Article Text

Abstract
Background and aims Immune checkpoint inhibitor (ICI) enterocolitis is a common immune-related adverse event and can be fatal, especially when not diagnosed and treated promptly. The current gold standard for diagnosis is endoscopy with biopsy, but CT scan is a possible alternative. The primary objective of this study is to identify the diagnostic performance of CT in the evaluation of ICI enterocolitis.
Methods With institutional review board approval, we conducted a retrospective cohort study of patients who received ICI therapy between 2015 and 2019 across a healthcare system. Patients were included if they underwent both abdominal CT and endoscopy with biopsy within 3 days. The radiological and pathological diagnoses, as well as clinical characteristics, were extracted from the electronic medical record. We calculated the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of CT for diagnosing ICI enterocolitis when compared with tissue diagnosis.
Results Of the 4474 patients screened, 138 met inclusion criteria. Most common tumor types were melanoma (37%) and lung cancer (19%). Seventy-four per cent were treated with antiprogrammed cell death (PD-1)/PD-L1 therapy. Thirty-nine per cent had signs of enterocolitis on CT scan and 58% had biopsy-proven ICI enterocolitis. Sensitivity and specificity of CT were 50% and 74%, respectively. PPV was 73% and NPV was 52%. Of those with confirmed ICI enterocolitis, 70% had grade 3 or higher symptoms, 91% received steroids and 40% received infliximab.
Conclusion The performance of CT scan for diagnosis of ICI enterocolitis is moderate to poor and does not replace endoscopy with biopsy.
- inflammation
- autoimmunity
- immunotherapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Immune checkpoint inhibitor (ICI) therapies targeting cytotoxic T lymphocyte antigen (CTLA)−4, programmed cell death protein (PD)-1 or its ligand (PD-L1) are now approved for the treatment of over a dozen malignancies.1 While these agents can result in durable responses, they also induce substantial inflammatory toxicities.2–4 ICI enterocolitis, inflammation of the small intestine and colon, is one of the most common toxicities and can be fatal, especially when diagnosis and treatment are delayed.5 6 Endoscopy with biopsy is the gold standard for diagnosis, allowing for both macroscopic and microscopic direct visualization of inflammation, but it is invasive and resource intensive. Limited evidence suggests that CT may be an alternative for diagnosing enterocolitis secondary to CTLA-4 inhibition, with a sensitivity of 85.2%, specificity of 75.0%, positive predictive value (PPV) of 95.8% and negative predictive value (NPV) of 42.9%.7 However, data on the diagnostic utility of CT for enterocolitis secondary to PD-1/PD-L1 blockade are lacking. Despite the lack of evidence, some current guidelines recommend imaging as part of the initial workup for suspected PD-1/PD-L1 enterocolitis.2 8 9
Enterocolitis secondary to CTLA-4 inhibition is typically dose-dependent, with a relatively predictable time to onset.6 10 PD-1/PD-L1-induced enterocolitis is clinically distinct, with a more insidious onset, wider range of presenting symptoms and variable severity.11 These clinical differences signal that previous work regarding the diagnosis of enterocolitis secondary to anti-CTLA-4 therapy may not be generalizable to that from PD-1/PD-L1 inhibition. As anti-PD-1/PD-L1 therapies have rapidly become standard first-line treatment for many malignancies, and are now more commonly administered than anti-CTLA-4 therapies such as ipilimumab, data on the optimal diagnostic algorithm of PD-1/PD-L1-induced enterocolitis are needed.12
In this study, we aim to evaluate the diagnosis of ICI enterocolitis secondary to both CTLA-4 and PD-1/PD-L1 inhibition in a heterogeneous population of patients presenting with variable symptoms and clinical severity. We compared the diagnostic performance of CT, as well as endoscopy alone, to the gold standard of endoscopy with biopsy. These data provide a framework for the appropriate diagnostic workup of possible ICI enterocolitis in real-world clinical practice.
Methods
Study design and inclusion criteria
We conducted a retrospective cohort study of patients at the Mass General Brigham healthcare system between 2015 and 2019, following the adoption of a unified electronic health record (EHR). Patients were identified using a system-wide data warehouse, the Research Patient Database Registry. Inclusion criteria required patients receive at least one dose of ICI therapy including anti-CTLA-4 monotherapy, PD-1/PD-L1 inhibition±CTLA-4 antagonism and combination chemotherapy-ICI and targeted therapy-ICI combinations. Patients receiving these agents on clinical trials were included. Eligible patients underwent both endoscopy with biopsy (including esophagogastroduodenoscopy (EGD), flexible sigmoidoscopy and colonoscopy) and abdominal CT scan within a 3-day period of each other and within a year of last ICI dose. Patients were excluded if they did not have both diagnostic tests, and if no tissue samples were collected during the upper or lower endoscopy. Repeat CT scans within the 3-day window were excluded from analysis if the imaging was not correlated with a clinical change to avoid duplicate data points.
Data extraction
We used the EHR to extract data on patient characteristics, including age, sex, tumor type and ICI treatment course. Diarrhea and colitis grade as per Common Terminology Criteria for Adverse Events (CTCAE) V.5.0 was determined through provider documentation; where not recorded, grade was determined by maximum frequency of bowel movements and severity of colitis symptoms documented and resolution was determined by improvement in diarrhea and abdominal pain. Dates of symptom onset, resolution, as well as the colitis-specific treatments administered were extracted from the EHR. Data on the diagnostic workup performed—specifically endoscopy and imaging, including type of scope, date of procedure and date of CT scan—were collected.
Pathological analysis
Patients were determined to have signs of inflammation on endoscopy if the finding was documented in the endoscopic report in the EHR, as assessed by the evaluating gastroenterologist. Patients were considered to have biopsy-proven ICI enterocolitis if there was histological evidence consistent with ICI enterocolitis on the tissue sample obtained during endoscopy, as assessed by the evaluating pathologist. Patients were considered to have enterocolitis of any etiology if there was histologic evidence of inflammation, as assessed by the evaluating pathologist.
Image analysis
Patients were determined to have radiological evidence of enterocolitis on CT if the diagnosis was noted in the impression of the radiology report in the EHR, as assessed by the evaluating radiologist. All imaging was then reviewed by two expert radiologists using a predesigned template of imaging features for diagnosis of enterocolitis, both independently and in consensus. Both radiologists were blinded to the initial radiology report and the final diagnosis. Imaging findings of enterocolitis included bowel wall thickening, mucosal or mural hyperenhancement, pericolonic stranding, fluid-filled loops of bowel and mesenteric hyperemia. Each scan was given a consensus score from 1 to 5, with 1 being not enterocolitis and 5 being definite enterocolitis. Cases with a score of 4 or 5 were considered to be enterocolitis.
Statistical analysis
Biopsy results were used to validate the CT and endoscopy findings. We assessed the sensitivity, specificity, PPV and NPV of CT compared with the ‘gold standard’ of endoscopy with biopsy, as well as endoscopic identification of inflammation compared with biopsy results. We evaluated both the initial imaging diagnosis, documented on the official radiology report at the time of presentation and the diagnosis after retrospective blinded expert review. Test characteristics were assessed for diagnosis of ICI enterocolitis and enterocolitis of any etiology. The software package R Studio (V.3.5.2; Vienna, Austria) was used for the statistical analyzes.
Results
Patient population
Of the 4474 patients who underwent endoscopic evaluation after ICI therapy, 229 patients had CT imaging within 3 days of endoscopy. Of those patients, three were excluded as imaging did not correlate with a clinical change and 88 were excluded as no biopsy samples were taken. One hundred and thirty-eight had both CT scan and endoscopy with biopsy for paired analysis, representing 127 unique patients (figure 1). Median age was 65 years and 57% of patients were female. The most common tumor types were melanoma (37%) and non-small cell lung cancer (NSCLC; 19%). Seventy-four per cent of patients were treated with anti-PD-1/PD-L1 therapy, either as monotherapy or in combination with another oncologic therapy, and 22% were treated with anti-CTLA-4/anti-PD-1 combination therapy, with the remaining patients treated with CTLA-4 monotherapy (table 1).
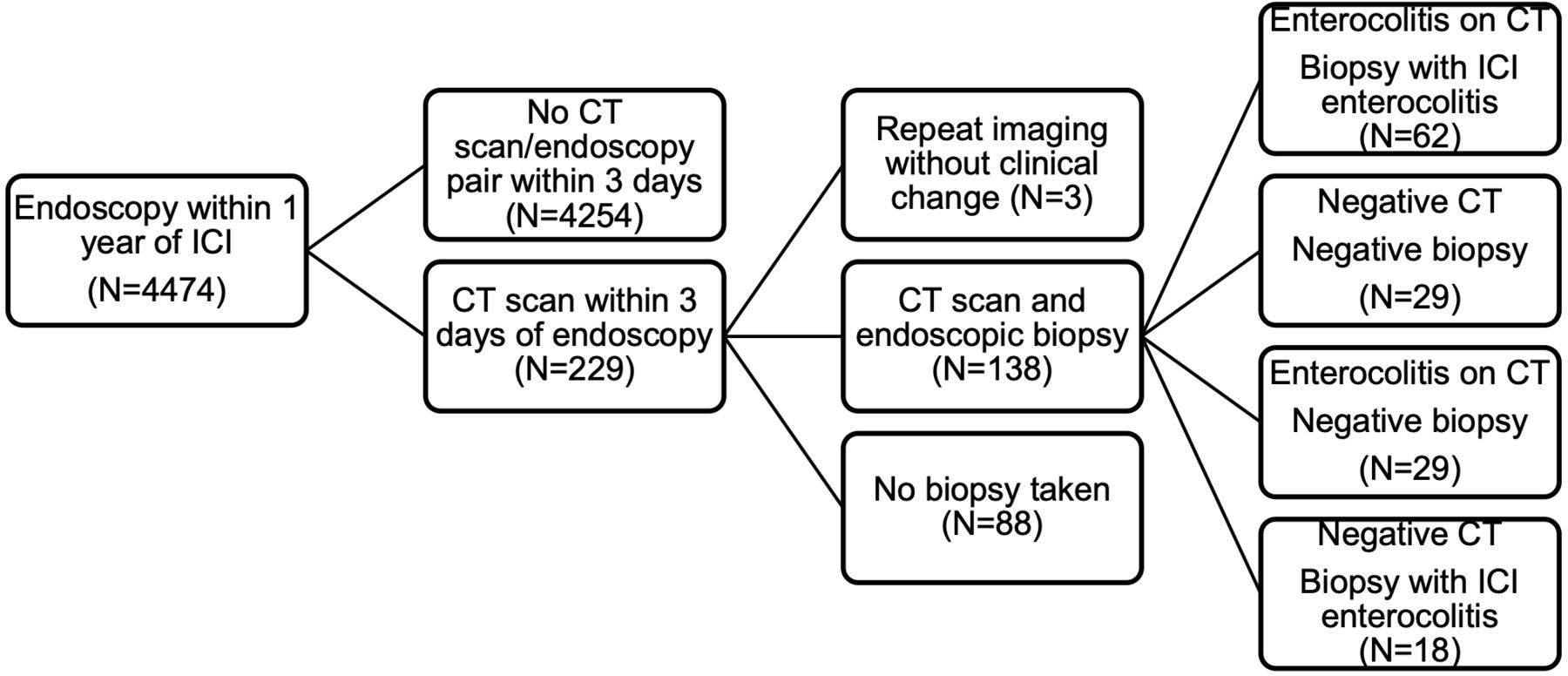
{kind=link}
Case identification. ICI, immune checkpoint inhibitor.
Patient demographics at time of biopsy
Presentation and evaluation
Treating clinicians were concerned for ICI enterocolitis prior to diagnostic workup in most patients (88%). In a small minority (12%), there was no concern for ICI enterocolitis documented in the medical record and patients underwent workup for alternative possible diagnoses, including esophagitis and gastrointestinal bleeding. Median CTCAE grade of diarrhea symptoms was 2.14 (IQR 2). Most patients underwent CT imaging with intravenous contrast (86%); nearly half (48%) received both intravenous and oral contrast. Seven per cent received oral contrast only and 7% had non-contrast CT scans. Median time from last ICI dose to endoscopy was 25 days. Most patients underwent flexible sigmoidoscopy, either alone (49%) or in combination with EGD (12%); others underwent colonoscopy, either alone (19%) or with EGD (5%). Fourteen per cent underwent EGD only. Macroscopic inflammation was seen on endoscopic evaluation in 58% of cases (table 2).
Clinical presentation, radiographic workup and endoscopic workup
Diagnosis and treatment
Fifty-five of the 138 patients (39%) meeting eligibility criteria had a diagnosis of enterocolitis in the radiology report. With expert review, the number of patients diagnosed with enterocolitis increased to 97 patients (70%). One hundred and eleven patients (80%) had biopsy findings consistent with enterocolitis of any etiology; eighty patients (58% of total) had biopsy-proven ICI enterocolitis. Of those with biopsy-proven ICI enterocolitis, median time to onset of symptoms was 74 days from start of ICI therapy. Most patients (70%) had grade 3 or higher colitis symptoms. Relative to CTCAE grade of diarrhea symptoms, grade of colitis symptoms was equal in 54 patients (67%), less severe in 5 patients (6%) and more severe in 21 patients (26%). Nearly all patients (91%) were treated with steroids; 45% were treated with additional therapies, including infliximab (40%) and vedolizumab (6%). Median time to symptom resolution was 25 days from documentation of symptom onset (table 3).
Characteristics of confirmed ICI enterocolitis cases
Evaluation of endoscopy
The test performance of endoscopy alone was evaluated in comparison to endoscopy with biopsy. Endoscopic findings of erythema and ulceration were correlated with a histologic diagnosis of ICI enterocolitis. The sensitivity and specificity for endoscopic evaluation alone, without biopsy, were 71% and 60%, respectively. The PPV was 71% and the NPV was 60%.
Evaluation of CT scan
The test performance of CT scan was evaluated in comparison to endoscopy with biopsy. Radiographic findings consistent with enterocolitis, including bowel wall thickening, mucosal or mural hyperenhancement, pericolonic stranding, fluid-filled loops of bowel and mesenteric hyperemia were correlated with a histological diagnosis of ICI enterocolitis. Based on radiology reports generated during standard care, the sensitivity and specificity for CT scan were 50% and 74%, respectively. The PPV was 73% and the NPV was 52%. Test characteristics were similar in the subgroups of patients treated with ICI targeting the PD-1/PD-L1 axis, as well as those treated with anti-CTLA-4 therapy. Expert radiology review identified 42 additional patients with imaging signs of enterocolitis, which increased the sensitivity of CT scan to 81%. The specificity decreased to 45% (table 4). When stratifying based on severity of diarrhea symptoms, CT scan had an improved PPV in those with high-grade symptoms (grades 3 and 4) compared with low-grade (grades 0–2) symptoms, both in real-world use and after expert review. However, sensitivity and specificity for both subgroups were similar to the overall sample (table 5).
Test performance of CT
Test performance of CT stratified by severity of diarrhea
We also evaluated the utility of CT scan in diagnosing enterocolitis of any etiology in this population. Findings of enterocolitis on imaging were correlated with a histological diagnosis of enterocolitis. Diagnoses included ICI enterocolitis, infectious enterocolitis, graft versus host disease and ischemic colitis. After expert review of imaging, the sensitivity and specificity for CT scan were 76% and 51%, respectively. The PPV was 86% and the NPV 37%.
Overall, of the 138 cases evaluated, 18 had a positive CT and signs of inflammation on biopsy without findings consistent with ICI enterocolitis. The most common diagnoses were viral enterocolitis (n=4) and ischemic colitis (n=3). Twelve cases had a positive CT and no signs of inflammation on biopsy; most commonly, symptoms and findings were non-specific, and the final diagnosis was not determined (n=7). Twelve patients were treated with at least one dose of steroids despite biopsies inconsistent with ICI enterocolitis.
Discussion
In this study, the utility of CT for diagnosis of ICI enterocolitis was found to be lower than had previously been reported.7 We evaluated the role of CT scan in a heterogeneous patient population representing multiple tumor types and patients treated with both CTLA-4 inhibitors and PD-1/PD-L1 inhibitors, which is more representative of real-world ICI use. Notably, median time from ICI start to symptom onset in this population was 10.5 weeks, with an IQR of 5–22 weeks. This wide-ranging time to symptom onset is in keeping with previous work, which has placed colitis onset from combination PD-1/CTLA-4 therapy at 6–8 weeks and from PD-1 monotherapy at 25.4 weeks, with a range from 0.6 to 119 weeks. This suggests that we are capturing a representative real-world population presenting with similar symptoms in a similar time course to what has been previously described.11 13 Patients generally had moderate to severe diarrhea on presentation. The majority of those diagnosed with ICI enterocolitis also had severe symptoms based on colitis grade and treatment response, including the need for intravenous steroids and second-line therapies including infliximab and vedolizumab. Importantly, only two-thirds of patients had concordant grade of diarrhea and grade of colitis, indicating that severe diarrhea does not always correspond with severe colitis that might be visible on imaging. Even after subgroup analysis of those with severe diarrhea, sensitivity and specificity of CT scan, both in everyday clinical practice and after expert review, remained moderate to poor.
We demonstrated the NPV of CT scan in everyday clinical practice is poor, improving to only 63% from 52% following expert review. Even with careful review of possible signs of inflammation by expert abdominal radiologists, CT scan does not capture all cases of ICI enterocolitis. Poor NPV, especially as defined in a population at a large academic cancer center with a high prevalence of ICI enterocolitis cases, makes CT scan especially limited in the workup of diarrhea and suspected colitis, as negative imaging will not rule out the diagnosis. Taken together, this work demonstrates that, both in real-world settings and after review by expert radiologists, CT currently has limited utility in the diagnosis of ICI enterocolitis and cannot substitute for endoscopy with biopsy. As ICI enterocolitis can progress rapidly, with worsening inflammation and increasing symptom severity if not diagnosed and treated promptly, endoscopic assessment with biopsy should be performed in all patients with suspicion of this immune-related adverse event.11 14
Consensus guidelines state that moderate to severe diarrhea (CTCAE grades 2–4) coupled with a negative infectious workup is sufficient to begin treatment with steroids, and even to escalate treatment to infliximab if ulceration is visible on endoscopy.2 8 9 Although endoscopic evaluation with biopsy is strongly recommended, it is not necessary prior to steroid initiation. Systemic steroids for the treatment of ICI enterocolitis are not benign, potentially abrogating the antitumor response of ICI and leading to reduced survival.15 As such, the consideration of multiple diagnoses and a comprehensive workup should be undertaken prior to starting immunosuppressive therapy. Here, we demonstrate that CT alone is an insufficient work up. A negative CT scan should not rule out the need for GI consultation and endoscopy with biopsy.
This study has several limitations. It is retrospective and limited to three hospitals within a single healthcare system. Although the inclusion of multiple hospitals allows for more generalizable conclusions, all sites have a high volume of patients treated with ICI, and therefore, increased incidence in ICI enterocolitis. They have highly specialized physicians with ICI expertize, so these results may not be generalizable to settings with different patient populations and without access to prompt endoscopic evaluation. We chose to focus on a heterogeneous patient population representing many malignancies, therapies and clinical presentations. Although we believe that this varied sample provides valuable real-world evidence, the heterogeneity may obscure important positive relationships between CT scan and diagnosis of ICI enterocolitis, as was seen previously in a more focused study examining melanoma patients presenting with diarrhea.7 A larger sample size would allow for more detailed subgroup analysis and the possible identification of patient populations for whom CT scan may play a more important role in diagnosis.
Patients were also evaluated with a range of endoscopic methods. Patients who only underwent endoscopy of the upper gastrointestinal tract may have had colonic inflammation and vice versa. Prior work has demonstrated that alterations in gastric mucosa are associated with ICI injury, and can be seen more frequently than inflammation in the colon, suggesting that EGD may be sufficient for diagnosis of ICI enterocolitis in many patients.16 In our subset of patients that underwent EGD only, one patient had isolated colitis on CT scan without radiographic evidence of concurrent gastroenteritis. This patient was ultimately found to have pathological evidence of ICI enterocolitis in the gastric mucosa. Nevertheless, the lack of consistency of endoscopic methods in this data set may have resulted in the missed diagnosis of ICI enterocolitis in some patients.
In patients with suspected enterocolitis, CT remains important for the exclusion of extraluminal complications such as perforation and abscess formation in patients considered clinically at risk but cannot presently substitute for endoscopy with biopsy. Endoscopy has the added advantage of the ability to assess the severity of mucosal inflammation, potentially helping to guide enterocolitis therapy, although we show that endoscopy alone cannot substitute for biopsy evaluation.17–20 However, endoscopy with biopsy is time-intensive and resource-intensive and may not be a readily available diagnostic tool in all settings. Continued exploration of possible noninvasive biomarkers and previously unidentified radiological signatures will be necessary to advance the care of patients presenting with concern for ICI enterocolitis.
References
Footnotes
Contributors SD performed the data extraction and analysis with assistance from MJM, LZ and DFC. AK and NP reviewed all of the radiology images and reported and provided the expert analysis with assistance from FJF. KLR and MD supervised the project. SD, KLR and MD wrote the paper with input from all of the authors.
Funding MD is supported by National Institutes of Health Mentored Clinical Scientist Development Award 1K08DK114563-01 and the American Gastroenterological Association Research Scholars Award.
Competing interests MJM. is a consultant and received honoraria from AstraZeneca. MD is a consultant for Tillotts Pharma, Partner Therapeutics, ORIC Pharmaceuticals, and Genentech-Roche, receives research funding from Novartis, and is on the Scientific Advisory Board for Neoleukin. All other authors declare no competing interests.
Patient consent for publication Not required.
Ethics approval The study was approved by the Partners Healthcare Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. All available data are published in the manuscript.