Article Text

Abstract
Background Immune checkpoint inhibitors (ICIs) have transformed treatment for melanoma, but identifying reliable biomarkers of response and effective modifiable lifestyle factors has been challenging. Obesity has been correlated with improved responses to ICI, although the association of body composition measures (muscle, fat, etc) with outcomes remains unknown.
Methods We performed body composition analysis using Slice-o-matic software on pretreatment CT scans to quantify skeletal muscle index (SMI=skeletal muscle area/height2), skeletal muscle density (SMD), skeletal muscle gauge (SMG=SMI × SMD), and total adipose tissue index (TATI=subcutaneous adipose tissue area + visceral adipose tissue area/height2) of each patient at the third lumbar vertebrae. We then correlated these measures to response, progression-free survival (PFS), overall survival (OS), and toxicity.
Results Among 287 patients treated with ICI, body mass index was not associated with clinical benefit or toxicity. In univariable analyses, patients with sarcopenic obesity had inferior PFS (HR 1.4, p=0.04). On multivariable analyses, high TATI was associated with inferior PFS (HR 1.7, p=0.04), which was particularly strong in women (HR 2.1, p=0.03). Patients with intermediate TATI and high SMG had the best outcomes, whereas those with low SMG/high TATI had inferior PFS and OS (p=0.02 for both PFS and OS).
Conclusions Body composition analysis identified several features that correlated with improved clinical outcomes, although the associations were modest. As with other studies, we identified sex-specific associations that warrant further study.
- CTLA-4 antigen
- immunotherapy
- biomarkers, tumor
- melanoma
- tumor biomarkers
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Immune checkpoint inhibitors (ICIs) have revolutionized metastatic melanoma treatment over the past decade, leading to increased durable responses and long-term survival rates compared with historical benchmarks.1 2 Given the success of ICI, intensive research efforts are now focused on determining which patients are most likely to respond to treatment and on identifying modifiable patient factors associated with therapeutic benefit.
Recently, several studies have found an association between obesity and response to ICI. One study observed improved OS and PFS among obese patients with metastatic melanoma treated with immunotherapy compared with patients with a normal body mass index (BMI).3 Of note, in this study, survival outcomes were sex-specific with significant associations observed only among male patients. Several other groups have published similar findings, although the relationship appears to be complex, and some studies have failed to report an association.4–6 For example, Donnelly et al examined the relationship between BMI and survival outcomes among 423 patients with metastatic melanoma and did not find any significant associations.7 Additionally, the mechanism of the association between BMI and response to ICIs is not well understood, although obesity may promote leptin-mediated T cell dysfunction which is reversed by Programmed cell death protein1 (PD-1)/Programmed death-ligand1 (PD-L1) blockade.6
BMI is a crude surrogate for more specific measures of body composition (ie, skeletal muscle and adipose tissue).8 Accordingly, the association of muscle quantity and quality, as well as fat distribution (eg, visceral vs subcutaneous) with ICI outcomes among patients with metastatic melanoma has not been well-characterized beyond two small studies.9 10 Thus, we examined the relationship between body composition and clinical outcomes in a large cohort of patients with metastatic melanoma treated with ICI, including the impact of sarcopenia, obesity, and muscle/fat composition and distribution.
Methods
Patient population
After obtaining institutional review board approval, the electronic medical record was reviewed to identify 349 consecutive patients with advanced melanoma treated with ICI (either anti-PD-1/PD-L1 monotherapy or combination ipilimumab and nivolumab) at Vanderbilt University Medical Center from October 2009 through October 2018. Of these, 290 patients had pretreatment scans available for analysis (defined as CT or positron emission tomography-computed tomography (PET-CT) obtained within 6 months of treatment start). After exclusion of three scans for excess artifact, a total of 287 patients were included. Chart review was performed to assess immune-related adverse events related to treatment as defined by Common Terminology Criteria for Adverse Events Version 4.03. Response, progression-free survival (PFS) and overall survival (OS) were investigator determined based on review of electronic medical records. Objective response was defined by RECIST V.1.1. PFS was defined as time of treatment start to progression by RECIST V.1.1, and OS was defined as time of treatment start to death or last follow-up.
Automatic segmentation
Pretreatment scans (either non-contrasted CT images from PET-CT scans or CT images) were analyzed using Slice-o-matic (Tomovision V.5.0) and ABACS (automated body composition analyzer using CT) software according to previously established methods (figure 1).11 Briefly, patient scans were viewed using AGFA IMPAX software (V.6.6.1.3525) and the L3 level was identified by study personnel. Axial, cross-sectional images at the L3 level were then uploaded to Slice-o-matic and automatically segmented into muscle tissue, subcutaneous adipose tissue (SAT) and visceral adipose tissue (VAT) using ABACS automatic segmentation software. This software identifies muscle tissue as tissue with a radiodensity between −29 and +150 Houndsfield units (HU). Given the radiodensity of organs also falls within this range, the software incorporates knowledge of L3 muscle shape to avoid erroneously labeling organs as muscle tissue.12 Once muscle tissue was identified, SAT was defined as tissue lying outside the border of the defined muscle area with a radiodensity between −190 and −30 HU and VAT was tissue lying inside the border of the defined muscle area with a radiodensity between −150 and −50 HU. This software has been previously validated through comparison with manual segmentation and was found to have excellent concordance.11
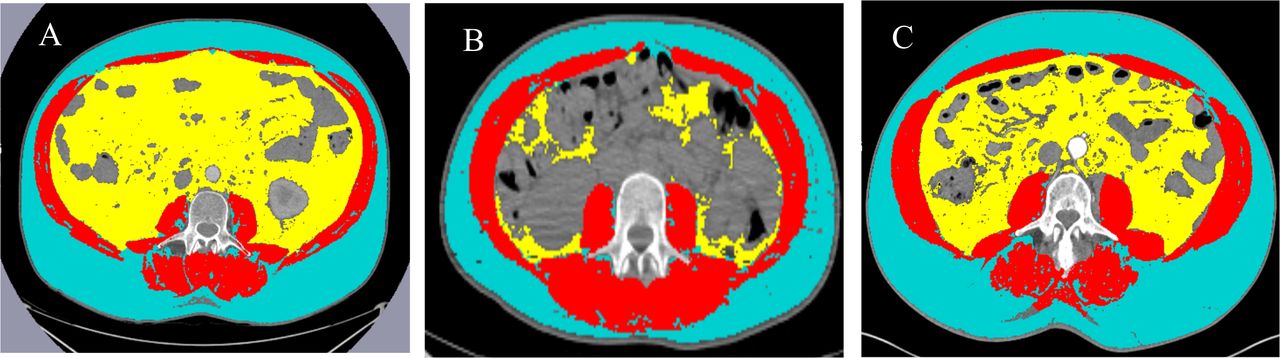
Representative segmentation results. Yellow = VAT, Blue = SAT, Red = muscle. (A) Representative low SMG/high TATI. (B) Representative high SMG/low TATI. (C) Representative high SMG/high TATI. SAT, subcutaneous adipose tissue; SMG, skeletal muscle gauge; TATI, total adipose tissue index; VAT, visceral adipose tissue.
Measures of body composition
Skeletal muscle index (SMI) was used to normalize muscle area for height and was calculated as follows: (skeletal muscle area (cm2))/(height (m2)). Sarcopenia was defined according to Martin et al.13 For patients with BMI <25, sarcopenia was defined as SMI <43 cm/m2 for men and <41 cm/m2 for women and for BMI ≥26, sarcopenia was defined as <53 cm/m2 for men and <41 cm/m2 for women. Sarcopenic obese was defined as patients who met above criteria for sarcopenia with BMI ≥30. Skeletal muscle density (SMD) is a measure of muscle attenuation and was determined by Slice-o-matic software by taking the average HU of muscle present at the L3 level. SMD is known to be inversely related to myosteatosis and has also been shown to be associated with survival among patients with cancer in several studies.13–16 Low SMD was defined according to previously established cut-offs by Martin and colleagues.13 For patients with BMI <20 to 24.9, low SMD was defined as <41 HU. For patients with BMI >25, low SMD was defined as <33 HU. Of note, there are multiple definitions of SMD in the literature. We chose the Martin et al definition because it was the first pivotal study to address SMD in oncology and it is the most commonly employed in the literature.17 Total adipose tissue index (TATI) was used to normalize adipose tissue for height and was calculated as follows: (subcutaneous adipose tissue area (cm2) +visceral adipose tissue area (cm2))/(height (m2)). We used tertiles to categorize TATI because there is no clinically established threshold for TATI and we felt that tertiles would be the most appropriate way to categorize a continuous variable without an established threshold. Skeletal muscle gauge (SMG) incorporates both muscle area and muscle density and has strongly correlated with patient outcomes including toxicity and functional status among patients with breast cancer treated with chemotherapy.18–20 SMG was calculated as follows: (SMI cm2/m2)×(skeletal muscle density in HU). Patients were divided into high and low SMG groups based on previously established cut-offs by Shachar et al (SMG cut-off 1475).19 VAT index and SAT index were calculated as follows: (visceral adipose tissue area (in cm2)/(height (m2)) for VAT index and (subcutaneous adipose tissue (in cm2)/(height (in m2)) for SAT index.
Body mass index
BMI was calculated as weight (kg) divided by height (m2). Patients were subdivided according to their pretreatment BMI. Only three patients were underweight with pretreatment BMI<18.5, thus underweight and normal categories were combined; hereafter referred to as ‘Normal’. BMI categories were established based on Centers for Disease Control (CDC) definitions: Normal = <25, overweight = ≥25 to <30, and obese = ≥30.21 Classes of obesity were also defined according to CDC definitions as follows: Class I: BMI 30 to <35, Class II: 35 to <40, and Class III: >40.21
Statistical methods
Continuous variables were compared between groups using t-test or non-parametric Mann-Whitney U test. Categorical variables were compared using χ2 test. PFS and OS were assessed using the Kaplan-Meier method and compared between groups using the log-rank test. Multivariable Cox regression models were developed to estimate patient survival in association with TATI and SMG, as well as their interaction term, adjusted for covariates including age, sex, stage, and prior therapy. Regarding the SMG:TATI interaction term, we thought that patients with high skeletal muscle and high adipose tissue would behave differently than those with low skeletal muscle and high adipose tissue and thus we included an interaction term to allow the estimated effect of SMG to differ at different TATI levels. The interaction term was significant for response (pinteraction=0.0499) but not statistically significant for PFS and OS (pinteraction >0.1). Given the study sample size as well as the number of OS/PFS events, we were able to afford to include the interaction term along with other specified covariates in the multivariable analyses without causing overfitting concerns. Of note, the effect of SMG on PFS appeared to be lower for patients in the highest TATI tertile compared with patients in the lowest tertile, independent of age and gender (adjusted HR=0.55, p=0.08). Age appeared to have a non-linear relationship with survival outcomes and therefore was fitted using restricted cubic splines with three knots. A sex-stratified analysis was performed to assess for body composition differences that are sex-specific. All statistical analyses were performed using R V.3.6.0.
Results
Patient characteristics
There were 287 patients with metastatic melanoma included (see table 1 and online supplementary table 1). Median follow-up time was 519 days. A total of 136 patients were alive at last follow-up. The median age was 63 and most (64.1%) patients were male. Most patients had stage IV M1c or M1d disease (51.9%) and had received prior treatment (53.3%). Pembrolizumab was the most common ICI (64.8%) followed by combination ipilimumab and nivolumab (21.6%). The median BMI was 28.9, slightly higher than the national average (26.6 for men and 26.5 for women).22 Over half (53.7%) of patients were sarcopenic at baseline.
Supplemental material
Patient baseline characteristics (n=287)
Associations with BMI
We did not find any statistically significant associations between BMI and response, toxicities (any grade), PFS, or OS in univariable or multivariable analyses (table 2; online supplementary table 2). Next, we considered the possibility that sex differences were masking associations between BMI and outcomes by performing sex-stratified analysis (table 2). We found that this was not the case given that even in the sex-stratified analysis, we did not find any statistically significant associations between BMI and response, toxicities, PFS, or OS.
Supplemental material
Univariable and multivariable analysis examining response, toxicities, PFS, and OS in association with BMI (n=287)
Next, we sought to determine whether different classes of obesity were associated with any of the above outcomes (online supplementary table 3 and online supplementary figure 1). Although there were no statistically significant differences in response, toxicity, or PFS when examining different classes of obesity, there was a statistically significant difference in overall survival among patients with class III obesity compared with patients with class I obesity (HR 2.4, 95% CI 1.1 to 4.9, p value = 0.03).
Supplemental material
Supplemental material
Lastly, to determine if associations differed between the monotherapy and combination therapy cohorts, we fitted the same multivariable Cox regression models for response, PFS and OS for the combination therapy cohort and the monotherapy cohort separately (online supplementary table 4). There were no major differences between the individual cohorts and the pooled analysis. Again, there were no statistically significant associations between BMI and Response, PFS or OS.
Supplemental material
Correlation between BMI and body composition measures
Given BMI is often used as a surrogate for body composition, we next examined the correlation between BMI and various body composition measures. BMI was most strongly correlated with TATI (correlation coefficient 0.88; online supplementary table 5). The weakest correlation was between BMI and SMG (correlation coefficient 0.15).
Supplemental material
Association of body composition measures
Given the strong correlation of TATI and BMI, we first assessed whether TATI correlated with clinical outcomes. In the univariable analyses (table 3 and online supplementary table 2), we did not find any statistically significant associations between TATI (assessed by tertiles) and response, toxicities, PFS or OS. Patients with sarcopenic obesity had inferior PFS (HR 1.47, 95% CI 1.02 to 2.12, p=0.037), although there were no differences in response or OS.
Univariable analyses examining response, toxicities, PFS and OS in association with body composition measures (n=287)
Multivariable analysis
In multivariable analyses (table 4) adjusted for age, sex, SMG:TATI interaction, stage and prior therapy, there were no differences in response, PFS or OS among patients with high SMG versus low SMG. Although there was no difference in response among different TATI tertiles when examining the total cohort, when stratified by sex, females in the highest TATI tertile were significantly less likely to respond to ICI compared with females in the lowest TATI tertile (OR 0.18, 95% CI 0.04 to 0.76, p=0.02). This difference was not seen among males. Additionally, multivariable analyses showed that patients in the highest TATI tertile were more likely to experience progression (HR PFS 1.71, 95% CI 1.01 to 2.87, p=0.04) than those in the lowest tertile. In the sex-stratified analysis, this association was even stronger among women (HR PFS 2.06, 95% CI 1.06 to 3.98, p=0.032) but did not persist among men (HR PFS 1.40, 95% CI 0.59 to 3.31, p=0.45). There was, however, no statistically significant difference in OS between patients with high and low TATI in the total cohort or when stratified by sex.
Multivariable and sex-stratified analysis examining body composition measures and response, PFS and OS
We next sought to determine if associations differed between the monotherapy and the combination therapy cohorts. We fitted the same multivariable Cox regression models for response, PFS and OS for the combination therapy cohort and the monotherapy cohort separately (online supplementary table 6). The associations in the monotherapy cohort were consistent with the results of the pooled analysis. There were no statistically significant associations in the combination therapy cohort which may be due to limited power as a result of the small number of patients in this group (n=62).
Supplemental material
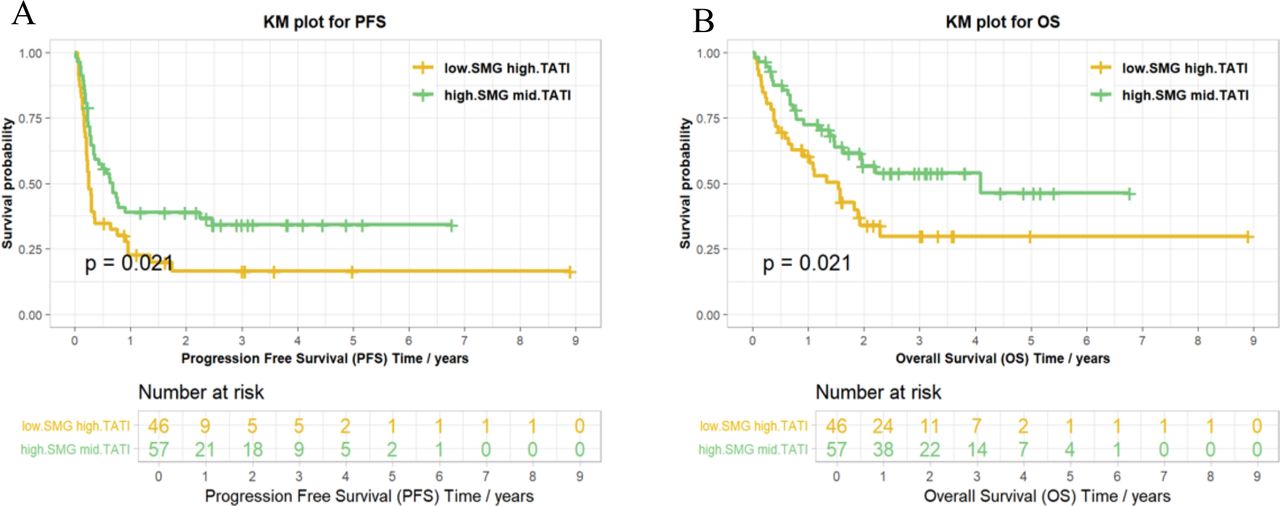
To further investigate the relationship between SMG and TATI, we assessed different combinations of SMG and TATI. Although within the full group, outcomes were not statistically different. when comparing cohorts with the poorest outcomes (low SMG:high TATI) to those with the best outcomes (high SMG:mid TATI), there was a significant difference in both PFS and OS with patients in the low SMG:high TATI group having significantly worse outcomes (p=0.02 and 0.02 respectively, figure 2).

{kind=link}
{kind=link}
Kaplan-Meier curves for PFS and OS for various combinations of SMG:TATI. OS, overall survival; PFS, progression-free survival SMG, skeletal muscle gauge; TATI, total adipose tissue index.
Given the inverse relationship between TATI and response, we were interested in whether one adipose tissue compartment was primarily driving this association. Thus, we assessed SAT and VAT in relation to response, PFS and OS (online supplementary table 7). We found that there were no statistically significant differences among patients with low versus high SAT or low versus high VAT with regard to these outcomes.
Supplemental material
Discussion
To our knowledge, this is the largest study examining the association between body composition measures and outcomes in patients with metastatic melanoma receiving ICI. In this study, we found that high TATI was associated with decreased response rate and PFS among women. Interestingly, this association was only significant in multivariable analysis when accounting for the interaction between SMG and TATI. This suggests that patients with higher muscle (higher SMI and SMG—a metric which incorporates muscle size and density) and low or intermediate fat content seem to have better outcomes than those with high fat/low muscle. These findings are in agreement with other studies which have found that sarcopenic obesity is more closely associated with outcomes than obesity alone across other cancer settings.23 However, the results observed in our study were only of modest clinical and/or statistical significance, and are thus of doubtful utility as biomarkers.
Several preclinical studies have linked adipose tissue with increased rate of tumor progression. One study found that melanoma tumors (both in vivo and in vitro) that were surrounded by adipocytes had increased progression and invasion in part due to direct lipid transport from adipocytes to tumor cells with a concomitant decrease in tumor cell de novo lipogenesis.24 Furthermore, a number of studies across cancer types have demonstrated poor outcomes associated with adiposity, particularly with sarcopenic obesity outside the context of immune therapy (eg, cancer surgery or chemotherapy).25–27
Within the context of cancer immunotherapy, one study showed that obesity/adiposity could actually have favorable effects.6 Increased markers of exhaustion were found in tumor-infiltrating lymphocytes from diet-induced obese (DIO) mice which was in part regulated by leptin signaling. Increased T cell exhaustion led to increased tumor progression among DIO mice compared with control mice. When given anti-PD-1 therapy, tumors in DIO mice returned to progression rates similar to the control mice, suggesting that immunotherapy has the ability to reverse T cell exhaustion in obese mice. These data support the concept that obesity may drive T cell exhaustion and more aggressive tumor biology which, when reversed by ICI, levels the playing field.
In this study, we did not find any statistically significant associations between baseline BMI and response to ICI. We did find a significant association between OS and Class III obesity (BMI >40, HR 2.4, 95% CI 1.1 to 4.9, p value = 0.03). Given there was no statistically significant difference in response or PFS, we hypothesize that this is likely due to overall poor health of these patients rather than an interaction between obesity and ICI. Thus far there have been mixed findings regarding BMI and response to ICI with several studies finding a positive association3–6 but not universally.7 There are several possible explanations for these inconsistencies. First, the effect of BMI may be small and sex-specific as demonstrated by several studies including our own. Second, the role of adipose tissue in cancer progression and response to ICI may be a dynamic one, with tumors in obese individuals being initially more vulnerable to ICI but ultimately associated with irreversible T cell exhaustion and worse outcomes. Thus, it might be possible to capture different associations between BMI and response at different clinical time points. Lastly, given the complex relationship between adipose tissue and both tumor and immune cells, it is likely that there are a host of underlying factors that require continued collaboration between basic and clinical scientists.
There were several limitations to this study. We did not take into account tumor characteristics, including tumor mutational burden and PD-L1 expression. Additionally, the study was performed at a single center in the Southeastern USA, a region with relatively high rates of obesity, and possibly other region-specific biases. Most patients in the study were either overweight or obese (76.3%) slightly higher than national rates (71.6%), but fairly representative for the region.28 Subset analyses produced small numbers in some groups, thus potentially obscuring modest associations. However, the labor-intensive nature of these study procedures would make dramatically increasing the sample size challenging. Patients who did not have pretreatment scans or whose scans were unanalyzable were not included in the study which could introduce selection bias. Patients’ pretreatment scans were obtained within 6 months of treatment start and it is possible that body composition changed in the months prior to treatment particularly in the setting of advanced cancer. The majority of patient scans, however, were obtained within 1 month prior to treatment start (228 out of 287 patient scans) and only 12 scans were obtained greater than 2 months prior to treatment start making significant changes in body composition that would affect the results of the present study less likely.
In conclusion, we did not observe associations with outcomes and BMI in this study but did identify trends toward worse outcomes in patients with higher adiposity and lower muscle quantity and quality. These trends were of modest clinical and statistical significance, despite a fairly large sample size. Given these findings, we conclude that although body composition may have some value in predicting response to ICIs, it will likely not play a major role in clinical decision-making. Additional clinical and translational studies are needed to elucidate the effects of body composition and other host factors on the antitumor immune response.
References
Footnotes
Twitter @YoungArissa
Contributors AY and HQ collected patient data and performed segmentation using Slice-o-matic/ABACs software. AY was also a major contributor in writing the manuscript. HS and FY performed statistical analyses. EJD and JJM made edits and revisions to the manuscript. GW contributed expertise in body composition measures and offered guidance on use of Slice-o-matic/ABACS software. DBJ designed the study and was a major contributor to the manuscript. All authors read and approved the final manuscript.
Funding DBJ receives funding from the NCI/NIH grant numbers K23 CA204726 and R01 CA227481. AY receives funding from the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number R38 HL143619. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. GW receives funding from the NCI/NIH grant number K08 CA234225-01. JJM is supported by the National Heart, Lung and Blood Institute of the National Institutes of Health under award number R01 HL141466.
Competing interests DBJ serves on advisory boards for Array Biopharma, BMS, Incyte, Merck, and Novartis, and receives grant support from BMS and Incyte outside the scope of this study. JM serves on advisory boards for Novartis, BMS, Pfizer, Takeda, AstraZeneca, Nektar and Regeneron. EJD receives research funding from BMS, Incyte, Karyopharm, Genentech and Five Prime. GRW works as a consultant for Carevive Systems. A portion of this manuscript was presented at the American Society of Clinical Oncology Annual Meeting 2019.
Patient consent for publication Not required.
Ethics approval This study was approved by the Institutional Review Board of Vanderbilt University Medical Center (IRB# 150625). The IRB waived the requirement to obtain informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Deidentified patient data are available upon reasonable request. Please contact Douglas Johnson, 2220 Pierce Ave, 777 PRB, Nashville TN 37232, douglas.b.johnson@vumc.org.