Article Text

Abstract
Immune-checkpoint inhibitors have deeply changed the therapeutic landscape of advanced non-small cell lung cancer without actionable genomic alterations. Immune-checkpoint inhibitors have become standard front-line therapy, especially among patients with tumours expressing high levels of programmed death ligand-1; yet, many patients do not respond to therapy. This has led to the adoption of front-line combination therapies, administering programmed death-1 inhibitors concomitantly either with other checkpoint inhibitors, chemotherapy or both. Today’s approved standard of care includes options with chemoimmunotherapy or dual checkpoint blockade, but each combination has only been compared to chemotherapy alone and no head-to-head trials exist. In cross-trial comparisons, combinations trials appear to show numerically superior responses to single-agent checkpoint inhibitors but the question is whether they ultimately offer a survival advantage. In this manuscript, we summarize and analyse all currently available front-line immune-checkpoint inhibitor trials in non-small cell lung cancer, whether as monotherapy or in combination with chemotherapy, second immunotherapy agents or both. Should standards of care change given the current data? While we ponder this question, we illustrate current data and conclude that the answer lies in tracking the tail of the survival curves.
- immunotherapy
- lung neoplasms
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Immune-checkpoint inhibitors (ICIs) have deeply changed the therapeutic landscape of advanced non-small cell lung cancer (NSCLC) without actionable genomic alterations. Targeting the programmed death-1/programmed death ligand-1 (PD-1/PD-L1) axis has emerged as the standard of care, initially in second-line, then first-line therapy, with potential long-term survival in a subset of patients.1
Following positive results in KEYNOTE-001,1 pembrolizumab, an anti-PD-1 checkpoint inhibitor, was Food and Drug Administration (FDA)-approved as second-line monotherapy for NSCLC. Subsequently, in KEYNOTE-010, pembrolizumab confirmed an overall survival (OS) benefit, compared with second-line docetaxel in patients with tumors expressing PD-L1 in ≥1% of cells.2 Further randomized phase III trials with both atezolizumab, an anti-PD-L1 antibody, and nivolumab, an anti-PD-1 antibody, yielded similar results compared with docetaxel in the second-line, this time including patients whose tumors did not express PD-L1.3 4
Subsequently, KEYNOTE-024 and KEYNOTE-042 compared front-line pembrolizumab to platinum-based chemotherapy in tumors with PD-L1 ≥50% and 1%, respectively.5 6 Both studies showed an OS advantage which led to FDA approval of pembrolizumab in both patients population.7 Followed this, an international panel of thoracic oncologists published a position paper to share their concern about the approval of pembrolizumab in patients with NSCLC with PD-L1 >1%.8 The authors raised a few points: first of all in the KEYNOTE-042 nearly half (46.6%) of the patients enrolled had a PD-L1 ≥50%, which represented a potential bias for the over-performing efficacy of pembrolizumab in the intention to treat population. Second in the predefined OS analysis by PD-L1 expression, a survival benefit from pembrolizumab was not seen in the PD-L1 1%–49% subgroup (median OS 13.4 vs 12.1 months, HR 0.92, 95% CI 0.77 to 1.11). This suggests that the observed benefit with pembrolizumab has been largely driven by the “high PD-L1 expression” group, in which the HR for OS benefit mirrors that from a similar population in the KEYNOTE-024 trial (0.69 and 0.63, respectively). They concluded by stating that pembrolizumab monotherapy might not be the best treatment for patients with tumor PD-L1 of 1%–49% and this strategy could expose patients at risk of fast progression.
Similar findings were echoed by atezolizumab in IMpower 110,9 where a benefit in terms of OS was again driven by high PD-L1 expressors.9 In this trial, nearly 40% of the patients in both arms had a PD-L1 ≥50%. Unlike other trials in which the importance of high PD-L1 expression was known, the Checkmate 026 trial set a 5% cut-off for PD-L1 and did not stratify for PD-L1 ≥50%. The trial aimed to prove that nivolumab could improve progression-free survival (PFS) compared with standard platinum-based chemotherapy in that population. It failed to meet its primary endpoint.10 It is nonetheless worth mentioning that there was a clear imbalance among high PD-L1 expressors with 41% in the nivolumab arm and 60% in the chemotherapy arm.
However, many patients do not respond, leading to the adoption of front-line chemotherapy-ICI combinations across PD-L1 expression subtypes11 (table 1).
Selection of phase III combination chemotherapy-checkpoint inhibitor trials
Alternate strategies have explored combined PD-1 and CTLA-4 checkpoint blockade with conflicting results. Rizvi and colleagues12 recently reported findings from the Mystic trial. 1118 patients with previously untreated metastatic NSCLC without EGFR or ALK gene alterations were randomized (1:1:1) to receive platinum-based doublet chemotherapy, single-agent durvalumab (anti-PD-L1), or durvalumab with tremelimumab (anti-CTLA-4) combination therapy. It should be noted that KRAS alterations are not an exclusion factor, as these appear not to influence response to checkpoint inhibitors.13 14 The primary endpoints of the study were assessed in the 488 patients with PD-L1 expression in 25% of tumor cells or more and included OS for durvalumab versus platinum-based doublet chemotherapy, and OS and PFS for the durvalumab and tremelimumab combination versus chemotherapy. The study did not meet its primary endpoints. The median OS in patients with PD-L1 ≥25% was 16.3 months for patients treated with durvalumab, compared with 12.9 months with platinum-based doublet chemotherapy, without a statistically significant difference. The median OS for the durvalumab and tremelimumab combination was 11.9 months, which was lower than both the durvalumab and the chemotherapy arms. The median PFS for durvalumab and tremelimumab was quite disappointing, at 3.9 months, whereas the PFS with chemotherapy was 5.4 months.
The second coprimary endpoint of Checkmate 227, OS in patients with tumors with PD-L1 ≥1%, compared nivolumab plus ipilimumab to chemotherapy.15 The median OS was 17.1 months (95% CI 15.0 to 20.1) with nivolumab plus ipilimumab and 14.9 months (95% CI 12.7 to 16.7) with chemotherapy (p=0.007). OS rates at 1 and 2 years were 62.6% and 40.0%, respectively, with nivolumab plus ipilimumab, compared with 56.2% and 32.8% with chemotherapy. The HR for death of 0.79 (97.72% CI 0.65 to 0.96) should be interpreted in the context of the shape of the curves: a transient initial survival benefit with chemotherapy, followed by a significant long-term benefit with nivolumab plus ipilimumab. Response rate (RR) was 35.9% (95% CI 31.1 to 40.8) with nivolumab plus ipilimumab versus 30.0% (95% CI 25.5 to 34.7) with chemotherapy. Median duration of response among PD-L1 positive patients was 23.2 months (95% CI 15.2 to 32.2) with nivolumab plus ipilimumab and 6.2 months (95% CI 5.6 to 7.4) with chemotherapy. More patients had an ongoing response with nivolumab plus ipilimumab than chemotherapy (64.2% vs 27.9% at 1 year, 49.5% vs 11.0% at 2 years). Recently, the 3-year OS update was released at the American Society of Clinical Oncology 2020 Meeting, confirming durable benefit for the double immunotherapy blockade in the PD-L1 >1% cohort.16 The median OS was 17.1 months with nivolumab plus ipilimumab compared with 14.9 months with chemotherapy, with a HR of 0.79. OS rates at 3 years were 33% with nivolumab plus ipilimumab, compared with 22% with chemotherapy.
Nivolumab plus ipilimumab was also compared with chemotherapy in a prespecified descriptive analysis in patients with PD-L1 <1%, as well as in the entire population. Median OS was again longer with nivolumab plus ipilimumab (17.2 months; 95% CI 12.8 to 22.0) than chemotherapy (12.2 months; 95% CI 9.2 to 14.3), with a HR for death of 0.62 (95% CI 0.48 to 0.78) in that subgroup 2-year OS was 40.4% for nivolumab plus ipilimumab and 23.0% for chemotherapy. In all trial patients, duration of response to nivolumab plus ipilimumab was 19.6 months and 5.8 months with chemotherapy. The 3-year OS update confirmed durable benefit for the double immunotherapy blockade even in this exploratory subgroup.16 The median OS was 17.2 months with nivolumab plus ipilimumab versus 12.2 months with chemotherapy with a HR of 0.64. OS rates at 3 years were 34% with nivolumab plus ipilimumab, compared with 15% with chemotherapy.
The ongoing RR in the Checkmate 227 trial was 49% with nivolumab plus ipilimumab, but only 11% with chemotherapy at the 24-month analysis. Nevertheless, the OS was longer with nivolumab plus ipilimumab in all trial patients, including those with PD-L1 <1%, a population for whom anti-PD-1 monotherapy is not an effective option. Although the relative benefit of nivolumab plus ipilimumab compared with chemotherapy was numerically greater in patients with tumors expressing PD-L1 <1% than in those with PD-L1 >1%, it was likely due to performance variations in control arms. Median duration and rates of 1-year and 2-year OS with nivolumab plus ipilimumab were nearly identical in both PD-L1 subgroups, but chemotherapy underperformed in the PD-L1 <1% group.
The Checkmate 9LA trial (NCT03215706) was designed in order to provide rapid disease control while building on the durable OS benefit observed with the combination of nivolumab and ipilimumab, the. In this phase III trial, two cycles of standard platinum-based chemotherapy were added upfront to the dual immune blockade, compared with standard platinum-based chemotherapy in first-line stage IV NSCLC. The primary endpoint was OS, and secondary endpoints included PFS, objective response rate (ORR), and efficacy by PD-L1 expression. The combination of chemotherapy, nivolumab and ipilimumab was previously explored and proven to be safe in part 2 of the Checkmate 568 trial.17
During a minimum follow-up of 12.7 months, nivolumab and ipilimumab with chemotherapy resulted in prolonged OS, with a median of 15.6 months compared with 10.9 months in patients receiving chemotherapy alone, with a HR of 0.66. The 1-year OS was 63% in the combination group compared with 47% in the chemotherapy-only group. The benefit was seen regardless of PD-L1 positivity, histology and multiple subgroups. There was, however, reduced efficacy among patients older than 75 and never smokers. Median PFS was also improved in the combination arm, at 6.7 months compared with 5.0 months with chemotherapy alone (HR, 0.68; 95% CI 0.57 to 0.82). The 1-year PFS was 33% and 18% in the combination and chemotherapy arms, respectively. The ORR was 38% with the combination compared with 25% with chemotherapy alone. The median duration of response was 11.3 months with nivolumab and ipilimumab plus chemotherapy compared with 5.6 months with chemotherapy.
The median OS, PFS and early landmark OS are important when evaluating efficacy, but the critical benchmark for success with immunotherapy is long-term survival. Improved 5 and even 10-year survival rates are new measures of success. The tail of the Kaplan-Meier curve captures our imagination. A subset of heavily pretreated patients from phase I ICI trials remains alive years later.1 Chemotherapy-ICI or ICI-ICI each have relative merits but how we gage success will be long-term OS. Unfortunately, there is no clear surrogate, no shortcut to those results. Chemotherapy improves RR and short-term PFS, but will that translate to long-term survival? Could cytotoxic chemotherapy ultimately hamper formation of immune-memory, improving short-term results but mortgaging long-term OS? There is no clear answer to these pressing questions for now, but perhaps a longer follow-up will provide much needed clarity.
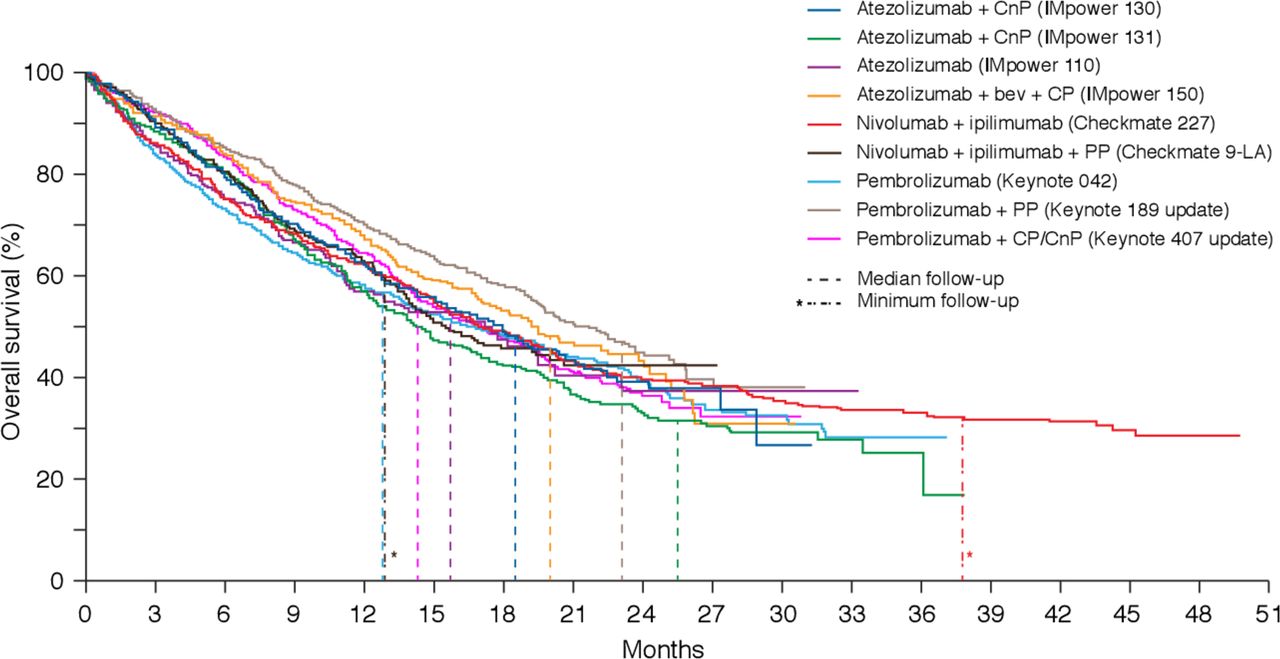
We summarize current data in a visual representation of Kaplan-Meier curves of first-line options for fit patients,18 including median follow-up as a reminder that current tails are not yet mature (figure 1). We conclude by pondering whether the standard of care has changed after Checkmate 227 and Checkmate 9LA. In our opinion, it has not, at least not yet. We need time to evaluate long-term efficacy of each strategy. It is unlikely that one size fits all, as unique patients will need individualized approaches, so it remains crucial to develop biomarkers.19 20 There are now several first-line options and we will develop our own practice patterns, but we must reassess as more mature data emerge.
{kind=link}
Overall survival curves from current front-line checkpoint-inhibitor trials in non small-cell lung cancer. CnP, carboplatin nab-paclitaxel; CP, carboplatin paclitaxel; PP, platinum pemetrexed.
We will place different values on the advantages of each strategy, but for us, tracking the tail will guide us to the answer.
Footnotes
Twitter @StephenVLiu
Contributors All the authors have equally contributed to the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AA has received compensation from Bristol-Myers Squibb, AstraZeneca, Merck Sharpe & Dohme, Takeda, Pfizer, Roche and Boehringer Ingelheim for participating on advisory boards. SVL Research: Ignyta, Genentech, Pfizer, Threshold, Clovis, Corvus, Esanex, Bayer, OncoMed, Merck, Lycera, AZ, Molecular Partners, Rain Therapeutics; Advisory boards: Ignyta, Genentech, Pfizer, Takeda, Celgene, Lilly, Taiho, BMS, AZ, Regeneron, Merck. S.P. Chawla: Honoraria/research/Advisory boards: Amgen, Roche, GSK, Threshold Pharmaceuticals, CytRx Corporation, Ignyta, Immune Design, TRACON Pharma, Karyopharm Therapeutics, Sarc, Janssen. AF has received compensation from Roche, Pfizer, Astellas and Bristol-Myers Squibb for service as a consultant.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.