Article Text

Abstract
Background In this phase I/II trial, we evaluated the safety and effectiveness of pembrolizumab, with or without concurrent radiotherapy (RT), for lung and liver lesions from metastatic non-small cell lung cancer (mNSCLC).
Methods Patients with lung or liver lesions amenable to RT plus at least one additional non-contiguous lesion were included regardless of programmed death-ligand 1 (PD-L1) status. Pembrolizumab was given at 200 mg every 3 weeks for up to 32 cycles with or without concurrent RT. Metastatic lesions were treated with stereotactic body RT (SBRT; 50 Gy in 4 fractions) if clinically feasible or with traditionally fractionated RT (45 Gy in 15 fractions) if not. The primary end point was the best out-of-field lesion response, and a key secondary end point was progression-free survival (PFS).
Results The median follow-up time was 20.4 months. One hundred patients (20 phase I, 80 phase II) were evaluable for toxicity, and 72 phase II patients were evaluable for treatment response. No patients in the phase I group experienced grade 4–5 events; in the phase II group, two had grade 4 events and nine had grade 3 events. The ORR in the combined-modality cohort (irrespective of RT schema) was 22%, vs 25% in the pembrolizumab group (irrespective of receipt of salvage RT) (p=0.99). In the concurrent pembrolizumab+RT groups, the out-of-field ORRs were 38% in the pembrolizumab+SBRT group and 10% in the pembrolizumab+traditional RT group. When examining the pembrolizumab-alone patients, the out-of-field ORRs were 33% in those designated to receive salvage SBRT (if required) and 17% for salvage traditional RT. In all patients, the median PFS for pembrolizumab alone was 5.1 months (95% CI 3.4 to 12.7 months), and pembrolizumab/RT (regardless of schema) was 9.1 months (95% CI 3.6 to 18.4 months) (p=0.52). An exploratory analysis revealed that for patients with low PD-L1 expression, the median PFS was 4.6 vs 20.8 months for pembrolizumab with and without RT, respectively (p=0.004).
Conclusions Concurrent immunoradiotherapy for mNSCLC is safe, although larger trials are required to address which patients benefit most from RT.
Trial registration number NCT02444741.
- radioimmunotherapy
- radiotherapy
- immunotherapy
- lung neoplasms
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Recent advances in cancer immunotherapy have profoundly influenced care for patients with metastatic non-small cell lung cancer (mNSCLC).1 The previous standard of care for mNSCLC had been platinum-based chemotherapies,2 but programmed cell death protein 1/programmed death-ligand 1 (PD-1/PD-L1)—targeted therapies now represent the standard of care in most cases.3–5 However, response rates remain less than ideal; overall, the response rates to immunotherapy alone range from 20% to 30%, and even those of biomarker-selected subgroups are no higher than 45%. Because primary resistance of mNSCLC to immunotherapy may underlie these low response rates, methods to overcome mechanisms of primary and secondary resistance to PD-1/PD-L1-directed therapies by using combination strategies such as chemoimmunotherapy are under intense investigation.5
Radiotherapy (RT) may enhance immunotherapeutic effects. Radiation can prime antigen release, allowing improved antigen processing and ultimately enhanced T-cell killing.6–8 Immunoradiotherapy has shown promise in several cancers, potentially attenuating the development of resistance and improving outcomes.9 However, evidence of synergism between immunotherapy and RT in terms of response of mNSCLC from randomized studies is largely lacking. To address this gap, we undertook a prospective randomized phase I/II trial in which the phase I component tested the safety of immunoradiotherapeutic regimens, and the phase II component evaluated the out-of-field lesion response rate and progression-free survival (PFS) of pembrolizumab with or without RT (given in one of two schedules).
Methods
Patients
Eligible patients were at least 18 years of age and had pathologically confirmed mNSCLC (PD-L1 testing was not mandated, but generally done when adequate tissue was available), with one to four lung or liver lesions amenable to RT and at least one additional non-contiguous lesion amenable to radiographic evaluation for out-of-field objective responses. Both newly diagnosed and previously treated cases were eligible. Prior RT and systemic therapy were allowed unless they precluded safe administration of immunoradiotherapy on our study protocol. Patients with brain metastases after undergoing individualized treatment were included except for those presenting with neurological symptoms or requiring corticosteroids. Patients were required to have a baseline Eastern Cooperative Oncology Group performance status score of 0 or 1 and adequate organ function. Notable exclusion criteria included a history of immunodeficiency or autoimmune disease.
Study design and treatment
All patients underwent baseline positron emission tomography or CT scans within 4 weeks before beginning protocol treatment. For all patients, these baseline images were used to judge, before randomization, whether stereotactic body RT (SBRT) could be delivered safely. If clinically feasible, SBRT (50 Gy in 4 daily fractions) was delivered starting on day 1. For lesions that were not amenable to SBRT (eg, were centrally located), traditional hypofractionated RT (45 Gy in 15 daily fractions) was begun on day 1.
The phase I portion of the trial consisted of a standard 3+3 dose-escalation design, with pembrolizumab administered at 100 mg followed by 150 and 200 mg if the former dose was tolerated. Pembrolizumab was given concurrently with either RT schema (day 1) and administered every 21 days for up to 32 cycles. Follow-up CT or positron emission tomography/CT scans were obtained every 12 weeks (±4 weeks) to evaluate response to therapy.
In the phase II component, randomization was conducted 1:1 by the MD Anderson Department of Biostatistics according to the adaptive randomization method described by Pocock and Simon,10 with a minimization probability parameter of 0.90. Patients were randomized to receive pembrolizumab alone or combined with RT. The logistics and dosing of both RT and immunotherapy were similar to those in the phase I portion, except that the maximum tolerated dose of pembrolizumab was used. Notably, for the patients randomized to receive pembrolizumab only, if disease had progressed after delivery of the second pembrolizumab dose, salvage radiation (either SBRT or traditional RT) was given before the third pembrolizumab dose, in accordance with institutional policies and recommendations.
The primary objective of the phase I portion of the study was to determine the safety and maximum tolerated dose of pembrolizumab with RT based on the presence of dose-limiting toxicities. These toxicities (possibly, probably or definitely related to protocol therapy) were defined as any grade ≥3 non-hematological event, any grade ≥4 hematological event lasting >5 days and any toxic effects that prevented the administration of pembrolizumab for >21 days from the scheduled administration. Toxicity was scored with the Common Terminology Criteria for Adverse Events (V.4.0).
The primary end point of the phase II component was the best out-of-field objective response rate (ORR). PFS was a key secondary end point. Progression was defined from the time of treatment initiation (first cycle of pembrolizumab or RT, whichever came first) and was evaluated according to the Immune-Related Response Criteria.11 Briefly, complete response (irCR) was defined as complete elimination of all tumors, partial response (irPR) was defined as at least a 50% reduction in total tumor burden and progressive disease (irPD) was defined as a >30% increase in tumor burden. All other cases were classified as stable disease (irSD). Out-of-field response referred to irCR or irPR. Progression was determined after consecutive imaging demonstrated an increase in tumor burden but was backdated to the initial time of progression. Overall survival analysis was not performed owing to the lack of events at the time of data cut-off.
Standard-of-care complete blood counts, which included absolute lymphocyte, platelet, neutrophil and monocyte counts, were obtained periodically starting at study initiation and before administration of subsequent cycles of pembrolizumab for monitoring and biomarker analysis. For analysis of cell counts by fractionation schedule (SBRT vs traditional RT), samples collected 2 weeks before RT were considered the baseline, and post-RT samples were collected at least 1 week after RT completion.
Mutation analysis
Sequencing platforms used for mutation analysis included in-house Clinical Laboratory Improvement Amendments-certified next-generation panel sequencing (MD Anderson Molecular Diagnostics Laboratory) and the Foundation Medicine platform (Cambridge, Massachusetts, USA) for tissue samples and Guardant360 (Guardant Health, Redwood City, California, USA) for blood samples.
Statistical analysis
All statistical analyses were done with SPSS (V.24; IBM, Armonk, New York, USA) and Prism (V.8; GraphPad Software, San Diego, California, USA). Two equally sized groups of 40 patients each were estimated to have 80% power to detect a 30% difference in ORR (eg, 25% vs 55% between groups). The Kaplan-Meier product limit method was used to estimate PFS distributions, with HRs computed and tested with Cox proportional hazards regression analysis. ORRs between groups were evaluated by using χ2 tests, with 95% CIs calculated using the binomial exact method. The Student’s t-test was used to compare serum markers by radiation schedule (SBRT vs traditional RT).
Results
Patient characteristics
From September 2015 to August 2018, we enrolled a total of 100 patients with mNSCLC, 20 of whom were in the phase I cohort, with the remaining 80 in the phase II cohort (Consolidated Standards of Reporting Trials diagram for phase II cohort). Clinical characteristics of all 100 patients are shown in table 1.
Patient characteristics
The median follow-up time was 20.4 months (range 1.4‒30.2 months). At the cut-off date for analysis (May 15, 2019), all 20 patients in the phase I portion were evaluable for treatment response (3 of whom received 100 mg, 3 received 150 mg and 14 received 200 mg of pembrolizumab; n=10 SBRT and n=10 traditional RT) along with 72 subjects in the phase II population (the remaining 8 patients did not have any follow-up imaging and hence could not be evaluated for response).
In the phase II cohort, the median number of metastatic lesions at baseline was three (range 1‒10) in both groups. Of the 40 subjects who received concurrent pembrolizumab and RT, most received RT to one site (n=36) or two sites (n=4). Thirty-five of the irradiated sites were in the lung. The median number of pembrolizumab infusions was seven in the pembrolizumab-alone group and nine in the pembrolizumab+RT group. Seven of the 36 patients in the pembrolizumab-alone arm eventually received salvage RT (6 of whom received SBRT, 6 received single-site irradiation and 5 received radiation to a lung lesion).
Toxicity
Toxic effects attributable to the protocol treatments are shown in table 2 for the phase I patients and in online supplemental tables S1 and S2 for the phase II patients. In the phase I group, most adverse events were self-limiting, and no patients experienced grade 4 or 5 toxic effects. Six (30%) experienced grade 3 events: rash (n=2), fatigue (n=1), nausea (n=1), lung infection (n=1) and pneumonitis (n=1). Notably, two patients discontinued treatment due to toxic effects after the initial observation window. One patient had pneumonitis, which was first diagnosed after administration of four doses of pembrolizumab. The other patient had increased myalgia and fatigue (both grade 2) and a diagnosis of polymyalgia rheumatica, also after receiving four doses of pembrolizumab.
Supplemental material
Treatment-related adverse events in 20 phase I patients evaluable for toxicity of concurrent pembrolizumab+radiation therapy
In the phase II group, we observed two grade 4 toxic effects (both considered possibly related to protocol treatment) in the concurrent pembrolizumab+SBRT group but no grade 4 or 5 effects in any other group. These two grade 4 effects occurred in one patient, who had a myocardial infarction and subsequent ventricular tachycardia (outside the RT field) with grade 3 right ventricular dysfunction 2 weeks after the first cycle of pembrolizumab. This patient was subsequently removed from the study.
Seven grade 3 toxic effects occurred in the pembrolizumab-salvage SBRT group in the phase II component (one case each of myositis, pain, dyspnea, dysphagia, aspartate transaminase and alanine transaminase elevation, and two cases of leukopenia), and two grade 3 events in the concurrent pembrolizumab-SBRT (group 1) arm (right ventricular dysfunction and pneumonitis). In the pembrolizumab-salvage traditional RT group (group 4), we observed three grade 3 toxic effects (mucositis, aspartate transaminase elevation and alanine transaminase elevation), and in the concurrent pembrolizumab-traditional RT group (group 3), we saw five grade 3 toxic effects (one case each of rash, pericardial effusion, atelectasis and pleural effusion and two cases of pneumonitis).
Treatment response
Figure 1 displays the ORRs for various groups. The ORR in the combined-modality cohort (regardless of RT schema) was 22% (8/36), vs 25% (9/36) in the pembrolizumab group (regardless of receipt of salvage RT) (p=0.99). In the concurrent pembrolizumab+RT groups, the out-of-field ORRs were 38% in the pembrolizumab+SBRT group and 10% in the pembrolizumab+traditional RT group. When examining the pembrolizumab-alone patients, the out-of-field ORRs were 33% in those designated to receive salvage SBRT (if required) and 17% for salvage traditional RT. Online supplemental table S3 shows the irPR, irSD and irPD rates of each individual group.
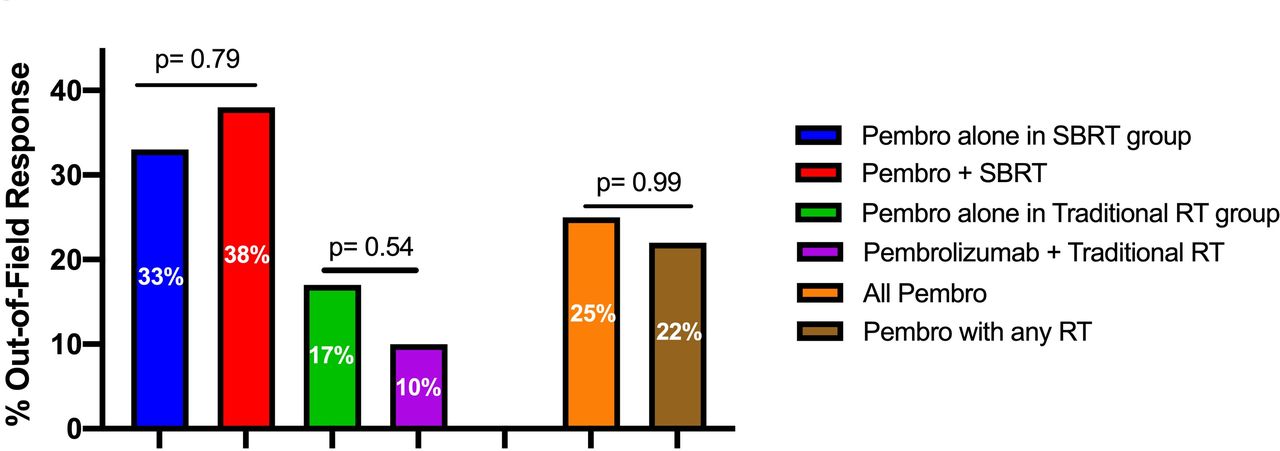
Out-of-field overall response rates (ORRs) for patients with metastatic non-small cell lung cancer evaluated with immune-related response criteria, stratified according to the treatment received. RT, radiotherapy; SBRT, stereotactic body RT.
PFS was then examined (figure 2). In all patients, the median PFS for pembrolizumab alone was 5.1 months (95% CI 3.4 to 12.7 months), and pembrolizumab/RT (regardless of schema) was 9.1 months (95% CI 3.6 to 18.4 months) (p=0.52, figure 2A). When stratifying for RT schema, in patients for whom SBRT was deemed feasible, the median PFS times were 14.2 months (95% CI 12.4 to 15.8 months) for the pembrolizumab-only group and 20.8 months (95% CI 17.7 to 23.9 months) for the pembrolizumab+SBRT group (p=0.76, figure 2B). In the traditional RT cases, respective PFS times were 4.7 months (95% CI 3.1 to 6.2 months) for the pembrolizumab-only group and 6.8 months (95% CI 3.0 to 10.7 months) for the pembrolizumab+traditional RT group (p=0.79, figure 2C).
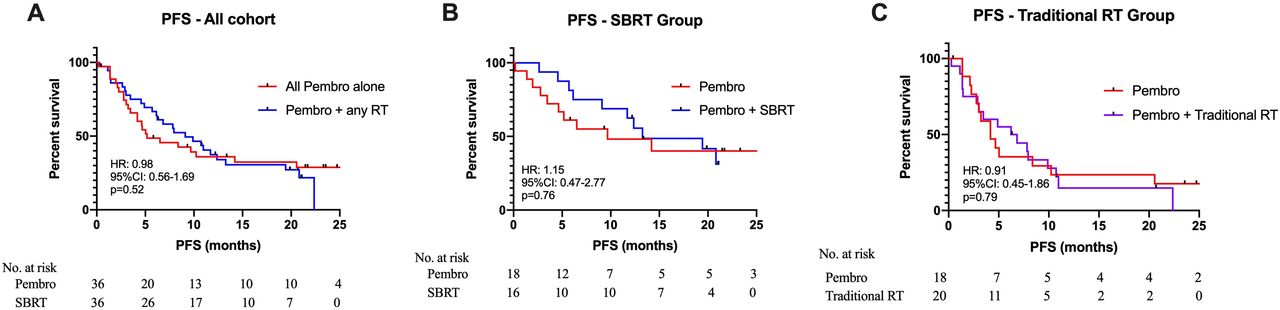
Progression-free survival (PFS) times in (A) all patients, (B) patients with disease amenable to stereotactic body RT (SBRT) and (C) patients with disease requiring traditional radiotherapy (RT).
Waterfall plots of out-of-field lesion responses in all four groups are shown in online supplemental figure S1A-D.
PD-L1 status
Overall, PD-L1 status (from biopsy) was available for 51 of 80 patients in phase II cohort (26 pembrolizumab-only and 25 pembrolizumab+RT), and hence this analysis remains exploratory. In the pembrolizumab-only group, tumors in 10 patients (38%) were negative for PD-L1 (tumor proportion score <1%), 7 (27%) had low PD-L1 expression (1%‒50%) and 9 (35%) had high PD-L1 expression (>50%). In the pembrolizumab+RT group, tumors in 9 patients (35%) were negative for PD-L1, 12 (46%) had low expression and 4 (15%) had high expression.
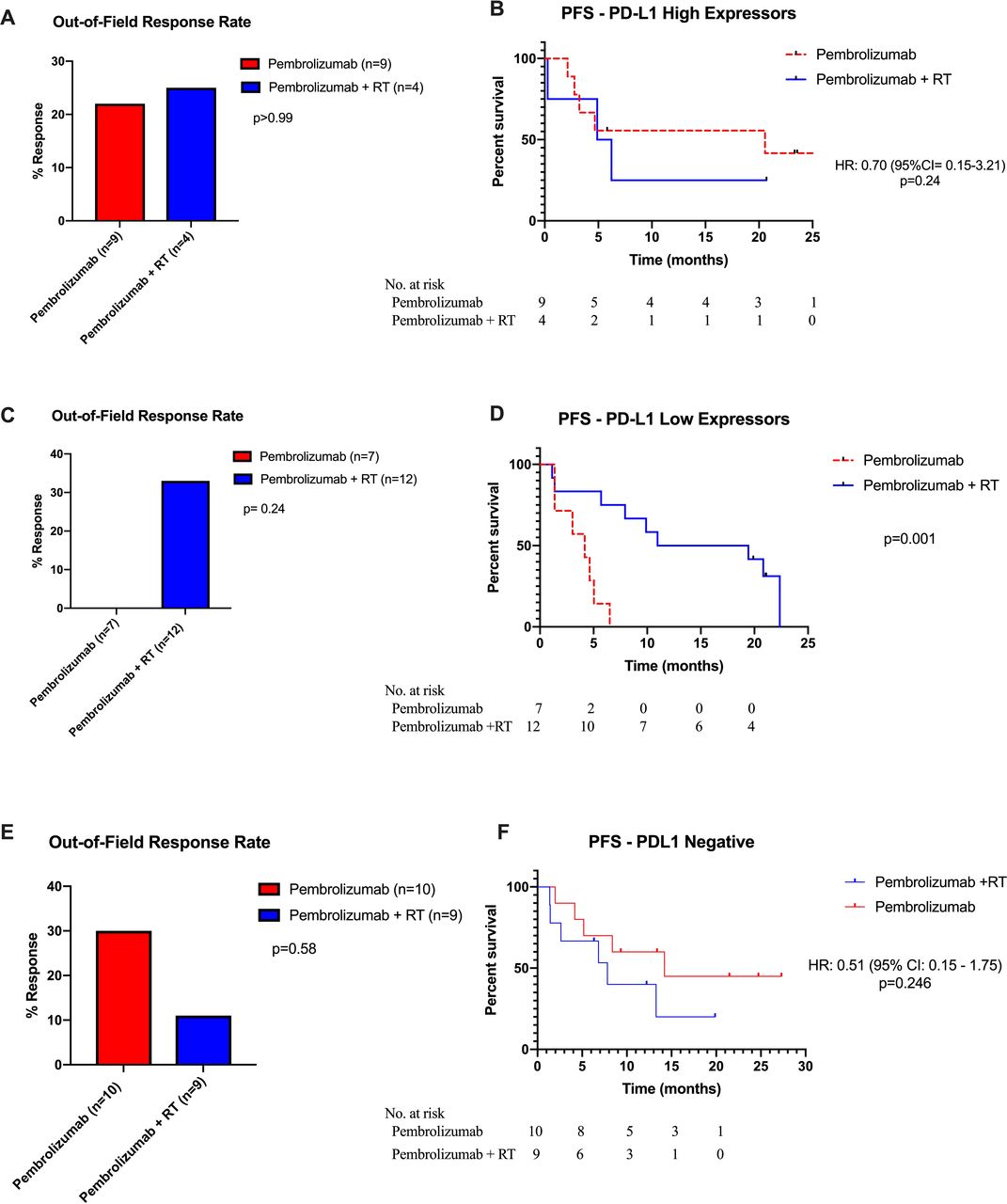
In the 13 subjects with high PD-L1 expression, the ORRs were 22% in the pembrolizumab-only group and 25% in the pembrolizumab+RT group (p=0.99) (figure 3A); the corresponding median PFS times were 20.6 and 5.6 months (p=0.49) (figure 3B). In the 19 patients with low PD-L1, the ORRs were 0% in the pembrolizumab-only group and 33% in the pembrolizumab+RT group (p=0.24) (figure 3C), with corresponding median PFS times of 4.6 and 20.8 months (p=0.001) (figure 3D). Among the 19 patients negative for PD-L1, the ORRs were 30% in the pembrolizumab-only group and 11% in the pembrolizumab+RT group (figure 3E), with corresponding median PFS times of 14.2 and 7.8 months (p=0.25) (figure 3F).
{kind=link}
{kind=link}
{kind=link}
Out-of-field overall response rates (ORRs) and progression-free survival (PFS) in the (A and B) high-programmed death-ligand 1 (PD-L1) expression group, (C and D) low-PD-L1 expression group and (E and F) PD-L1-negative group. RT, radiotherapy.
RT regimens
An exploratory analysis revealed that when patients were stratified by RT fractionation, the out-of-field ORRs were 38% for SBRT vs 10% for traditional RT (p=0.11) (online supplemental figure S2A), with corresponding median PFS times of 20.8 and 6.8 months (p=0.03) (online supplemental figure S2B).
We also looked at response to each RT fractionation type in terms of absolute lymphocyte counts. Mean reductions in counts were ‒19% in the SBRT group and ‒47% in the traditional RT group (p=0.003). We also evaluated changes in platelet, absolute neutrophil and absolute monocyte counts to determine whether these differences were related to myelosuppression. Mean changes in the platelet counts were ‒3% in the SBRT group and ‒12% in the traditional RT group (p=0.23); changes in absolute neutrophil counts were ‒10.1% and 9.9% (p=0.99) and changes in absolute monocyte counts were ‒5.3% and ‒6.2% (p=0.88).
Prior RT
In the pembrolizumab-only group, 7 patients (19%) had received RT within 6 months of beginning protocol therapy, and 29 (81%) had not. The corresponding out-of-field ORRs in these groups were 43% and 20% (p=0.33) (online supplemental figure S3A). The median PFS time was not reached in the prior-RT group but was 6.5 months for patients who had not had prior RT (online supplemental figure S3B).
Driver mutations
Sixty-nine patients had available results of mutation testing. Tumors in 11 patients had activating epidermal growth factor receptor (EGFR) mutations (5 in the pembrolizumab+RT group and 6 in the pembrolizumab-only group); tumors in 6 patients had Kras and STK11 mutations (4 in the combination group and 2 in the pembrolizumab-only group) and tumors in 9 patients had Kras and TP53 mutations (3 in the combination group and 6 in the pembrolizumab-only group). We saw no significant differences in PFS or ORRs between pembrolizumab with or without additional RT (EGFR mutations: p=0.57 for PFS and p=0.74 for OR; Kras+TP53 mutations: p=0.96 for PFS and p=0.16 for OR) (online supplemental figure S4A and S4B). The sample size was too small to compare those with Kras and STK11 mutations.
Discussion
This randomized study compared pembrolizumab with or without RT for mNSCLC. We found that combined immunoradiotherapy was safe, with few high-grade adverse events. Moreover, although we saw no significant differences in ORRs or PFS time in this study, exploratory findings suggest that RT may be more beneficial for patients with low PD-L1 expression. Hence, analogous randomized trials using these factors to enhance mNSCLC patient selection are recommended.
Several factors can potentially explain why the combined-modality patients did not experience statistically higher ORRs or PFS than subjects having received pembrolizumab alone. First, the relatively smaller sample sizes may have limited the ability to detect finer differences between arms. Second, the vast majority of the patients received RT to a single site, which may stimulate the immune system to a considerably lesser degree than RT to multiple sites.12 Third, the mixed use of SBRT and hypofractionated RT could have diminished differences between groups, especially since the use of wider fields in the latter could have led to lymphocyte inactivation and hampering of the antitumoral immune response.13 14 At the time this trial was designed, there were no data suggesting differential outcomes by RT field size/dose/technique (eg, the trial was powered for a two-group comparison of pembrolizumab vs pembrolizumab plus either SBRT/hypofractionated RT). However, these findings provide important evidence to design future trials using stratification for RT dose/technique.
An additional cause of the dampened results between arms could be the lack of PD-L1 standardization and stratification. Subjects with high PD-L1 expression did not seem to benefit from RT (perhaps because response rates to pembrolizumab alone tend to be notably higher in this subset), although this claim must be taken with caution given the unknown PD-L1 status for some patients as well as the overall lower sample size. Nevertheless, it is possible that if low PD-L1 expressors were enrolled in this trial, the results between groups might have been more pronounced since pembrolizumab alone is less effective with lower levels of PD-L1 expression.3
Because the vast majority of patients were oligometastatic, these results may not apply to polymetastatic disease. Nevertheless, this trial offers important clinical information regarding the utility of RT in the setting of immunotherapy. Currently, patients with oligometastatic NSCLC may benefit from immunotherapy alone as part of inclusion in various randomized trials, or local consolidative RT to all sites of disease.3 15 However, RT has been scarcely evaluated in the setting of immunotherapy to date. Whether there is an additional benefit of RT if immunotherapy is being uniformly administered is currently an open question, which our data (as well as the ongoing NRG LU002 trial) may help to address.
Our findings can be considered in juxtaposition with results of the PEMBRO-RT study conducted in the Netherlands.16 That randomized phase II trial was somewhat different from this trial, having evaluated mostly previously treated and polymetastatic patients (n=76). Patients in that trial were randomized to receive pembrolizumab (at the same dose as in our phase II study) with or without single-site SBRT to 24 Gy in three fractions. The combined-modality cohort had a substantially higher 12-week ORR (41% vs 19%) and longer median PFS time (6.4 vs 1.8 months). These figures were lower than those in our trial, probably because of differences in the patient populations, the total number of metastatic lesions and the specific sites irradiated. Efforts to examine this trial and the PEMBRO-RT trial in a pooled manner are underway.
We acknowledge that our trial had some limitations, despite its prospective randomized nature, that may hinder interpretation of the results. The nascence of the field of immunoradiotherapy means that the only mature randomized trials to date have had small numbers of patients and short follow-up times. Also, our chosen end point of best ORR should be viewed with caution, given that stable disease may also indicate disease control. Moreover, neither our study nor the PEMBRO-RT study prestratified patients according to PD-L1 status, and we allowed salvage RT in the pembrolizumab-only arm. We also included patients who received RT shortly before trial enrollment (<6 months), which may have made their immune systems more susceptible to T-cell penetration and activation. Finally, although mNSCLC is inherently heterogeneous, applying exclusion criteria such as disease burden, histology, prior therapy and response to first-line induction immunotherapy would have greatly hindered accrual to this trial. Nevertheless, these shortcomings do not obviate the need for further randomized studies of subsets of patients with mNSCLC who may benefit from RT.
In short, we conclude from this admittedly small, preliminary trial that concurrent immunoradiotherapy for mNSCLC is safe and potentially effective for some subsets (eg, possibly for low PD-L1 expressors). We look forward to the findings from future larger trials, with greater numbers of patients and longer follow-up, to explore which subsets of patients with mNSCLC are most likely to benefit from immunoradiotherapy.
Acknowledgments
The authors would like to thank Christine F. Wogan, MS, ELS, of MD Anderson’s Division of Radiation Oncology for reviewing and editing the manuscript.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
JW, HM and DC contributed equally.
Contributors Study design and conception: JW, JVH, DC and HM. Clinical investigators: JW, JVH and DC. Clinical trial statistical analysis: KH. All authors drafted the initial version of this manuscript. DC and HM interpreted the data. All authors participated in review and revision of the manuscript. All authors read and approved the final manuscript.
Funding Funding for and access to pembrolizumab was provided by Merck. Supported in part by NIH/NCI grant no. P30CA016672 to The University of Texas MD Anderson Cancer Center.
Competing interests JW, JVH, MA and JYC have received research grants from Bristol-Myers Squibb. JW has received grants from Merck. JVH also received research funding from AstraZeneca and Spectrum Pharmaceuticals. MA has also received research funding from Lilly, Novartis and GSK. JW is a co-founder of Healios, MolecularMatch and OncoResponse; he is on the scientific advisory board of RefleXion Medical, Mavupharma, Alpine Immune Sciences and Checkmate Pharmaceuticals; he has received grants from Varian and OncoResponse; he has also received laboratory research support from Bristol-Myers Squibb, Merck, Aileron, Nanobiotix and Checkmate Pharmaceuticals; he has ownership interest in OncoResponse. VP is advisory board members for Bristol-Myers Squibb. JYC is a shareholder of Global Oncology One. JVH has ownership interest in Cardinal Spine and Bio-Tree.
Patient consent for publication Not required.
Ethics approval This study was approved by The University of Texas MD Anderson Cancer Center’s institutional review board, and written informed consent to participate was obtained from all patients.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.