ≥10 mm. It was possible to consider skin lesions if they were measurable. All measurable lesions, up to a maximum of 5 lesions per organ and 10 lesions in total were identified as index lesions, measured and recorded at screening and follow-up. The index lesions were representative of all involved organs. Non-index lesions corresponded to measurable lesions that were recorded and evaluated at the same assessment time points as the index lesions and that were irradiated according to the trial irradiation design.
Blood immune monitoring
Blood samples were collected at baseline (T0), at week 4 (W4) (before second injection of ipilimumab) and at week 6 (W6) (after radiotherapy and before third injection of ipilimumab) (online supplementary figure S2). Phenotyping was performed on fresh whole blood, and peripheral blood mononuclear cells (PBMCs) isolated by Ficoll density gradient were frozen for later analyses. Data analysis from standard blood tests was realized to estimate the derived neutrophil to lymphocyte ratio (dNLR) at baseline, W4 and W6 to see whether or not granulocytes could impact the prognosis of patients. Whole blood or PBMCs were incubated with fluorochrome-conjugated antibodies for 15 min at room temperature or at 4°C, respectively, followed by 20 min of lysis (Versalyse, Beckman Coulter, Mervue, Galway, Ireland). The following fluorochrome-conjugated antibodies were used: fluorescein isothiocyanate anti-ICOS (CD278, clone: DX29), phycoerythrin (PE)-conjugated anti-CD25 (clone: B1.49.9), allophycocyanin-cyanine 7 (APC-Cy7)-conjugated CD45RA (clone: HI100), phycoerythrin-cyanine 7 (PE-Cy7)-conjugated anti-CD45RA (clone: 2H4), allophycocyanin Alexa Fluor 700 (AA700)-conjugated anti-CD3 (clone: UCHT1), Pacific Blue (PB)-conjugated anti-CD4 (clone: 13B8.2) and Krome orange-conjugated anti-CD8 (clone: B9.11) were obtained from Beckman Coulter. Stained cells were acquired using a FACS Canto II cytometer (BD Bioscience) or a Gallios Cytometer (Beckman Coulter) and analyzed using Kaluza software (Beckman Coulter). Conventional T cells (CD3+CD4+ and CD3+CD8+) were, respectively, defined by CCR7+CD45RA+ for naïve T cells, CCR7+CD45RA- for central memory T cells (TCM), CCR7-CD45RA- for effector T cells (TEM) and CCR7-CD45RA+ for terminally differentiated T cells (TEMRA). Treg cells were defined as CD3+CD127lowCD25+.
Supplemental material
Tumor growth rate analysis
To assess the systemic immunologic antitumor response, tumor growth rate (TGR) of irradiated lesions and non-irradiated lesions were analyzed. Briefly, TGR estimates the variation in tumor volume over time using each patient as his own control and has shown to be interesting to identify the specific therapeutic effect of a treatment regardless of the disease course of each patient.16 17 TGR was expressed as a percentage increase in tumor volume during 1 month, in accordance with Hiniker et al,11 using the following formula: TGR=100 [exp[(3.Log(Dt/Dt0))/t] −1], with D0=tumor size defined as the sum of the longest diameters of the lesions at baseline; Dt=tumor size defined as the sum of the longest diameters of the lesions at the time (t) of evolution evaluation (in months).
TGR=100 [exp(3.Log(Dt/Dt0)/t)−1].
The TGR was computed for irradiated lesions (TGRirr), and non-irradiated target lesions defined by the radiologist for the irRC evaluation (TGRnon-irr) for two treatment periods when data were available: (1) the Reference-TGR (REF-TGR), assessed before the onset of the treatment using the baseline CT and a CT realized before the baseline (prebaseline CT), (2) the Experimental-TGR (EXP-TGR), assessed between the onset of the treatment and the first evaluation. The TGR was computed using the same target lesions at each evaluation time. A positive value of the EXP-TGR reflected a bigger lesion at the first evaluation than at baseline. Therefore, new lesions related to PD were not included in the TGR computation. Difference between EXP-TGR and REF-TGR was used to assess the effect of the treatment (ΔTGR=EXP TGR−REF-TGR), a negative value reflecting a slowdown of the natural course of the disease (ie, a slower tumor growth or a tumor response) between the two periods.
Statistical analysis
Demographic and baseline characteristics were summarized for all registered subjects using descriptive statistics. Toxicity grades per subject were tabulated for AEs and on-study laboratory measurements by using the NCI CTCAE version 4.0. Analyses of efficacy endpoints were based on all subjects evaluable for efficacy.
The Kaplan-Meier method was used to estimate overall survival and immune-related progression-free survival (PFS). Overall survival was defined as the time from treatment initiation to the date of death or date of last follow-up in persons alive at last follow-up. Immune-related progression was defined according to irRC. An event was defined as progression or death whichever comes first. PFS was defined as the time from treatment initiation to the date of occurrence of the event. Follow-up of patients who did not experience was censored at the date of last evaluation. Duration of follow-up was estimated using the Schemper and Smith method.18 All statistical analyses were done using SAS software V.9.4.
Evolution of innate immune cells was analyzed using GraphPAD PRISM software: values at W4 and at W6 were described and compared with baseline by using Friedman test followed by Dunn's multiple comparisons test.
Study oversight
The study was conducted in accordance with the protocol, Good Clinical Practice guidelines and the provisions of the Declaration of Helsinki. All patients provided written informed consent.
Results
Patient population
Nineteen patients with advanced melanoma were treated at Gustave Roussy in the Mel-Ipi-Rx phase 1 trial between August 2011 and July 2015 (online supplementary table S1). The database lock occurred on April 30, 2019. Nine patients received the four doses of ipilimumab and two patients received maintenance ipilimumab (one and two cycles, respectively). All patients received the combined radiotherapy at week 4 in three fractions. Thirteen patients were enrolled at dose level 1 (9 Gy) and six patients at dose level 2 (15 Gy). Demographic data of patients are summarized in table 1. Overall, 8 patients presented visceral metastases (M1c), 10 had elevated level of lactate dehydrogenase (LDH), 10 tumors were BRAF mutated and none had a history of brain metastases. All patients had received systemic therapy previously. Prior therapy included chemotherapy in 7 patients, BRAF inhibitors in 8 patients, radiotherapy in 1 patient and surgery in 16 patients, respectively, and all of them were immune checkpoint inhibitor naïve. Irradiation was delivered on subcutaneous lesions in 10 patients (8 and 2 patients in the cohorts treated with 9 and 15 Gy, respectively) and on lymph nodes in 9 patients (5 and 4 patients in the cohorts treated with 9 and 15 Gy, respectively) (online supplementary table S2). The average irradiated tumor volumes were relatively homogeneous with a median of 34 mm (IQR 34–46.5).
Supplemental material
Patient baseline characteristics
Safety
All patients presented at least one AE of any grade. These AEs were felt to be probably related to ipilimumab. The role of concurrent radiotherapy on these AEs was difficult to assess. However, no radiation-induced necrosis or local symptoms were observed inside the radiation field. AEs of all grades are summarized in table 2, regardless of their attribution.
Adverse events of all grade (safety population)
Asthenia was the most commonly reported AE of any grade. It occurred in 14 patients. Among them, nine patients were treated in the 9 Gy cohort and five patients in the 15 Gy cohort. The median time to onset of asthenia was 4 (Q1-Q3=4–10) weeks, and the median duration was 10 (Q1-Q3=4–19) weeks. The other most common AEs of any grade included diarrhea, disease-related pain, fever, nausea and vomiting.
Thirteen patients discontinued the study owing to treatment-related AEs (nine patients in the cohort receiving 9 Gy and four patients in the cohort receiving 15 Gy). Nine of these 13 patients had AEs of grade 3. Multiple AEs of grade 3 occurred in some patients. AEs of grade 3 included colitis (n=2), hepatitis (n=2), asthenia (n=2), thyroid disorders (n=1), DRESS (drug rash with eosinophilia and systemic symptoms) syndrome (n=1) and nausea/vomiting (n=1). Online supplementary table S3 presents the grade 3 and grade 4 events for each dose level for all events. There were no treatment-related deaths.
Four of the 13 patients who discontinued the study did not have grade 3 or 4 AEs. Indeed, three patients had grade 2 colitis associated with (1) either contraindication to corticosteroids because of uncontrolled diabetes mellitus, or (2) complete remission after four cycles of ipilimumab leading to regular follow-up without maintenance ipilimumab. One patient had a grade 2 asthenia after four cycles of ipilimumab, leading to regular follow-up without maintenance ipilimumab.
Dose escalation and DLTs
Eighteen patients were evaluable for DLTs in this study (12 patients in the cohort treated with 9 Gy and 6 patients in the cohort treated with 15 Gy). Among them, four patients experienced DLTs. All the DLTs occurred outside the radiation field.
In the cohort treated with 9 Gy, 2 of 12 evaluable patients experienced DLTs after two cycles of ipilimumab combined with radiotherapy. Indeed, one of these patients presented grade 3 hepatitis, and the other one presented grade 3 colitis with grade 3 hypokalemia, grade 3 anorexia and grade 3 thyroid disorders. In both patients, the three fractions of radiotherapy (on Monday, Wednesday and Friday) were delivered on week 4. DLTs led to permanent ipilimumab discontinuation in both patients.
In the cohort treated with 15 Gy, two of the six evaluable patients experienced a DLT after two and three cycles of ipilimumab, respectively, combined with radiotherapy. One of these patients presented grade 3 hepatitis, and the other one presented grade 3 colitis with unusually normal macroscopic colonoscopy but a total villous atrophy mimicking celiac disease on biopsies. In both patients, the 3 radiotherapy fractions (on Monday, Wednesday and Friday) were delivered on week 4. DLTs led to permanent ipilimumab discontinuation in both patients.
The MTD of radiotherapy was thus 9 Gy when combined with ipilimumab 10 mg/kg in the present design. Consequently, the RPTD of radiotherapy administered in combination with ipilimumab at 10 mg/kg in patients with metastatic melanoma was 9 Gy.
Clinical outcomes
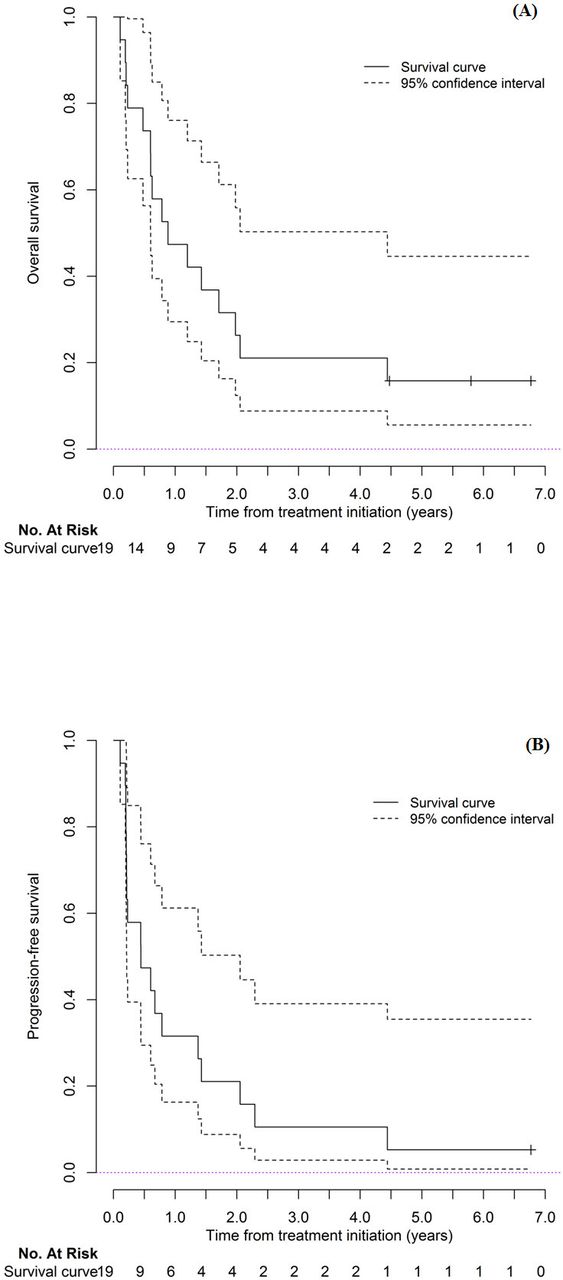
At the time of analysis, the median duration of follow-up was 5.8 years (Q1=4.5; Q3=6.8). The median overall survival (95% CI) was estimated at 0.9 years (0.5–2). The median PFS (95% CI) was 0.4 (0.2–1.4). Figure 1 shows Kaplan-Meier median overall survival and PFS curves with 95% CI. According to irRC, the best response within the trial was CR for two patients (both in the cohort receiving 9 Gy), PR for three patients (two patients in the cohort receiving 9 Gy and one patient in the cohort receiving 15 Gy) and SD for seven patients (six patients in the cohort receiving 9 Gy and one patient in the cohort receiving 15 Gy), giving an ORR of 31% and a clinical benefit rate of 75% at week 24 (online supplementary table S2). The initial melanoma staging of the patients who had CR was M1a for one patient (multiple subcutaneous nodules) and M1c (multiple subcutaneous nodules and lymph nodes associated with an elevated LDH) for the other patient. The initial melanoma staging of the patients who had PR was M1a for one patient (multiple subcutaneous nodules) and M1c for two patients (one of these patients had a subcutaneous nodule, a lymph node and elevated LDH). The other patient had multiple lymph nodes and bone metastasis).

Kaplan-Meier median overall survival (A) and progression-free survival (B) curves with 95% CI.
No pseudoprogression was observed among the patients treated in this study, nor radiation-induced necrosis or edema. Of note, three patients were not evaluable for response because they progressed and died before the radiologic assessment scheduled in this study.
Treatments administered after the ‘Mel Ipi Rx’ study in patients with disease progression are summarized in online supplementary figure S3.
Supplemental material
Variation of tumor growth rate across lesions
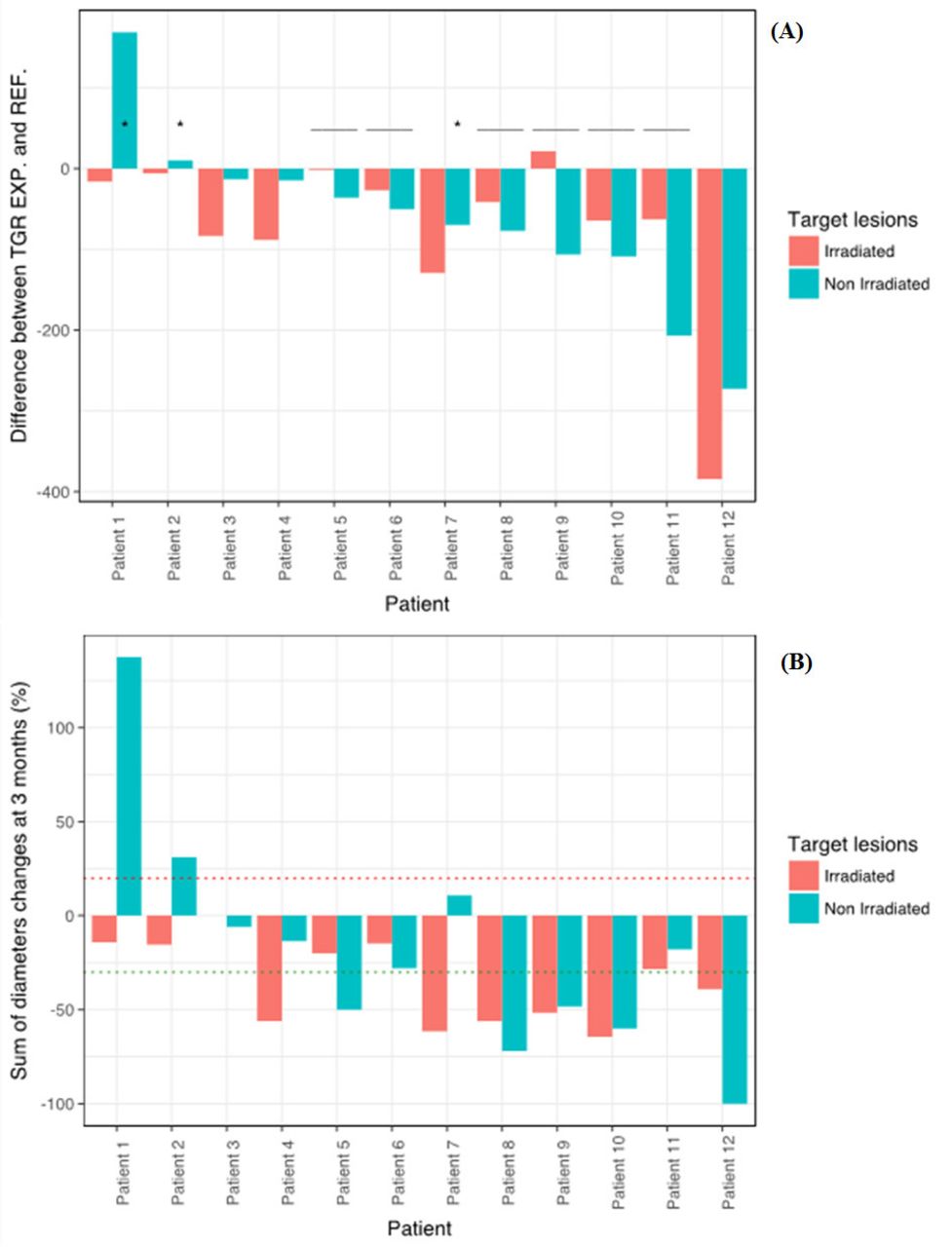
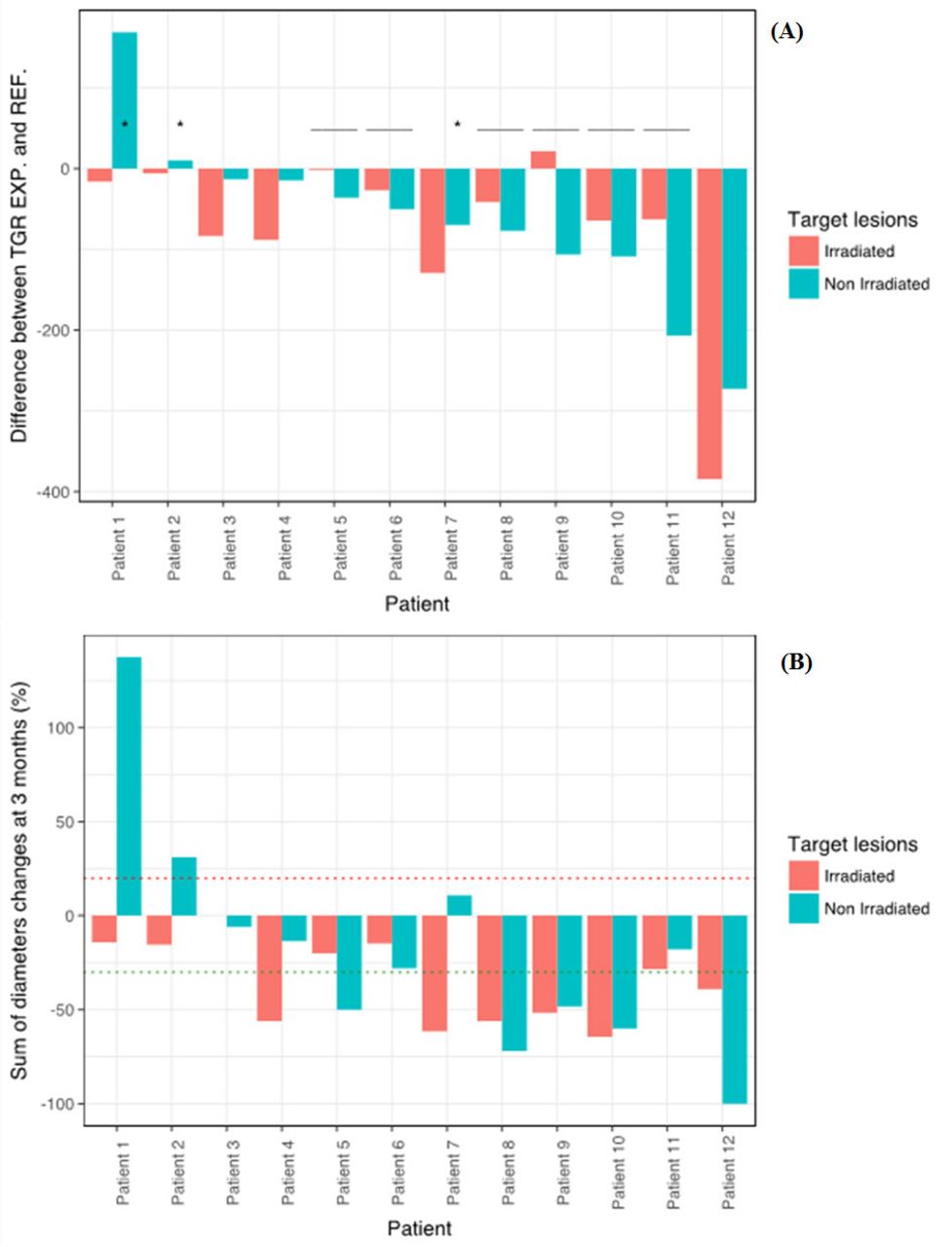
TGR variation for irradiated and non-irradiated lesions before and after the treatment was evaluable for 12 patients (figure 2). A total of 24 non-irradiated lesions with up to 5 lesions for one patient were evaluated for the REF and EXP-TGRnon-irr (median 2 (IQR 1–3) non-irradiated lesions by patient), and 13 irradiated lesions for the REF and EXP-TGRirr (one patient had two irradiated lesions). Median reference and experimental period were 1.23 (IQR 0.90–1.65 and 2.96 (IQR 2.91–3.20) months, respectively. The sum of diameters of lesions at the three evaluation times (prebaseline, baseline, first evaluation) and corresponding TGR are presented in table 3. The EXP-TGR (on treatment) was not correlated with the REF-TGR (before treatment) (Spearman’s rho=0.11, p=0.73). Decrease of the TGR was −60.03% of the tumor size/months (IQR –106.76 to –14.14) for irradiated lesions and −52.16 %/month (IQR –84.54 to –13.62) for non-irradiated lesions, although the difference was not significantly different (p=0.82). Response of non-irradiated lesions seemed more representative of patient outcomes (vs irradiated lesion): EXP-TGRnon-irr was significantly higher in patients with PD. Although the number of patients was too low for statistical test, p values are shown for information in table 4, figure 2 and online supplementary figure S4.
Supplemental material
{kind=link}
{kind=link}
(A) Waterfall plot of patients according to the variation of tumor growth rate (ΔTGR) between reference (before treatment) and experimental period (on treatment). For each patient, specific ΔTGR of irradiated and non-irradiated lesions are represented. *ΔTGR on treatment >0: lesions at the first evaluation are bigger than at baseline. ΔTGR of non-irradiated lesions was superior to the irradiated lesion. (B) Changes of the sum of diameters of the target lesions (irradiated and non-irradiated, respectively) at 3 months (in %) compared with the baseline.
Characteristics of lesions evaluated for tumor growth rate (TGR)
Univariate analysis of tumor growth rate (TGR)
Immune analyses
We analyzed immune parameters in the blood that have been previously described to be changed during ipilimumab treatment to determine if radiotherapy could modify ipilimumab pharmacodynamics.19 20 For CD4+ T cell counts and as expected, ipilimumab alone (W4) could favor accumulation of TEM, Treg and ICOS+CD4+ T cells. Interestingly, at W6 (after ipilimumab+radiotherapy), only TEM and ICOS+CD4+ T cells remained significantly increased, suggesting that combination favored accumulation of activated memory CD4+ T cells rather than Treg cells. For CD8+ T cell counts, no accumulation could be observed at W4, while augmentation of TCM and TEMRA could be depicted between W4 and W6, suggesting that adjunction of radiotherapy to ipilimumab was more prone to boost these CD8+ T populations (online supplementary figure S2). High fold change in CD8 from baseline to week 4 was significantly correlated with PFS (p=0.0223), but not significantly correlated with overall survival (p=0.2355) (online supplementary figure S5).
Supplemental material
Innate immune cells and NLR (absolute neutrophils count (ANC) divided by the number of lymphocytes) or dNLR (ANC divided by (the number of white blood cells−ANC)) have been shown to have a prognostic role in patients treated with immunotherapy and even might represent a predictive biomarker of response. We took advantage of standard blood tests to determine if neutrophils, monocytes, NLR or dNLR at baseline, W4 and W6 could correlate with the prognosis in our study. ANC or monocytes did not correlate with the prognosis of patients while absolute count of lymphocytes significantly increased at W6 compared with baseline in only patients with a clinical benefit (CR+PR+SD). Both NLR and dNLR were significantly lower at W6 only in patients with clinical benefit (online supplementary figure S6). Note that we did not found an association with the dose of radiotherapy (data not shown).
Supplemental material
Supplemental material
Discussion
In this dose escalation phase 1 study, four patients experienced DLTs. All the DLTs occurred outside the radiation field. Therefore, it was difficult to assess the role of concurrent radiotherapy on the DLTs. The MTD of radiotherapy combined with ipilimumab at 10 mg/kg was 9 Gy. The RPTD of radiotherapy administered in combination with ipilimumab at 10 mg/kg in patients with metastatic melanoma was 9 Gy. A hypofractionated radiation regimen (higher doses per fraction) was used in this study. It is usually preferred for melanoma which displays low alpha/beta ratio. Our three fractions hypofractionated regimen is in line with the radiation standard in the metastatic setting. Moreover, it has been shown recently that radiation doses per session inferior to 10 Gy combine more favorably with immunotherapy through interferon type 1 induction.21 Of note, our study is the only one that combines radiotherapy and high dose of ipilimumab 10 mg/kg.
The incidence of treatment-related AEs was high with this combination in our study but numerically similar to the incidence reported previously with ipilimumab monotherapy at 10 mg/kg. Grade 3 or 4 AEs occurred in 42% of patients in our study, whereas they occurred in 47%–55% of patients treated with ipilimumab monotherapy at 10 mg/kg.2 22 23 The overall AE spectrum of the combination in this study was consistent with previous findings with the drug’s immune-based mechanism of action. The high rate of AEs might be partially attributed to the high dose of ipilimumab. The dose of 10 mg/kg was chosen based on data from the randomized phase 2 trial that compared various doses of ipilimumab in patients with advanced melanoma, showing the best results with 10 mg/kg. This dose is substantially higher than the approved dose of 3 mg/kg for the treatment of patients with advanced melanoma. However, a recent publication that evaluated 3 mg/kg vs 10 mg/kg demonstrates a higher efficacy of the 10 mg/kg dose, although more toxic.24 25 Toxicity was not observed specifically in the region that was irradiated, suggesting that the combination of ipilimumab to radiotherapy does not affect tolerance to each of those modalities for the range of doses and schedules evaluated in the present study.
Although the treatment landscape of advanced melanoma has changed with the implementation of pembrolizumab, nivolumab, ipilimumab plus nivolumab and targeted therapies, this combination of ipilimumab plus radiotherapy may have a clinical utility in refractory patients or patients with unmet medical needs. This combination appeared to be associated with a higher antitumor activity compared with ipilimumab monotherapy, as illustrated by the high control rate of irradiated metastases and responses in non-irradiated metastases. This higher antitumor activity was observed despite the fact that the delivered doses of radiotherapy were low, suggesting synergetic activity of ipilimumab combined with radiotherapy. The ORR (31%) was numerically higher than the 11% response rate of ipilimumab monotherapy at 10 mg/kg reported in the phase 2, dose-ranging study in patients with pretreated advanced melanoma.2 The clinical benefit was also numerically higher (75%) than the 50% reported in the prospective clinical study combining radiotherapy with ipilimumab at 3 mg/kg.11 Of note, the range of radiotherapy doses that we used 9 and 12 Gy total dose are not likely to induce a major tumor response in melanoma underscoring the fact that the response of both the non-irradiated and the irradiated lesions might reflect a favorable interaction between ipilimumab and radiotherapy. However, it is inherently difficult to compare efficacy of the combination therapy with ipilimumab monotherapy as the study design, number of patients included and patient demographics differ among studies. We evaluated the interest of the TGR to estimate the specific effect of the irradiation by assessing the evolution (growth rate) of the irradiated lesion compared with a group of non-irradiated target lesions for the same patient. While the number of patient was too low to be able to draw conclusion due to the lack of power, it was interesting to see that the variation of TGR of non-irradiated lesions after treatment could be more important than for irradiated lesion (ΔTGRnon-irr deeper than ΔTGRirr), despite the direct additive effect of radiotherapy. This may be related to the synergistic effect of radiation and immunotherapy on non-irradiated lesions (abscopal effect), although it could also be related to a transitory edema-related increase size of the irradiated lesion following stereotactic radiotherapy which could have reduce the ΔTGRirr.26 27
Ipilimumab combined to radiotherapy was able to clearly increase CD4+ and CD8+ICOS+ T cells. These results are aligned with previous studies where ICOS induction on CD4+ T cells during the course of ipilimumab treatment has been proposed as a biomarker of ipilimumab efficacy in patients with cancer.28–30 Moreover, a statistically significant association was reported between a high fold change in CD8 from baseline to week 4 and PFS, and a positive trend in terms of overall survival was reported in patients with a high fold change in CD8 from baseline to week 6.
Systemic inflammatory status has been closely correlated with worse prognosis; NLR and dNLR are known prognostic factors in patients with cancer. The dNLR might be more relevant since it includes monocytes and other granulocyte subpopulations. High dNLR has been associated with shorter survival in patients with several tumor types, including melanoma. In melanoma, dNLR of 3 or greater had an independent negative effect on survival in patients treated with ipilimumab.30 31 In our study, it seems that adjunction of radiotherapy to ipilimumab enhanced the decrease of dNLR as well as NLR only in responding patients. Thus, normalization of the inflammatory status of patients might be an important feature to achieve clinical response when treated with ipilimumab.
These complementary analyses regarding immune parameters are of interest but have limitations due to the low number of patients and should be confirmed in larger cohort in the future since no multivariate analysis could be performed.
Conclusions
Our data suggest that a subset of patients may benefit from combination therapy and that immune response biomarkers may be useful for early evaluation of response to therapy. These results are aligned with recent data reported in metastatic non-small-cell lung cancer, where radiotherapy combined with CTLA-4 blockade induced systemic antitumor T cells, with significant ORR (18%) and disease control (31%), suggesting abscopal response.32 These results highlight the importance of continued clinical investigations to assess the response of radiotherapy combined with immunotherapy and also pave the way for non-ablative radiotherapy doses in combination with immunotherapy.
Supplemental material
References
Footnotes
CR and ED contributed equally.
Contributors CR, ED and CB designed the study, contributed to the data analysis and interpretation, and wrote, edited and reviewed the manuscript. NC-G and LC designed and performed immune analysis, and analyzed the data. SR, CB, EL, AL and DS collected and analyzed the clinical data. ED, RS and AL designed and performed tumor growth rate analysis. All authors read and approved the final manuscript.
Funding This study was funded by Gustave Roussy Cancer Campus, SIRIC SOCRATE (INCa DGOS INSERM 6043), SIRIC SOCRATE 2.0 (INCa-DGOS-INSERM_12551).
Competing interests CB has acted as a board advisor for BMS, has been a speaker for Merck and has received travel fees from Amgen and Pfizer. NC-G has received research grants from Cytune Pharma, GSK and Sanofi. She has acted as a board advisor for AstraZeneca and has been a speaker for Sanofi and AstraZeneca. CM has acted as consultant of BMS and Merck. ER has acted as a consultant for BMS, Novartis and Roche, and has received travel fees from BMS and Novartis. RS has received travel fees from AstraZeneca. CM has acted as a consultant from Amgen, Astellas, Astra Zeneca, Bayer, BeiGene, BMS, Celgene, Debiopharm, Genentech, Ipsen, Janssen, Lilly, MedImmune, MSD, Novartis, Pfizer, Roche, Sanofi and Orion. He is the principal or subinvestigator of clinical trials for Abbvie, Aduro, Agios, Amgen, Argen-x, Astex, AstraZeneca, Aveopharmaceuticals, Bayer, Beigene, Blueprint, BMS, BoeringerIngelheim, Celgene, Chugai, Clovis, DaiichiSankyo, Debiopharm, Eisai, Eos, Exelixis, Forma, Gamamabs, Genentech, Gortec, GSK, H3 biomedecine, Incyte, InnatePharma, Janssen, Kura Oncology, Kyowa, Lilly, Loxo, Lysarc, LytixBiopharma, Medimmune, Menarini, Merus, MSD, Nanobiotix, NektarTherapeutics, Novartis, Octimet, Oncoethix, OncopeptidesAB, Orion, Pfizer, Pharmamar, Pierre Fabre, Roche, Sanofi, Servier, Sierra Oncology, Taiho, Takeda, Tesaro and Xencor. J-CS has received consultancy fees from AstraZeneca, Astex, Clovis, GSK, GamaMabs, Lilly, MSD, Mission Therapeutics, Merus, Pfizer, PharmaMar, Pierre Fabre, Roche/Genentech, Sanofi, Servier, Symphogen and Takeda. He has been a full-time employee of MedImmune since September 2017. He is a shareholder of AstraZeneca and Gritstone. CR has acted as a consultant of Amgen, BMS, GSK, Merck, Novartis and Roche. ED has received research grants from Roche, Servier, AstraZeneca, Merck Serono, BMS, MSD, Amgen, Accuray and Boerhinger. He has received personal fees from Roche, AstraZeneca, Merck Serono, Amgen, Accuray and Boerhinger.
Patient consent for publication Not required.
Ethics approval The protocol was approved by the relevant institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. All data relevant to the study are included in the article or uploaded as supplementary information. The data generated by our present research may be made openly and publicly available upon publication of our article. Where it is not possible or viable to make data openly available (due to confidentiality or sensitivity issues), they should be shared through a controlled access repository.