Article Text

Abstract
Background Colitis is one of the common immune-related adverse events that leads to morbidity and treatment discontinuation of immunotherapy. The clinical presentation, endoscopic and histopathological features and best management of this toxicity are not well defined.
Patients and methods Patients with metastatic melanoma who received immunotherapy (programmed cell death protein 1 (PD1) antibodies, alone or in combination with a cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) antibody (PD1 +CTLA-4)) and who developed clinically significant colitis (requiring systemic corticosteroids) were identified retrospectively from two academic centers. Clinical data were collected for all patients; endoscopic and histopathological data were examined in a subset.
Results From May 2013 to May 2019, 118/1507 (7.8%) patients developed significant colitis; 80/553 (14.5%) after PD1+CTLA-4, 35/1000 (3.5%) PD1 alone, and three patients after Ipilimumab (IPI) alone. Combination therapy-induced colitis was more frequent (14.5% vs 3.5% in PD1 alone, p=<0.0001), had an earlier onset (6.3 weeks vs 25.7 weeks, p=<0.001), was more severe (grade 3/4 69% vs 31%, p=<0.001), and are more likely to require higher doses of steroids (91% vs 74%, p=0.01) than PD1 colitis. Among all patients treated with steroids (N=114), 54 (47%) responded and required no further therapy (steroid sensitive), 47 patients (41%) responded to infliximab (infliximab sensitive), and 13 (11%) were infliximab refractory and needed further immunosuppressive drugs. Infliximab-refractory patients all had onset within 4 weeks of immunotherapy commencement and were more likely to have an underlying autoimmune disease, have higher grade colitis, and require longer immunosuppression, yet had similar response and survival than other patients with colitis. Of 43 (37%) patients re-resumed treatment with PD1 monotherapy after colitis resolution, 16 (37%) of whom developed recurrent colitis. Endoscopic and histopathologic data were available for 64 patients. Most had left-sided colitis, with an increase in chronic inflammatory cells and neutrophils within the lamina propria, an increase in neutrophils in the surface epithelium, without increased lymphocytes or increased eosinophils. Infliximab-refractory colitis had a trend towards more confluent pancolitis with edema, erythema, ulceration, and absent vascularity with neutrophilic infiltration and erosion.
Conclusion Clinically significant colitis varies in presentation, response to immunosuppression, and endoscopic/histologic features depending on the immunotherapy type. Infliximab-refractory colitis occurs early, is often high grade, and has adverse endoscopic and histopathologic features
- immunotherapy
- programmed cell death 1 receptor
- CTLA-4 antigen
- inflammation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Immunotherapy has revolutionized cancer treatment in recent years. Antibodies against the immune checkpoints cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), programmed cell death protein 1 (PD1) and its ligand are now important treatments across oncology. Perhaps nowhere has immunotherapy had a greater impact than in melanoma, where the 5-year overall survival (OS) for metastatic patients has improved from less than 10% to over 50% with combination immunotherapy1 2 and adjuvant anti-PD1 therapy has halved the risk of disease recurrence.3 4
Immunotherapy is thought to primarily act by augmenting adaptive T cell responses through inhibition of checkpoints that control T cell activation and proliferation.5 This results not only in antitumor immunity but also often leads to immune-related adverse events (irAEs) as a result of aberrant T cell activation and inflammation in normal host tissue. While almost any organ of the body can be affected, colitis is a frequent and problematic irAE that can result in morbidity, death and may limit future treatment options.6 7 While empiric guidelines suggest that corticosteroids should be used and are effective in most cases, some patients require further management with biologics (infliximab, vedolizumab), non-selective immunosuppressants (cyclosporin, mycophenolate, mammalian target of rapamycin (mTOR) inhibitors) or surgery.8 9 To date, few studies have described the clinical, endoscopic, and histologic features of colitis, in particular, the frequency and clinicopathological correlates of steroid-refractory and infliximab-refractory colitis.10–16
In this study, we retrospectively explored the clinical, endoscopic and histopathological characteristics and management outcomes of immunotherapy colitis to identify factors that may direct optimal management and offer insight into the pathogenesis of this important and frequent toxicity. In particular, we examined for features that may be associated with steroid or infliximab-refractory colitis.
Materials and methods
Patients, treatment, and colitis characteristics
This study was approved by the institutional human research ethics committee and written informed consent was obtained from each patient. All patients with melanoma treated with anti-PD1 (nivolumab, pembrolizumab), anti-CTLA-4 (ipilimumab) monotherapy, or the combination at Melanoma Institute Australia (MIA) and Westmead Hospital between May 2013 and May 2019 were identified retrospectively using the MIA medical records database. Patients received ipilimumab, pembrolizumab and nivolumab monotherapy as per standard approved weight-based or flat doses and schedules. Combination therapy was given as standard dosing and schedule ipilimumab (3 mg/kg) and nivolumab (1 mg/kg) or ipilimumab (1 mg/kg) and nivolumab (3 mg/kg)/pembrolizumab (2 mg/kg or flat dose 200 mg) every 3 weeks, the latter ‘low-dose ipilimumab’ was administered as part of clinical trials.17–20 One patient received ipilimumab 100 mg every 12 weeks with pembrolizumab 200 mg 3 weekly as per protocol under a clinical trial.21 Patients who received either anti-PD1 monotherapy (PD1) or combination therapy (IPI+PD1) blinded on a clinical trial were excluded (n=3). Patients who had sequential treatment with ipilimumab directly followed (within 2 weeks) by anti-PD1 were incorporated into the combination therapy group for all analyses. Patients treated with anti-PD1 and other agents (Talimogene Laherparevec (TVEC), Toll-like receptor 9 (TLR9) agonist, Stimulator of interfron genes (STING) agonist, etc) on clinical trials were included in the PD1 monotherapy group.
Patients who developed clinically significant diarrhea/colitis requiring systemic immunosuppressive therapy following initiation of immunotherapy (herein termed colitis) underwent detailed assessment. Baseline characteristics included age, sex, and history of prior autoimmune disease. Melanoma history included BRAF/NRAS (rapidly acclerated fibrosacroma kinase, Neuroblastoma RAS viral oncologene homolog) mutation status, eighth edition American Joint Committee of Cancer (AJCC),22 Eastern Cooperative Oncology Group (ECOG) performance status, lactate dehydrogenase level, prior systemic therapy, and immunotherapy treatment type (PD1, CTLA-4, or combination IPI+PD1). Colitis characteristics included time to onset, CTCAE V.5.0 grade, the timing of diagnostic tests, management (timing of steroid, dose, and duration of steroid, infliximab, and other immunosuppressive drugs) and colitis outcome (resolution and recurrence in those who received further immunotherapy treatment). Endoscopy reports were examined and information was collected on bowel preparation, colitis distribution, and the presence and severity of inflammation. Tissue sections from colonic biopsies were examined by a pathologist (RVR) blinded to the clinical data.
Statistical analysis
The distribution of continuous variables was summarized as mean/median and range and categorical variables as frequencies and percentages. The associations between categorical variables and treatment type were tested using either the Fisher exact test or the χ2 test as appropriate. Clinical outcomes analyzed were objective response determined as per RECIST V.1.1, OS calculated from the time treatment initiation to death or censored at last follow-up, progression-free survival (PFS) calculated from the time of initiation of treatment to clinical/radiological progression (unresectable stage IIIC and stage IV melanoma), and recurrence-free survival (RFS) defined as the time of treatment initiation to recurrence (resected stage III melanoma). All survival outcomes were stratified by treatment and described using the Kaplan-Meier method. Survival differences between treatments were tested using the log-rank test. A p value of <0.05 was considered statistically significant. The analysis was performed on SAS V.9 and GraphPad Prism V.8.
Results
Incidence of colitis
Between May 2013 and May 2019, 1507 patients received immunotherapy for melanoma; among them, 1000 received PD1 monotherapy, 553 IPI+PD1 combination immunotherapy, either as an initial treatment or sequentially (92 patients received both treatments) and 46 patients received ipilimumab monotherapy. A total of 118/1507 (7.8%) patients developed colitis; 80/553 (14.5%) with combination therapy, which was higher than those with anti-PD1 (35/1000, 3.5%) or ipilimumab monotherapy (3/46, 6.5%; p=<0.0001, (online supplemental table 1). The median follow-up of colitis patients from the commencement of immunotherapy was 19.41 months (range 0.66–85.66). The patients who developed colitis were younger than those without colitis (median age 62 vs 66, p=0.02). Sex did not influence colitis risk (p=0.62).
Supplemental material
Characteristics of patients with colitis
Patients who developed colitis from either PD1 monotherapy or combination IPI+PD1 had a median age of 62, most were men (66%), with good performance status (ECOG 0 80%), and with no prior history of autoimmune disease (89%) (online supplemental table 2). The most frequent additional irAEs in those who developed colitis included rash (44%), vitiligo (20%), thyroid irAEs (20%), and hepatitis (20%).
Patients with colitis from combination therapy were younger than those with colitis from PD1 monotherapy (median 62 vs 66 years, p=0.02) and were more likely to have stage IV disease (89% vs 69%, p=0.01), likely reflecting treatment selection bias, and were more likely develop thyroid irAEs (27% vs 3%, p≤0.01). There were no differences in sex, performance status, prior history of autoimmune disease, or the development of other irAEs between the combination and monotherapy colitis cohorts.
Clinical features of colitis
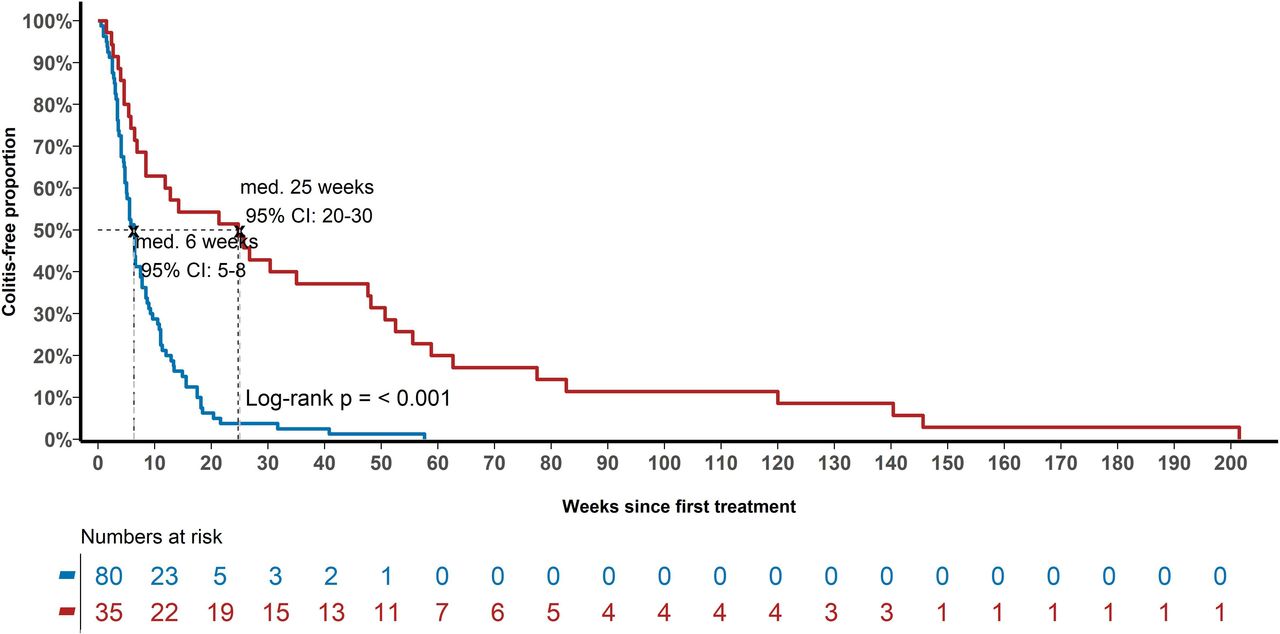
The median time to colitis was 6.7 weeks (range 0.5–201.5) (figure 1). Sixty-four (64/115, 56%) of patients had grade 3–4 colitis, the remaining 51 patients (44%) had grade 1–2 (table 1). Approximately half (n=64, 56%) of the patients underwent endoscopy with 35 (55%) undergoing flexible sigmoidoscopy and 29 (45%) having full colonoscopies. The median time to endoscopy from the onset of symptoms was 10 days (range 0–91 days), by which time 38 (59%) patients had received oral steroids, 20 (31%) had also received intravenous steroids, 2 (3%) had infliximab, while 4 (6%) had not received any treatment. On endoscopic examination, 33/64 (52%) had left-sided colon involvement, right-sided involvement alone was uncommon (3/64, 5%). Fifteen (24%) patients had pancolitis while 13 (21%) had no visual evidence of colitis on endoscopy. There was a spectrum in the degree and pattern of inflammation, vascularity, congestion, erythema, ulceration, and mucopurulent exudate (table 1 and online supplemental table 3). Histopathologically, most patients had an increased chronic inflammatory infiltrate within the lamina propria (85%), which was diffuse (59%), and with increased neutrophils in lamina propria (74%) and surface epithelium (70%), without increased intraepithelial lymphocytes or an increase in eosinophils in the lamina propria or surface epithelium. There were no chronic architectural changes in the majority of cases (61%) and most cases showed no apoptotic cells within the surface epithelium (69%).
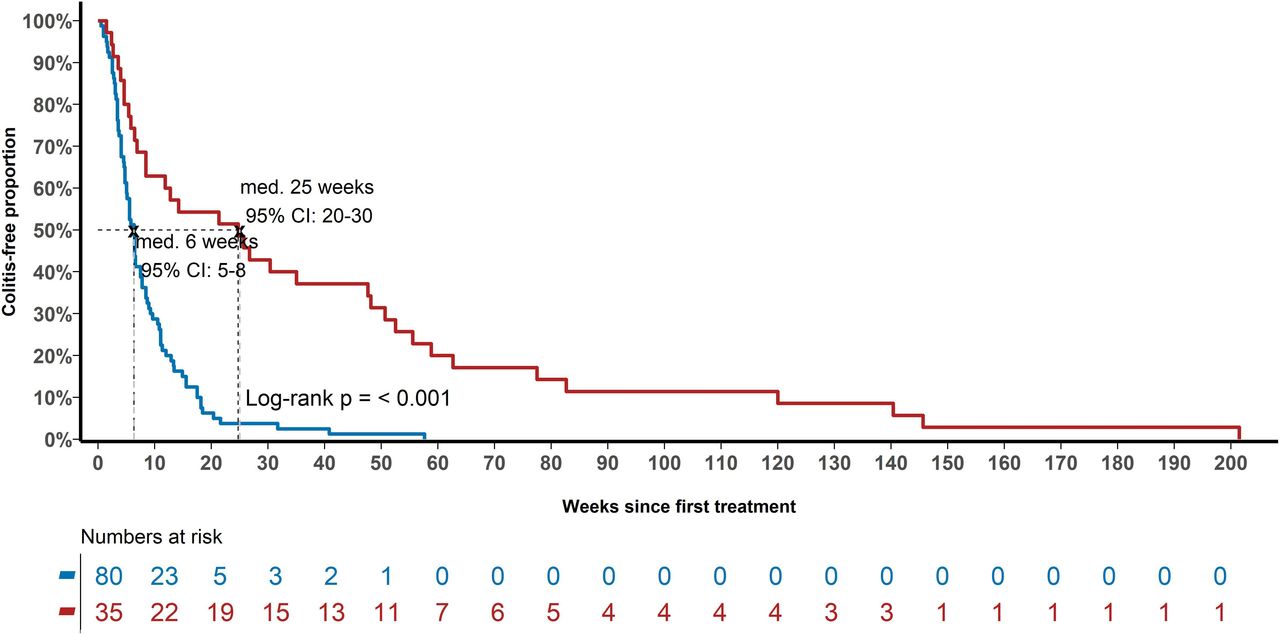
Time from the commencement of immunotherapy to the onset of symptoms of colitis in weeks with median and confidence intervals. Time to colitis by immunotherapy regimen (IPI +PD1 in blue vs PD1 in red; p=<0.001). PD1,programmed cell death protein 1; IPI, ipilimumab.
Features of colitis
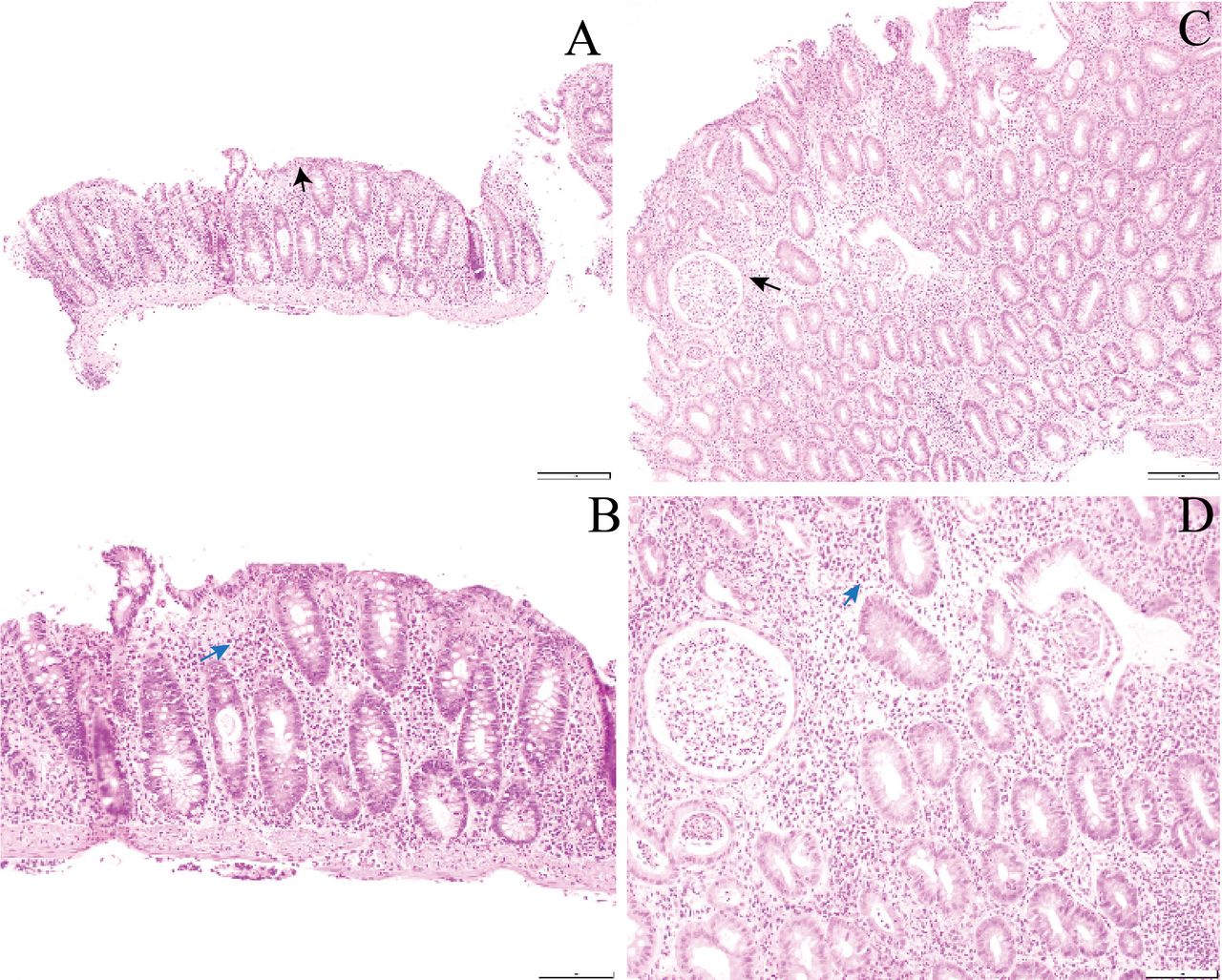
Patients with combination therapy colitis had a shorter time to colitis (median 6.3 vs 25.7 weeks, p<0.0001) and a higher grade of colitis (grade 3/4 66% vs 31%, p<0.001) than those with PD1 monotherapy colitis (figure 1, table 1). Combination therapy colitis occurred early, the median onset was 6.3 weeks after the commencement of therapy, whereas PD1 monotherapy colitis occurred as late as 202 weeks. The number of immunotherapy doses to the development of colitis was significantly less in IPI+PD1 group (median one cycle, range 1–6 cycles) compared with PD1 colitis group (median eight cycles, range 1–46 cycles, p≤0.0001). Similar proportions of patients underwent endoscopy in both cohorts. The type of endoscopic procedure, area of colon affected, degree, and pattern of inflammation or other endoscopic features did not differ between combination and monotherapy colitis. Histopathologically, combination therapy colitis had a greater degree of neutrophilic crypt infiltrate, but a lower degree of intraepithelial lymphocytosis than monotherapy colitis, and a higher likelihood of erosion (all p<0.05) (figure 2A–D). Other pathologic features were similar across both groups.
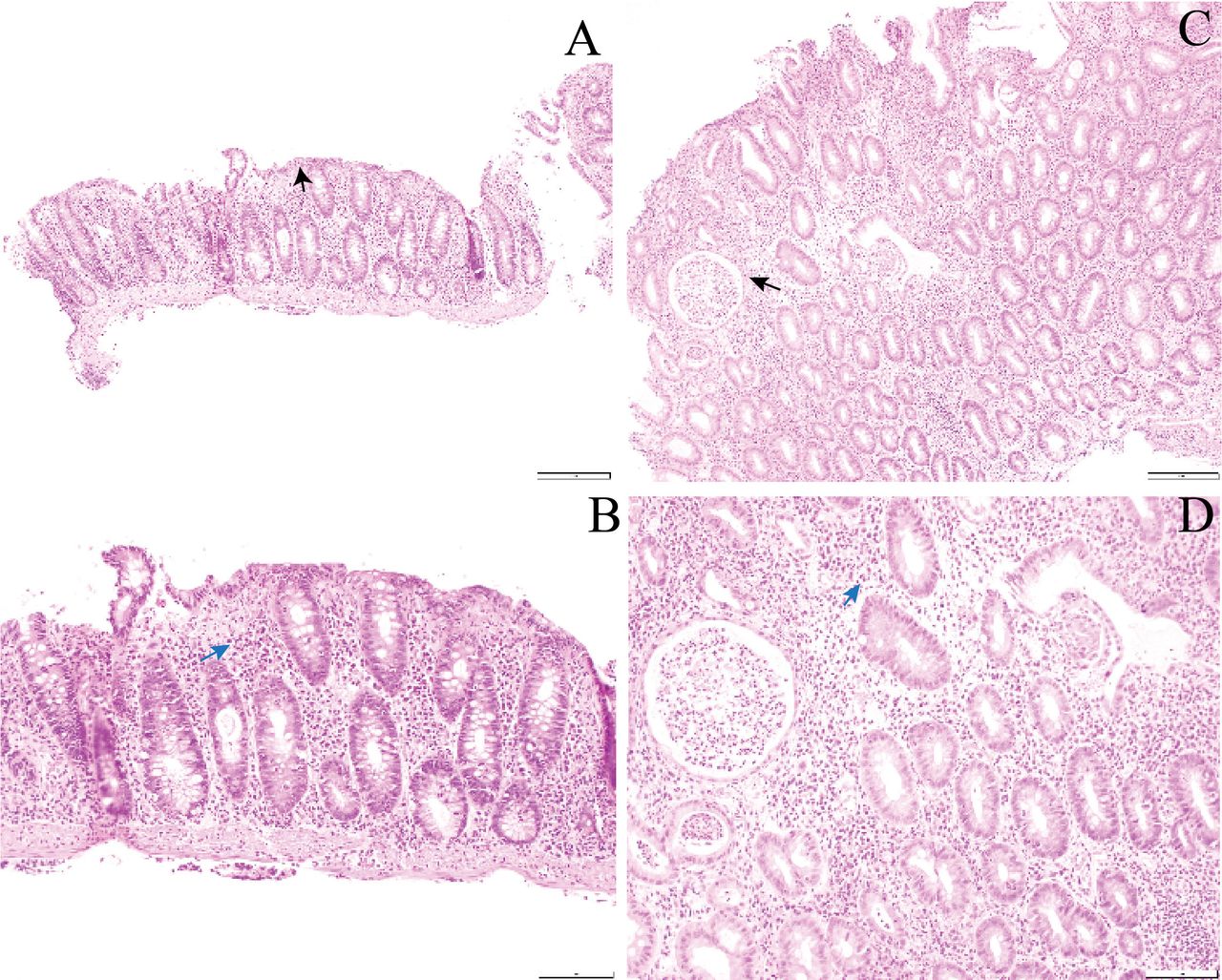
Representative H&E stained sections demonstrating increased different cellular infiltrates in colitis patients treated with monotherapy and combined immunotherapy (IPI+PD1). Representative H&E sections demonstrating increased different cellular infiltrates in colitis patients treated with monotherapy and combined immunotherapy. (A and B) Histopathology image of colonic biopsy of patient treated with anti-PD1 showing a diffuse chronic inflammatory infiltrate within the lamina propria (blue arrow) and an increase in lymphocytes with the surface epithelium (black arrow). A. H&E ×10; B. H&E ×20. (C and D) Histopathology image of colonic biopsy of patient treated with anti-PD1 and anti-CTLA-4 showing a diffuse infiltration of neutrophils within the lamina propria with numerous neutrophilic crypt abscesses (black arrow) and foci of cryptitis (blue arrow). C. H&E ×10; D. H&E ×20. CTLA-4, cytotoxicT-lymphocyte-associated protein 4; PD1, programmed cell death protein 1, IPI,ipilimumab
Management of colitis
All patients with colitis except one (n=114) received initial treatment with corticosteroids; 78 (69%) patients commenced with an oral corticosteroid (median starting dose 75 mg/day) and 36 (31%) with intravenous corticosteroids (methylprednisolone, median dose 1000 mg/day ×3). Fifteen of 79 (19%) patients who started with oral steroids subsequently received intravenous steroids (table 2). Fifty-five patients (48%) had a sustained response to corticosteroids and were deemed steroid-sensitive. The median duration of steroids was 10.9 weeks (range 1.7–66.1 weeks). Infliximab was used in 60 (52%) patients after a median of 13 days from colitis onset (range 2–62 days). Most patients (n=46, 77%) required one dose at 5 mg/kg, 14 (23%) had two or more doses (5–10 mg/kg), and most (n=47, 78%) had resolution of colitis and were deemed infliximab-sensitive. Thirteen (22%) patients failed to respond to infliximab, were deemed infliximab-refractory, and were managed with further immunosuppressive drugs. In the infliximab-refractory group, six patients (6/13,c46%) were treated with mycophenolate mofetil (median duration 21.3 weeks, range 7.1–34.1 weeks), two patients (2/13, 15%) received mesalazine (median duration 3.4 weeks, range 2.8–4.0 weeks) and one patient (1/13, 8%) received azathioprine (duration 5.0 weeks), all of whom had colitis resolution without later recurrence. Four patients (4/13, 31%) received cyclosporin (median duration 11.5 weeks, range 6.3–12.1 weeks), three of them (75%) had resolution of colitis. One patient (25%) had recurrence of colitis shortly after cessation of cyclosoprin so was reinstituted with resolution of symptoms. One hundred and ten patients (96%) with colitis ultimately resolved with medical therapy but 5 (4%) required colectomy, and no patient died from colitis. A total of 43 patients (37%) resumed PD1 monotherapy after colitis resolution either as maintenance therapy while in response or as rechallenge due to disease progression. With further immunotherapy, 16 patients (16/43, 37%) had a recurrence of colitis. Most of these responded to steroids (11/16, 69%) while 5/16 (31%) required infliximab.
Management of colitis
Patients with combination therapy colitis were more likely to require higher doses of oral steroid (>75 mg prednisolone, 91% vs 74%, p=0.01) and more intravenous steroids (54% vs 23%, p<0.01) than those with monotherapy colitis and be steroid refractory and receive infliximab (59% vs 37%, p=0.03). When used, infliximab was equally effective in both cohorts and usually only required a single dose. The duration of steroids was similar between the two cohorts (10.5 vs 11.3 weeks, p=0.99). Similar proportions of patients resumed immunotherapy following colitis resolution, with similar rates of colitis recurrence.
Features of steroid-sensitive, infliximab-sensitive, and infliximab-refractory colitis
In the total cohort of 115 patients with PD1 monotherapy or combination therapy colitis, 54 (47.4%) were steroid sensitive, 47 (41.2%) infliximab sensitive, and 13 (11.4%) infliximab refractory (one patient did not receive steroid treatment and was excluded from further analysis). The baseline characteristics and endoscopic and histologic features are shown in table 3 and online supplemental table 4. Neither age nor the type of immunotherapy used was associated with steroid or infliximab responsiveness. Thirteen (11%) patients had a history of autoimmune disease (psoriasis n=7, thyroiditis n=2, Grave’s disease n=1, inflammatory arthritis n=2, Eaton-Lambert syndrome n=1). Interestingly, infliximab-refractory patients were more likely to have an autoimmune disease (31%) than infliximab-sensitive (6%) or steroid-sensitive (11%) patients (p=0.05).
Features of steroid-sensitive, infliximab-sensitive and infliximab-refractory groups
Infliximab-refractory patients had higher grade colitis (G3/4 in 92%) compared with infliximab-sensitive (72%) or steroid-sensitive (33%) patients (p=<0.001). Five patients (4.2%) suffered grade 4 colitis and had a colectomy; three were infliximab refractory, one had surgery due to colonic perforation and one due to severe colitis (without steroid). The time to colitis onset was not different based on the management subgroup, however, all patients who had infliximab-refractory colitis had onset within 3.2 weeks. Patients with infliximab-refractory colitis had a similar maximum daily dose of oral steroids (≥75 mg, 100%) compared with infliximab-sensitive colitis (≥75 mg, 96%) and higher than those with steroid-sensitive colitis (≤50 mg, 72%, p=<.001), while there was a trend towards a longer median duration of steroid use in those with infliximab-refractory colitis of 15.4 weeks versus 11.6 weeks versus 9.2 weeks, respectively (p=0.71). The PD1 monotherapy resumption rate was lower in the infliximab-refractory cohort (2/13, 15%) than the infliximab-sensitive (22/47, 47%) and steroid-sensitive cohorts (19/54, 35%, p=0.08). Most of those who resumed PD1 monotherapy and had recurrent colitis were in the infliximab-sensitive cohort (12/16, 75%), while few steroid-sensitive (3/16, 19%) and infliximab-refractory (1/16, 6%) patients had recurrent colitis (p=0.01).
The type (colonoscopy vs sigmoidoscopy) and time to endoscopy from the onset of clinical symptoms were not different between the colitis management groups (data not shown). At the time of endoscopy, more patients with infliximab-refractory colitis had received infliximab (2/9, 22%) and intravenous steroids (4/9, 44%) than those with infliximab-sensitive and steroid-sensitive patients (p=0.006). There were neither significant differences in endoscopic examination between the groups, including the degree, pattern and area of inflammation, nor vascularity, congestion (edema), erythema or ulceration. Infliximab-refractory patients, however, had a trend to a higher degree of confluent pancolitis with edema, erythema, ulcers, and absent vascularity. Histologically, patients with infliximab-refractory colitis had more marked neutrophilic infiltrate in the lamina propria (p=0.03) and neutrophilic crypt abscesses (p=0.02) with erosion (p=0.001), whereas steroid-sensitive colitis tended to have little to no increase in neutrophils. In general, there was a trend to a more diffuse chronic inflammatory infiltrate from steroid-sensitive to infliximab-sensitive and infliximab-refractory colitis.
Melanoma response and survival
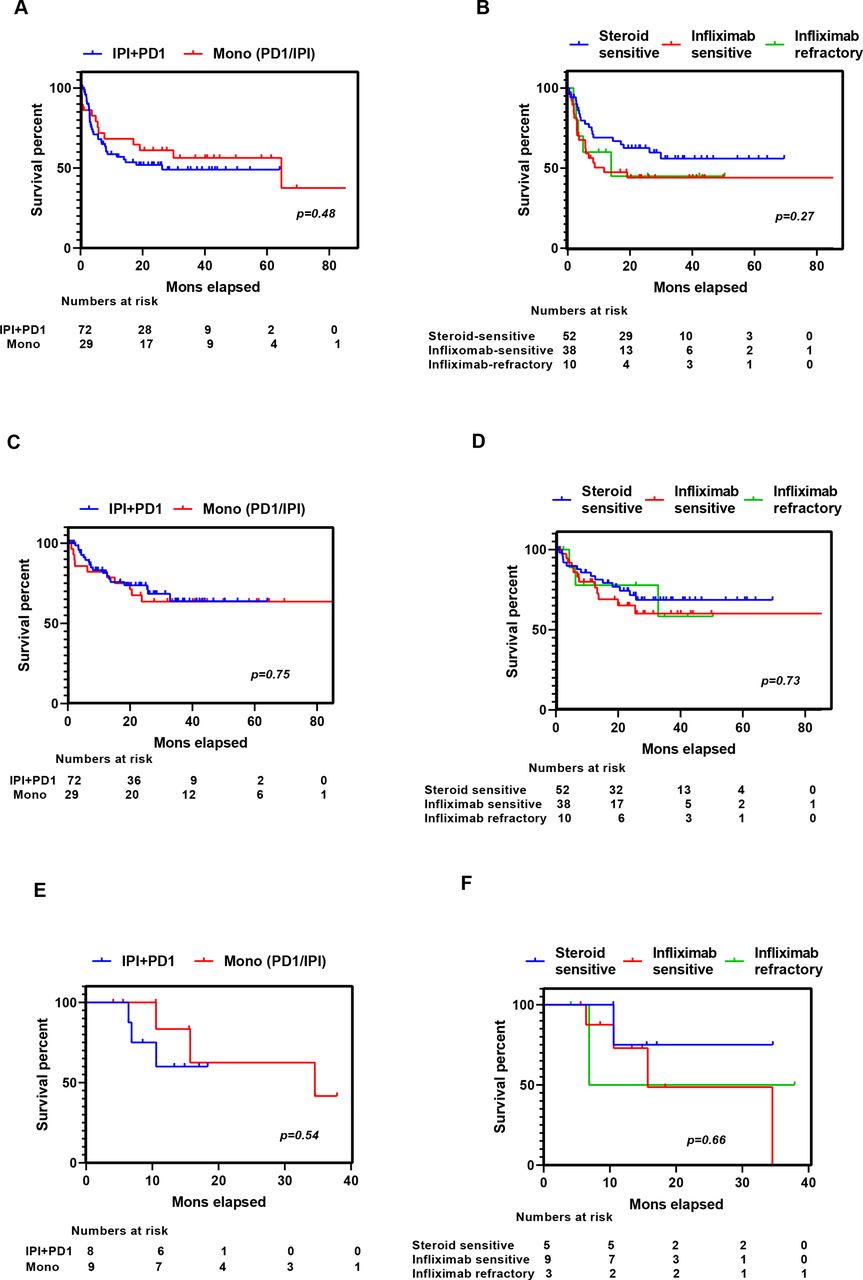
The overall objective response rate (ORR) in those with advanced melanoma (unresectable IIIC/IV melanoma) with colitis was 54%; similar between PD1 monotherapy and combination therapy cohorts (online supplemental table 2). The ORR among the steroid-sensitive, infliximab-sensitive, and infliximab-refractory groups was similar at 60% (31/52), 47% (18/38), and 50% (5/10), respectively (p=0.49, data not shown). After a median 19.24 months, follow-up for the cohort, the 1-year and 2- year landmark PFS in those with advanced melanoma were 60% and 54%, respectively, and PFS was similar in those with combination and monotherapy colitis (figure 3A). The median OS for the advanced melanoma cohort was not reached; 1-year and 2-year OS were 82% and 70%, respectively, again similar in those with combination and monotherapy colitis (figure 3C). The RFS for patients who received adjuvant treatment (resected stage III) at 1 and 2 years was 71% and 59%, respectively, with similar results in combination and monotherapy cohorts (figure 3E). Similarly, PFS, OS (for advanced melanoma patients), and RFS (for resected stage III patients) were similar in the three colitis management groups (figure 3B,D,F).
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curve stratified by immunotherapy treatment type (IPI+PD1 vs monotherapy with PD1/ipilimumab) and colitis management type (steroid sensitive vs infliximab sensitive vs infliximab refractory) for PFS (A and B) and OS (C and D) (patients with advanced melanoma) and RFS (E and F) (patients receiving adjuvant treatment). (A) PFS by immunotherapy treatment in patients with advanced melanoma (unresectable IIIC/IV). (B) PFS by colitis management type in advanced melanoma patients (unresectable IIIC/IV). (C) OS by immunotherapy treatment type in patients with advanced melanoma (unresectable IIIC/IV). (D) OS by colitis management type in patients with advanced melanoma (unresectable IIIC/IV). (E) RFS by immunotherapy treatment type in patients receiving adjuvant treatment. (F) RFS by colitis management type in patients receiving adjuvant treatment. OS, overall survival; PD1, programmed cell death protein 1; PFS, progression-free survival; RFS, recurrence-free survival.
Discussion
This is an important study of patients with clinically significant colitis (defined at that requiring steroids) from both PD1 monotherapy and combination PD1 and CTLA antibodies, with detailed clinical, endoscopic, and histologic data linked to colitis management outcomes, in particular, for infliximab-refractory colitis. We show that only half of the patients with colitis respond to steroid therapy and only 80% of steroid-refractory patients respond to subsequent infliximab. Patients with infliximab-refractory colitis, approximately 10% of all colitis patients, develop colitis within 4 weeks of immunotherapy commencement and are more likely to have an underlying autoimmune disease and have higher grade colitis. They require higher and longer immunosuppression, yet have similar cancer survival as those with steroid-sensitive and infliximab-sensitive colitis. While most patients with colitis have left-sided colitis with an increased chronic inflammatory cell infiltrate within the lamina propria with increased neutrophils in the surface epithelium and lamina propria, infliximab-refractory colitis also tends to have more confluent pancolitis with edema, erythema, ulceration, and absent vascular pattern with similar neutrophilic infiltration and erosion than steroid-sensitive or infliximab-sensitive colitis. Interestingly, colitis does not tend to demonstrate predominantly lymphocyte or eosinophilic infiltrates, rather neutrophilic infiltrate, suggesting dysregulation of innate immunity.
The incidence of colitis in our cohort was 3.5% on PD1 monotherapy and 14.5% on combination therapy, which is in keeping with published literature.15 23 Although ‘colitis’ and ‘diarrhea’ are often coded and reported separately in clinical trials despite likely representing the same underlying phenomenon. In this study, we regarded any colitis or diarrhea that warranted systemic steroid treatment as ‘clinically significant colitis’ to reflect a more realistic clinical scenario. A previous study of 53 patients has also shown no clear association between grades of diarrhea and colitis,16 while a recent case series showed higher use of infliximab in patients with severe endoscopic findings (by Mayo Endoscopic Score) but dissociation between clinical symptoms and endoscopic severity scores, highlighting the importance of endoscopy when deciding further immunosuppression in steroid-refractory cases.24 Similar to these studies, we observed that infliximab-treated patients (steroid refractory) tend to have higher grade colitis (46/60, 77%) and ulceration on endoscopy (30%) though this did not reach statistical significance (p=0.07). Compared with previous case series that reported endoscopic and histologic outcomes on immune-mediated colitis, our cohort had greater numbers of combination immunotherapy patients reflecting substantial clinical trial recruitment and a change in clinical practice over time.13 14 16 24
Approximately half of the patients with PD1 monotherapy or combination therapy colitis in our cohort received infliximab for steroid-refractory disease, which is in line with published case series.11 13 16 Infliximab is recommended in current guidelines for the steroid-refractory disease,9 and in our series, patients received this therapy due to ongoing symptoms despite adequate initial steroid therapy or relapse while tapering. The choice of immunosuppressive agents in steroid-refractory cases was decided by the gastroenterologist and medical oncology multidisciplinary teams. The addition of further immunosuppressive agents in infliximab-refractory cases was guided by persistence or recurrence of symptoms after initial response to infliximab and/or ongoing endoscopic evidence of inflammation. The most commonly used immunosuppressive drug was mycophenolate (46%) followed by ciclosporin, mesalazine, and azathioprine. All patients had clinical resolution of colitis with these non-selective immunosuppressives, however, alternative agents may be more appropriate. A recent multicentre case series (28 patients) described the utility of vedolizumab in immune-mediated colitis.25 The clinical remission rate in infliximab-refractory cases was 67% (6/9) with a median of three infusions, compared with 95% (18/19) in cases who were infliximab-naïve. Another single-center case series showed that early introduction of vedolizumab or infliximab resulted in less hospitalization, shorter steroid duration, and fewer steroid taper failure attempts.10 Also, a recent case report examined the utility of janus kinase inhibitor (JAK) tofacitinib for severe infliximab/vedolizumab refractory autoimmune colitis with sustained clinical remission.26 Regardless of the use of non-selective immunosuppressives in our study, OS was similar irrespective of colitis management strategy (steroids, infliximab, or other drugs) and similar to phase 3 clinical trial data, suggesting that immunosuppression in patients with significant immune activation (in the form of colitis) may not impact melanoma outcome.24 27 28
Thirteen patients (13/64, 21%) in our cohort had an endoscopically ‘normal’ colon despite clinical symptoms of colitis. Of note, in the infliximab-refractory group, 22% had no visible area of involvement of colon despite higher grade colitis (grade 3–4, 92%) similar to other case series.16 25 Further invasive investigations may be considered in this subgroup of patients to rule out other pathology such as enteritis. Therefore, caution should be taken when interpreting ‘normal’ endoscopic findings that reinforce the importance of clinical severity of symptoms at presentation for evaluation and optimization of therapy. Histopathological characterization of immune-mediated colitis still largely based on features described in the inflammatory bowel disease (IBD) spectrum. Interestingly the majority of immune-mediated colitis cases showed no chronic architectural changes in the crypts, a key diagnostic feature of IBD. A few case series have described a pattern of acute and chronic inflammatory changes on histopathology with significant overlap induced by Immune checkpoint inhibitors (ICIs) similar to microscopic colitis.12–14 29 The pattern of acute, chronic lymphocytic, or chronic inflammation has a significant overlap between patients and does not seem to correlate with the type of ICI used. The most common finding is an increased chronic inflammatory infiltrate (86% of cases). We noted significantly increased neutrophilic infiltration in lamina propria and neutrophilic crypt abscess in steroid-refractory cases that may be used as a marker of severity in conjunction with endoscopic and clinical findings for an earlier switch to infliximab treatment. An influx of acute inflammatory cells such as neutrophils is regarded as a key marker of disease activity in IBD.30 An ongoing area of major research is to investigate whether immune colitis represents/shares similar pathogenesis to IBD, wherein active inflammation is postulated to be due to loss of tolerance to gut microbiota due to the reduction of regulatory T cell activity.31 Translational research delineating the detailed make-up of inflammatory infiltrates in this setting is required.
About one-third (43/115, 37%) of our cohort resumed PD1 monotherapy after the initial resolution of colitis. A total of 16 (16/43, 37%) patients experienced a recurrence of colitis of any grade and this was managed as per current standard management guidelines. A similar result was observed in a recent multicenter case series that reported an overall recurrence rate of 34% in a mixed cohort of patients with cancer following the resumption of immunotherapy.32 Another case series reported a 6% recurrence rate of all grade colitis in patients with melanoma treated with combination immunotherapy after rechallenge with PD1 monotherapy, while the initial incidence of all grade colitis was 44%.33 Although the recurrence rate was higher among infliximab treated patients (9/16, 75%), most responded to the steroid, with only 30% requiring repeat infliximab. Our study also reports that patients who experienced immune toxicity can be rechallenged especially with PD1 monotherapy if required although infliximab-treated cases should be cautiously considered.
The results of this study, examining the characteristics and management of immunotherapy colitis, provide important clinical information as to the success of steroids, infliximab, and other agents for the management of colitis, the likelihood of recurrence in those who resume PD1 monotherapy. The data suggest that all forms of colitis share similar histopathological features and are characterized by a predominance of chronic inflammatory cells and neutrophils. Further research is required to understand the pathogenesis of immune-mediated colitis, to predict who is at risk of this toxicity and to enable effective acute management and prophylaxis.
Acknowledgments
GL and RAS are supported by NHRMC practitioner fellowships. GL is supported by the University of Sydney Medical Foundation and Melanoma Institute Australia. AM is supported by Cancer Institute NSW and Melanoma Institute Australia. Support from colleagues at Melanoma Institute Australia, Mater Hospital, Royal North Shore Hospital, Royal Prince Alfred Hospital & New South Wales Health Pathology is gratefully acknowledged.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Twitter @ProfRScolyerMIA
Contributors AM was the senior author of the study, developed the concept and designed the study. KJN collected the data, interpreted the results, and wrote the manuscript with AM. RVR reviewed the histopathology with input from RAS. KJN, TA and SL conducted data analysis. All authors read and approved the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests GL is a consultant advisor for Aduro, Amgen, Bristol-Myers Squibb, Mass-Array, Merck, MSD, Novartis, OncoSec Medical, Pierre Fabre, Roche, Q biotics and Sandoz. MC is a consultant advisor for BMS, MSD, Novartis, Roche, Pierre Fabre, Sanofi, Merck Serono, Eisai, Nektar, Ideaya and Q biotics. AM is a consultant advisor to BMS, MSD, Novartis, Roche and Pierre-Fabre.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Data are available on reasonable request from the corresponding author, alexander.menzies@sydney.edu.au.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.