Article Text

Abstract
Background T-cell immunoglobulin and ITIM domain (TIGIT) is identified as a novel checkpoint receptor that can facilitate immune escape via mediating T-cell exhaustion in tumors. However, the clinical significance and immune contexture correlation of intratumoral TIGIT+ CD8+ T-cells remain to be further explored in muscle-invasive bladder cancer (MIBC).
Methods 259 patients with MIBC from two clinical centers (Zhongshan Hospital, n=141; Shanghai Cancer Center, n=118) were analyzed to evaluate the prognostic value and immune contexture association of TIGIT+ CD8+ T-cells through immunohistochemistry. Fresh tumor tissue samples from 26 patients with MIBC were examined to discover the phenotype of this CD8 subpopulation by flow cytometry.
Results High infiltration of intratumoral TIGIT+ CD8+ T-cells predicted poor overall survival (OS) and recurrence-free survival (RFS) in MIBC. For patients with stage II MIBC with low infiltration of TIGIT+ CD8+ cells, adjuvant chemotherapy (ACT) could significantly prolong their OS and RFS. Intratumoral TIGIT+ CD8+ T-cell abundance was correlated with impaired CD8+ T-cell cytotoxicity and exhibited production of immunosuppressive cytokine IL-10. Further analysis of tumor-infiltrating immune cell landscape revealed TIGIT+ CD8+ T-cells were associated with suppressive immune contexture, including Th2 cells, regulatory T-cells, mast cells and neutrophils.
Conclusion Intratumoral TIGIT+ CD8+ T-cell abundance could serve as an independent prognosticator for clinical outcome and a predictive biomarker for inferior ACT responsiveness. Intratumoral TIGIT+ CD8+ T-cell abundance correlated with dampened CD8+ T-cell antitumor immunity and immunosuppressive contexture abundance, highlighting a tumor-promoting role of TIGIT+ CD8+ T-cells.
- urological neoplasms
- immune evation
- immunotherapy
- tumor microenvironment
- CD8-positive T-lymphocytes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Bladder cancer, a complex disease associated with high morbidity and mortality rates, is the ninth most common malignant disease worldwide.1 Approximately 25% of patients are diagnosed as muscle-invasive bladder cancer (MIBC), an advanced urothelial tumor with inferior prognosis.2 For these patients, the systemic cisplatin-based chemotherapy offers the chance to cure but still lacks enough evidence.3 4 Immune checkpoint inhibitors (ICIs) targeting program death-1 (PD-1)/program death-ligand 1 (PD-L1) axis and cytotoxic T lymphocyte-associated antigen-4 (CTLA-4) are emerging as a viable salvage treatment for patients in whom chemotherapy cannot control the disease, while the response rates are relatively low (21%).5 Hence, biomarkers for predicting patient survival outcomes and efficacy of chemotherapy and ICIs are being pursued.
As we have previously reported, tumor-infiltrating immune cells, including regulatory T-cells (Tregs), macrophages, mast cells and B cells, could affect the balance between antitumor immunity and immune evasion in MIBC.6–9 CD8+ T-cells, as the main effector immune cells, are critical to tumor initiation and progression and play a significant role in antitumor effect.10 However, CD8+ T-cells can be shifted from the effector state to the dysfunction state.11 Increasing studies have reported that intratumoral CD8+ T-cells are a highly heterogeneous population.12 A more precise identification of CD8+ T-cell subtypes is necessary for predicting disease progression and understanding the intrinsic antitumor mechanism in patients with MIBC.
T-cell immunoglobulin and ITIM domain (TIGIT), also known as Vstm3 and VSIG9, is a novel coinhibitory receptor.13 Within the tumor microenvironment, TIGIT that is mainly expressed on NK cells, CD8+ T-cells, and Tregs can facilitate immune evasion in acute myeloid leukemia, colon cancer and melanoma.14–17 TIGIT inhibits immune responses mediated by T-cells and NK cells through triggering CD155 on dendritic cells (DCs) or tumor cells.13 Currently, several studies have paid close attention to the role of targeting TIGIT in antitumor immunity and facilitate the development of anti-TIGIT monoclonal antibodies (mAbs).18 Preclinical models indicated that anti-TIGITs have demonstrated synergy with anti-PD-1/PD-L1 treatment.19 Previous studies have shown that a CD8+ T-cell subset expressing high levels of TIGIT infiltrated into multiple myeloma and glioblastoma multiforme, in which the TIGIT blockade strategies rapidly enhance the CD8+ T-cell-mediated immune response.20 21 However, the TIGIT+ CD8+ T-cell subset is poorly explored in MIBC, and the clinical significance of this subset still remains ambiguous.
In this study, we evaluated that intratumoral TIGIT+ CD8+ T-cells could be applied as a prognosticator and a predictive biomarker for adjuvant cisplatin-based chemotherapy with the retrospective analysis of 259 patients with MIBC from two independent clinical centers. Furthermore, we discovered an immunosuppressive contexture infiltration with TIGIT+ CD8+ T-cell abundance. This work is the first exploration of the comprehensive clinical value of TIGIT+ CD8+ T-cells in MIBC.
Materials and methods
Study cohort
This study enrolled two independent patient cohorts, including 393 patients with bladder cancer who were treated with radical cystectomy (RC) at Zhongshan Hospital of Fudan University from 2008 to 2012 (ZSHS cohort, n=215) and Fudan University Shanghai Cancer Center from 2002 to 2014 (FUSCC cohort, n=178). A total of 132 patients were excluded: 95 patients without MIBC, 19 patients without urothelial carcinoma, and 18 patients with unavailabe clinical or follow-up data. Because of the immunohistochemistry (IHC) detachment, a specimen was lost on the TMA in each cohort. Therefore, 259 eligible patients with MIBC were included (ZSHS cohort, n=141; FUSCC cohort, n=118). There were 119 patients of the two cohorts who received adjuvant cisplatin-based chemotherapy and lasted at least one therapeutic cycle. Patients received follow-up every 3 months in the first year, every 6 months for 2 years and once per year afterwards, which included clinical history, physical examination and laboratory test. All follow-up data were collected until July 2016. The overall survival (OS) and the recurrence-free survival (RFS) were defined the time from the date of RC to the date of death and the first recurrence, or to the last follow-up.
Immunohistochemistry
IHC staining was performed on formalin-fixed, paraffin-embedded tissue microarray (TMA) as described previously.22 The IHC antibodies are listed in online supplementary table 1. In brief, the slides were baked at 60°C for 6 hours, deparaffinized in xylene (three times, 15 min each) and rehydrated in graded alcohol. Next, the slides were immersed in sodium citrate buffer (0.01 M sodium citrate buffer, pH=6) for antigen retrieval and then blocked with 3% H2O2 in methanol at 37°C for 30 min. For single IHC staining, the slides were incubated with the primary antibodies at 4°C overnight and visualized by 3,3′-diaminobenzidine (DAB) stain system. For double IHC staining, after being processed as the same of single IHC DAB staining, the slides were incubated with the second primary antibodies at 4°C for 2 hours, and then Vector Blue AP Substrate Kit (Vector Laboratories) was applied. All TMA slides were evaluated under Leica DM6000 B Microsystems by PZ and LC independently, who were blinded to clinical data. The positive cells were enumerated from the representative view of the three sections in high-power field (HPF, ×200 magnification), and the mean value was adopted. The cut-off value was determined by X-tile V.3.6.1 (Yale University). For CD8+ T-cells, the cut-off value was 34 cells/HPF. For TIGIT+ CD8+ cells, the cut-off value was 8 cells/HPF.
Supplemental material
Flow cytometry
Fresh samples, including tumor tissues (n=26) and peritumor tissues (n=13), were collected from five different clinical centers (Zhongshan Hospital of Fudan University, Fudan University Shanghai Cancer Center, Ruijin Hospital, Shanghai General Hospital and Shanghai Ninth People’s Hospital). The peritumor tissues are obtained from an area of ≥2 cm from the tumor margin.
Single-cell suspension was performed as described.23 Then samples were stained with the indicated mAbs for 30 min at 4°C after lysing red blood cells. Cells were stimulated for 5 hours with phorbol myristate acetate (50 ng/mL) and ionomycin (1 µg/mL) in the presence of GolgiStop protein transport inhibitor (1:1000) for intracellular cytokine measurement. Cells were stained with interested surface markers, and Fixation/Permeabilization Solution Kit (BD Biosciences) was used for intracellular protein staining according to the manufacturer’s instructions. Stained cells were washed and resuspended in phosphate-buffered saline/0.1% bovine serum albumin coupled with azide. Flow cytometry data were analyzed by FlowJo software (Tree Star, San Carlos, California, USA). All flow cytometry antibodies are listed in online supplementary table 2.
Statistical analysis
Descriptive statistics was used to summarize patients’ baseline characteristics and disease factors. Results are shown as mean±SD, and Mann-Whiney U test, Wilcoxon signed-rank test, χ2 test and Spearman correlation analysis were used in this study. OS and RFS were determined by the Kaplan-Meier method, which was evaluated by log-rank tests. Multivariate analyses of the Cox regression model were applied to estimate HRs and 95% CIs. A two-tailed p value of <0.05 was considered statistically significant in our study. All statistical analyses were conducted using IBM SPSS Statistics V.25.0, R V.3.5.1, GraphPad Prism Software V.8.0 and MedCalc V.15.
Results
Residency of intratumoral TIGIT+ CD8+ T-cells correlates with disease progression in MIBC
The residency of TIGIT+ CD8+ T-cells in MIBC was identified through double IHC staining and flow cytometry (figure 1A,B and online supplementary figure 1). The patient characteristics are listed in online supplementary table 3. We found the proportion of patients with high TIGIT+ CD8+ T-cell infiltration expanded with progression of pathology Tumor (pT) or pathology Node (pN) stage (figure 1C). Moreover, the infiltration of TIGIT+ CD8+ T-cells, as well as the proportion of TIGIT+ CD8+ T-cell among CD8+ T-cells, was positively associated with the increased tumor stages (figure 1D and online supplementary figure 2). Furthermore, compared with peritumor tissues, we found that TIGIT+ CD8+ T-cells were dramatically more infiltrated in matched tumor tissues (figure 1E). In conclusion, these results confirmed the existence of TIGIT+ CD8+ T-cells in MIBC and indicated that intratumoral TIGIT+ CD8+ T-cells were correlated with MIBC progression.
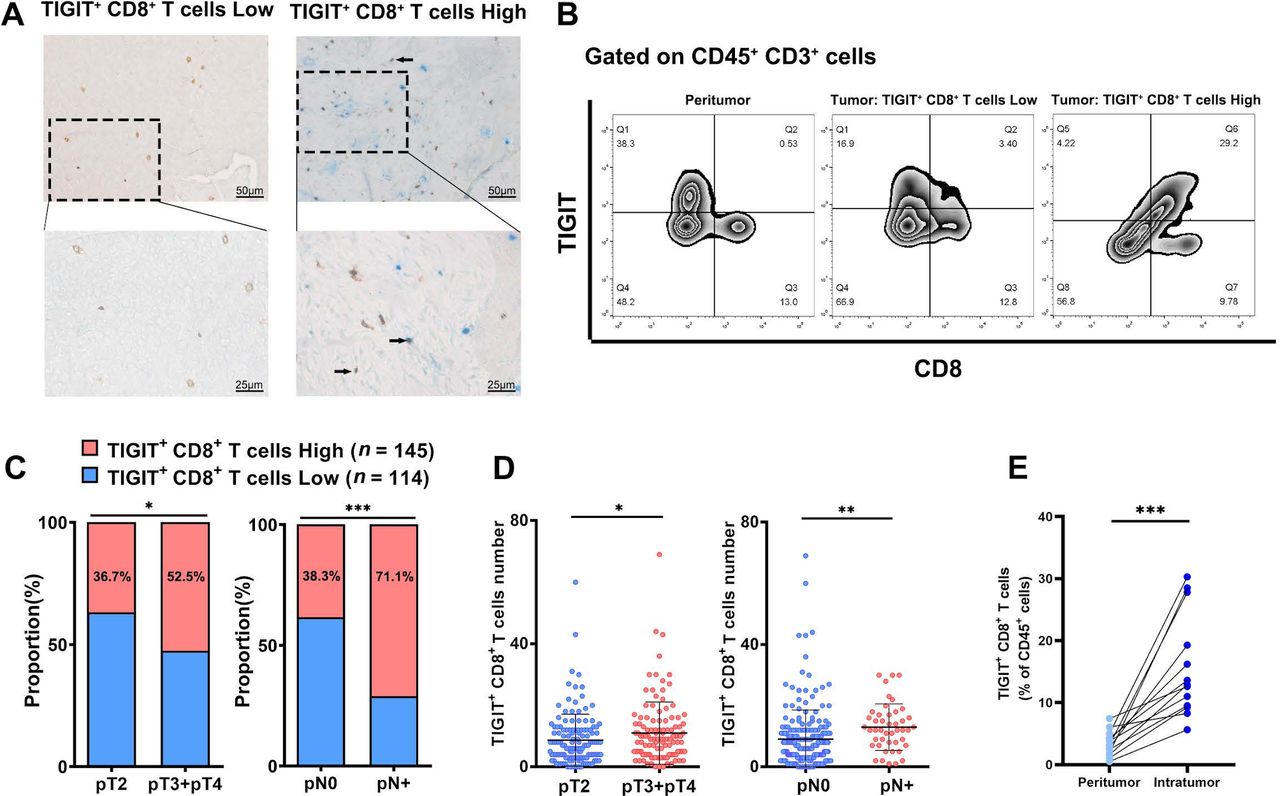
Intratumoral TIGIT+ CD8+ T-cells accumulate in MIBC and correlate with tumor progression. (A) Double immunohistochemistry staining for TIGIT (blue) and CD8 (brown) in MIBC tissues. Black arrowheads indicate TIGIT+ CD8+ T-cells. (B) Comparison of TIGIT+ CD8+ T-cell infiltration in tumor and peritumor tissues of patients with MIBC. (C) Proportion of patients with high/low TIGIT+ CD8+ T-cell infiltration in pT stage and pN stage. (D) Association of TIGIT+ CD8+ T-cell infiltration with pT stage and pN stage. (E) Comparison of TIGIT+ CD8+ T-cells among CD45+ cells in tumor and peritumor tissues of patients with MIBC. *P<0.05, **P<0.01, ***P<0.001 by χ2 test, Mann-Whitney U test and paired t-test. pT, pathology Tumor; pN, pathology Node; MIBC, muscle-invasive bladder cancer; TIGIT, T-cell immunoglobulin and ITIM domain.
Intratumoral TIGIT+ CD8+ T-cells act as a prognosticator for survival outcome in MIBC
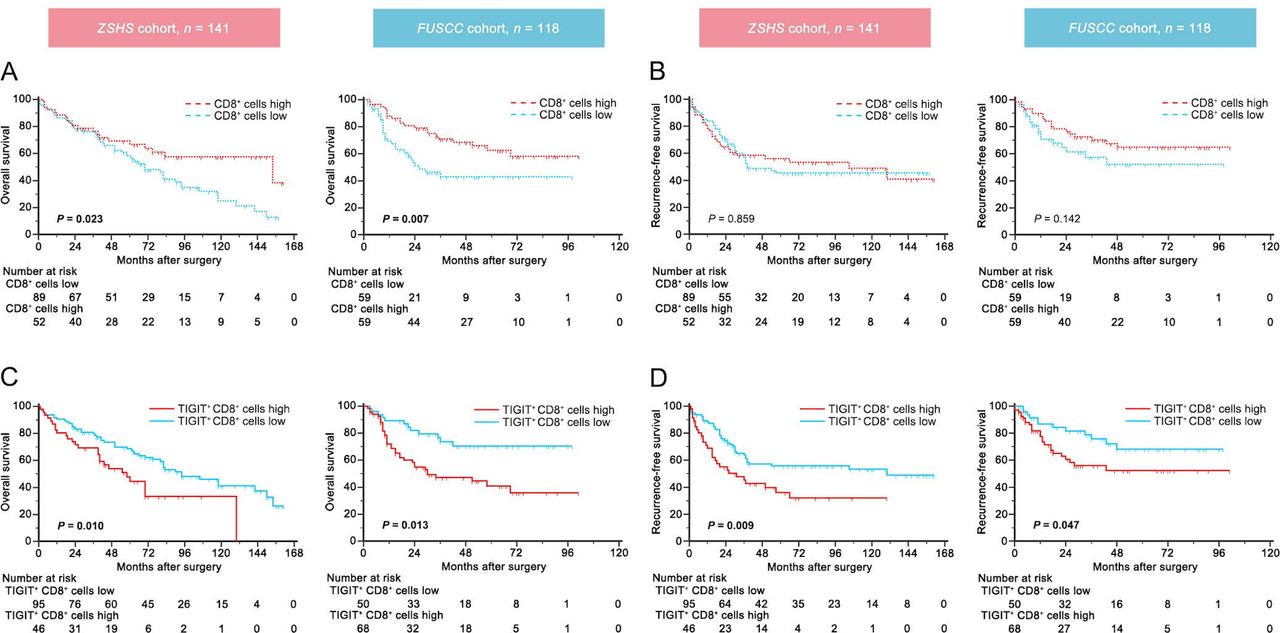
The prognostic ability of TIGIT+ CD8+ T-cells was next explored. We found that CD8+ T-cell infiltration could prolong the OS of patients with MIBC both in the ZSHS cohort and the FUSCC cohort (p=0.023 and p=0.007, figure 2A). However, the RFS showed no difference with CD8+ T-cell strata (p=0.859 and p=0.142, figure 2B). Interestingly, the TIGIT+ CD8+ cells high infiltration group possessed inferior OS and RFS than the TIGIT+ CD8+ cells low infiltration group in both cohorts (OS: p=0.010 and p=0.013, figure 2C; RFS: p=0.009 and p=0.047, figure 2D), which was entirely contrary to the prognosis of CD8+ T-cell infiltration. Additionally, multivariate Cox regression analysis showed that TIGIT+ CD8+ T-cell infiltration was an independent prognostic factor for patients with MIBC after adjustment for age, gender, grade, lymphovascular invasion, adjuvant chemotherapy (ACT), pathological T/N stage and CD8+ T-cell infiltration as confounders (online supplementary table 4). Therefore, TIGIT+ CD8+ T-cells proved to be an independent unfavorable factor to predict survival and recurrence in patients with MIBC.

Intratumoral TIGIT+ CD8+ T-cell infiltration yields poor prognosis in muscle-invasive bladder cancer. (A,B) Kaplan-Meier curves for OS (A) and RFS (B) according to high/low CD8+ T-cell infiltration in the ZSHS cohort (n=141) and the FUSCC cohort (n=118). (C,D) Kaplan-Meier curves for OS (C) and RFS (D) according to high/low TIGIT+ CD8+ T-cell infiltration in the ZSHS cohort (n=141) and the FUSCC cohort (n=118). Log-rank test was performed for Kaplan-Meier curves. FUSCC, patients with bladder cancer who were treated with radical cystectomy at Fudan University Shanghai Cancer Center from 2002 to 2014; OS, overall survival; RFS, recurrence-free survival; TIGIT, T-cell immunoglobulin and ITIM domain; ZSHS, patients with bladder cancer who were treated with radical cystectomy at Zhongshan Hospital of Fudan University from 2008 to 2012.
Intratumoral TIGIT+ CD8+ T-cells could predict ACT effectiveness within patients with stage II MIBC
ACT has been widely used in the treatment for patients with MIBC with pT3/4 or pN+ disease.24 Thus, we evaluated whether intratumoral TIGIT+ CD8+ T-cell abundance was associated with ACT responsiveness. Both cohorts were combined for further investigation. In all patients or patients with stage III MIBC, intratumoral TIGIT+ CD8+ T-cell infiltration failed to predict ACT responsiveness (online supplementary figure 3). No evidence suggested that ACT could improve OS or RFS in patients with stage II MIBC (OS: p=0.087, RFS: p=0.128; figure 3A,D). CD8+ T-cells still failed to predict ACT effectiveness in patients with stage II MIBC (online supplementary figure 4). However, after dividing patients into TIGIT+ CD8+ T-cells high and low infiltration subgroups, we found that ACT successfully prolonged both OS and RFS in patients with low TIGIT+ CD8+ T-cell infiltration (OS: p=0.043, RFS: p=0.013; figure 3C,F), while no survival benefit was observed in patients with high TIGIT+ CD8+ T-cell infiltration (OS: p=0.261, RFS: p=0.769; figure 3B,F). In addition, univariate Cox regression analysis was performed to assess the relationship between TIGIT+ CD8+ T-cell infiltration and ACT benefit, which suggested that patients with stage II MIBC with TIGIT+ CD8+ T-cells low infiltration could receive more benefit from ACT (OS: HR, 0.340, 95% CI, 0.114 to 0.950, p=0.049; RFS: HR, 0.239, 95% CI, 0.070 to 0.817, p=0.022; online supplementary table 5). Herein, these results suggested that TIGIT+ CD8+ T-cells high abundance predicted suboptimal ACT responsiveness within patients with stage II MIBC. Patients with low TIGIT+ CD8+ T-cell infiltration could benefit more from ACT.
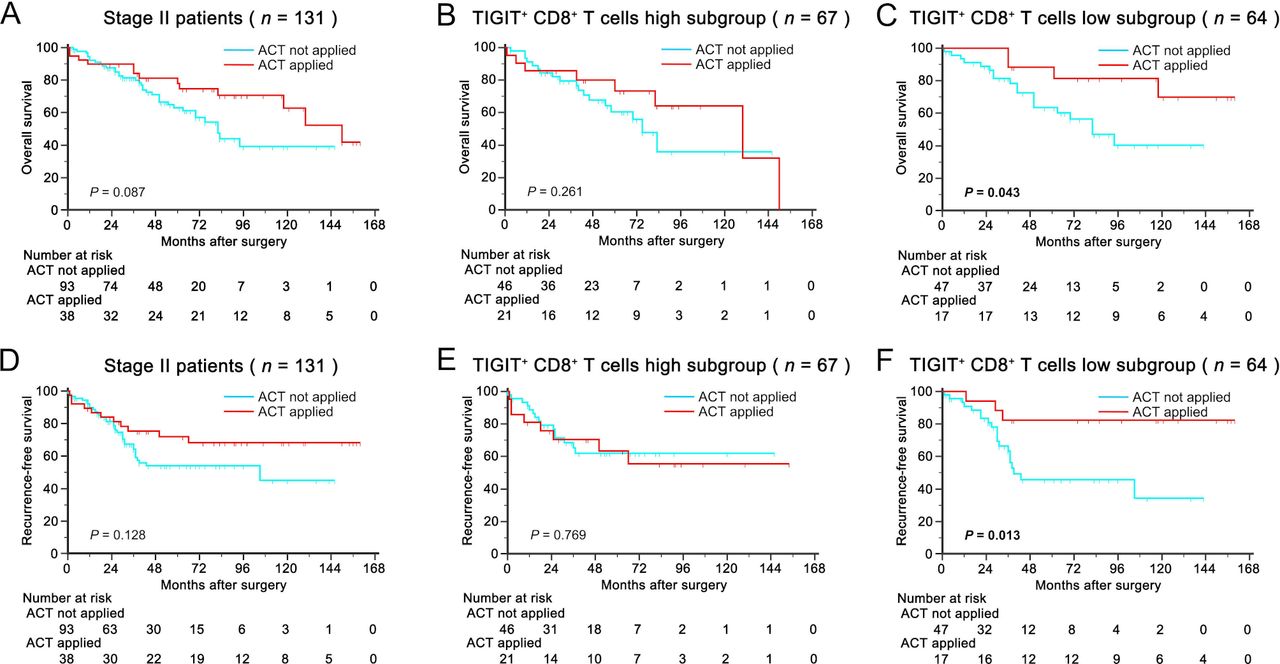
Intratumoral TIGIT+ CD8+ T-cell infiltration predicts suboptimum responsiveness to ACT in patients with stage II MIBC. (A–C) Kaplan-Meier curves for overall survival with ACT application strata in patients with stage II MIBC (A), TIGIT+ CD8+ T-cells high subgroup (B) and TIGIT+ CD8+ T-cells low subgroup (C). (D–F) Kaplan-Meier curves for recurrence-free survival with ACT application strata in patients with stage II MIBC (D), TIGIT+ CD8+ T-cells high subgroup (E) and TIGIT+ CD8+ T-cells low subgroup (F). Log-rank test was performed for Kaplan-Meier curves. ACT, adjuvant chemotherapy; MIBC, muscle-invasive bladder cancer; TIGIT, T-cell immunoglobulin and ITIM domain.
Intratumoral TIGIT+ CD8+ T-cell abundance impairs CD8+ T-cell antitumor immunity in patients with MIBC
Coinhibitory receptors, also known as immune checkpoints, are often coexpressed on dysfunctional CD8+ T-cells.25 Compared with TIGIT- CD8+ T-cells, TIGIT+ CD8+ T-cells expressed higher levels of immune checkpoints, including PD-1, CTLA-4, Lag-3 and Tim-3 (online supplementary figure 5A). Meanwhile, TIGIT+ CD8+ T-cells had a higher level of proliferative marker (Ki-67), effector markers (interferon (IFN)-γ, tumor necrosis factor (TNF)-α and interleukin (IL)-2) and cytolytic marker (CD107a) compared with their TIGIT− counterparts (online supplementary figure 5B–D), which inferred that TIGIT+ CD8+ T-cells could be closely related to a terminally exhausted CD8+ T-cell phenotypes as previously reported.26
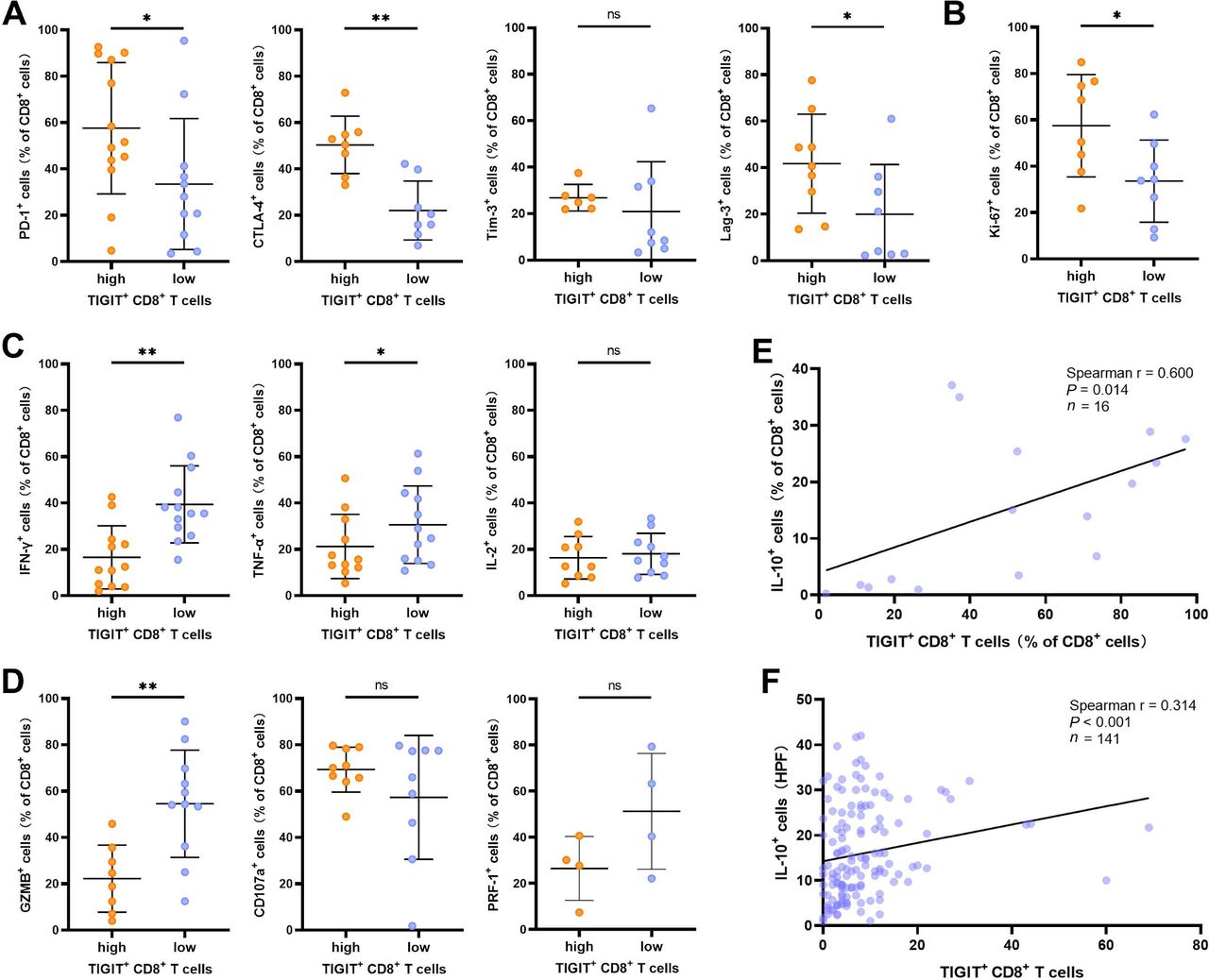
The global characterization of CD8+ T-cells was subsequently investigated according to TIGIT+ CD8+ T-cell abundance. We found that CD8+ T-cells in TIGIT+ CD8+ T-cells high infiltration tumors expressed increased immune checkpoints, including PD-1, CTLA-4 and Lag-3 (figure 4A) while exhibiting more proliferative ability (Ki-67) than their counterparts in TIGIT+ CD8+ T-cells low infiltration tumors (figure 4B). Additionally, the effector cytokines (IFN-γ and TNF-α) and cytotoxicity activation molecules (granzyme B (GZMB)) expressed by CD8+ T-cells were decreased in TIGIT+ CD8+ T-cells high infiltration tumors (figure 4C,D). These results indicated that high TIGIT+ CD8+ T-cells were associated with impaired CD8+ T-cell antitumor immunity. In addition to CD8+ T-cells, CD45+ T-cells in TIGIT+ CD8+ T-cells high infiltration tumors expressed increased immune checkpoints, including PD-1, CTLA-4 and Tim-3, while the percentage of CD45+ T-cells expressing effector cytokines (IFN-γ and TNF-α) decreased in TIGIT+ CD8+ T-cells high infiltration tumors. (online supplementary figure 6). Interestingly, we found that TIGIT+ CD8+ T-cells could produce immunosuppressive cytokine IL-10 (online supplementary figure 5E). TIGIT+ CD8+ T-cell infiltration was also found positively associated with intratumoral IL-10+ CD8+ T-cells and IL-10 expression in the tumor microenvironment (figure 4E,F). These results preliminarily verified our conjecture that intratumoral TIGIT+ CD8+ T-cell abundance may contribute to immune suppression and dampen CD8+ T-cell immune response in MIBC.
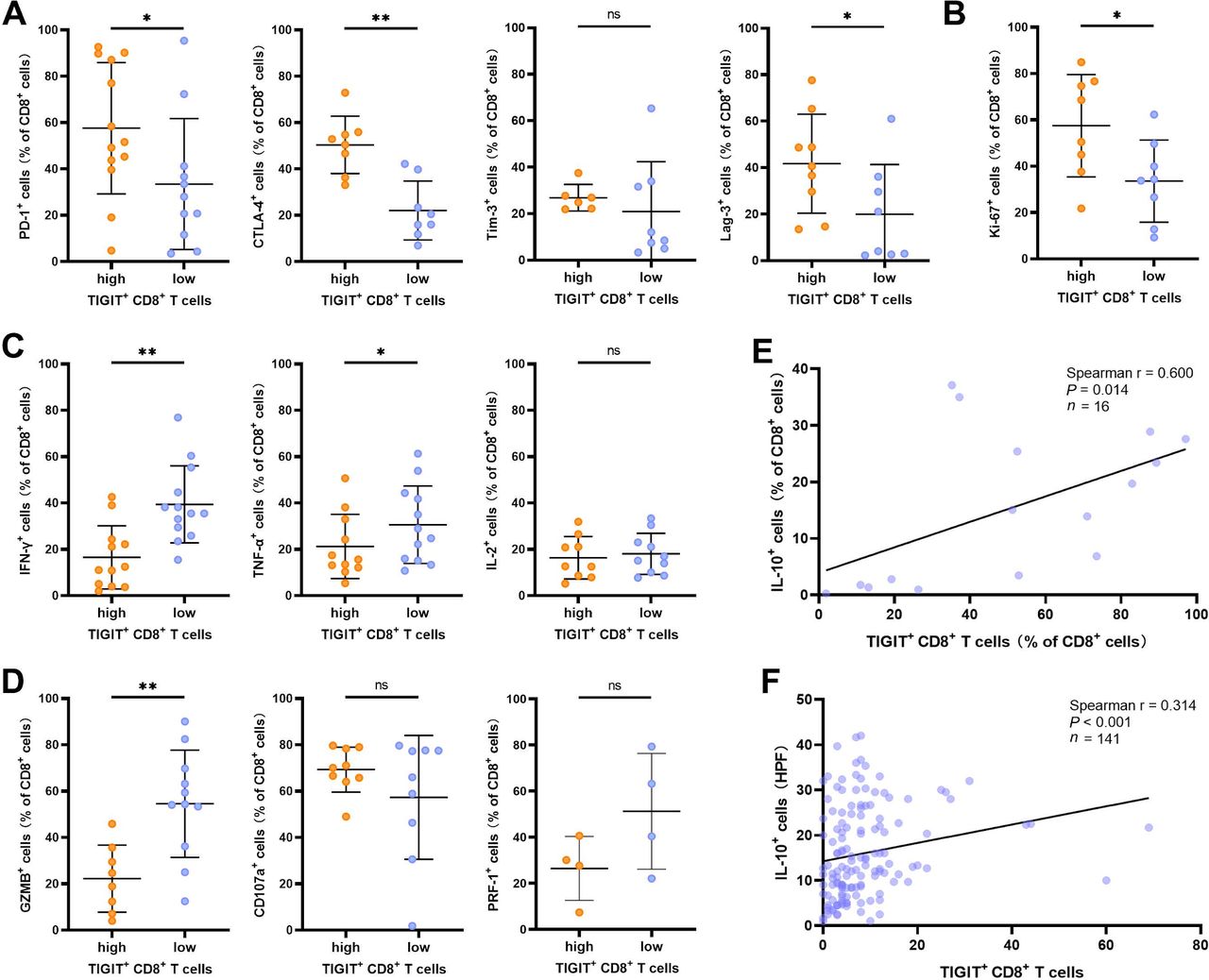
Intratumoral TIGIT+ CD8+ T-cell infiltration impairs CD8+ T-cell antitumor immunity in patients with muscle-invasive bladder cancer. (A) Expression of coinhibitory receptors (PD-1, n=24; CTLA-4, n=16; Tim-3, n=14; Lag-3, n=17) on CD8+ T-cells in TIGIT+ CD8+ T-cells high/low infiltration group. (B) Expression of proliferation marker (Ki-67, n=16) on CD8+ T-cells in TIGIT+ CD8+ T-cells high/low infiltration group. (C) Expression of effector cytokines (IFN-γ, n=23; TNF-α, n=23; IL-2, n=19) on CD8+ T-cells in TIGIT+ CD8+ T-cells high/low infiltration group. (D) Expression of cytotoxicity activation molecules (GZMB, n=19; CD107a, n=18; PRF-1, n=8) on CD8+ T-cells in TIGIT+ CD8+ T-cells high/low infiltration group. (E) Correlation between TIGIT+ CD8+ T-cells among CD45+ cells and IL-10+ CD8+ T-cells among CD45+ cells based on the results of flow cytometry. (F) Correlation between TIGIT+ CD8+ T-cells and IL-10+ cells based on the evaluation of immunohistochemistry staining. *P<0.05, **P<0.01 by Mann-Whitney U test. PD-1, program death-1; CTLA-4, cytotoxic T lymphocyte-associated antigen-4; IFN, interferon; IL, interleukin; GZMB, granzyme B; ns, no significance; TIGIT, T-cell immunoglobulin and ITIM domain.
Intratumoral TIGIT+ CD8+ T-cell abundance contributes to immunosuppressive contexture in patients with MIBC
Next, the association between immune contexture and TIGIT+ CD8+ T-cell abundance was explored in MIBC. Eleven types of immune cells were evaluated inthe ZSHS cohort (figure 5A, n=141). The representative images of immune cells are illustrated in online supplementary figure 7. TIGIT+ CD8+ T-cell infiltration was positively correlated with protumor Th2 cells (Spearman r=0.317, p<0.001), Tregs (Spearman r=0.309, p<0.001), mast cells (Spearman r=0.334, p<0.001), neutrophils (Spearman r=0.178, p=0.035) infiltration and antitumor NK cells (Spearman r=0.183, p=0.029), and M1 macrophages (Spearman r=0.251, p=0.003) infiltration (figure 5B,C). These data indicated that intratumoral TIGIT+ CD8+ T-cell abundance indicated tumor-promoting immune microenvironment in MIBC.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Intratumoral TIGIT+ CD8+ T-cell infiltration shapes immunosuppressive contexture in patients with muscle-invasive bladder cancer. (A) Heatmap displaying scaled expression of various immune cell types between high/low percentage of TIGIT+ CD8+ T-cells. (B,C) Correlation between TIGIT+ CD8+ T-cell infiltration and CD8+ T-cells, CD4+ T-cells, Th1 cells, Th2 cells, regulatory T-cells, natural killer cells, M1 macrophages, M2 macrophages, mast cells and neutrophil infiltration based on the evaluation of immunohistochemistry staining. P<0.05 by Spearman rank correlation test. TIGIT, T-cell immunoglobulin and ITIM domain.
Discussion
Currently, CD8+ T-cells were regarded as a protective factor in various solid tumors, including bladder cancer.27 28 However, CD8+ T-cells remain heterogeneous, and several subtypes of intratumoral CD8+ T-cells are associated with poor clinical outcomes.29 TIGIT, a novel coinhibitory receptor, can promote tumor growth and drive the exhaustion of tumor-infiltrating lymphocytes, including CD8+ T-cells in multiple cancer types.14 15 20 In this study, we reported that intratumoral TIGIT+ CD8+ T-cell abundance was positively correlated with tumor development and enriched in MIBC tissues. Contrary to CD8+ T-cells in MIBC, TIGIT+ CD8+ T-cells were identified as an adverse prognosticator through the retrospective analysis of a considerable population.
The application of ACT is supported by recent data while still lacking enough evidence.4 It is showed that a tumor immune microenvironment may influence the chemotherapeutic efficacy.30 Our previous studies have uncovered the contribution of certain immune contexture to ACT resistance, including tumor-infiltrating masT-cells, neutrophils, B cells and an immunotype A/B classification.6–9 Though no association was found between CD8+ T-cell infiltration and ACT beneficial, TIGIT+ CD8+ T-cell abundance could predict a suboptimal ACT responsiveness, which further exhibited the potential heterogeneity of intratumoral CD8+ T-cells. The identification of certain CD8+ T-cell subpopulation could assist in guiding adjuvant therapy. Of note, the usage of ACT was not randomized; there could be possible bias introduced by comparing those groups. The confounders could be the tumour, node, metastasis stage of the patients and other possible factors. Through adjusting these confounders, we found that intratumoral TIGIT+ CD8+ T-cell infiltration failed to predict ACT responsiveness in all patients or patients with stage III MIBC. However, in patients with stage II MIBC, ACT successfully prolonged both OS and RFS in patients with low TIGIT+ CD8+ T-cell infiltration. We would further validate our findings in a prospective, larger, multicentered randomized trial in the future.
The expression of TIGIT on NK cells and Tregs often relates to cytotoxicity inhibition and enhanced suppressive function.16 17 Present findings revealed that TIGIT expressed on CD8+ T-cells downregulated T-cell cytotoxicity and activation,31 supporting our results that TIGIT+ CD8+ cell abundance impaired CD8+ T-cell antitumor immunity. Additionally, TIGIT+ CD8+ T-cells were associated with suppressive immune contexture, including Th2 cells, Tregs, mast cells and neutrophils,32 of which mast cells and neutrophils infiltrating into MIBC were identified as protumor immunocytes in our previous studies.7 9 A confusing point was that TIGIT+ CD8+ T-cells were positively correlated with M1 macrophages. One possible explanation could be that the elevated M1 macrophages triggered an antitumor immunity. In order to escape the antitumor immunity, the tumor microenvironment upregulated the expression of TIGIT on CD8+ T-cells. It is showed that TIGIT is highly expressed on NK cells,13 which might be the cause of the positive correlation between TIGIT+ CD8+ T-cells and NK cells. Early studies revealed that TIGIT could exert immunoregulatory function through multiple mechanisms, including promoting IL-10 by Tregs and dendritic cells,17 33 suppressing the activity of its costimulatory counterpart CD22634 or directly inhibiting the intrinsic recruitment of Src homology domain containing tyrosine phosphatase (SHP).35 Interestingly, we found that TIGIT+ CD8+ T-cells have the capacity for IL-10 production, which could be one explanation for the CD8+ T-cell dysfunction and immunoevasive microenvironment in tumors with high TIGIT+ CD8+ T-cell infiltration. Although there were limited reports about IL-10 producing CD8+ T-cells in the tumor immune microenvironment, specific CD8+ T-cells producing IL-10 on antigen recognition could be observed in chronic infection like hepatitis B virus (HBV) and human T-cell lymphotropic virus type 1 (HTLV-I).36 37 The intrinsic mechanism of TIGIT shaping the dysfunction state of CD8+ T-cells needs further investigation.
Intriguingly, the phenotype of TIGIT+ CD8+ T-cells presented a high level expression of both immune checkpoints and effector molecules, which were identified as terminally exhausted CD8+ T-cells with cytotoxicity but short-lived in tumor immunity.26 Thus, these subpopulations presented inferior tumor control compared with the poorly cytotoxic but long-survived counterpart (progenitor exhausted CD8+ T-cells). Immune checkpoint blockade therapy, such as nivolumab (anti-PD-1) and atezolizumab (anti-PD-L1), presented a confirmed but relatively low response rate on advanced cancer of urinary bladder (19.6% and 13.4%).38 39 It is reported that PD-1 blockade shows no act on terminally exhausted CD8+ T-cells.26 Therefore, the existence of TIGIT+ CD8+ T-cells in MIBC may be one explanation for the low response rate of anti-PD-1 therapy. On the other hand, whether TIGIT+ CD8+ T-cells could predict traditional immune checkpoint blockade efficacy should be investigated. Moreover, the combination of anti-PD-1 and anti-TIGIT presented a considerable efficacy in glioblastoma multiforme.21 The immunotherapeutic potential of TIGIT and the synergistic effect of double immune checkpoint blockade in MIBC are worthy of further study.
Conclusion
In summary, the current investigation identified intratumoral TIGIT+ CD8+ T-cell abundance as an adverse prognostic factor for clinical outcome and a predictive biomarker for suboptimal ACT responsiveness in MIBC. Furthermore, intratumoral TIGIT+ CD8+ T-cell abundance correlated with impaired CD8+ T-cell antitumor immunity and shaped immunosuppressive contexture, highlighting its tumorgenic role. These findings indicated that TIGIT might be a potential immunotherapeutic target in MIBC.
Acknowledgments
We thank Dr Lingli Chen (Department of Pathology, Zhongshan Hospital, Fudan University, Shanghai, China) and Dr Yunyi Kong (Department of Pathology, Fudan University Shanghai Cancer Center, Shanghai, China) for their excellent pathological technology help.
References
Footnotes
ZL, QZ, ZW and HZ contributed equally.
Contributors ZLiu, QZ, ZW and HZh: acquisition of data, analysis and interpretation of data, statistical analysis and drafting of the manuscript; HZe, QH, YChe, WJ, ZLin, YQ, YXio, QB, YXia, YW, LL, YZ, LX, BD and JG: technical and material support; JW, YCha and WZ for study concept and design, analysis and interpretation of data, drafting of the manuscript, obtainment of funding and study supervision. All authors read and approved the final manuscript.
Funding This work was supported by grants from National Natural Science Foundation of China (81671628, 81702496, 81702497, 81702805, 81772696, 81871306, 81872082, 81902556, 81902563, 81902898 and 81974393), National Key R&D Program of China (2017YFC0114303), Shanghai Municipal Natural Science Foundation (16ZR1406500, 17ZR1405100 and 19ZR1431800), Guide Project of Science and Technology Commission of Shanghai Municipality (17411963100), Shanghai Sailing Program (18YF1404500, 19YF1407900, 19YF1427200, 20YF1406100 and 20YF1406200), Shanghai Municipal Commission of Health and Family Planning Program (20174Y0042, 201840168 and 20184Y0151), Fudan University Shanghai Cancer Center for Outstanding Youth Scholars Foundation (YJYQ201802) and Shanghai Cancer Research Charity Center.
Disclaimer All these study sponsors have no roles in the study design, in the collection, analysis and interpretation of data.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study followed the Declaration of Helsinki and was approved by the clinical research ethics committee of Zhongshan Hospital of Fudan University, Fudan University Shanghai Cancer Center, Ruijin Hospital, Shanghai General Hospital and Shanghai Ninth People’s Hospital. Signed informed consent was obtained from each patient.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. All data generated that are relevant to the results presented in this article are included in this article. Other data that were not relevant for the results presented here are available from the corresponding author, WZ, upon reasonable request.