Article Text

Abstract
Background To determine safety and efficacy of single cycle induction treatment with cisplatin/docetaxel and durvalumab/tremelimumab in stage III-IVB head and neck cancer.
Methods Patients received a single cycle of cisplatin 30 mg/m² on days 1–3 and docetaxel 75 mg/m² on day 1 combined with durvalumab 1500 mg fix dose on day 5 and tremelimumab 75 mg fix dose on day 5. Patients with pathologic complete response (pCR) in the rebiopsy after induction treatment or at least 20% increase of intratumoral CD8+ cell density in the rebiopsy compared with baseline entered radioimmunotherapy with concomitant durvalumab/tremelimumab. The objective of this interim analysis was to analyze safety and efficacy of the chemoimmunotherapy-induction treatment before radioimmunotherapy.
Results A total of 57 patients were enrolled, 56 were treated. Median pretreatment intratumoral CD8+ cell density was 342 cells/mm². After induction treatment, 27 patients (48%) had a pCR in the rebiopsy and further 25 patients (45%) had a relevant increase of intratumoral CD8+ cells (median increase by a factor of 3.0). Adverse event (AE) grade 3–4 appeared in 38 patients (68%) and mainly consisted of leukopenia (43%) and infections (29%). Six patients (11%) developed grade 3–4 immune-related AE. Univariate analysis computed p16 positivity, programmed death ligand 1 immune cell area and intratumoral CD8+ cell density as predictors of pCR. On multivariable analysis, intratumoral CD8+ cell density predicted pCR independently (OR 1.0012 per cell/mm², 95% CI 1.0001 to 1.0022, p=0.016). In peripheral blood CD8+ cells, the coexpression of programmed death protein 1 significantly increased especially in patients with pCR.
Conclusions Single cycle induction treatment with cisplatin/docetaxel and durvalumab/tremelimumab is feasible and achieves a high biopsy-proven pCR rate.
- radioimmunotherapy
- head and neck neoplasms
- CD8-Positive T-lymphocytes
- clinical trials
- Phase II as topic
- combined modality therapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- radioimmunotherapy
- head and neck neoplasms
- CD8-Positive T-lymphocytes
- clinical trials
- Phase II as topic
- combined modality therapy
Introduction
Immune checkpoint inhibitors directed against programmed death protein 1 (PD-1) have become standard treatment in patients with recurrent and/or metastatic head and neck squamous cell carcinoma (HNSCC).1 2 A first phase Ib trial proved the feasibility of the PD-1 inhibitor pembrolizumab in combination with radiochemotherapy with weekly administration of cisplatin in locally advanced tumors.3 The ongoing phase III trials Keynote-412 and Javelin head and neck 100 add anti-PD(L)1 agents to standard radiochemotherapy with three administrations of high-dose cisplatin in locally advanced tumors. However, recently it was reported in a press release that Javelin head and neck 100 will not meet its primary endpoint.
Beside primary radiochemotherapy, the strategy of induction chemotherapy followed by radio(chemo)therapy has become a treatment option for laryngeal cancer.4 However, when this strategy was expanded to other locations in the head and neck, randomized trials failed to prove a survival benefit compared with radiochemotherapy alone.5 In more recent trials using induction chemotherapy, excellent responders were identified after three cycles and subsequently treated with dose and volume-reduced radiotherapy in order to minimize late toxicity.6 7
The CheckRad-CD8 study was conducted to develop an efficient single cycle induction therapy, which allows patient selection for a further chemotherapy-free treatment based on pathologic response evaluation. Induction treatment consisted of cisplatin, docetaxel, durvalumab and tremelimumab. Patients with pathologic response entered definitive radiation therapy combined with durvalumab and tremelimumab followed by durvalumab maintenance, here called radioimmunotheapy.
The combination of durvalumab with platinum-based chemotherapy was studied in the phase III CASPIAN trial in extensive-stage small cell lung cancer. In this trial, the addition of durvalumab increased overall survival (OS) without relevant increase in toxicity.8 The combination of durvalumab and tremelimumab with chemotherapy was studied in the Canadian phase IB IND226 trial mainly in patients with lung cancer. This was the first trial that proved the feasibility of a quadruple combination consisting of durvalumab and tremelimumab in combination with platinum-doublet chemotherapy and provided first dose recommendations.9
In this interim analysis of the CheckRad-CD8 trial the safety, antitumor activity and biological response of this single cycle induction treatment were studied in locally advanced HNSCC. To our knowledge, this is the first report on safety and antitumor activity of a combination scheme consisting of chemotherapy, programmed cell death ligand 1 (PD-L1) and cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) antagonists.
Material and methods
Trial design and treatment
CheckRad-CD8 is a multicenter open-label phase II study with a single treatment arm in patients with locally advanced HNSCC. Eligible patients received a single cycle of induction treatment in week 1 with cisplatin 30 mg/m² body surface area (BSA) on days 1–3 and docetaxel 75 mg/m² BSA on day 1. In patients with impaired renal function, cisplatin could be replaced by carboplatin AUC 1.5 on days 1–3. The immune checkpoint inhibitors tremelimumab (anti-CTLA4) at a fixed dose of 75 mg and durvalumab (anti-PDL1) at a fixed dose of 1500 mg were both administered on day 5. Restaging was performed in week 4 with contrast-enhanced CT or MRI of the neck and endoscopy with representative rebiopsy. The density of intratumoral CD8+ cells was assessed via immunohistochemistry and digital image analysis before treatment and in the rebiopsy at the restaging. Biopsies were always taken of the primary tumor and not of the lymph nodes. Patients with at least stable disease in imaging according to RECIST 1.1 criteria and an increase of intratumoral CD8+ cells of at least 20% compared with baseline continued with trial treatment and entered radioimmunotherapy. Also patients with no remaining tumor in a sufficiently covered tumor bed in the rebiopsy (pathologic complete response, pCR) continued with trial treatment. Coverage of a former tumor bed was considered to be sufficient, if a relevant resorptive inflammation (macrophages, neutrophil granulocytes, lymphocytes) in conjunction with granulation and scar tissue could be found in post therapeutic biopsies. To ensure that minute residual tumor parts were not overseen, multiple section levels were evaluated (six levels per specimen). These patients received radiotherapy up to 70 Gy in 35 fractions with additional three cycles of combined durvalumab/tremelimumab, followed by 8 cycles of durvalumab monotherapy administered every fourth week. Patients not meeting these criteria receive standard radiochemotherapy outside the trial.
Trial oversight
The trial was registered with ClinicalTrials.gov (identifier: NCT03426657). All patients gave written informed consent before the first study procedures were performed.
Patients
Eligible patients had histologically confirmed HNSCC stage III-IVB of the oral cavity, oropharynx, hypopharynx or supraglottic larynx. Main inclusion criteria were an Eastern Cooperative Oncology Group (ECOG) performance status of 0–1, adequate bone marrow, hepatic and renal function and provided tumor tissue for CD8+ cell assessment in central pathology. Main exclusion criteria were prior surgical procedures or systemic treatments of the HNSCC, autoimmune diseases and history of radiotherapy to the head and neck region.
Endpoints and assessments
Co-primary endpoints of the CheckRad-CD8 trial are the feasibility of induction chemoimmunotherapy followed by radioimmunotherapy and the predictive character of changes of the intratumoral CD8+ immune cells. Key secondary endpoints are OS and progression-free survival. In this interim analysis, the safety and efficacy of this single cycle induction treatment before radiotherapy were studied together with first biomarker analyses. Toxicity was evaluated weekly from study inclusion until after the restaging assessments (before radiotherapy) using the Common Terminology Criteria for AE (CTCAE version 4.03). Pathologic response was assessed centrally in the Institute of Pathology Erlangen and scored as rate of patients without residual tumor in rebiopsy (CR). The intratumoral CD8+ cell density was analyzed quantitatively. Response by imaging was evaluated according to RECIST 1.1 criteria by the investigators, there was no central review.
Biomarker analyses
Immunohistochemistry
Immunohistochemistry was performed on 2 µm whole slide sections on a Ventana Benchmark Ultra autostainer (Ventana) according to accredited staining protocols (https://www.dakks.de/en) using the following antibodies: PD-L1 (closed SP263 assay, Ventana; companion diagnostic assay for durvalumab/tremelimumab), CD8 (C8/144B, mouse monoclonal; ThermoFisher-Scientific; dilution 1:100). All sections were counterstained with hematoxylin. PD-L1 positive immune cells (ICs) and tumor cells (TCs) were scored by two systematically trained pathologists according to the distributor’s PD-L1 scoring algorithm (‘AstraZeneca’/Durvalumab algorithm). PD-L1 positive TCs were scored as percentage of the PD-L1 positive TC area per total TC area (%; positive tumor cell area/total tumor cell area; Ventana TC-score). PD-L1 positive ICs were scored as proportion of the area occupied by PD-L1 positive tumor-associated IC per total area occupied by tumor-associated IC (%; area occupied by positive IC/total area occupied by IC; Ventana IC-area score). Whole tissue sections stained for CD8 were scanned using the Panoramic P250 slide scanner (3DHistech) and imported into QuPath (QuPath v0.2.0).10 Regions of interest (ROI; tumor cell area, tumor-associated stroma area, total tumor area) were annotated manually by an experienced pathologist, and cells were quantified automatically with the ‘Positive Cell Detection’ tool for immunohistochemically stained slides. CD8+ cytotoxic T cells were quantified absolutely per millimeter square in all ROIs.
Multicolor flow cytometry
Whole blood samples of the patients were collected and analyzed by multicolor flow cytometry according to our previously published modularly immunophenotyping (IPT) protocols.11 12 Direct antibody staining of whole blood samples was performed without previous isolation of blood mononuclear cells, which allows the detection of all types of circulating ICs, including granulocytes. IPT was performed within 24 hours after the collection of whole blood. Data were acquired on a Gallios Flow Cytometer (Beckman Coulter, Brea, California, USA) in the standard filter configuration. The Kaluza Flow Analysis Software (Beckman Coulter) was used for data analyses.
Statistical analysis
The current interim analysis is an unplanned exploratory analysis, which was performed after an unexpected high rate of pCRs was detected in the first preplanned safety interim analysis after 30 patients.
The Wilcoxon-Mann-Whitney test and the Wilcoxon signed-rank test were used to compare continuous variables, that is, intratumoral CD8+ cells and PD-L1, in dependence of treatment response and HPV status, and between different time points of measurement, respectively. Fisher’s exact test was used to identify categorical predictive parameters for pCR in univariable analyses. In the multivariable analysis, logistic regression was applied considering all factors with a univariable p value of <0.1 to identify independent prognostic factors for pCR.
Statistical analyses were carried out using the software packages R, NCSS and GraphPad Prism V.8.1.2 (GraphPad Software, California, USA).
Results
Patient characteristics and treatment parameters
Fifty-seven patients were enrolled from September 2018 to December 2019 in seven German centers. One patient did not receive any dose of either drug due to tumor bleeding and was excluded from all analyses. Baseline characteristics are given in table 1. As the tumor, node, metastases (TNM) seventh edition was replaced during the trial, all tumor stages were adapted to the eighth edition (UICC stage according to the TNM seventh edition is given in the online supplemental table 1). PD-L1 status was scored as percentage of total tumor cell area with the previously established cut-off value of 25% for durvalumab±tremelimumab in HNSCC.13 PD-L1 was high (area ≥25%) on TCs in 10 patients (18%) and on ICls in 21 patients (38%). Six patients (11%) received carboplatin instead of cisplatin. Two patients (4%) received only induction chemotherapy without immune checkpoint inhibitors due to AE (one infection and one elevated transaminases).
Supplemental material
Patient characteristics of treated patients
Safety analyses
Adverse events (AEs) occurring between study inclusion and the end of the restaging assessments are listed in table 2. Among all patients enrolled, 52 (93%) experienced an AE of any grade. There were 37 patients (66%) who experienced a grade 3 AE and 7 patients (13%) who experienced a grade 4 AE, with 38 patients (68%) having at least one grade 3–4 AE (95% CI 54% to 80%). Most common AE grade 3–4 were leukopenia in 24 patients (43%) and infections in 16 patients (29%). The median duration of AEs grade 3–4 was 7 days. Detailed data about the duration of toxicities on patients’ level are shown in figure 1. Six patients (11%) developed grade 3–4 immune-related AE (irAE) including hepatitis in three patients, diarrhea in two patients and pancreatitis in one patient. One additional patient developed grade 3 elevated transaminases without prior immune checkpoint inhibitors. Study treatment was discontinued after the restaging assessment due to toxicity in six patients, including the above-mentioned three cases of hepatitis, one infection grade 4, one immune-related diarrhea grade 3 and one nephritis grade 2. These patients were subsequently treated with definitive radiotherapy with simultaneous chemotherapy or cetuximab outside the study protocol. Immune-suppressive medication for AE management was administered in eleven patients (20%). Reasons for systemic corticosteroids were the six grade 3–4 irAE mentioned above and further three cases of grade 2 diarrhea and one case of grade 2 nephritis. One patient received topical corticosteroids due to exanthema grade 1. The patient with hepatitis grade 4 was additionally treated with mycophenolat-mofetil.
Adverse events
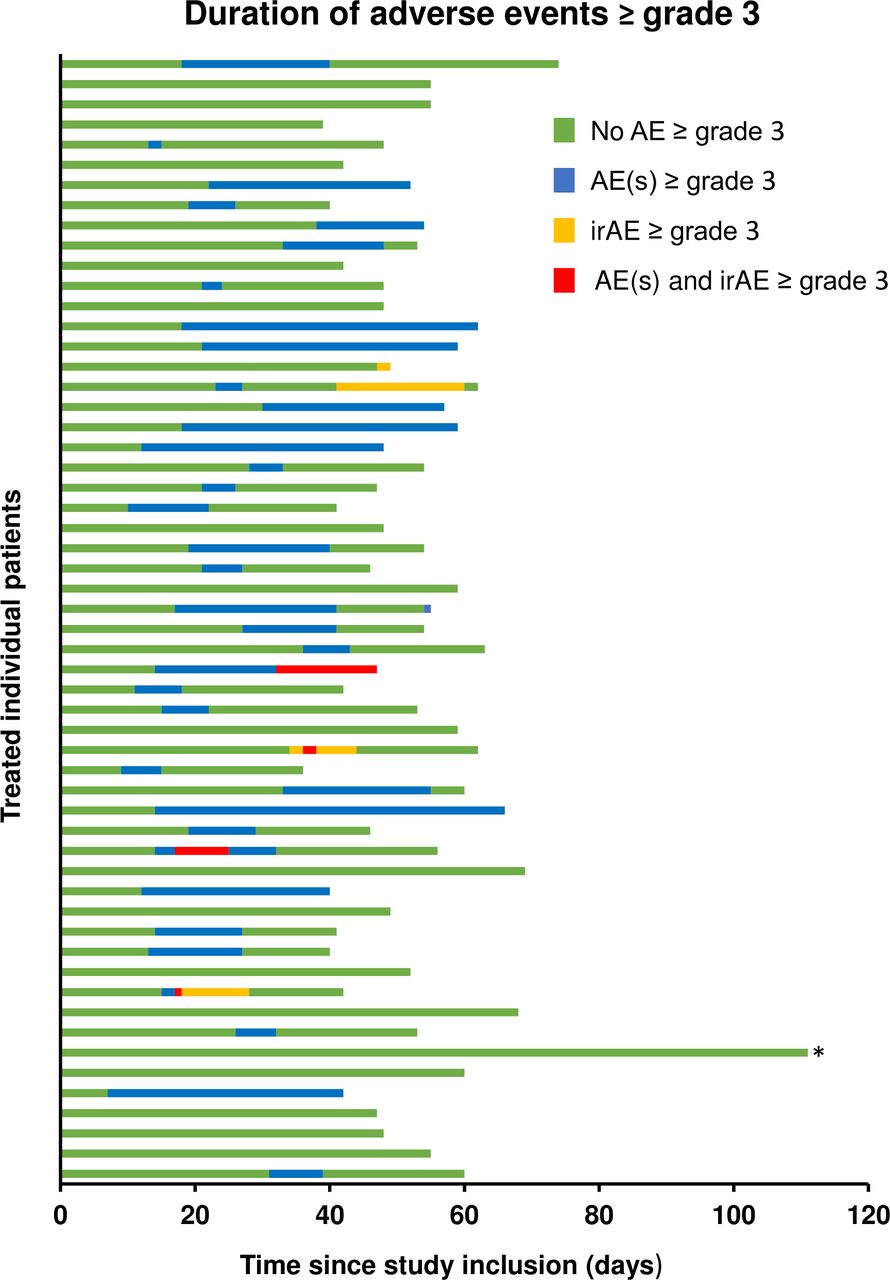
Duration of adverse events (AEs) ≥grade 3. The swimmer plot presents the duration of AE ≥grade 3 separated in conventional AE and immune-related AE (irAE) on patients level. Each bar represents an individual patient. Toxicity was assessed from study inclusion until the end of the restaging period (day before the first fraction of radiotherapy) or the safety follow-up (before subsequent treatment). *This patient denied further treatment after complete response (CR); after a follow-up of 12 months, the tumor is still in CR.
Efficacy outcomes
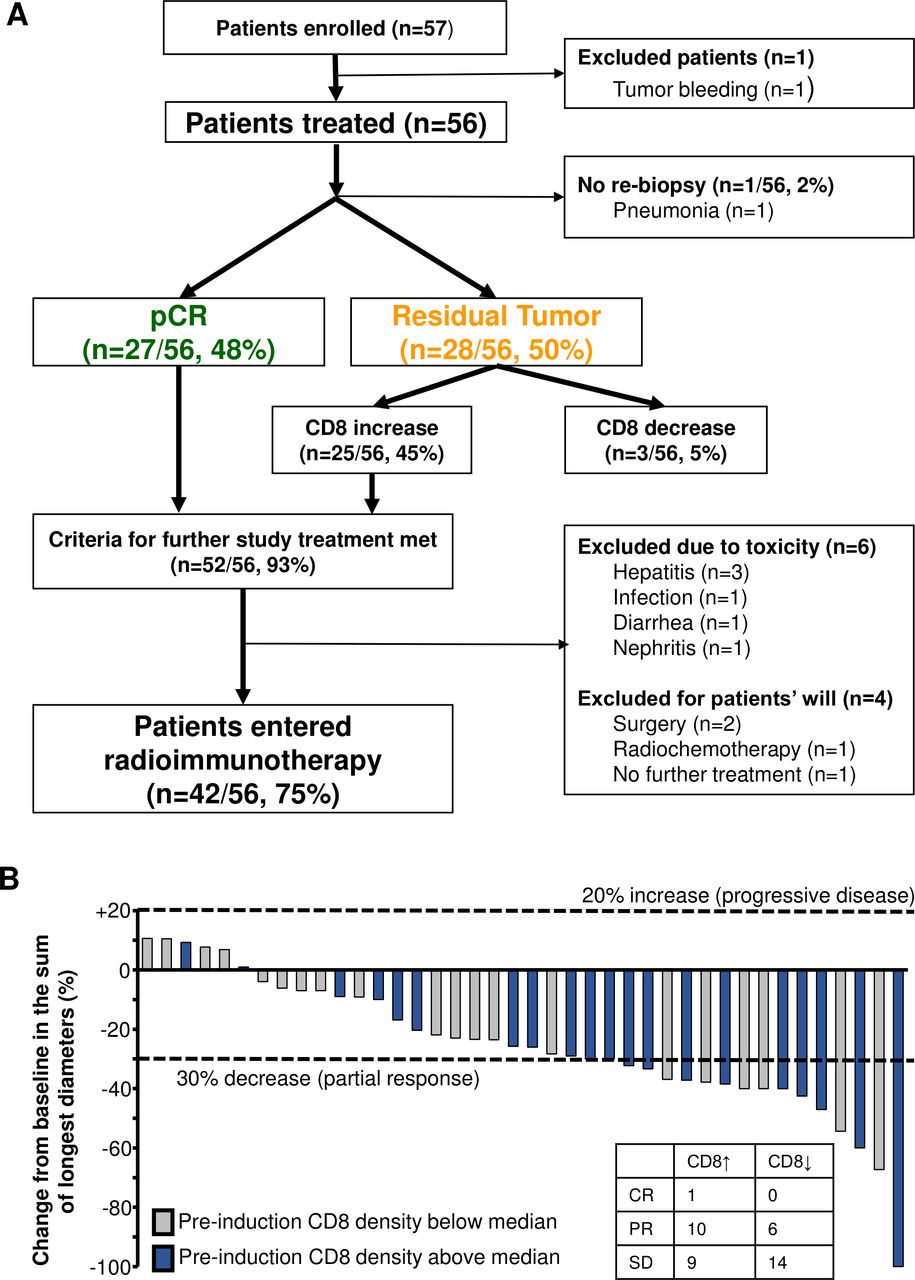
Restaging assessment with panendoscopy and rebiopsy of the primary tumor was performed in 55 of 56 treated patients (see figure 2A). The major finding of this trial was that 27 patients (48%; 95% CI 35% to 62%) had no residual primary tumor in the rebiopsy (pCR). In the other 28 patients with residual primary tumor, 25 patients (45%) had an intratumoral CD8+ cell increase of at least 20%, which is the cut-off value for further study treatment. In three patients (5%) CD8+ cells decreased. Taken together, 52 patients (93%) fulfilled the criteria for further study treatment. Six patients had to be excluded from further study treatment due to treatment-related AE and four patients decided for alternative or no further treatment. Finally, 42 patients (75%) entered radioimmunotherapy within the trial.

Consolidated Standards of Reporting Trials (CONSORT) diagram and treatment response. (A) CONSORT diagram including pathologic treatment response. pCR, pathologic complete response. (B) Radiographic response in dependence of baseline intratumoral CD8+ cell density (CD8↑, preinduction CD8 density above median; CD8↓, preinduction CD8 density below median). The radiographic response was evaluated according to RECIST 1.1 criteria. Tumor responses were measured at baseline and at the restaging before radiotherapy. The values shown are the percentage change in the sum of longest diameters. Each bar represents one patient. CR, complete response; PR, partial response; SD, stable disease.
Radiographic treatment response was evaluated according to RECIST 1.1 criteria (see figure 2B). In 40 evaluable patients, one (3%) had a complete response (CR), 16 (40%) had partial responses (PR) and 23 (58%) stable diseases. There was no progressive disease. When the responses are compared with the preinduction intratumoral CD8+ cell densities, 11 of the 17 responding patients had an intratumoral CD8+ cell density above the median.
Biomarker analyses
Immunohistochemistry
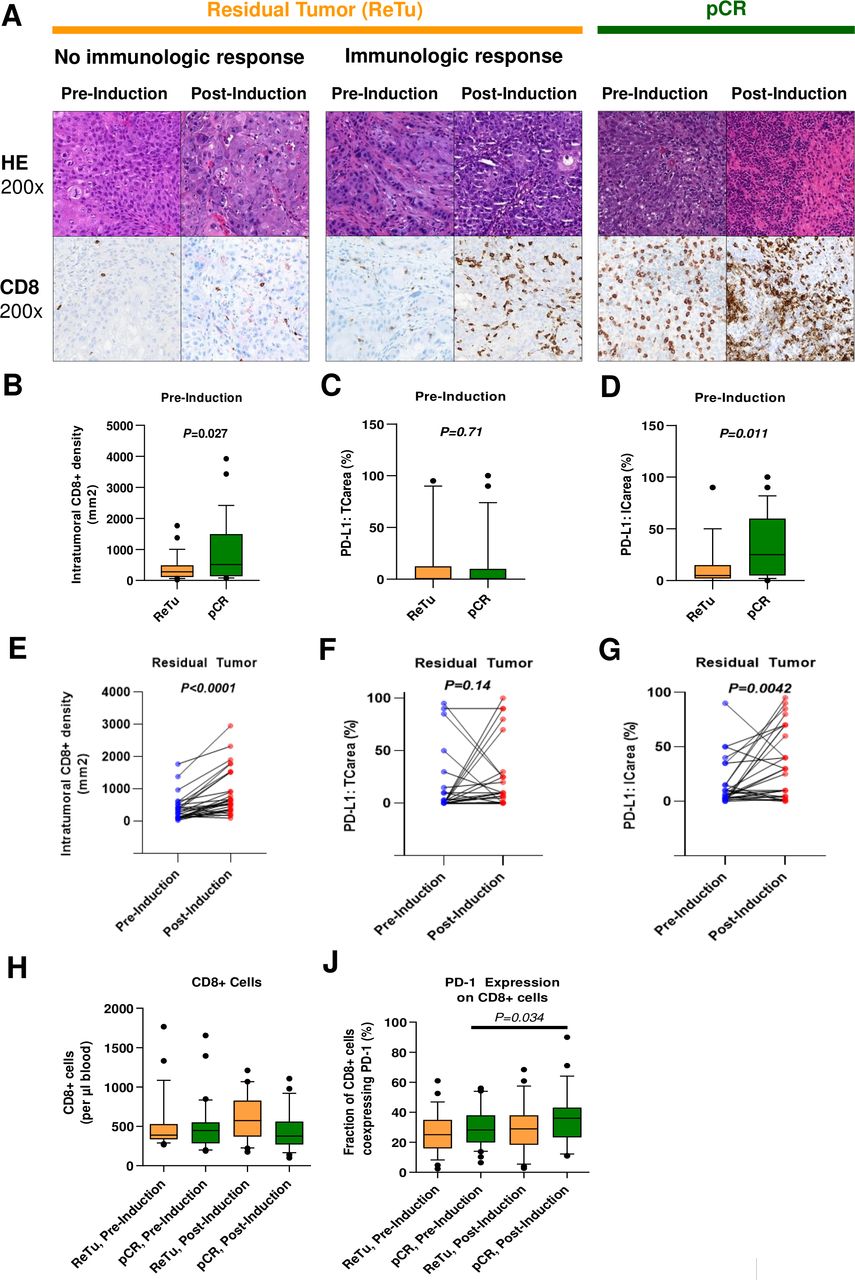
Intratumoral CD8+ cell density and PD-L1 were prospectively analyzed in the preinduction and postinduction tissue. Tissue was available preinduction in all 56 treated patients and postinduction in 55 patients. Preinduction and postinduction histologic findings of representative patients with residual tumor (without and with immunological response) and pCR are shown in figure 3A. The median pretreatment intratumoral CD8+ cell density was 342 cells/mm² (range 22–3922 cells/mm²). The preinduction intratumoral CD8+ cell density was significantly higher in patients who developed a pCR than in patients with residual tumor (figure 3B). The preinduction PD-L1 tumor cell area (TCarea) did not differ significantly between patients with pCR and residual tumor (figure 3C). In contrast, the preinduction PD-L1 immune cell area (ICarea) was significantly higher in cases with pCR (figure 3D). In patients with residual tumor, the intratumoral CD8+ cell density increased after induction treatment (figure 3E) by a median factor of 3.0. In contrast to tumor cells, induction treatment led to a significant increase of PD-L1 expression on immune cells (figure 3F,G). The raw data of these analyses are displayed in the online supplemental table 2. Human papilloma virus (HPV) positive tumors had a significantly higher preinduction CD8+ cell density compared with HPV-negative tumors (online supplemental figure 1A). The PD-L1 TCarea did not differ significantly in HPV positive and negative tumors. In contrast, HPV-positive tumors showed a significantly increased PD-L1 ICarea (online supplemental figure 1B,C).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Histological parameters associated with treatment response. HE and immunohistochemical CD8 staining (brown) of representative patients. Residual tumors (ReTu) without immunologic response typically showed no tumor-infiltrating immune cells preinduction and postinduction neither in the HE nor in the CD8 staining. In residual tumors with immunological response, an increase of intratumoral immune cells is typically found both in HE and CD8 staining postinduction compared with preinduction. In patients who developed pCR, tumor-infiltrating immune cells are typically present preinduction and even increase post-induction. Comparison of (B) intratumoral CD8+ cell density, (C) programmed cell death ligand 1 (PD-L1) tumor cell area (TC area) and (D) PD-L1 immune cell area (IC area) in patients with residual tumor (ReTu) and pathologic complete response (pCR). Changes of (E) intratumoral CD8+ cell density, (F) PD-L1 TC area and (G) PD-L1 IC area before and after induction treatment in patients with residual tumor. (H) Peripheral blood concentration of CD8+ cells before and after induction treatment in patients with ReTu and pCR. (J) PD-1 coexpression of peripheral blood CD8+ cells before and after induction treatment in patients with ReTu and pCR.
Univariable analyses identified p16 positivity, PD-L1 IC area and intratumoral CD8+ cell density as significant positive predictors of pCR (online supplemental table 3). Additionally, a significant correlation between the amount of PD-L1+ with CD8+ ICs was found (PD-L1 ICarea ≥25%: median 619 CD8+ cells/mm² vs PD-L1 ICarea <25%: median 264 CD8+ cells/mm², p=0.0009). As this correlation has also been described before14 and recently also the functional role of the expression of PD-L1 on CD8+ lymphocytes was published in detail,15 PD-L1 on ICs was excluded from the multivariable analysis. In the multivariable analysis, intratumoral CD8+ cell density remained an independent predictor of pCR (OR 1.0012 per cell/mm², 95% CI 1.0001 to 1.0022, p=0.016), whereas p16 positivity lost its statistical significance.
Multicolor flow cytometry
Due to this crucial role of the CD8+ cytotoxic T cells in the tumor, this cell type was also studied in the peripheral blood. The number of CD8+ cytotoxic T cells showed no significant differences in patients with pCR or residual tumor and did not change significantly after induction treatment (figure 2H). However, PD-1 coexpression significantly increased after induction treatment especially in patients with pCR (figure 2J).
Discussion
The results of the CheckRad-CD8 trial support the feasibility of the combination of docetaxel/cisplatin with durvalumab/tremelimumab as single cycle induction treatment in locally advanced HNSCC. The feasibility of radiotherapy combined with durvalumab/tremelimumab, including the whole safety of all the treatment, will be studied in a future analysis. Grade 3–4 AE mainly consisted of leukocytopenia and infections. This may be prevented by prophylactic use of G-CSF, which was not part of the study protocol. However, prophylactic G-CSF has to be discussed critically, as it may also increase myeloid-derived suppressor cells leading to impaired tumor control.16 The incidence of irAE grade 3–4 in 11% of the patients was in the expected range and the events were treated effectively by immune-suppressive treatment. The first study that established data on feasibility of durvalumab and tremelimumab in combination with platinum-doublet chemotherapy was the Canadian IND226 trial.9 In this trial, patients with different tumors, mainly non–small cell lung cancer, received durvalumab and tremelimumab at different dose levels in combination with chemotherapy. The studied chemotherapy regimens included pemetrexed/platinum, gemcitabine/platinum, etoposide/platinum and nab-paclitaxel/carboplatin, but not the scheme of the CheckRad-CD8 trial docetaxel/platinum. Treatment was feasible up to the highest dose level of 1500 mg durvalumab q3w (every three weeks) and 75 mg tremelimumab q3w (up to four doses of tremelimumab). The frequency of irAE ≥grade 3 was 21% compared with 11% in the CheckRad-CD8 trial. As this analysis of the CheckRad-CD8 trial focuses on the period until the end of the restaging assessments, additional late irAE might increase the rate of irAE. In the IND226 study, irAE ≥grade 3 mainly consisted of diarrhea (9%), which also appeared in the CheckRad-CD8 trial (4%). The most frequent irAE ≥grade 3 in CheckRad-CD8 was hepatitis (5%), which also appeared in 3% in IND226. The studied induction treatment resulted in a high rate of biopsy-proven pCR in 48% of the patients after only a singe cycle of induction chemoimmunotherapy. In further 45% of the patients, intratumoral CD8+ cells increased, which has previously been described as predictor of treatment response to PD-1 antagonists.14 Patient selection was based on biopsies and not imaging, as the time period of a single cycle induction treatment is too short to allow sufficient tumor shrinkage. The pathologic response assessment in a rebiopsy opens the opportunity to study new pathologic parameters besides pCR as possible predictive values. A similar approach was performed in a study with neoadjuvant pembrolizumab using tumor necrosis, giant cells and histiocytic reaction as response criteria.17
The rate of clinical complete responses after three cycles of docetaxel, cisplatin and 5-fluorouracil 5FU (TPF) ranges from 17% to 43% in phase III trials with unselected patients.18–22 However, data about biopsy-proven pCR rates after induction chemotherapy are limited. In a Spanish phase III trial, biopsies were performed in a quarter of the 382 randomized patients, and a biopsy-proven pCR was found in 42% of the patients after three cycles of paclitaxel/cisplatin/5FU arm compared with 23% in the cisplatin/5FU arm.19 In a GORTEC trial, biopsies were performed in half of the 213 randomized patients, and a biopsy-proven pCR was found in 64% of the patients after three cycles TPF compared with 36% in the cisplatin/5FU arm.20 In a phase II trial with three cycles of TPF induction before planned surgery, the pCR rate of the primary tumor was 33%.23 A limitation of the CheckRad-CD8 trial is that only biopsies and not complete surgical specimens were available, which probably has a reduced sensitivity in the detection of residual TCs and may lead to an overestimation of the pCR rate. Taken together, the efficacy of only a single cycle induction treatment with cisplatin/docetaxel and durvalumab/tremelimumab seems to be at least comparable with three cycles of TPF induction.
Two phase II trials containing 21 and 28 patients, respectively, studied a single dose of pembrolizumab before planned surgery in locally advanced HNSCC.17 24 A limitation of the comparison of these trials with the CheckRad-CD8 trial is that in these trials complete surgical specimens were available compared with biopsies in CheckRad-CD8. However, as altogether only one pCR appeared in these two trials, the single agent induction seems to be less effective in inducing pCR compared with the combined induction therapy of the CheckRad-CD8 trial. In the IMCISION trial containing 12 patients, treatment consisted of two doses of nivolumab alone or in combination with a single dose of ipilimumab in a neoadjuvant setting.25 Their findings of one ‘near complete response’ in the monotherapy arm and two ‘near complete responses’ in the combined arm, together with an increased immune-related gene expression in the combined arm, favor a combined approach. In the CIAO trial, 28 patients received two cycles of neoadjuvant durvalumab either alone or in combination with tremelimumab.26 Two of 25 patients (8%) developed a pCR. Interestingly, three patients who received subsequent induction chemotherapy all developed pCR of their primary tumor, which favors induction treatments of combined chemoimmunotherapy. Similar approaches were also studied in non–small cell lung cancer. Two preoperative doses of nivolumab induced pCR of the primary tumor in 3e of 20 resected tumors (15%).27
In the phase III EAGLE trial, both durvalumab alone and durvalumab with tremelimumab failed to prove a significant improvement of OS compared with second line chemotherapy in recurrent and/or metastatic HNSCC.13 However, the 1-year survival rate of durvalumab with 37% was comparable to second line trials with nivolumab with 36% or pembrolizumab with 37%, whereas the 1-year survival rate of durvalumab with tremelimumab was only 30%.2 13 28 The results of the phase III KESTREL trial with a durvalumab/tremelimumab combination in first-line treatment are still outstanding. As tremelimumab enhances T-cell priming in an early phase, the combination with single PD-(L)1 agents that only can release a pre-existing immune reaction may not be efficient. Nevertheless, the combination with cell death inducing agents as chemotherapy or radiotherapy may release a real benefit of tremelimumab.29 30
The median pretreatment intratumoral CD8+ cell density of 342 cells/mm² in the CheckRad-CD8 trial is in line with previous reports with ranges between median cell densities of 220/mm² in the tumor center and 545/mm² in the invasive margin.31 The presented results of the CheckRad-CD8 trial emphasize the value of the baseline intratumoral CD8+ cell density as independent predictor for pCR after induction chemoimmunotherapy. These findings are in line with previous reports on the predictive role of intratumoral CD8+ cells in PD-1 inhibitor monotherapy.14 However, in the CIAO trial using immunotherapy without chemotherapy, no predictive value of intratumoral CD8+ cell density was reported.26 Tumor-infiltrating immune cells also have a prognostic value in chemoradiotherapy of HNSCC, whereas their role in chemotherapy alone is not clear.32 33 In the CheckRad-CD8 trial, patients with residual tumor had a median increase of intratumoral CD8+ cell density by a factor of 3.0. In the CIAO trial, CD8 density also increased, but only by a factor of 1.3 for durvalumab monotherapy and a factor of 1.2 for durvalumab combined with tremelimumab.26 The reason for this more intense immune activation in the CheckRad-CD8 trial is probably the combination with chemotherapy as especially docetaxel is expected to have immune-modulating properties.34 A limitation of the CD8 measurement and PD-L1 analyses is that intratumoral heterogeneity cannot be evaluated as only biopsies were analyzed in the CheckRad-CD8 trial. Regarding the staining method and subsequent pathologic evaluation, CD8+ cells have already been validated for colon cancer.35
Recent phase III trials with PD-1 inhibitors in HNSCC typically use PD-L1 on tumor cells or combined on TCs and ICs as predictive marker.1 2 28 In the CheckRad-CD8 trial, only PD-L1 on ICs and not on TCs was a predictor of pCR in the univariate analysis. Interestingly, this finding of a better predictive value of PD-L1 on immune cells compared with TCs has also been described before for PD-1 inhibitor monotherapy.36
HPV-positive tumors are typically identified via p16 immunohistochemistry and have superior prognosis, especially if treated with radiochemotherapy or induction treatment followed by radiochemotherapy,37 38 which has been attributed to significantly higher immune responses especially to HPV-positive oropharyngeal HNSCC.39 This effect was also found in a recent phase IB trial when radiochemotherapy was combined with pembrolizumab in locally advanced HNSCC.3 In the CheckRad-CD8 trial, p16 positive tumors had a higher CD8+ cell density and higher PD-L1 immune cell area compared with p16 negative tumors. Increased densities of tumor-infiltrating immune cells in p16-positive tumors have also been reported previously.40 Despite this increased immune cell infiltration in p16-positive tumors, the immune cell composition of T-cell subsets is similar to p16-negative tumors, but B-cells seem to differ in both tumor types.41 In a recent meta-analysis, patients with p16-positive HNSCC treated with immune checkpoint inhibitors had a favorable OS.42 This is in line with the CheckRad-CD8 trial, as p16 positivity had a positive predictive value for pCR after induction chemoimmunotherapy.
Another new finding of this trial is that, especially in patients with pCR, the coexpression of PD-1 increases on peripheral blood CD8+ cytotoxic T cells. This is probably not a sign of cell exhaustion, but indicates the expansion of cell subpopulations with high capacity for tumor recognition.43
In conclusion, single cycle of induction treatment with cisplatin/docetaxel and durvalumab/tremelimumab is feasible. This treatment achieves a high rate of biopsy-proven pCR of 48%. The pre-therapeutic intratumoral CD8+ cell density is the most valuable predictive factor for pCR. These results encourage the clinical development of induction treatments with combined chemoimmunotherapy in HNSCC.
References
Footnotes
Twitter @Markuseckstein3
Contributors MH: study design, clinical data collection, data interpretation and preparation of manuscript. AOG: clinical data collection and manuscript revision. ME: pathological analyses, data interpretation, preparation of manuscript. SR: study design and manuscript revision. JvdG: clinical data collection and manuscript revision. TI: clinical data collection and manuscript revision. MGH: clinical data collection and manuscript revision. GK: clinical data collection and manuscript revision. S: clinical data collection and manuscript revision. TB: clinical data collection and manuscript revision. A Hinke: statistical analyses and manuscript revision. IB: biological data collection and manuscript revision. BF: biological data collection and manuscript revision. SS: clinical data collection and manuscript revision. CIG pathological analyses and manuscript revision. A Hartmann: pathological analyses and manuscript revision. PB: study design, data interpretation and manuscript revision. WB study design, data interpretation and manuscript revision. USG: study design, data interpretation and preparation of manuscript. HI: clinical data collection, data interpretation and manuscript revision. RF: study design, data interpretation and manuscript revision.
Funding This work was supported and funded by AstraZeneca (ESR-16-12356). The trial was conducted as investigator sponsored trial.
Disclaimer The funding source did not influence design, data collection, analysis or interpretation. The manuscript was reviewed by the funding company. The corresponding author had full access to all the data and the responsibility for the decision to submit for publication.
Competing interests MH conflict of interest with Merck Serono (advisory role, speakers’ bureau, honoraria, travel expenses, research funding); MSD (advisory role, speakers’ bureau, travel expenses, research funding); AstraZeneca (research funding); Novartis (research funding); BMS (advisory role, honoraria, speakers’ bureau); Teva (travel expenses). ME conflict of interest with Diaceutics (employment, honoraria, advisory role, speakers’ bureau, travel expenses); AstraZeneca (honoraria, advisory role, speakers’ bureau, travel expenses); Roche (honoraria, travel expenses); MSD (honoraria, speakers’ bureau); GenomicHealth (honoraria, advisory role, speakers bureau, travel expenses); Astellas (honoraria, speakers’ bureau); Janssen-Cilag (honoraria, advisory role, research funding, travel expenses); Stratifyer (research funding, patents). SR conflict of interest with AstraZeneca (research funding); MSD (research funding). MGH conflict of interest with Roche (stock); Varian (stock); Sanofi (stock); AstraZeneca (honoraria); BMS (honoraria, advisory role); MSD (honoraria, advisory role); Merck Serono (honoraria); Celgene (honoraria). GK conflict of interest with BMS (advisory role); Lilly (advisory role); Roche (advisory role). SL conflict of interest with AstraZeneca (honoraria, advisory role); BMS (honoraria, advisory role, speakers’ bureau); MSD (honoraria, advisory role); Merck Serono (honoraria, speakers’ bureau); ISA-Pharmaceuticals (research funding). A Hinke conflict of interest with Roche (honoraria). SS conflict of interest with Strycker (stock); Varian (stock); Abbot (stock); Crispr Techn. (stock); Pfizer (stock); Merck Serono (stock); Symrise (stock); Ortho (honoraria, advisory role, speakers’ bureau, research funding, travel expenses); PharmaMar (speakers’ bureau, travel expenses); Haema (speakers’ bureau). A Hartmann conflict of interest with BMS (honoraria, advisory role); MSD (honoraria, advisory role); Roche (honoraria, advisory role, research funding); AstraZeneca (honoraria, advisory role, research funding); Boehringer Ingelheim (honoraria); Abbvie (honoraria); Cepheid (advisory role, research funding); Quiagen (advisory role); Janssen-Cilag (honoraria, advisory role, research funding); Ipsen (honoraria, advisory role); NanoString Technologies (advisory role, research funding, expert testimony); Illumina (advisory role); 3DHistech (advisory role); Diaceutics (advisory role); BioNTech (research funding). WB conflict of interest with BMS (advisory role); MSD (advisory role); Merck Serono (advisory role); Pfitzer (advisory role); AstraZeneca (advisory role). USG conflict of interest with AstraZeneca (advisory role, research funding); BMS (advisory role); MSD (research funding); Sennewald Medizintechnik (travel expenses). RF conflict of interest with MSD (honoraria, advisory role, research funding, travel expenses); Fresenius (honoraria); BrainLab (honoraria); AstraZeneca (honoraria, advisory role, research funding, travel expenses); Merck Serono (advisory role, research funding, travel expenses); Novocure (advisory role, speakers’ bureau, research funding); Sennewald (speakers’ bureau, travel expenses).
Patient consent for publication Not required.
Ethics approval The leading institutional review board at the Friedrich-Alexander-Universität Erlangen-Nürnberg (number: 131_18 Az) and all local ethic committees approved the trial.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Trial data will be posted on clinicaltrials.gov as required. Access to participant-level data for this study and supporting documents such as the protocol and informed consent will be made available on reasonable request. Please contact the corresponding author (markus.hecht@uk-erlangen.de).