Article Text

Abstract
Introduction Hepatocellular carcinoma (HCC) is the fourth leading cause of cancer-associated mortality globally. Immune-checkpoint blockade (ICB) is one of the systemic therapy options for HCC. However, response rates remain low, necessitating robust predictive biomarkers. In the present study, we examined the expression of CD38, a molecule involved in the immunosuppressive adenosinergic pathway, on immune cells present in the tumor microenvironment. We then investigated the association between CD38 and ICB treatment outcomes in advanced HCC.
Methods Clinically annotated samples from 49 patients with advanced HCC treated with ICB were analyzed for CD38 expression using immunohistochemistry (IHC), multiplex immunohistochemistry/immunofluorescence (mIHC/IF) and multiplex cytokine analysis.
Results IHC and mIHC/IF analyses revealed that higher intratumoral CD38+ cell proportion was strongly associated with improved response to ICB. The overall response rates to ICB was significantly higher among patients with high proportion of total CD38+cells compared with patients with low proportion (43.5% vs 3.9%, p=0.019). Higher responses seen among patients with a high intratumoral CD38+cell proportion translated to a longer median progression-free survival (mPFS, 8.21 months vs 1.64 months, p=0.0065) and median overall survival (mOS, 19.06 months vs 9.59 months, p=0.0295). Patients with high CD38+CD68+macrophage density had a better mOS of 34.43 months compared with 9.66 months in patients with low CD38+CD68+ macrophage density. CD38hi macrophages produce more interferon γ (IFN-γ) and related cytokines, which may explain its predictive value when treated with ICB.
Conclusions A high proportion of CD38+ cells, determined by IHC, predicts response to ICB and is associated with superior mPFS and OS in advanced HCC.
- macrophages
- immunotherapy
- liver neoplasms
- adenosine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Hepatocellular carcinoma (HCC) is the fifth and ninth most frequently diagnosed cancer in adult males and females, respectively, and the fourth leading cause of cancer-associated mortality in the world.1 Cirrhosis, a major risk factor for HCC, is often caused by chronic hepatitis B or C infection in Asia. Surgical resection and liver transplantation are potentially curative treatment options available for early-stage HCC. However, 5-year survival rates following surgical resection remain relatively low for early stage disease (17%–53%), with recurrence rates as high as 70%.2–4 Survival rates among patients with advanced HCC also remain challenging in the clinical practice.
At present, the multikinase targeted inhibitors, sorafenib and lenvantinib are used as first-line therapy for advanced HCC.5 6 These drugs primarily act through the inhibition of vascular endothelial growth factor. Another relatively recent addition to the HCC treatment armamentarium is immunotherapy, which uses antibodies to target specific checkpoint molecules such as cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4), programmed cell death protein-1 (PD-1) and programmed death-ligand 1 (PD-L1). The efficacy and safety of nivolumab in patients with HCC, which targets PD-1, were explored in a phase I/II trial (CheckMate 040). The preliminary results of this trial were promising, and resulted in the accelerated Food and Drug Administration approval of nivolumab treatment for patients with HCC who had previously been treated with sorafenib.7 8 However, the response rate of patients within phase I/II trials remains low, with only ~20% of participants responding to treatment. Moreover, a subsequent phase III study did not meet its primary endpoint of demonstrating increased survival benefit compared with oral sorafenib.9 A number of different biomarkers have been proposed to identify patients with other malignancies who are likely to benefit from immune-checkpoint blockade (ICB), including PD-L1 expression,10–12 tumor mutation burden, microsatellite instability and interferon γ (IFN-γ) gene signature. However, there are few robust predictive biomarkers available in HCC, with the use of a PD-L1 expression being of limited value.7 8 Thus, the perusal of the wider HCC tumor microenvironment (TME) has become imperative, if we hope to identify any novel, robust biomarkers.
One molecule of particular interest in the TME is CD38, which structurally resembles CD1a and, among other functions, serves as an ectozyme in the adenosinergic pathway.13 In the hypoxic TME, NAD+ is released by the salvage pathway and hydrolyzed by CD38 to form ADP ribose. This is further degraded to AMP through the CD38–CD203a–CD73 pathway. Following this, CD73 dephosphorylates AMP to adenosine.14 15 Accumulated extracellular adenosine then binds to receptors on a range of immune cells, impeding their infiltration and activation.16 17 This pathway forms an alternative immunosuppressive mechanism to the PD-1/PD-L1 pathway, and inhibition of the adenosine pathway has been shown to reduce immunosuppression in the TME.18 19 Furthermore, reversal of hypoxia via oxygen supplementation in a murine model resulted in a significant reduction of solid tumor growth and metastasis.20 Similarly, PD-1 blockade and adenosine receptor inhibitor cotreatment has been found to improve the immune response and result in increased tumor suppression in a range of mouse models.21–23 In addition to its role as an ectozyme, CD38 also functions as a surface membrane marker in various immune cells and non-lymphoid tissues.24
The relevance of CD38 to HCC in particular was established in a recent study by our group, which found a correlation between CD38+ tumor-infiltrating leukocyte density and improved prognosis.25 26 CD38 expression has been reported in a range of immune cell populations,24 but data regarding its expression by macrophages are limited. Our group recently reported that the presence of macrophages expressing both CD38 and CD68 in the TME is associated with improved prognosis after surgical resection in HCC; but notably, CD68+ macrophage density was associated with poor prognosis.27 This may indicate the presence of various macrophage subsets with different functions in the TME. For example, CD38 is known to be highly expressed by M1 macrophages, which produce large amounts of proinflammatory cytokines such as interleukin-6 (IL-6) and TNF-α.27 This may explain the association between these cells and improved prognosis.
In this present study, we further confirmed the expression of CD38 on immune cells present in HCC tissues. Following this, we determined whether increased expression of CD38+ by immune infiltrates, and particularly by macrophages in the TME, is associated with response to ICB in a cohort of Asian patients with advanced HCC (n=49). We propose that this IHC-based technique, which is easily transferrable to clinical diagnostic laboratories, should be adopted in clinical practice in the near future to more accurately identify those patients with HCC likely to benefit from immunotherapy.
Materials and methods
Patients and tumors
A total of 49 archival, formalin-fixed, paraffin-embedded (FFPE) specimens, taken from Asian patients with advanced HCC who received ICB therapy between January 2015 and December 2018 at the Division of Medical Oncology, National Cancer Centre, Singapore, were evaluated. All samples were intrahepatic resection or biopsy samples and were obtained prior to immunotherapy at the Department of Anatomical Pathology, Division of Pathology, Singapore General Hospital. Clinicopathological parameters are summarized in table 1, and further details for individual patients are presented in online supplementary table 1.
Supplemental material
Clinicopathological characteristics of patients included in the cohort
We further categorized the patients into three groups based on their treatment regimen: patients treated with (1) PD-1 or PD-L1 inhibitors only (n=30), (2) combination PD1 or PD-L1 inhibitors with CTLA-4 inhibitors (n=13) and (3) combination of PD-1 or PD-L1 inhibitors with other treatments (n=6). We analyzed the data based on all patients from the aforementioned groups (groups 1–3, n=49), termed ‘patients treated with PD-1/PD-L1 ICB therapy’. We also analyzed the data based on a subgroup (groups A, n=30), termed ‘patients treated with anti-PD-1/PD-L1 single agent therapy’.
For all patients, tumors were staged and graded according to BCLC staging system28 and Edmondson-Steiner grading system.29 The Centralized Institutional Review Board of SingHealth provided ethical approval for the use of patient materials in this study (CIRB ref: 2014/590/B).
Immunohistochemistry (IHC)
IHC was performed on the FFPE tissue samples as previously described.30–32 Tissue sections (4 µm thick) were labeled with antibodies targeting CD38 and PD-L1, as listed in online supplementary table 2. Appropriate positive and negative controls were included. To score the antibody-labeled sections, images were captured using an IntelliSite Ultra-Fast Scanner (Philips, Eindhoven, the Netherlands). The percentage of cells displaying unequivocal staining of any intensity for CD38 and PD-L1 were determined by two pathologists blinded to clinicopathological and survival information (JY and SS). PD-L1 tumor proportion score (TPS) was calculated as previously reported.7 Where discordant, the cases were reviewed and a consensus score was given.
Multiplex immunohistochemistry/immunofluorescence (mIHC/IF) analysis
mIHC/IF was performed using an Opal Multiplex fIHC kit (PerkinElmer, Inc, Waltham, Massachusetts, USA), as previously described by our group and in other studies.25 31–52 Tissue sections (4 µm thick) were labeled with primary antibodies against CD38, CD8 and CD68, followed by appropriate secondary antibodies. All antibodies used are listed in online supplementary table 2. This was followed by the application of a fluorophore-conjugated tyramide signal amplification buffer (PerkinElmer, Inc) and the nuclear counterstain DAPI. A Vectra three pathology imaging system microscope (PerkinElmer, Inc) was used to obtain images, and these were analyzed using inForm software (V.2.4.2; PerkinElmer, Inc)34 47 53 54 and HALO TM (Indica Labs, Albuquerqe, New Mexico, USA).55–59
The density of CD38+CD68+ macrophages and CD8+ T cells were determined as follows: cell count per predefined, high-powered field (334 μm × 250 μm) represents the density of CD38+CD68+ macrophages and CD8+ T cells in the TME. Samples were then categorized as ‘high’ or ‘low’ according to whether the CD38+CD68+ macrophage and CD8+ T cell count was above the cut-off points (best thresholds) that produced the lowest p value, which were determined using previously described methods.25 31 32 36 37 43–52 60 61
Gene and ingenuity pathway analysis (IPA)
Gene expression data were obtained from The Cancer Genome Atlas (TCGA; https://www.cancer.gov/tcga). Gene expression and survival data were obtained from cBioPortal after filtering for HCC samples.62 HCC samples were divided into ‘high’ or ‘low’ CD38 expression groups using the optimal thresholds that produced the lowest p value. IPA core analysis was performed to identify differentially expressed genes (DEGs) between HCC samples with high and low CD38 expression, using the entire list of genes from the TCGA data as the background. P<0.05 was the threshold used to identify significant gene enrichment.
Single cell gene expression
Single cell CD38 gene expression levels in the human liver were obtained from MacParland et al,63 using the author-provided web application hosted at http://shiny.baderlab.org/HumanLiverAtlas/. PDFs of CD38 expression levels, visualized using T-distributed stochastic neighbor embedding (t-SNE) dimension reduction, were generated using this web application. Cell populations identified by the authors are labeled on the plots.
Tissue dissociation and isolation of leukocytes
Liver tissue was cut into fine pieces and digested with 0.5 mg/mL Collagenase IV (Gibco; Thermo Fisher Scientific, Inc, Waltham, Massachusetts, USA) and 0.05 mg/mL DNAse I (Sigma-Aldrich; Merck KGaA, Darmstadt, Germany) in complete RPMI 1640 (Gibco; Thermo Fisher Scientific, Inc) for 30 min at 37 °C. Digested tissue was filtered using a 70 µm cell strainer. Cells were then pelleted and treated with red blood cell lysis buffer (G-Biosciences, St Louis, Missouri, USA) for 5 min at room temperature. Cell debris was removed using Debris Removal Solution, according to the manufacturer’s protocol (Miltenyi Biotec, Ltd, Bergisch Gladbach, Germany).
Flow cytometry
Cells were incubated with Fixable Viability Dye eFluor 455UV (eBioscience, Thermo Fisher Scientific, Inc) for 30 min at 4 °C for live/dead cell discrimination. Fc receptors were blocked using Human TruStain FcX (BioLegend, San Diego, California, USA) for 5 min at room temperature. Cell surfaces were labeled with antibodies targeting markers of interest (refer to online supplementary table 3 for antibody panel) for 30 min at 4 °C. Matched isotype controls were included for antibodies against CD38. Single color compensation controls were prepared using Ultracomp eBeads (eBioscience, Thermo Fisher Scientific, Inc). Samples were read in a Spectral flow cytometer Cytek Aurora (Cytek Biosciences, Fremont, California, USA). Data analysis was performed using FlowJo V.10 software (FlowJo LLC, Ashland, Oregon, USA).
THP-1 functional study in vitro
THP-1 cells were cultured and polarized based on a previously published protocol.27 64 In brief, cells were cultured in complete RPMI 1640 (Gibco, Thermo Fisher Scientific, Inc) supplemented with 10% fetal bovine serum (Gibco, Thermo Fisher Scientific, Inc), 1% penicillin/streptomycin (Gibco, Thermo Fisher Scientific, Inc), and 50 µM 2-mercaptoethanol (Gibco, Thermo Fisher Scientific, Inc). Cells were then plated in 24-well plates at a density of 5×105 cells/mL, differentiated with 50 ng phorbol myristate acetate (Sigma-Aldrich, Merck KGaA) for 24 hours, then washed and cultured in fresh medium for 48 hours. Macrophages were polarized to the M1 state with 20 ng/mL IFN-γ (R&D Systems, Inc, Minneapolis, Minnesota, USA) and 100 ng/mL lipopolysaccharide (Sigma-Aldrich, Merck KGaA), or to the M2 state with 20 ng/mL IL-4 (R&D Systems, Inc). After 24 hours, cells were harvested for flow cytometry analysis. Culture supernatant was collected for the analysis of cytokines using Luminex kits (Luminex Corporation, Austin, Texas, USA).
Multiplex cytokine analysis
A total of 65 analytes from the Immune Monitoring ProcartPlex Panel (Thermo Fisher Scientific, Inc) were measured. Assays were performed according to the manufacturer's protocol. Plates were washed using a Tecan Hydrospeed Washer (Tecan Group AG, Männedorf, Switzerland) and read with a Flexmap 3D system (Luminex Corporation). Data were analyzed using Bio-Plex manager V.6.2 software (Bio-Rad Laboratories, Hercules, California, USA) with a 5-parameter curve-fitting algorithm applied for standard curve calculations. Logarithmically transformed, averaged Luminex concentrations were standardized (mean-centered and standard deviation-scaled) by analyte and depicted as a heat map for CD38hi and CD38lo macrophage samples as defined and gated with FLOWJO (Becton, Dickinson&Company, USA) as previously described.27 Euclidean distance-based complete linkage clustering was performed for both analytes and samples. Numerical computations and heat maps were then generated using the ComplexHeatmap package in R V.3.3.1.
RNA extraction, NanoString measurement and analysis
RNA was extracted from 14 unlabeled FFPE sections (10 µm thick) using an RNeasy FFPE kit (Qiagen GmbH, Hilden, Germany) on a QIAcube automated sample preparation system (Qiagen GmbH), and was quantified using an Agilent 2100 Bioanalyzer system (Agilent Technologies, Santa Clara, California, USA). A total of 100 ng of functional RNA (> 300 nucleotides) was assayed on the nCounter MAX Analysis System (NanoString Technologies, Inc, Seattle, Washington, USA). The NanoString counts were normalized using positive control probes and the housekeeping genes, as previously reported.31 47 The count data were then logarithmically transformed prior to further analysis. P<0.05 was considered to indicate a statistically significant difference.
Validation, follow-up and statistical analysis
Patient follow-up data were obtained from medical records, and overall survival (OS) and progression-free survival (PFS) was calculated using time periods defined as from the start of treatment to either death, progression, or date of of last follow-up, respectively. We used an unpaired Mann-Whitney U test to investigate whether biomarker expression in patients, as determined by mIHC/IF, predicted their reponse to immunotherapy. The associations between clinicopathological parameters and biomarker expression were analyzed using χ² and Fisher’s exact tests. Cox regression was performed to evaluate the effects of these factors on PFS and OS. Statistical analysis was performed using RStudio 1.1.456 running R V.3.5.053, V.3.5.054 (R-core Team, R Foundation for Statistical Computing, Vienna, Austria) and GraphPad Prism V.8.0.0 for Windows (GraphPad Software, Inc, San Diego, California, USA). P<0.05 was considered to indicate a statistically significant difference.
Results
CD38 gene expression is a prognostic marker in HCC, and is associated with a proinflammatory state characterized by certain DEGs
We initially analyzed the gene expression data of a cohort of patients with HCC (n=321), taken from a publicly available database (TCGA),62 and found that increased CD38 gene expression levels were associated with an improved disease-free survival of 38 months compared with 20 months, as presented in figure 1A (p=0.005).

CD38 gene expression levels are positively correlated with improved clinical outcome and higher expression of immune gene signatures. (A) Kaplan-Meier survival analysis comparing DFS in patients with high and low CD38 gene expression levels. (B) Results of IPA, showing the enriched pathways. (C) A volcano plot showing the increase of key differentially expressed immune genes in the high CD38 expression group. DFS, disease-free survival; IPA, ingenuity pathway analysis.
IPA was then used to decipher the biological functions of the DEGs. As shown in figure 1B and online supplementary table 4, IPA core analysis identified significant functional enrichment in the expression of genes associated with the following canonical pathways: ‘Th1 and Th2 activation pathway’ (p<0.001), ‘Communication between innate and adaptive immune cells’ (p<0.001) and ‘iCOS-iCOSL Signaling in T Helper Cells’ (p<0.001). Furthermore, IPA upstream regulator analysis also revealed that the TNF, IL-10, IL-2 and IL-4 genes were enriched (p<0.001). This can be attributed to the Th1 and Th2 activation pathways, as well as communication between innate and adaptive immunity. Other canonical pathways, ‘Granulocyte Adhesion and Diapedesis’, ‘Th1 Pathway’ and ‘Th2 Pathway’ were also found to be enriched (p<0.001), warranting further investigation in future studies.
Notably, as presented in the volcano plot (figure 1C and online supplementary figure 1), the CD3 and CD8 genes, along with PD-L1 (CD274), PD-L2 (PDCD1LG2), IFNG, GZMK, IL2R and TIGIT, were enriched. These genes reflect the level of T cell infiltration. Genes that indicated myeloid cell accumulation, such as CD68, CD163, SINGLEC5, HLA-DRB1, HLA-DQA2, IDO, BATF3, CD1C, and CD1A, were also highly expressed in the high CD38 gene expression group.
Macrophages and other myeloid immune cells express CD38 in HCC
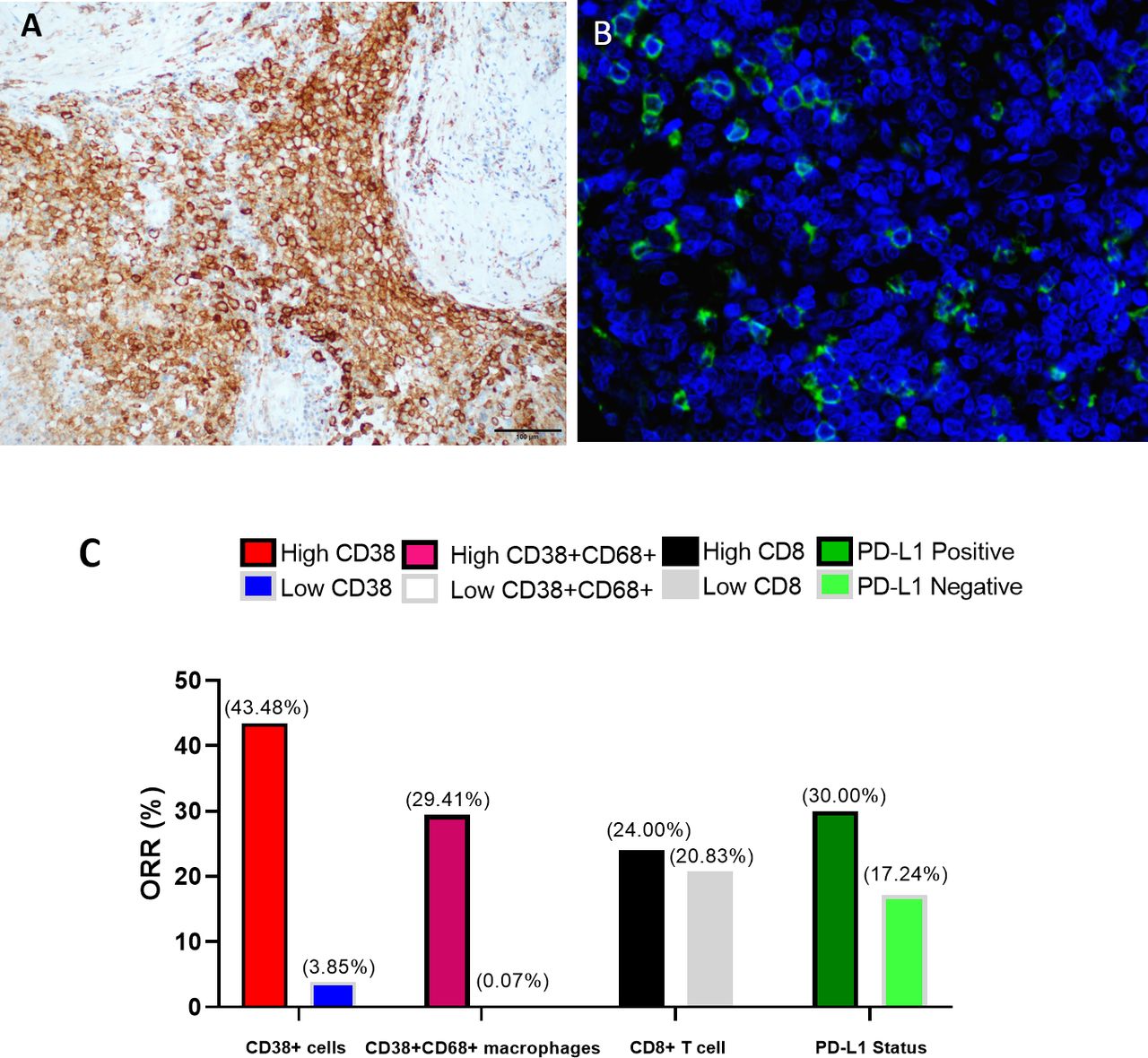
We then sought to verify the expression of CD38 by tumor cells and different immune infiltrates in our HCC samples (n=49). First, we visualized the HCC samples using conventional IHC, and found that while some HCC samples had a relatively low number of CD38+ cells (figure 2A), these cells were abundant in other samples (figure 2B). Next, we examined the samples that harbored relatively high numbers of CD38+ cells using mIF/mIHC, and found a high level of colocalization between CD38 and CD68 (figure 2C), indicating that CD38 is expressed by macrophages.
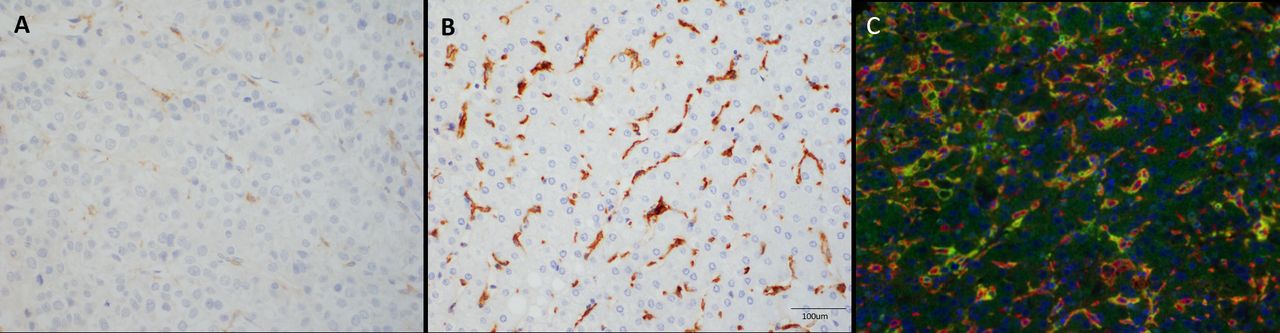
CD38 expression in the HCC TME, as visualized using IHC and mIHC/IF. Representative, conventional IHC images of tumors with (A) a low proportion of total CD38+ cells, and (B) a high proportion of total CD38+ cells. Cells expressing CD38 in the HCC TME are stained brown. The cells are irregularly shaped with numerous cytoplasmic extensions. Cell nuclei are counterstained with hematoxylin for IHC (blue). (C) mIHC/IF revealed that CD38 (green) and the macrophage marker CD68 (red) were also expressed in the HCC TME. CD68 is often colocalized with CD38 (green) in the HCC TME. Cell nuclei are counterstained with DAPI for mIHC/IF (blue Images are shown at a magnification of 400× for A, B, and C. HCC, hepatocellular carcinoma; IHC, immunohistochemistry; mIHC/IF, multiplex immunohistochemistry/immunofluorescence; TME, tumor microenvironment.
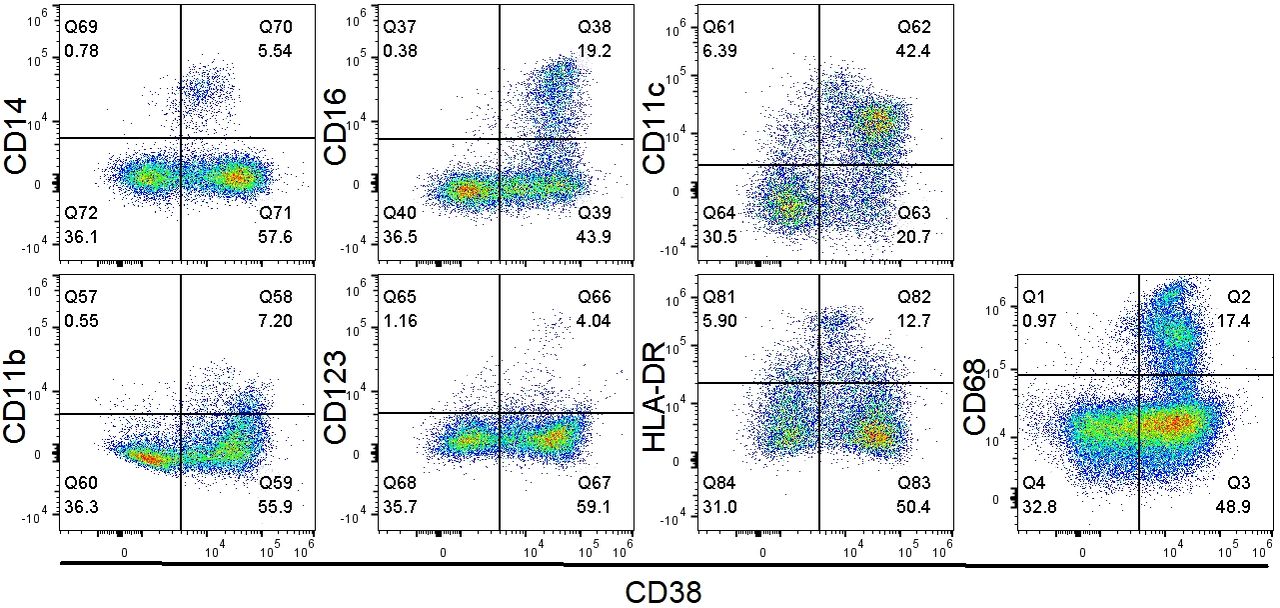
Notably, using a publicly available, single cell RNA sequencing human liver dataset,63 we also found that the CD38 gene is primarily expressed by macrophages and immune cells such as plasma and natural killer (NK) cells, compared with hepatocytes and stromal cells (online supplementary figure 2). This finding is in line with those from recent reports by our group.27 We then used flow cytometry to validate CD38 expression by immune cells in our HCC samples, as shown in figure 3. As expected, CD38 was expressed by monocyte, macrophage and dendritic cell populations, including CD14+ cells, CD16+ cells, CD11b+ cells, CD11c+ cells, CD68+ cells and CD123+ cells. These results are in line with those of previous publications,25 65 including our recent findings.27

CD38 expression in macrophages in HCC tissues was validated using flow cytometry. Flow cytometry analysis of CD38 expression on macrophages present in HCC tissue. The representative pseudocolor plots of selected macrophage markers (CD14, CD16, CD11c, CD11b, CD68, CD123, HLA-DR) were gated from the total single live cell population. HCC, hepatocellular carcinoma.
Total CD38 cell proportion predicts response to immunotherapy in HCC, as demonstrated by IHC
Next, we investigated whether the presence of CD38+ cells on the FFPE tissues taken from our patients with advanced HCC treated with ICB were predictive of response. The clinicopathological parameters of the patient cohort are listed in table 1. Responses were determined according to RECIST V.1.1.66 Patients who achieved a best response of Complete Response (CR)/Partial Response (PR) according to RECIST V.1.1 were termed responders and patients who achieved a best response of Stable Disease (SD)/Progressive Disease (PD) according to RECIST 1.1 were termed non-responders.
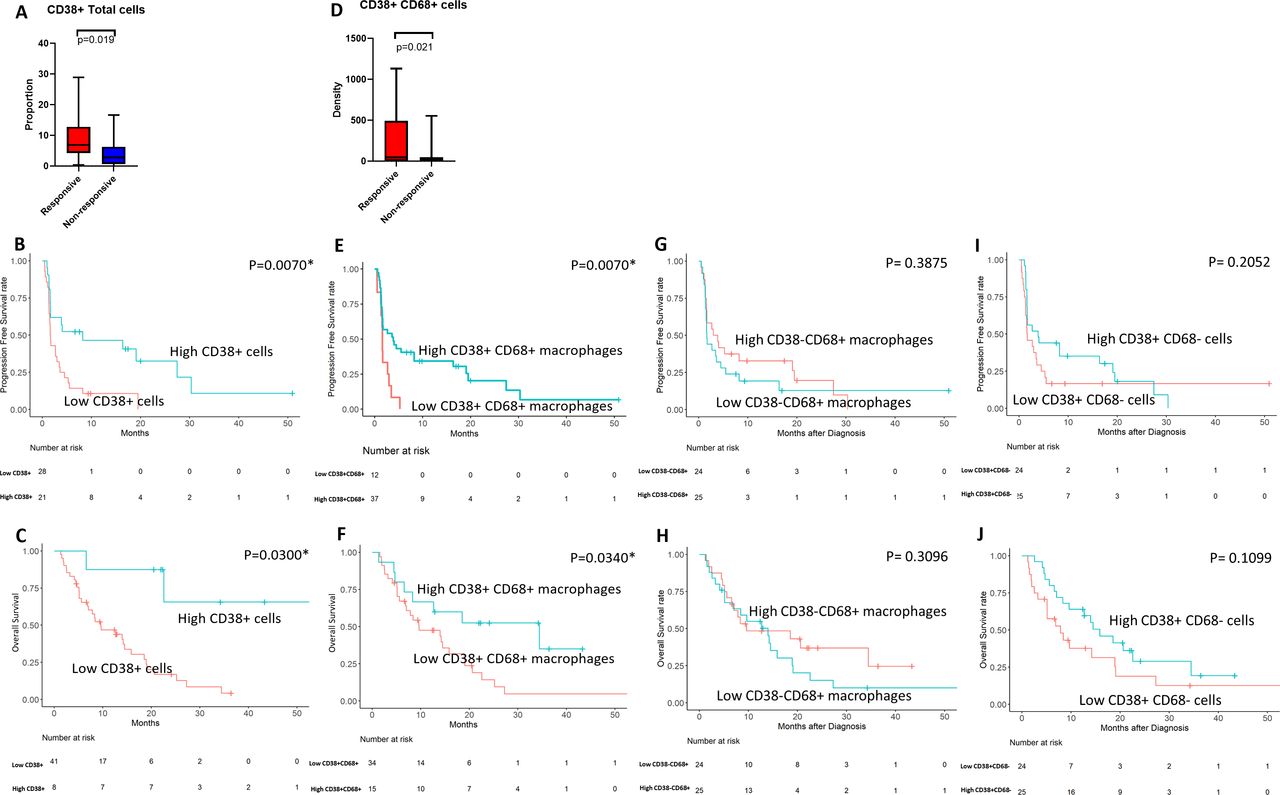
First, we studied the expression of CD38 at the protein level using conventional IHC. Using traditional manual scoring methods, as described in the Materials and methods section, we found that responders had a significantly higher proportion of intratumoral total CD38+ cells compared with non-responders (p=0.019; figure 4A). The majority of the intratumoral CD38+ cells morphologically resembled macrophages or lymphocytes, but no convincing expression of CD38 by tumor cells was observed.

Response to ICB in patients with HCC, in relation to intratumoral total CD38+ cell proportion and CD38+CD68+ macrophage density. (A) The total CD38+ cell proportion within the tumors of responders and non-responders treated with ICB. (B) Kaplan-Meier curve showing the association between a high total CD38+ cell proportion and improved PFS after treatment with ICB. (C) Kaplan-Meier curve showing the association between a high total CD38+ cell proportion and improved OS after treatment with ICB. (D) The CD38+CD68+ macrophage density of responders and non-responders treated with ICB. (E) Kaplan-Meier curve showing the association between high CD38+CD68+ macrophage density and improved PFS after treatment with ICB. (F) Kaplan Meier curve showing the association between high CD38+CD68+ macrophage density and improved OS after treatment with ICB. (G) Kaplan-Meier curve showing the association between high CD38−CD68+ macrophage density and improved PFS after treatment with ICB. (H) Kaplan-Meier curve showing the association between high CD38−CD68+ macrophage density and improved OS after treatment with ICB. (I) Kaplan-Meier curve showing the association between high CD38+CD68− cell density and improved PFS after treatment with ICB. (J) Kaplan-Meier curve showing the association between high CD38+CD68− cell density and improved OS after treatment with ICB. ICB, immune checkpoint blockade; OS, overall survival; PFS, progression-free survival.
For patients who underwent ICB therapy (n=49), an optimal cut-off for total CD38+ cell proportion can be accurately defined using receiver-operating characteristic analysis (online supplementary figure 3A). The cut-off used was 5% positivity among total immune infiltrates, and this cut-off achieved 75.5% accuracy, 71.1% specificity and 90.9% sensitivity. The area under curve was 0.785. With this cut-off, patients with a high proportion of intratumoral CD38+ immune cells achieved an overall response rate (ORR) of 43.48%, compared with 3.85% for those with a low proportion as described in the following. Patients with a high total CD38+ cell proportion experienced a superior median PFS (mPFS) of 8.21 months compared with 1.64 months in patients with low total CD38+ cell proportion (p=0.0065; HR=0.383; figure 4B; table 2). Similarly, patients harboring a high proportion of total CD38+ cells experienced a significantly better median OS (mOS) of 19.06 months, compared with 9.59 months in patients with low CD38+ cell proportion (p=0.0295; HR=0.463; figure 4C; table 3). Importantly, no other clinicopathological parameters predicted for PFS or OS.
Analysis of mPFS in patients with HCC treated with ICB (n=49)
Analysis of mOS in patients with HCC treated with ICB (n=49)
Importantly, similar survival advantage was observed in patients with high intratumoral total CD38+ cell proportion who received anti-PD-1/PD-L1 single agent treatment in this cohort (n=30/49; PFS: p=0.0253, HR=0.397; OS: p=0.0483, HR=0.418; ORR=38.46% (high), 5.88% (low); online supplementary tables 5 and 6, figure 4A,B).
Total CD38+ cell proportion and CD38+CD68+ macrophage density predicts responsiveness to ICB more accurately than PD-L1 scoring or CD8+ T cell density
Our group recently reported that a large proportion of the CD38+ cells present in HCC tissues are CD38+CD68+ macrophages (62.9%±19.2%).27 Thus, we investigated whether quantification of CD38+CD68+ macrophages in patients with HCC could be a useful predictive biomarker of response to ICB (figure 4). Using mIHC/IF, we found that a higher density of CD38+CD68+ macrophages within the tumor was significantly associated with response to ICB therapy (n=49; p=0.021; figure 4D). Notably, we found that a high CD38+CD68+ macrophage density was associated with better mPFS, 3.88 months compared with 1.61 months in patients with low CD38+CD68+ macrophage density (p=0.0072; HR=0.368; figure 4E, table 2). Most strikingly, patients harboring a high density of CD38+CD68+ macrophages experienced a significantly greater mOS of 34.43 months compared with 9.59 months in patients with low CD38+CD68+ macrophage density (p=0.0336; HR=0.416; figure 4F; table 3). However, both CD38−CD68+ macrophage density and CD38+CD68− cells density do not show any association with PFS (table 3; figure 4G,I) and OS (table 4; figure 4H,J). Furthermore, for patients who underwent ICB therapy (n=49), an optimal cut-off for CD38+CD68+ macrophages density can be accurately defined using receiver operating characteristic analysis (online supplementary figure 3B). The cut-off used was 1 cell, which achieved 71.4% accuracy.
Change in the log-likelihood of the models with added predictive terms
In addition, in the subgroup that received anti-PD-1/PD-L1 single agent treatment in this cohort (n=30/49), the association of CD38+CD68+ macrophage density with survival is also observed (PFS: p=0.0325, HR=0.381; OS: p=0.0422, HR=0.374; online supplementary tables 5 and 6, online supplementary figure 4C,D). Whereas the association is not seen for both CD38−CD68+ macrophage density and CD38+CD68− cells density (online supplementary tables 5 and 6, online supplementary figure 4E–H), suggesting the non-macrophages CD38+ immune cells (such as plasma and NK cells) as well as the CD38− macrophages might play negligible predictive and prognostic role in this cohort treated with ICB or anti-PD-1/PD-L1 single agent.
The association between the BMS 4-gene inflammatory signature and melanoma or gastroesophageal cancer treated with immunotherapy has been investigated in previous literature.67–69 Thus, to investigate this in HCC, we compared the use of CD38 as a predictive marker to two of the genes included in this signature. We assessed PD-L1 TPS with IHC (figure 5A) and CD8+ T cell density with mIHC/IF (figure 5B), and found that the ORR of the high CD38 expression group was the highest, at 43.48%. Furthermore, low CD38+CD68+ macrophage density group conferred the lowest response rate, 0.07%. This underlines the utility of CD38 as a predictive biomarker (figure 5C).Neither PD-L1 TPS nor CD8+ T cell density alone predicted PFS or OS in this cohort. However, as presented in table 4, the addition of PD-L1 TPS and CD8+ T cell density to total CD38+ cell proportion significantly increased the predictive value of this biomarker for PFS (∆LRχ2=7.86; p=0.0197), compared with total CD38+ cell proportion alone. Meanwhile, the inclusion of PD-L1 TPS and CD8+ T cell density to CD38+CD68+ macrophage density increased the predictive value for PFS (∆LRχ2=8.82; p=0.0121) compared with CD38+CD68+ macrophage density alone. However, there was no statistical significance observed in terms of OS when PD-L1 TPS and CD8+ T cell density was added to either total CD38+ cell proportion or CD38+CD68+ macrophage density.

ORR for the predictive value of CD38+ leukocyte proportion and macrophage density. (A) Representative image of PD-L1+ tumor cells (highlighted in brown) in the HCC TME. Cell nuclei are counterstained with hematoxylin for IHC (blue). (B) Representative mIHC/IF image of CD8+ T cells (highlighted in green) in the HCC TME. Cell nuclei are counterstained with DAPI for mIHC/IF (blue). (C) ORRs of each biomarker. Images are shown at a magnification of 400× for A and B. HCC, hepatocellular carcinoma; IHC, immunohistochemistry; mIHC/IF, multiplex immunohistochemistry/immunofluorescence; ORRs, overall response rates; PD-L1, programmed death-ligand 1; TME, tumor microenvironment.
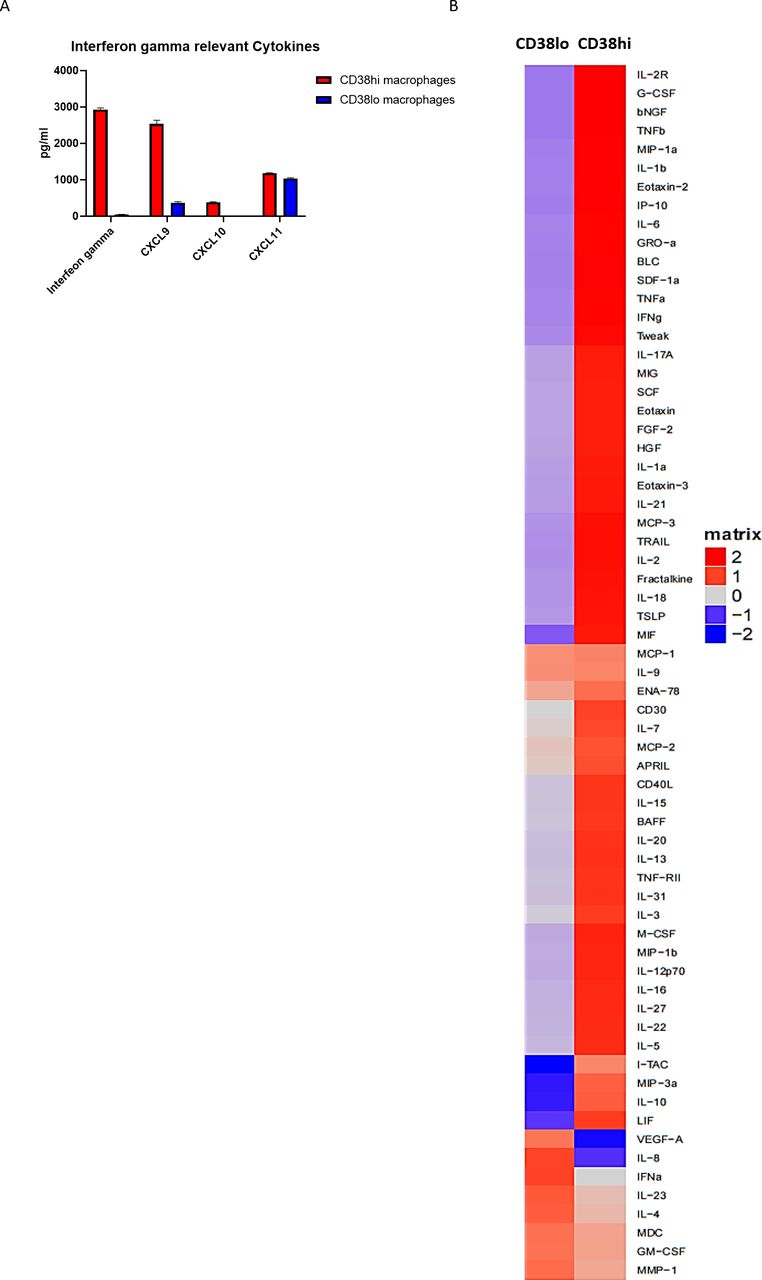
CD38hi macrophages are characterized by the secretion of proinflammatory cytokines
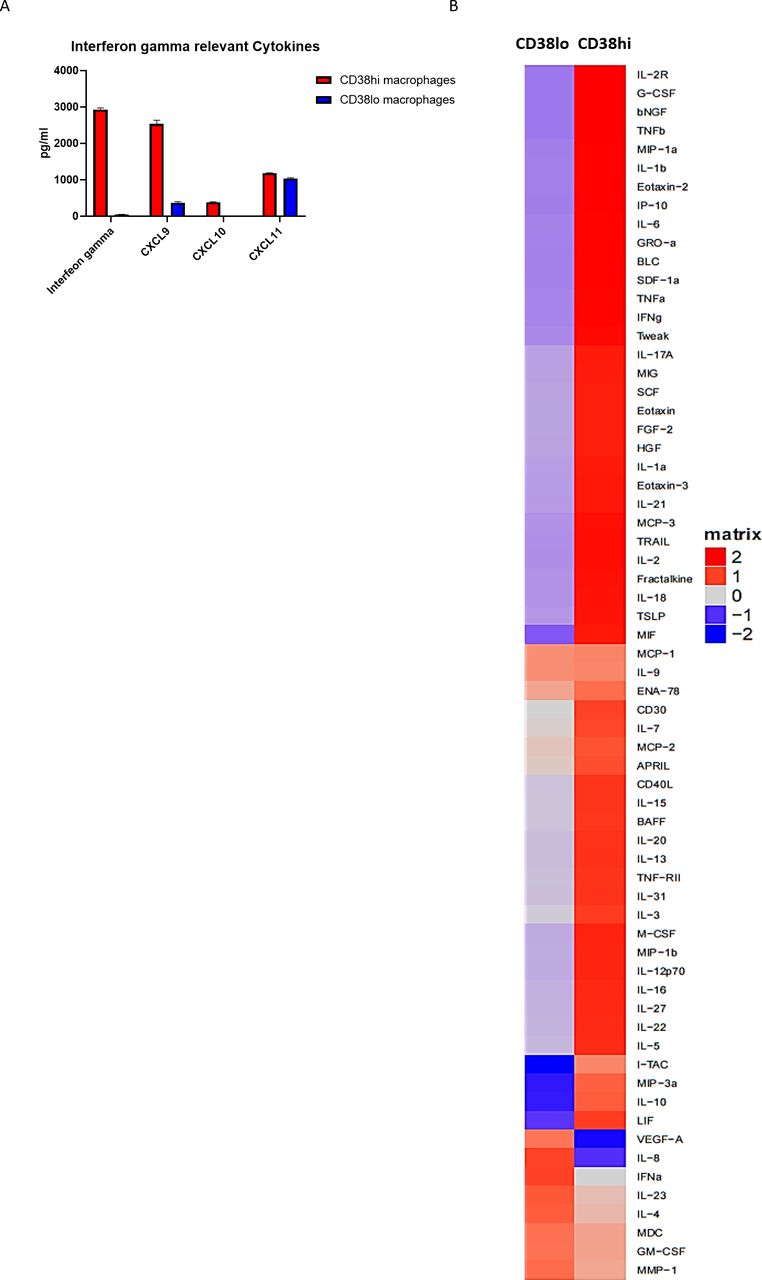
Our recent publication concerning CD38hi macrophages revealed the differential expression of CD80 and DC-SIGN compared with CD38lo macrophages, as well as the production of higher levels of proinflammatory cytokines, such as IL-6 and TNF-α.27 In the present study, we performed a Luminex experiment to simultaneously detect 65 cytokines in supernatant collected from both CD38hi and CD38lo macrophages. We not only validated that CD38hi macrophages produce more IL-6 and TNF-α than CD38lo macrophages but also found that these cells also produced more IFN-γ and related cytokines, including CXCL9, CXCL10 and CXCL11 (figure 6). Similarly, utilizing NanoString technology, we also demonstrated that the IFN-γ gene level trended higher in the patients who harbored high CD38+CD68+ macrophages (n=7), compared with the patients who harbored low CD38+CD68+ macrophages (n=7, online supplementary figure 5). However, the statistical significance was not reached.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CD38+ macrophages secrete proinflammatory cytokines. (A) IFN-γ and related cytokine secretion levels were determined by Luminex using cell culture supernatant. The data represent the mean±SD. (B) Heat map showing the standardized, averaged, logarithmically transformed Luminex concentrations for CD38hi and CD38lo macrophages. Analyte concentrations higher than the average are depicted in red, while the concentrations lower than the average are depicted in blue. Hierarchical clustering using Euclidean distance with complete linkage are shown for both analytes and samples. IFN-γ, interferon γ; VEGF, vascular endothelial growth factor.
Discussion
In this study, we used a range of readily translatable methods, including mIHC/IF, to confirm the expression of CD38 by macrophages and myeloid immune cells in the TME of a cohort of patients with HCC treated with anti-PD-1/PD-L1 blockade therapy. Further analysis of CD38 density established that higher CD38+ immune infiltrate and macrophage levels within the TME was associated with an improved immunotherapeutic response. Patients with a high proportion of intratumoral CD38+ immune cells achieved an ORR of 43.48%, compared with 3.85% for those with a low proportion. This improved response rate translated to a longer mPFS (8.21 months) and mOS (19.06 months). A high CD38+CD68+ macrophage density was also associated with a better ORR of 29.41% and longer mOS of 34.43 months. None of the classical clinicopathological variables including viral hepatitis status, PD-L1 expression or CD8+ T cell density were associated with survival in our cohort.
CD38 serves an important role in lymphocyte activation.65 70 Previous studies by our group have ascertained the involvement of activated lymphocytes and CD38 in HCC prognosis,25 26 and expression of CD38 has also been shown to be a prognostic marker in other types of cancers.71 72 We have also recently studied the effects of CD38 on macrophages and found that increased CD38 expression in HCC is associated with activation of the M1 pathway in macrophages.27 This process is characterized by increased CD80 expression and the induction of IL-6 and TNF-α secretion, all of which contribute to increased anti-tumor immunity in HCC.27 In the present study, we further demonstrated that CD38+ macrophages produce significantly more IFN-γ and related cytokines than those that lack CD38 expression. This may at least partially explain the relatively favorable response to anti-PD-1 therapy in patients whose tumors harbor increased numbers of this cell type.73 74
Cancer immunotherapy is mechanistically different from other treatment modalities, such as cytotoxic therapies and small module inhibitors, as it can target the TME as well as the tumor itself. Thus far, ICB therapy represents a promising novel treatment modality for a wide range of cancers. However, overall patient response rate to PD-1/PD-L1 inhibitors remains relatively low in certain types of cancers, limiting its application. This may be due to variability in the immune microenvironment between different types of cancer. Thus, further investigation of potential biomarkers in different cancers is of the utmost importance to identify patients most likely to benefit from treatment. With nivolumab failing to achieve statistical significance for OS in patients with advanced HCC when compared with sorafenib in the CHECKMATE 459 study (HR=0.85; 95% CI: 0.72 to 1.02; p=0.0752), it is thus paramount to identify patients most likely to benefit from ICB.75
Multiple previous studies have identified correlations between therapeutic response rates and PD-L1 expression in tumors, likely due to the close relationship between PD-L1 and PD-1. Increased PD-L1 expression is generally thought to be associated with an increased response rate and improved clinical benefit in PD-1 blockade therapy. However, these findings have not been reported across all tumor types.76–81 In the present study, we examined the PD-L1 TPS in our cohort using clone SP263, and found it not to be of predictive value (p=0.0716; table 2), consistent with prior clinical trials.7 8 Thus, the investigation of alternative immunosuppression mechanisms is necessary to identify more effective biomarkers.
One such mechanism thought to be of relevance is the adenosinergic pathway, where extracellular adenosine exerts local immunosuppressive effects through tumor-intrinsic and host-mediated mechanisms. In a recent study, CD38 was found to be expressed by a subset of tumors with high levels of basal or treatment-induced infiltration.65 Other previous studies have also demonstrated that tumors treated with PD-1/PD-L1-specific antibodies develop resistance to treatment through the upregulation of CD38, which follows the release of all-trans retinoic acid and IFN-β in the TME. This results in the suppression of CD8+ T cell function via the adenosine signaling pathway.65 In our study, we have observed that PD-L1 expression is higher for CD38+CD68+ macrophages, compared CD38−CD68+ macrophages by using mIHC/IF staining (online supplementary figure 6). However, PD-1+CD38hi CD8+ cells, which were reported to be predictive of immunotherapy response in advanced melanoma, failed to do so in HCC (online supplementary figure 7).82 Thus, the biological link between CD38 and PD-L1 appears to be complex and further studies are warranted.
Previously, CD38 was found to be expressed by macrophages isolated from mice,83 84 cell lines85 and was also found in human ex vivo experiments.64 Recently, our lab has also shown in vivo CD38 expression on macrophages in humans with HCC.27 This colocalization is also replicated here (figures 2 and 3). The present study established that CD38 expression in the HCC TME, particularly by immune cells such as macrophages, is associated with responsiveness to immunotherapy. Gene expression data from the present study also ascertained that CD38 is associated with improved prognosis in HCC, in accordance with the results of previous studies.25 86 Taken together, these results suggest that CD38 is part of a complex interplay between the inflammatory response and immune suppression via adenosine production and represents a potential biomarker for HCC immunotherapy.
Hepatitis B and C are integral in the pathogenesis of HCC and phenotype of HCC-infiltrating immune cells.87–89 Composition of CD38+ cells as well as CD38+CD68+ macrophages between patients with or without viral hepatitis (31 vs 18) was not different (online supplementary figure 8A,B). Interestingly when we examine the predictive value of CD38+ cells and CD38+CD68+ macrophages in viral-related HCC and non-viral-related HCC separately, both biomarkers are only significantly associated with responsiveness in the viral-related HCC (online supplementary figure 8A,B), but not in the non-viral-related HCC (online supplementary figure 8C,D).
The ORRs to ICB was significantly higher among patients with high proportion of total CD38+ cells compared with patients with low proportion (72.73% vs 0%) in viral-related HCC. Similarly, the ORRs to ICB was significantly higher among patients with high density total CD38+CD68+ macrophages compared with patients with low density (38.10% vs 0%, online supplementary figure 8E,F). On the contrary, comparable ORR was noted between high and low subgroups in the non-viral-related HCC (online supplementary figure 8E,F). As shown in online supplementary figure 9A–D, patients with viral-related HCC with either a high total CD38+ cell proportion or high density of total CD38+CD68+ macrophages had better PFS and OS when treated with ICB. (online supplementary table 7). No PFS/OS differences were noted in patients with non-viral-related HCC (online supplementary table 8, figure 9E–H). These findings suggest linkage between CD38 and viral-related HCC. However, more studies would be required to understand this relationship. As both the viral-related and non-viral-related HCC cohorts in this study is relatively small, further validation is needed.
In addition to the use of PD-1-specific monotherapy ICB in HCC, multiple strategies involving a combination of treatments are currently being evaluated. IMbrave150 (NCT03434379), a phase III,90 open-label, multicenter, randomized study evaluating combined atezolizumab and bevacizumab treatment versus sorafenib in patients with advanced HCC, recently met its coprimary endpoint; with improvements in both PFS and OS.90 The associations between CD38+ immune cell density and the outcome of combined ICB strategies warrant further evaluation.The detection of biomarkers using peripheral blood mononuclear cells for cancers have been a hot topic in the scientific community.91–93 In our study, we detected CD38+CD68+ macrophage in peripheral blood mononuclear cells (PBMCs) (online supplementary figure 10). It would be interesting to study its predictive value in a clinical trial prospectively.
As the overall patient response rate to ICBs remains relatively low in some other types of cancers, we also looked for prior studies of anti-PD-1 treatment and for which transcriptomic data were publicly available to investigate if the transcription level of CD38 could serve as an indicator of responsiveness to PD-1 axis blockade in those cancers. Two melanoma studies satisfied these requirements,94 95 while one was found for non-small cell lung cancer (NSCLC).96 For each study, we compared the CD38 transcription levels between patients who were responsive or non-responsive to anti-PD-1 treatment. We found no significant difference between the groups in the melanoma studies but found a significant difference between the groups in the NSCLC study (online supplementary figure 11), suggesting that the predictive potential of CD38 to be cancer type specific.
To the best of our knowledge, our study is the first to demonstrate that the expression of CD38 by certain immune subsets, such as macrophages, is a potential biomarker that predicts patient response to immunotherapy. While our anti-PD-1/PD-L1-treated HCC cohort is the largest of its kind to be reported thus far with potential biomarker correlative studies (n=49) compared with previous studies by Harding et al (n=27),97 Ang et al (n=17),98 and Ma et al (n=9)99 confirmatory studies in larger multinational cohorts will be needed to validate our observations. The present study is somewhat limited by the retrospective, and heterogeneous nature of this cohort, with multiple types of immunotherapy being received by the patients. However, in this study we have also tested for the anti-PD-1/PD-L1 single agent treatment cohort (n=30) and found that both biomarkers, namely intratumoral total CD38+ cell proportion and CD38+CD68+ macrophage density are associated with improved PFS and OS.
Another limitation is the choice of diagnostic PD-L1 clone used in this study. Given that a significant number of patients in this cohort are treated with anti-PD-L1 alone as well as anti-PD-1 alone, a comparison of 28–8 and SP263 clones would have been appropriate. However, the diagnostic clone 28–8 is not available in Singapore.
Notwithstanding, a high proportion of total CD38+ cells, as determined by IHC, predicts response to ICB and is associated with superior mPFS and OS in advanced HCC. Use of IHC-based techniques to evaluate for CD38 has its advantage as it is readily available and optimized in most diagnostic pathology departments enabling ease of translation and access in clinical practice. It is already in use as a diagnostic antibody for blood cancers, such as leukemia, plasmacytoma and multiple myeloma.100 101
Conclusion
In conclusion, the present study established an association between CD38 expression and the response to immunotherapy in HCC, using readily available and translatable IHC-based techniques. Most notably, to the best of our knowledge, the present study is the first to report a predictive marker of responsiveness to immunotherapy in HCC, using the largest reported cohort to date. Future investigations will involve the use of a larger, multinational cohort to confirm our results. We strive to apply these findings as a routine test in clinical practice, identifying patients most suited for ICB.
Acknowledgments
We thank the funding bodies such as the Centre Grant of Singapore General Hospital (grant no. NMRC/CG/M011/2017_SGH, NMRC/CIRG/1454/2016) and the AM-ETHOS Duke-NUS Medical Student Fellowship Award (grant no. AM-ETHOS01/FY2018/10-A10). We also thank Dr Alice Bridges, Dr Lam Jianhang, Mr Lim Chun Chye and Dr Lim Tong Seng for critical review as well as experimental inputs of the manuscript.
References
Footnotes
HHMN and RYL contributed equally.
Presented at This study has been partially presented as a preliminary study in a preprint: https://doi.org/10.1101/638981.
Contributors JY, DT and TL conceived, directed and supervised the study. HHMN, RYL and SG collated and interpreted the data and performed biostatistical analysis with help from BL, BT and HL. ISYT and JJHL performed IHC and histology-related technique. HHMN, SS and JY performed immunohistochemical scoring. XL, BA and JEC performed the immune-profiling such as flowcytometry and luminex. FM, TL and WQL contributed to the scientific content of the study. SYL and PC provided scientific inputs from surgery perspectives. EWN and VC provided scientific inputs from immunology perspectives. DT, JJXL, SPC and HCT provided scientific inputs from oncology perspectives. SG and HHMN drafted the manuscript with the assistance of JY and DT, with final review from all authors.
Funding This research was partially funded by the Centre Grant of Singapore General Hospital (grant no. NMRC/CG/M011/2017_SGH, NMRC/CIRG/1454/2016) and the AM-ETHOS Duke-NUS Medical Student Fellowship Award (grant no. AM-ETHOS01/FY2018/10-A10).
Competing interests DT is in the advisory board in MSD for clinical trials, and as research support in BMS. FM received research support from Janssen Pharmaceuticals, Celgene, Tusk Therapeutics and Centrose, and served on advisory boards for Centrose, Tusk Therapeutics, Jenssen, Takeda and Sanofi. JJXL has research funding from Bayer and has participated in advisory boards for Ipsen and Bayer.
Patient consent for publication Not required.
Ethics approval The Centralized Institutional Review Board of SingHealth provided ethical approval for the use of patient materials in this study (CIRB ref: 2014/590/B).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. All data relevant to the study are included in the article or uploaded as supplementary information.