Article Text

Abstract
Background Immune checkpoint inhibitors (ICIs) provide significant survival benefits in non-small cell lung cancer (NSCLC). Nevertheless, while some patients obtain a prolonged benefit, a non-negligible fraction of patients experiences an ultrarapid disease progression. Identifying specific molecular backgrounds predicting opposite outcomes is instrumental to optimize the use of these agents in clinical practice.
Methods We carried out an observational study with prospective design envisioning targeted next-generation sequencing (NGS) with an approved assay in 55 patients with metastatic NSCLC (Rome cohort), of whom 35 were treated with ICIs. Data from three clinically comparable datasets were collected and combined into a metadataset containing 779 patients. The datasets were related to the Memorial Sloan Kettering Cancer Center (MSKCC) cohort (tissue-based NGS) and the randomized phase II and III POPLAR and OAK trials (blood-based NGS).
Results In patients treated with ICIs in the Rome cohort, co-occurring mutations in NOTCH1-3 and homologous repair (HR) genes were associated with durable clinical benefit. Using the MSKCC/POPLAR/OAK metadaset, we confirmed the relationship between the NOTCHmut/HRmut signature and longer progression-free survival (PFS) in ICI-treated patients (multivariate Cox: HR 0.51, 95% CI 0.34 to 0.76, p=0.001). The NOTCHmut/HRmut genomic predictor was also associated with longer survival (log-rank p=0.008), despite patients whose tumors carried the NOTCHmut/HRmut signature had higher metastatic burden as compared with their negative counterpart. Finally, we observed that this genomic predictor was also associated with longer survival in patients with other tumor types treated with ICIs (n=1311, log-rank p=0.002).
Conclusions Co-occurring mutations in the NOTCH and HR pathways are associated with increased efficacy of immunotherapy in advanced NSCLC. This genomic predictor deserves further investigation to fully assess its potential in informing therapeutic decisions.
- immunotherapy
- lung neoplasms
- tumor biomarkers
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Immune checkpoint inhibitors (ICIs) represented a major therapeutic breakthrough in non-small cell lung cancer (NCSLC).1 2 However, the efficacy of ICIs is characterized by a remarkable interpatient heterogeneity, which is exemplified by two opposite patterns of disease evolution: durable clinical benefit (DCB) and hyperprogressive disease (HPD).3 4 Alterations in genome-safeguarding mechanisms, denoted by microsatellite instability (MSI), high tumor mutational burden (TMB) or POLE mutations, were proposed as biomarkers of ICI efficacy.5–9 Nevertheless, while MSI is uncommon in NSCLC, the usefulness of additional molecular predictors, particularly TMB, is still the focus of an intense debate.10 Indeed, genomic signatures predicting efficacy/inefficacy of ICIs are not exploitable in the routine clinical practice, despite the growing use of genomic tests, and the only predictive biomarker remains the immunohistochemical assessment of programmed death-ligand 1 (PD-L1).10 On this basis, in the present study we assessed the potential of pathway level analysis coupled with a co-occurrence/mutual exclusivity approach to identify genomic predictors of DCB in ICIs-treated patients with NSCLC.
Methods
Patients
In this observational study, prospective clinical sequencing was carried out in tissue samples from 55 patients with metastatic NSCLC treated at two oncological centers, of whom 35 had received an ICI in the routine clinical setting from January 2018 to November 2019. Patients were considered eligible if complete data on clinical features and treatment outcomes were available. Targeted DNA sequencing was performed with the FoundationOne CDx assay. The FoundationOne CDx assay detects mutations and copy number variations (CNVs) in 324 cancer-related genes, and selected rearrangements. The assay also provides information on MSI and TMB. Regarding TMB, it is reported with the following cut-offs: low (1–5 mutations/mb), intermediate (6–19 mutations/mb) and high (≥20 mutations/mb). Detailed information on the assay and the variant calling pipeline are available at https://www.rochefoundationmedicine.com/f1cdxtech. The immunohistochemical assessment of PD-L1 was performed in formalin-fixed paraffin-embedded tissues with the monoclonal mouse anti-PD-L1 antibody clone 22C3 (Dako). PD-L1 expression was evaluated in tumor cells and considered positive when expressed in ≥1% of neoplastic cells.
For external validation, we used three different and publicly available datasets. The Memorial Sloan Kettering Cancer Center (MSKCC) clinical sequencing cohort (tissue-based next-generation sequencing (tNGS)) was downloaded from cBioPortal (last accessed on the February 12, 2020).6 11 Data from blood-based NGS (bNGS) carried out in patients enrolled in the randomized phase II POPLAR trial and the randomized phase III OAK trial, both comparing atezolizumab versus docetaxel as second-line treatment in patients with NSCLC, were obtained as an excel file format, being available as supplementary information.12–14 The three datasets were merged into a metadaset containing 779 ICI-treated patients evaluable for overall survival (OS) and 669 patients evaluable for progression-free survival (PFS). We also analyzed the MSKCC pan-tumor cohort on exclusion of patients with NSCLC (n=1.311) to evaluate whether results from NSCLC can be extended to other tumor types. We did not use any variant interpreter to generate the model tested in survival analyses. However, the functional consequence of the detected mutations was evaluated in all the three cohorts using Fathmm (fathmm.biocompute.org.uk/), PROVEAN (provean.jcvi.org), SIFT (sift.bii.a-star.edu.sg) and PolyPhen (genetics.bwh.harvard.edu) (online supplementary files 1 and 2). In order to ensure the reproducibility of the results (and the generation of the model) in the various datasets, we did not consider CNVs.
Supplemental material
Supplemental material
Statistical analyses
Survival curves were estimated with the Kaplan-Meier product-limit method and compared by log-rank test. The nature of clinical variables included in multivariate Cox regression models for PFS and OS was determined on the basis of the possible association with the outcome of interest, and taking into account some differences in the nature of variables reported in the various databases. On this ground, we considered the following variables: smoking status, gender, TMB and histology. The related estimates were reported as HR and 95% CI. The relationship between categorical variables was assessed with the Pearson’s χ2 test of independence. Level of significance was defined as p<0.05. Statistical analyses were carried out using SPSS V.21.0 (SPSS, Chicago, Illinois, USA).
Results
Co-occurring mutations in NOTCH1-3 and homologous repair genes are associated with durable clinical benefit
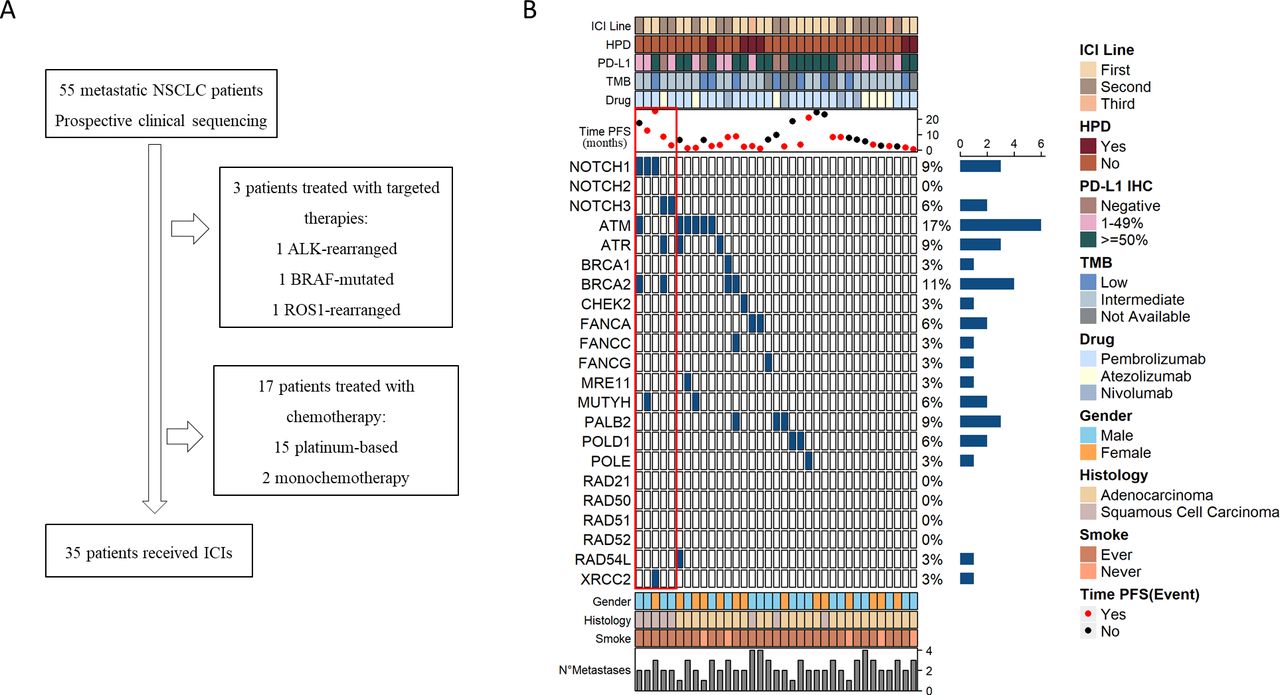
Among the 55 patients whose tissue samples underwent targeted sequencing in our observational study (Rome cohort), 20 were excluded as they did not receive immunotherapy (figure 1, panel A). Basal characteristics of the 35 ICIs-treated patients, along with the treatment received, disease evolution pattern and mutational landscape are illustrated in figure 1 (panel B) and summarized in table 1. Focusing on the mutations enriched in tumors from patients who obtained a DCB (defined as stable disease or tumor response lasting ≥6 months), we noticed four NOTCH gene mutations (patients 1–4). However, we also observed that a NOTCH3 mutation was present in a patient with rapidly progressing disease (patient 5). On this ground, we turned our attention to the pattern of co-occurrence/mutual exclusivity with other altered molecular networks. With this approach, we observed that while NOTCH-mutant tumors associated with DCB also harbored mutations in one or more homologous repair (HR) genes (ATR, ATM, BRCA1, BRCA2 and MUTYH), the only NOTCH-mutant tumor characterized by unresponsiveness did not carry any alterations in the HR machinery. Next, we noticed a trend towards higher TMB in HR-mutant tumors as compared with wild-type cases (online supplementary figure 1). Hypothesizing that co-occurring NOTCH and HR mutations may delineate an uncommon genomic background associated with sensitivity to ICIs, we gathered data from three different studies exploiting either tNGS and bNGS. These datasets contained largely overlapping HR genes (ATR, ATM, BRCA1, BRCA2, CHEK1, CHEK2, FANCA, FANCC, FANCG, MUTYH, PALB2, POLE, POLD, RAD50, RAD51 and its paralogs), which enabled us to recapitulate our model, where NOTCHmut/HRmut tumors were defined by a mutation in NOTCH1, NOTCH2 or NOTCH3 co-occurring with at least one mutation in the aforementioned HR genes.
Supplemental material
Characteristics of patients with NSCLC treated with ICIs included in the Rome cohort (n=35)

Characteristics of the patients. Panel A: study flow diagram. Panel B: OncoPrint illustrating the mutational status of NOTCH1-3 and homologous repair (HR) genes in the Rome cohort. The red box within the OncoPrint highlights the co-occurrence pattern (patient 1–4: co-occurring mutations; patient 5: NOTCH-only mutation). In the upper section, the OncoPrint treatment-related features are reported (progression-free survival (PFS) time and status, treatment administered, tumor mutation burden, programmed death-ligand 1 (PD-L1) expression, hyperprogressive disease (HPD), line of treatment). In the lower section, baseline characteristics (gender, histology, smoking history and number of metastatic sites) are summarized. ICI, immune checkpoint inhibitor; NSCLC, non-small cell lung cancer; TMB, tumor mutation burden.
The NOTCH/HR signature in the MSKCC/POPLAR/OAK cohort
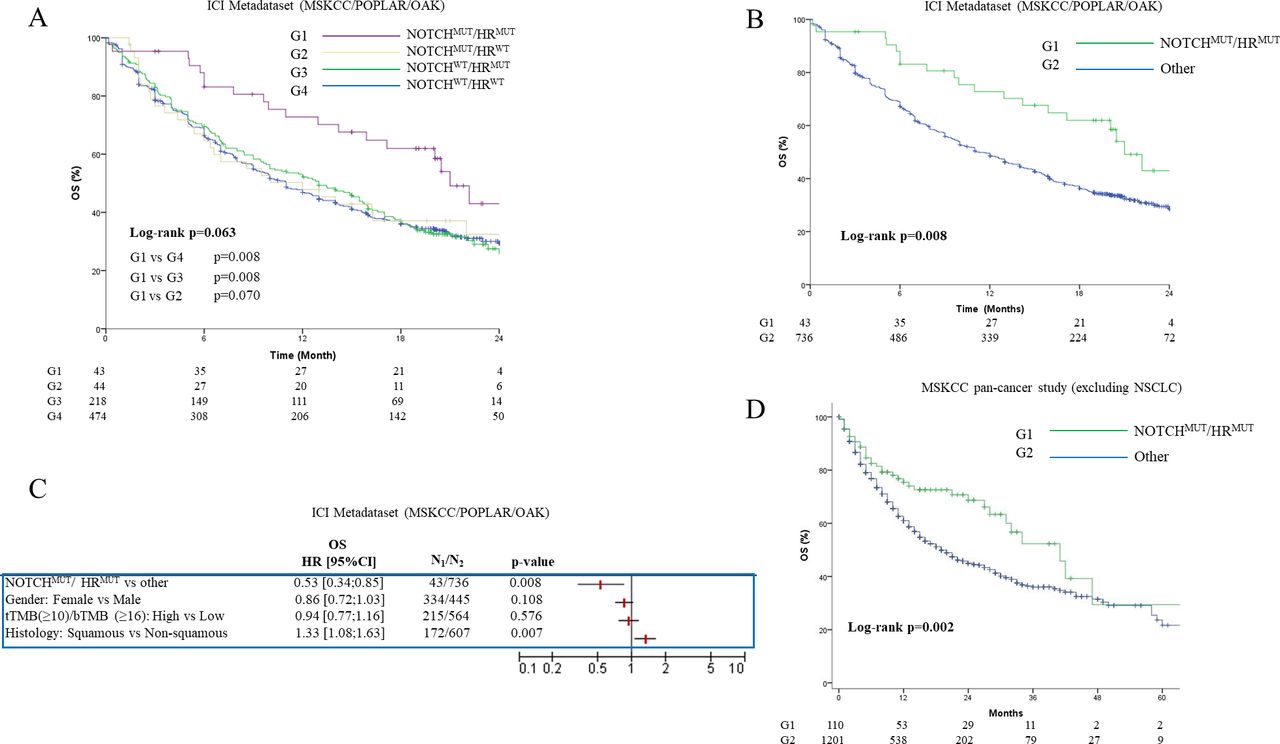
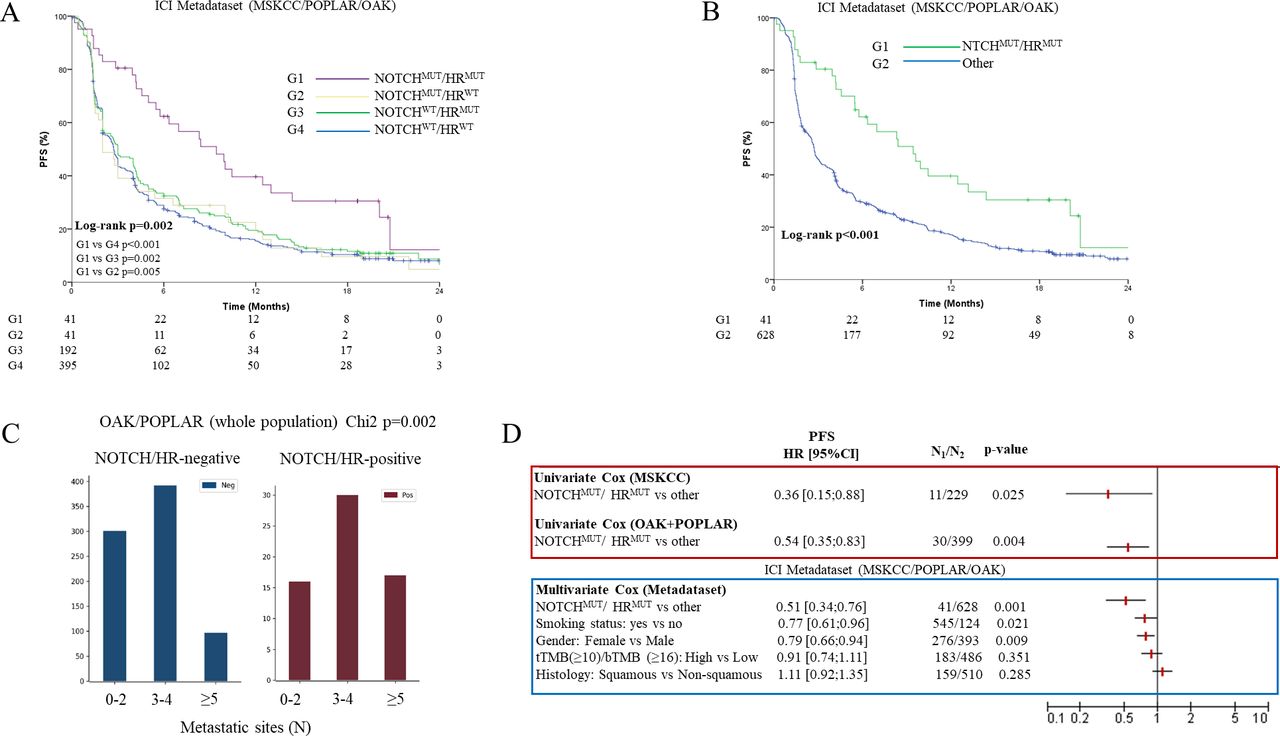
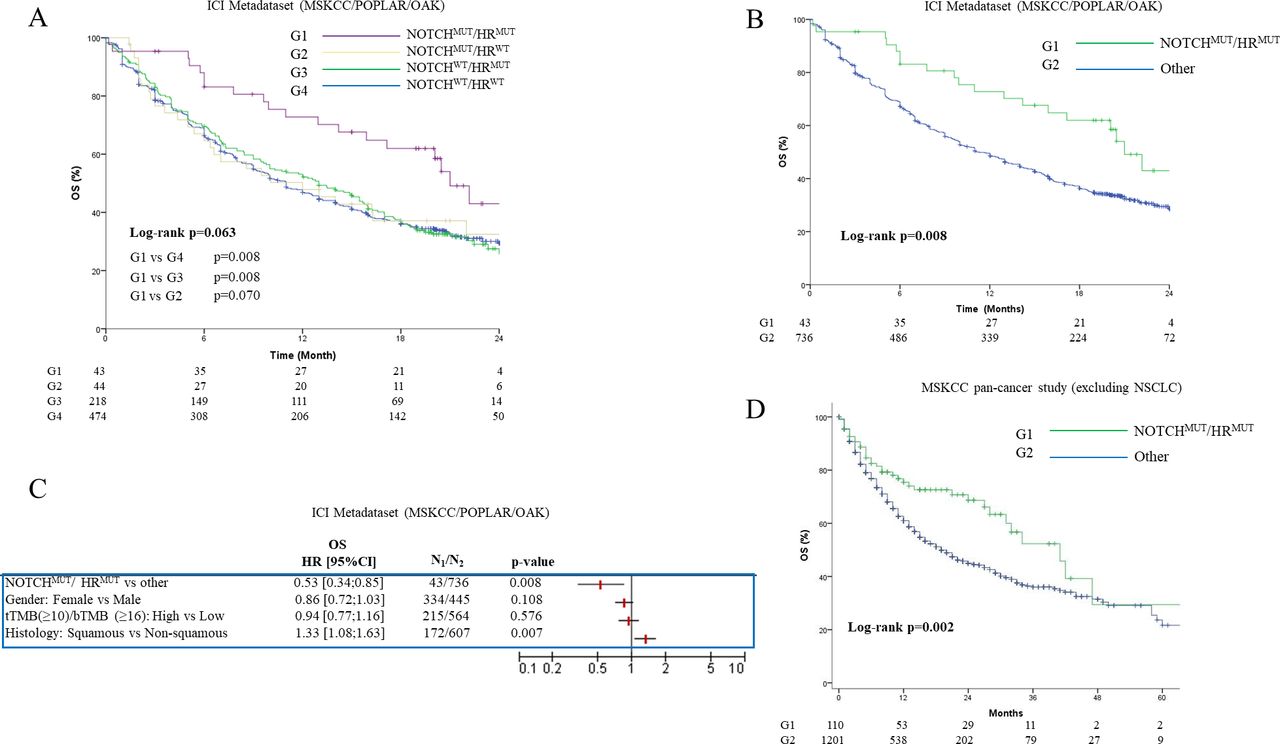
In the metadaset, patients whose tumors carried the NOTCHmut/HRmut signature had significantly longer PFS as compared with their negative counterparts (log-rank p=0.002, figure 2, panel A and B). The performances of the model were strictly dependent on the presence of alterations in both pathways, as documented by the drop of survival curves in patients with alterations in either NOTCH or the HR pathway (panel A). Importantly, the NOTCHmut/HRmut signature was associated with a higher metastatic burden (figure 2, panel C). On this basis, a ‘Janus-faced’ significance of the model may be envisioned, namely, an increased immune responsiveness coupled with more aggressive biological traits. In the multivariate Cox regression model, the genomic signature was associated with a decreased risk of disease progression (HR 0.51, 95% CI 0.34 to 0.76, p=0.001) (figure 2, panel D, blue box). The model retained its significance when separately evaluated (univariate analyses) in the MSKCC cohort (tNGS) and the POPLAR/OAK cohort (bNGS) (figure 2, panel D, red box). Patients with NOTCHmut/HRmut tumors also had longer survival (figure 3, panel A and B), as further confirmed in the multivariate Cox regression model (HR 0.53, 95% CI 0.34 to 0.85, p=0.008) (figure 3, panel C). Survival outcomes observed in the OAK/POPLAR (atezolizumab) and MSKCC cohorts (anti-PD-(L)1 monotherapy or in combination with anticytotoxic T-lymphocyte antigen-4 antibody) were comparable (online supplementary figure 2).
Supplemental material

Relationship between the NOTCHmut/HRmut signature and progression-free survival (PFS) in the MSKCC/POPLAR/OAK metadataset. Panel A and B: Kaplan-Meier survival curves of PFS comparing NOTCHmut/HRmut-positive versus NOTCHmut/HRmut-negative cases (ICI metadataset: MSKCC/POPLAR/OAK). Panel C: bar chart summarizing the association between the NOTCHmut/HRmut predictor and metastatic burden (number of metastatic sites) in the whole OAK/POPLAR cohort (atezolizumab or docetaxel). Panel D: forest plot illustrating univariate Cox regression analyses for PFS in the MSKCC and OAK/POPLAR studies (red box), and the multivariate Cox regression model in the metadataset (MSKCC/POPLAR/OAK, blue box). ICI, immune checkpoint inhibitor; MSKCC, Memorial Sloan Kettering Cancer Center; tTMB, tissue-based tumor mutation burden; bTMB, blood-based tumor mutation burden.
{kind=link}
{kind=link}
{kind=link}
Relationship between the NOTCHmut/HRmut signature and overall survival (OS). Panel A and B: Kaplan-Meier survival curves of OS comparing NOTCHmut/HRmut-positive versus NOTCHmut/HRmut-negative cases in the ICI metadataset (MSKCC/POPLAR/OAK). Panel C: forest plot illustrating the multivariate Cox regression model for OS in the ICI metadataset. Panel D: Kaplan-Meier survival curves for OS comparing NOTCHmut/HRmut-positive versus NOTCHmut/HRmut-negative cases in the MSKCC pan-cancer cohort (excluding NSCLC).
Interestingly, in chemotherapy-treated patients (docetaxel arm of the OAK/POPLAR trials, crossover not allowed, n=424) co-occurring NOTCH and HR mutations had an opposite clinical significance (online supplementary figure 3, panel A and B). Likewise, in the Rome cohort the two patients with tumors harboring co-existing mutations who experienced a DCB with immunotherapy in the second-line setting had a fairly short PFS with first-line chemotherapy (online supplementary figure 3, panel C). This observation was consistent with the clinical course of the disease recorded in the three patients with co-existing alterations who exclusively received chemotherapy (online supplementary figure 3, panel C). Thus, a treatment-dependent prognostic significance of the NOTCHmut/HRmut model may be envisioned.
Supplemental material
Finally, we verified whether the NOTCHmut/HRmut model retained its predictive capability in ICI-treated patients with other tumor types. Interestingly, the model was associated with longer OS also in the MSKCC pan-cancer dataset (ICI-treated patients) on exclusion of patients with NSCLC (n=1311, log-rank p=0.002, figure 3, panel D). In the pan-cancer cohort, cutaneous melanoma, bladder urothelial carcinoma and renal clear cell carcinoma are the most represented tumors (beyond lung adenocarcinoma). The frequency and type of NOTCH and HR mutations at the pan-cancer level is provided as online supplementary figure 4. For completeness, the mutational frequency of individual genes in the OAK/POPLAR and MSKCC studies is reported as online supplementary table 1.
Supplemental material
Supplemental material
Discussion
We herein presented first time evidence that pathway level alterations framed in a co-occurrence model may sharpen the therapeutic potential of ICIs in NSCLC. We are aware that our study has important limitations, mostly stemming from the small sample size of the original cohort. Likewise, it is worth mentioning that ~6% of NSCLC harbored a NOTCHmut/HRmut background, and this led to an imbalance in the size of the compared subgroups (NOTCHmut/HRmut, NOTCHmut/HRwt, NOTCHwt/HRmut, NOTCHwt/HRwt). Nevertheless, the reproducibility of the model across multiple cohorts leveraging different assays (tNGS and bNGS) suggests the robustness of our findings. Importantly, our data indicate that the NOTCHmut/HRmut signature retains its clinical significance also in other solid tumors.
From a biological perspective, alterations in the system deputed to repair DNA double-strand breaks, and in particular in the error-free HR machinery, culminate into increased mutational and neoantigen burden which, in turn, boost the immune response against tumors.15 16 Notch is involved in T-cell development, maintenance and activation.17 For instance, the pharmacological inhibition of NOTCH1 signaling, achieved by gamma-secretase inhibitors, reduced the number of activated T helper type 1 cells in murine models of autoimmune diseases.18 19 Moreover, preclinical evidence indicates that tumor cells and the tumor microenvironment evolves various mechanisms for evading T-cell-mediated killing, even including the suppression of NOTCH signaling.17 Consistently with the importance of NOTCH in regulating the immune response against tumors, chimeric antigen receptor T-cells generated with synthetic NOTCH receptors exhibit potent and specific cytotoxic responses.20 21 Furthermore, NOTCH mutations are thought to be enriched in NSCLC arising in smokers.22 The relationship between smoking status and NOTCH alterations is reported as online supplementary table 2. Overall, we can speculate that co-occurring mutations in the two aforementioned pathways may generate a tumor phenotype particularly vulnerable to immune-mediated killing.
Supplemental material
Conclusions
We provided evidence that co-occurring mutations in two pathways may predict a prolonged benefit from ICIs in NSCLC. The concept of pathway-level alterations combined through co-occurrence/mutual exclusivity deserves increased attention in the search of genomic biomarkers of ICIs efficacy. Consistently, we are further studying the co-mutation pattern of a restricted set of genes in NSCLC, pursuing the goal of delineating the genomic features of rapidly progressing tumors during immunotherapy. Collectively, our results encourage further investigations in prospective and adequately powered clinical trials, as well as in additional tumor types.
References
Footnotes
Twitter @dmarinelli93
Contributors Study conception: MM, RG, PV, MF, RDM, AV, GC, PM and MM-S. Data acquisition: MM, MF, MO, FR, AG, AB, GS and ADN. Data analysis and interpretation: MM, DM, SS, IT, FS, MP, EK, LP, MB, SC, FDN, LC, FG and MM-S. Manuscript drafting: MM and MM-S. Critical revision for important intellectual content: PV, MF, RDM, AV, GC and PM. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MM, MF, MO, DM, SS, IT, FS, MP, FR, AG, AB, GS, ADN, EK, MB, SC, MF, FDN, LC, FG, AV, GC, PM and MM-S declare no conflicts of interest. LP received travel grants from Eisai, Roche, Pfizer, Novartis; speaker fees from Roche, Pfizer, Novartis, Gentili. PV received travel grants from Eisai, Roche, Pfizer, Novartis; speaker fees/advisory boards from Roche, Pfizer, Novartis, Gentili. RDM declares to be a scientific advisory board member at ExosomicsSpA (Siena IT), Hibercell Inc. (New York, New York USA), Kiromic Inc. (Houston, Texas, USA) and at Exiris Inc. (Rome, Italy). RG received advisory boards/honoraria/speakers’ fee from AstraZeneca and Roche.
Patient consent for publication Not required.
Ethics approval This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee. Written informed consent was obtained from all participants.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request to the corresponding author.