Article Text

Abstract
Background Lutathera is a 177Lutetium-labeled somatostatin analog approved for the treatment of gastroenteropancreatic neuroendocrine tumors (NETs). Somatostatin receptors are expressed in small cell lung cancer (SCLC). Nivolumab, an anti-PD-1 antibody, may act synergistically with lutathera to generate antitumor immunity. We conducted a phase I study of lutathera plus nivolumab in patients with advanced NETs of the lung.
Methods Patients with relapsed/refractory extensive-stage SCLC (ES-SCLC), non-progressing ES-SCLC after first-line platinum-based chemotherapy, or advanced grade I-II pulmonary NETs were eligible. The primary objective was to determine the recommended phase 2 dose (RP2D). The phase I portion followed a standard 3+3 design, assessing two dose levels (dose level 1: lutathera 3.7 GBq every 8 weeks for four doses with nivolumab 240 mg every 2 weeks; dose level 2: lutathera 7.4 GBq every 8 weeks for four doses with nivolumab 240 mg every 2 weeks).
Results Nine patients were enrolled (six ES-SCLC, two pulmonary atypical carcinoid, one high-grade pulmonary neuroendocrine carcinoma). No dose-limiting toxicities (DLTs) were observed at dose level 1. At dose level 2, one patient with refractory ES-SCLC developed a DLT (grade 3 rash). The most common treatment-related adverse events (TRAEs) were lymphopenia (n=7), thrombocytopenia (n=4), anemia (n=3), and nausea (n=3). The most common grade 3 TRAE was lymphopenia (n=4). Among the seven patients with measurable disease, one patient with ES-SCLC had a partial response. Two patients with pulmonary atypical carcinoid had stable disease lasting 6 months. The RP2D was dose level 2.
Conclusions Lutathera plus nivolumab was well tolerated and showed signs of antitumor activity. This combination warrants further exploration.
Trial registration number NCT03325816
- lung neoplasms
- drug therapy, combination
- immunotherapy
- radioimmunotherapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Small-cell lung cancer (SCLC) is one of the most lethal cancers with a 5-year overall survival (OS) rate of 6.5%.1 About two-thirds of patients present with extensive-stage SCLC (ES-SCLC) at diagnosis. Despite initial responsiveness to front-line therapy, most patients with ES-SCLC relapse and die from their disease. Few effective treatment options for ES-SCLC exist and there is an unmet need for novel therapeutics.
The expression of somatostatin receptors has been demonstrated in SCLC cell lines2 and human SCLC samples.3 Imaging studies using somatostatin receptor scintigraphy and positron emission tomography (PET)/CT also demonstrated presence of somatostatin receptors in SCLC.4–6 Lutathera is a beta-emitting 177Lutetium-labeled somatostatin analog that targets somatostatin receptor expressing cells and is approved for the treatment of gastroenteropancreatic neuroendocrine tumors (GEP-NETs).7 Nivolumab is a humanized anti-PD-1 monoclonal antibody interfering with the inhibitory programmed death (PD)-1/PD-L1 pathway and is approved for ES-SCLC in the third-line setting based on durable responses seen in a fraction of patients with ES-SCLC.8 The role of combination radiotherapy and cancer immunotherapy is emerging.9 Radiation therapy can cause the release of tumor antigens and convert tumors into an in situ vaccine.10 It can also induce the expression of chemokines promoting the recruitment of T cells into the tumor and increase the expression of death receptors, MHC class I proteins, and costimulatory molecules on tumor cells.10 These responses may augment antitumor effects of anti-PD-1 monoclonal antibody therapy.
We hypothesized that nivolumab in combination with lutathera would act synergistically to generate antitumor immunity. Herein, we report the final results of the phase I study of lutathera and nivolumab in patients with ES-SCLC or pulmonary carcinoid.
Methods
In this single-center, open-label phase I study, we enrolled patients with either relapsed/refractory ES-SCLC, non-progressing ES-SCLC after first-line platinum-based chemotherapy, or advanced grade I-II pulmonary NETs. Eligible patients had tumor tracer uptake on 68Gallium-DOTATATE PET equal to or higher than that in normal hepatic tissue; those with ES-SCLC whose tumors had lower levels of uptake than liver were also eligible at the discretion of the principal investigator. Patients were eligible if they had an Eastern Cooperative Oncology Group (ECOG) performance status of 0–1 and adequate organ/bone marrow function. Patients with non-measurable disease were allowed. Key exclusion criteria included active autoimmune disease or other conditions requiring systemic glucocorticoid or immunosuppressive therapy, previous therapy with T cell modulating antibodies (including anti-CTLA-4, anti-PD-1, anti-PD-L1), HIV infection, or active viral hepatitis B or C. Subjects with symptomatic brain metastases were excluded but patients with asymptomatic brain metastases without steroid therapy for at least 2 weeks were eligible.
The primary objective was to determine the recommended phase 2 dose (RP2D). Dose-limiting toxicity (DLT) was defined as any of the following toxicities if attributable to study treatment: grade 2 thrombocytopenia, any grade 3 or 4 toxicity (with the exception of controlled grade 3 diarrhea, nausea, vomiting, or endocrinopathy), persistent (>21 days) non-hematologic grade 2 adverse events (AEs) despite optimal medical management, clinically relevant and/or unacceptable toxicity judged to be a DLT by the investigator, toxicity resulting in a protocol defined stopping criterion, or toxicity resulting in disruption of dosing schedule. DLT was assessed during cycle 1 (8 weeks). The RP2D was defined as the dose in which ≤2 out of 6 patients developed a DLT. An exploratory analysis was performed to assess the correlation between uptake of 68Gallium-DOTATATE and somatostatin receptor 2 (SSTR2) expression in archival tumor tissue. The correlation between baseline SUVmax values on 68Gallium-DOTATATE PET and 18F-fluorodeoxyglucose (FDG)-PET was also assessed.
The standard 3+3 design was used for dose escalation. Two dose levels were assessed (dose level 1: lutathera 3.7 GBq every 8 weeks for four doses with nivolumab 240 mg every 2 weeks; dose level 2: lutathera 7.4 GBq every 8 weeks for four doses with nivolumab 240 mg every 2 weeks). The first dose of lutathera was given 2 weeks after the first administration of nivolumab (figure 1). As amino acid infusion was shown to have renoprotective effects,11 an infusion of amino acids was started 30 min before the administration of 177Lu-DOTA0-Tyr3-Octreotate and infused over 4 hours. Tumor imaging was performed every 8 weeks. Response was evaluated using the Response Evaluation Criteria in Solid Tumors (RECIST) V.1.1. 68Gallium-DOTATATE PET was obtained on cycle 2 day 1 (±3 days) to assess the metabolic response. PET with 18F-FDG was obtained at baseline.
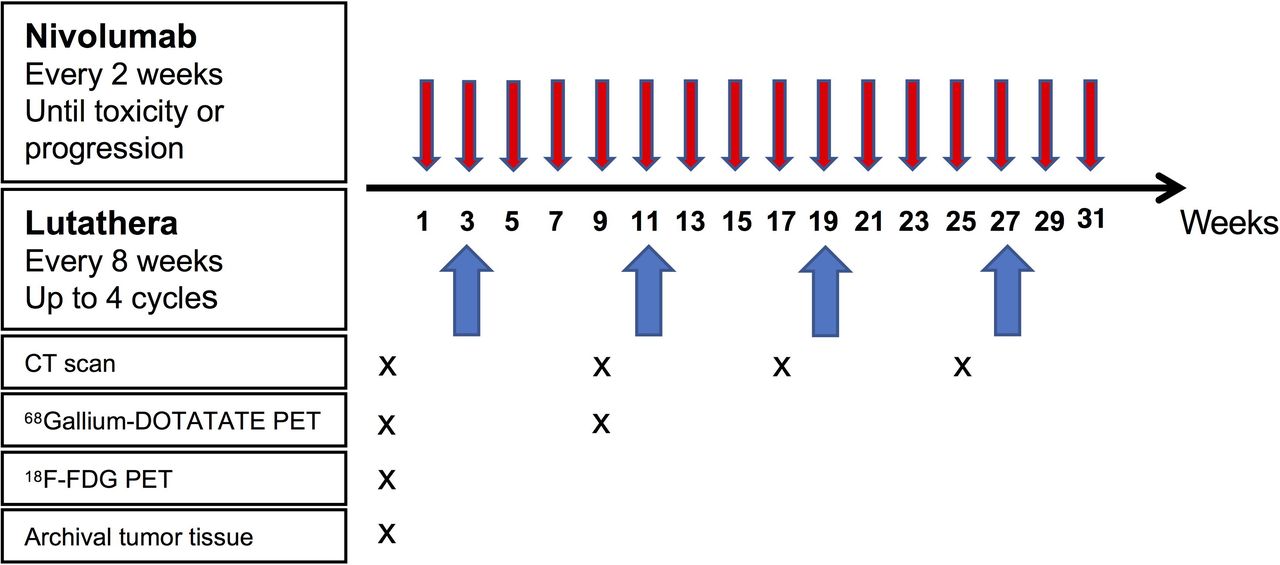
Study schema.
The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines as defined by the International Conference on Harmonization. Patients provided written informed consent form before screening and initiation of treatment.
Archival tumor tissue was obtained from study participants and analyzed for expression of PD-L1 and SSTR2. PD-L1 expression was assessed using PD-L1 IHC 22C3 pharmDx (Dako). SSTR2 was assessed using the polyclonal anti-somatostatin from Dako (Agilent Technologies).
Descriptive statistics were used to summarize primary and exploratory outcome measures. The safety profile of the combination was assessed in all treated patients through summaries of DLTs and AEs. The correlation between baseline SUVmax values on 68Gallium-DOTATATE and FDG-PET was analyzed using Spearman’s rank correlation. The database lock date was April 9, 2019.
Results
Patient characteristics
Baseline patient characteristics are presented in table 1. A total of nine patients were enrolled (5 female, 4 male). The median age at enrollment was 61 (range: 46–70). Six (66.7%) patients had ES-SCLC, two (22.2%) had metastatic atypical carcinoid of pulmonary origin, and one (11.1%) patient had high-grade neuroendocrine carcinoma of pulmonary origin. Among the six patients with ES-SCLC, one had refractory ES-SCLC, four had relapsed ES-SCLC, and one had stable disease (SD) after first-line platinum-doublet chemotherapy. Two (22.2%) patients had brain metastases at study entry which were previously treated with radiotherapy. The median follow-up time was 6.8 months.
Patient characteristics
Evidence of SSTR2 on 68Gallium-DOTATATE PET
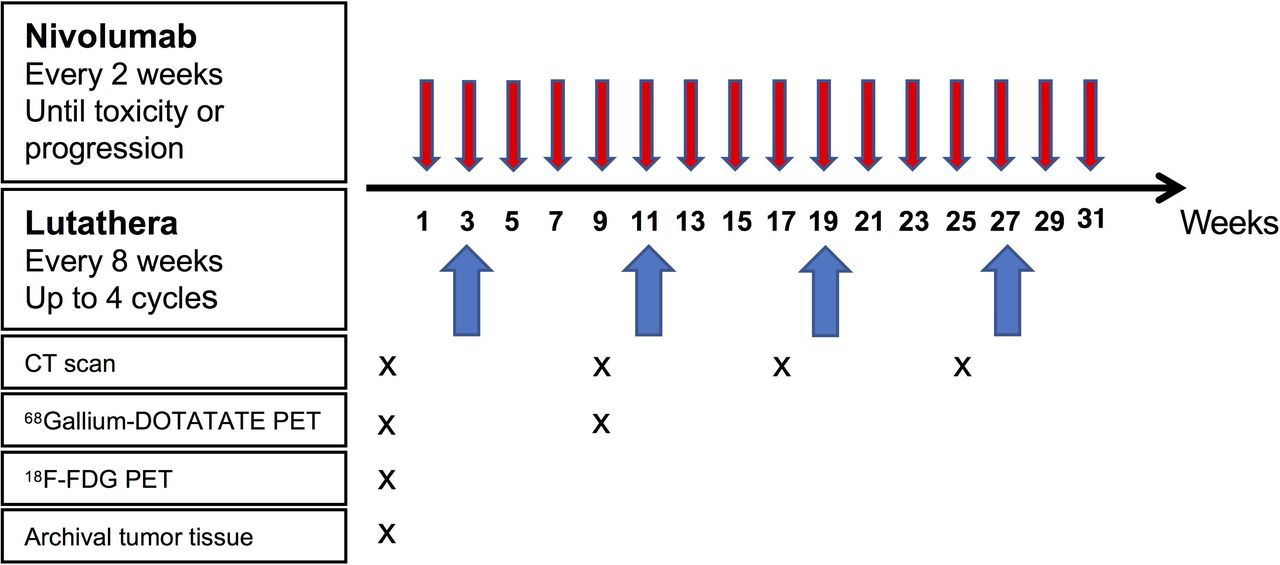
Among the seven patients with high-grade neuroendocrine carcinomas (six SCLC, one high-grade pulmonary neuroendocrine carcinoma), five (71.4%) patients had detectable SSTR2 visualization on 68Gallium-DOTATATE PET (figure 2), and in two patients, the scan was negative (online supplementary figure 1). The degree of SSTR2 positivity was variable among patients and there was intertumoral heterogeneity in 68Gallium-DOTATATE uptake within an individual patient. Patients with atypical carcinoid had tracer uptake in tumors but there were lesions without 68Gallium-DOTATATE uptake, suggesting intertumoral heterogeneity in SSTR2 expression (online supplementary figure 2).
Supplemental material
Supplemental material

In patient 1, there is increased gallium-68 DOTATATE (SUVmax=9.3) and fluorodeoxyglucose (FDG) uptake (SUVmax=19.8) in the right hepatic lobe lesion (A, B). A lesion in the left upper lobe shows faint activity on gallium-68 DOTATATE positron emission tomography (PET) (C) and mild activity on FDG PET (D). In patient 2, the left upper lobe mass exhibits higher uptake on gallium-68 DOTATATE PET (SUVmax=46.8) compared with FDG PET (SUVmax=10.0) (E, F). In patient 3, abnormal radiotracer uptake in the right lower lobe mass was noted on both gallium-68 DOTATATE and FDG PET (SUVmax=20.0 and 11.5, respectively) (G, H). Similarly, the right hepatic lesion was avid on both scans (SUVmax=20.0 and 14.9, respectively) (I, J). In patient 5, left hilar lymphadenopathy had uptake of gallium-68 DOTATATE (SUVmax=16.31) and FDG (SUVmax=5.5) (K, L). In patient 6, left lung mass had faint activity on gallium-68 DOTATATE PET (SUVmax=7.9), while FDG PET demonstrated high uptake (SUVmax=29.9) (M, N).
PD-L1 and SSTR2 expression in tissue and uptake of 68Gallium-DOTATATE and FDG on PET
Tumor tissue was available from eight patients (table 2). Tumor PD-L1 expression was positive (defined as tumor proportion score ≥1%) in two patients with ES-SCLC and negative in the rest of the patients. SSTR2 expression was positive (defined as tumor proportion score ≥1%) in four patients (one ES-SCLC, one high-grade neuroendocrine carcinoma, two pulmonary atypical carcinoid) and negative in other patients. There was discrepancy between tissue SSTR expression and 68Gallium-DOTATATE uptake. For instance, three patients with strong 68Gallium-DOTATATE uptake (patients 2, 3, 5) did not have SSTR2 expression in tissue and three patients with strong tissue SSTR2 expression (patients 6, 7, 8) had negative or mild 68Gallium-DOTATATE uptake on PET. There was no correlation between SUVmax values on 68Gallium-DOTATATE PET and FDG PET (data not shown).
Expression of PD-L1 and SSTR2 and uptake of 68Gallium-DOTATATE and FDG on PET
Safety
No DLTs were observed in three patients treated at dose level 1. Among the six patients treated at dose level 2, one patient developed a DLT (grade 3 rash). The patient was treated with topical and systemic corticosteroids with improvement of symptoms. The majority of TRAEs were grade 1 or 2 (77%) (table 3). Five (55.6%) of nine patients developed grade 3 TRAEs. The most common grade 3 TRAE was lymphopenia (n=4), followed by rash (n=1), pneumonitis (n=1), anemia (n=1), and thrombocytopenia (n=1). There were no grade 4 or 5 TRAEs. Four (44.4%) of nine patients developed immune-related AEs which included grade 1 hyperthyroidism followed by grade 2 hypothyroidism (n=1), grade 1 rash (n=1), grade 3 rash (n=1), and grade 3 pneumonitis (n=3).
Treatment-related adverse events (TRAEs) (n=9)
Efficacy
Two patients were non-evaluable for response because they did not have measurable disease. Among the seven evaluable patients, the overall response rate was 14.3% (table 4). One (14.3%) patient with non-progressing ES-SCLC after first-line platinum chemotherapy had a confirmed partial response, 2 (28.6%) patients with atypical carcinoid had SD as best response, and 4 (57.1%) patients had progressive disease (PD) as best response. The patient (patient 2) who achieved a partial response (figure 3A,B) had avid uptake of tumors on 68Gallium-DOTATATE PET (figure 3C). A reduction in uptake was noted on cycle 2 day 1 68Gallium-DOTATATE PET (figure 3D). Tumor expression of PD-L1 as well as SSTR2 assessed on archival lung tissue obtained at the time of initial diagnosis was negative. The patient had progression in the brain 4 months after study initiation. One of the patients with atypical carcinoid (patient 7) who completed 4 cycles of lutathera had progression in the liver where the lesions had poor 68Gallium-DOTATATE uptake, while the other lesions were stable. Of note, SSTR2 expression on archival liver tissue obtained at initial diagnosis was 60%. The other patient with atypical carcinoid (patient 4) received three cycles of lutathera before progression. SSTR2 expression on archival lung tissue obtained at initial diagnosis was 10%.
Summary of response to study treatment

{kind=link}
{kind=link}
{kind=link}
In a patient who achieved a partial response (study ID #2), baseline gallium-68 DOTATATE positron emission tomography (PET) shows avid uptake in tumors (A). The target lesion (right perihilar mass) was decreased in size with study treatment (A, B) and the uptake of gallium-68 DOTATATE was reduced (C, D).
When the response of each target lesion was assessed in relation to its SUVmax on 68Gallium-DOTATATE PET, no lesions without uptake of 68Gallium-DOTATATE exhibited reduction in size (online supplementary table 1).
Supplemental material
Discussion
In this phase I study of lutathera and nivolumab in patients with ES-SCLC and pulmonary atypical carcinoid, the combination was well tolerated with most TRAEs being grade 1 or 2. Only one patient had a DLT (grade 3 rash) which was attributed to nivolumab. Of note, lymphopenia was the most common grade 3 AE in our study, which has also been described in other studies of peptide receptor radionuclide therapy (PRRT) in patients with NETs.12 13 SSTR2 is overexpressed on B cells and PRRT can result in transient selective depletion of B cells.13 Given the relative sparing of T cells after PRRT, lutathera is unlikely to have a negative impact on the activity of anti-PD-(L)1 therapy.
Lutathera combined with nivolumab showed signs of antitumor activity, although no definitive conclusion about the efficacy can be drawn due to the small number of study patients. Notably, the patient who achieved a partial response had strong uptake of 68Gallium-DOTATATE in tumors, suggesting that the strong uptake of 68Gallium-DOTATATE may predict efficacy. Other studies also suggested that the degree of 68Gallium-DOTATATE uptake is associated with clinical outcomes in patients with NETs.14 15 Together, these results provide proof of concept that targeting SCLC with lutathera in combination with anti-PD-(L)1 therapy may be a viable therapeutic strategy.
Our study demonstrates that 68Gallium-DOTATATE PET can be used to visualize tumor uptake of radioligand with a predominant affinity for SSTR2 in patients with previously treated SCLC, enabling selection of patients potentially suitable for PRRT-based treatment. Of note, there was intrapatient and interpatient heterogeneity in uptake on 68Gallium-DOTATATE PET, as observed in other studies of SCLC.5 6 16 How the heterogeneity affects the efficacy of lutathera combined with immunotherapy will need to be evaluated in future studies.
Regarding the timing of administration of nivolumab and lutathera, we chose not to start both drugs at the same time in order to better delineate acute toxicities of the two drugs. Whether the timing of drug administration (eg, concurrent initiation of PRRT and PD-1/PD-L1 blockade) affects the treatment outcomes should be further explored.
There was no apparent relationship between SUVmax on 68Gallium-DOTATATE PET and expression of SSTR2 in archival tumor tissue in our study. Previous studies showed moderate to strong correlation between somatostatin receptor expression and SUVmax on 68Gallium-DOTATATE PET.5 17 18 We used archival tissue for SSTR2 expression and we cannot rule out that SSTR2 expression might have changed under therapeutic pressure. Other potential reasons for this discrepancy include the use of polyclonal antibody in our study which is subject to batch-to-batch variability affecting the staining results19 and binding of 68Ga-DOTATATE to SSTR receptors other than SSTR2. The contribution of the latter possibility to the discrepancy between SUVmax on 68Gallium-DOTATATE PET and tissue SSTR2 expression is expected to be minimal because of the high specificity of 68Ga-DOTATATE to SSTR2.20
Our study shows no apparent relationship between SUV values of 68Gallium-DOTATATE PET and FDG-PET. Prior studies have also shown no consistent findings between 68Gallium-DOTATATE PET and FDG-PET across different histologic grades in patients with NETs.21 A recent study suggests that SSTR2 signaling may play a role in tumor growth and survival in SCLC,22 but at the same time, more aggressive and undifferentiated tumors may lose expression of SSTR2. Given this consideration and the presence of multiple other pathways driving tumorigenesis in SCLC, the relationship between SSTR2 expression and the rate of tumor growth (reflected by uptake of 68Gallium-DOTATATE and 18F-FDG, respectively) is unlikely to be straightforward.
Since the inception of this study, the landscape of treatment in ES-SCLC has changed to incorporate PD-L1 inhibitor therapy in the first-line setting. Atezolizumab, an anti-PD-L1 inhibitor, plus carboplatin and etoposide was approved by the US Food and Drug Administration in patients with untreated ES-SCLC based on a randomized phase III trial demonstrating improved OS.23 Similarly, durvalumab, another anti-PD-L1 inhibitor, was shown to improve OS when added to platinum-based chemotherapy in patients with ES-SCLC.24 While the improved outcomes observed with addition of PD-L1 targeting therapy to chemotherapy is encouraging, the OS benefit was modest and there remains an unmet need to develop novel therapies in patients with ES-SCLC.
Based on our results, further studies of lutathera in combination with immune checkpoint inhibitors are warranted, potentially as a maintenance strategy.
Conclusions
In conclusion, this study provides proof of concept that somatostatin receptor expressing SCLC could be targeted using lutathera containing therapy and that the combination with nivolumab is safe. Additional studies are needed to further elucidate the potential role of somatostatin receptor targeting therapies in patients with SCLC.
References
Footnotes
Twitter @chulkimMD, @StephenVLiu
Contributors Provision of study materials or patients: All authors. Collection and assembly of data: all authors. Data analysis and interpretation: all authors. Manuscript writing: all authors. Final approval of manuscript: all authors. All authors read and approved the final manuscript.
Funding Research funding was provided by Advanced Accelerator Applications and Bristol-Myers Squibb.
Competing interests CK has received research grants (to institution) from AstraZeneca, BMS, Novartis, Regeneron, Tesaro, Karyopharm, Debiopharm, and Altor Bioscience, and has served on the advisory board of Novartis. SVL has received research grants (to institution) from Alkermes, AstraZeneca, Bayer, Blueprint, Bristol-Myers Squibb, Corvus, Genentech, Ignyta, Lilly, Lycera, Merck, Merus, Molecular Partners, Pfizer, Rain Therapeutics, RAPT, Spectrum, and Turning Point Therapeutics. He has served on the advisory board of AstraZeneca, Bristol-Myers Squibb, Catalyst, Celgene, G1 Therapeutics, Genentech/Roche, Guardant Health, Ignyta, Janssen, Lilly, LOXO, PharmaMar, Regeneron, and Takeda. DSS is an employee of AstraZeneca and has stock options with AstraZeneca starting July 29, 2019. DSS was on the speaker’s bureau of AstraZeneca, Genentech, and Takeda Oncology, and was on the advisory board of AstraZeneca. GE is on the speaker’s bureau of Advanced Accelerator Applications. The other authors declare no potential conflicts of interest.
Patient consent for publication Not required.
Ethics approval The study protocol and consent were approved by the Georgetown University Institutional Review Board. Informed consent to participate in the trial was obtained from patients.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.