Article Text

Abstract
Background Immune checkpoint inhibitors (ICIs) can cause unique, high-grade immune-related adverse events. Although rare, ICI related stroke events can have high morbidity and mortality. Neurological monitoring is not routinely performed in patients on ICI treatment, thus risk factors remain unknown. Characterisation of such rare, but fatal adverse events requires integration of real-world data.
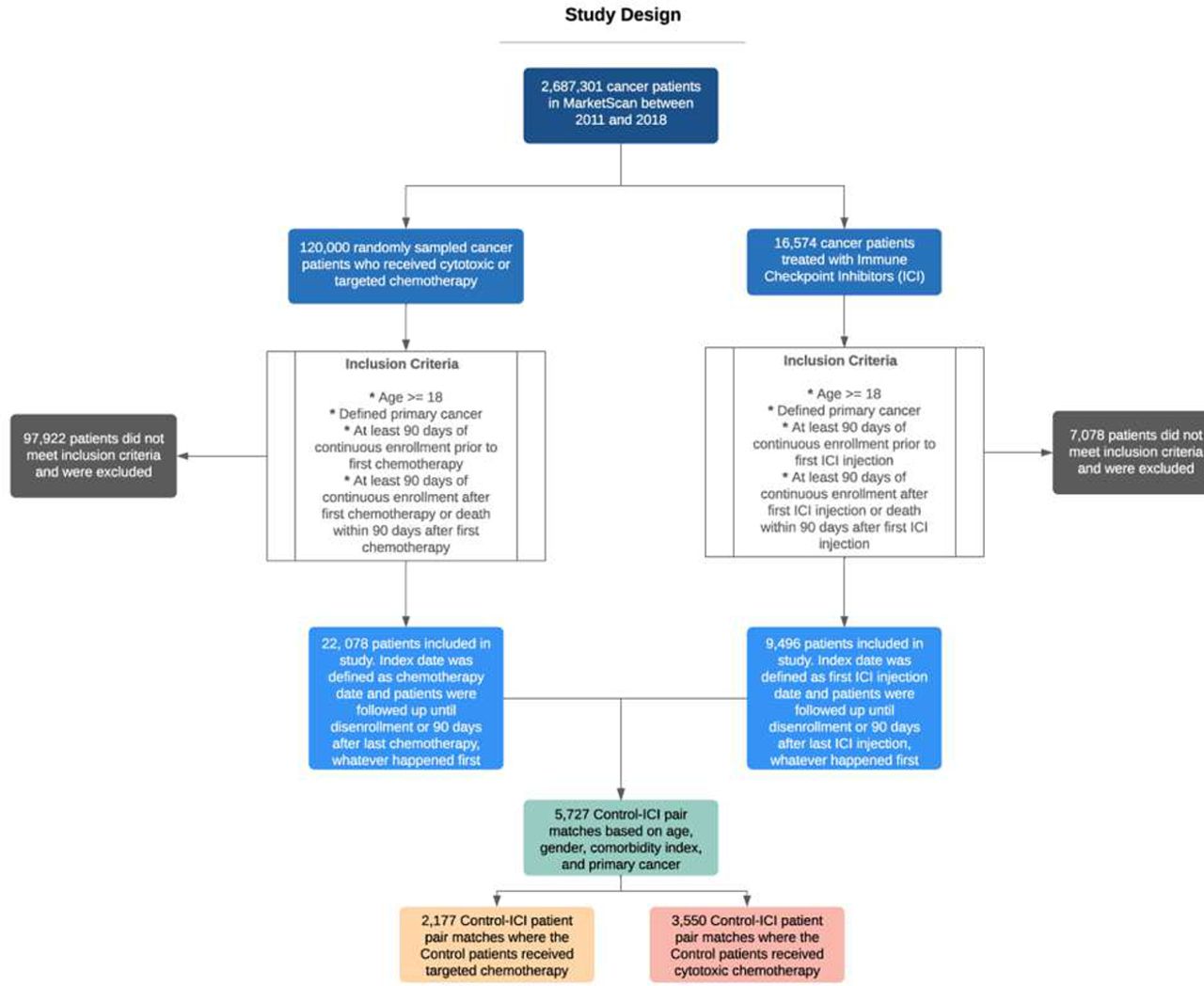
Methods U.S claims data (IBM MarketScan) of over 30 million commercially insured individuals was leveraged to identify 2,687,301 cancer patients between 2011–2018. Patients ≥18 years of age, treated with ICIs (targeting CTLA4 (ipilimumab) and/or the PD1 (nivolumab, pembrolizumab)/PDL1 (atezolizumab, avelumab, durvalumab) alone or in combination with ICI and/or chemotherapy were identified and followed until disenrollment. All strokes (ischemic or haemorrhagic), comorbidities, and treatment details were identified using diagnosis and billing codes. Patients from the ICI cohort were matched 1:1 to those in the chemotherapy cohort according to age, gender, NCI comorbidity score, and primary cancer as presented in the study design (figure 1). The matched cohorts were split by the specific type of chemotherapy (targeted or cytotoxic) used in the control patients. This yielded a total of 2,177 pairs of matched patients where the control arm received targeted chemotherapy, and 3,550 pairs of matched patients where the control arm received cytotoxic chemotherapy. Analyses included descriptive statistics and Cox proportional hazards regression.
Results A total of 16,574 patients received at least one dose of ICI therapy for any advanced cancer. Overall 9,496 patients who were treated with ICI met the study eligibility criteria. Stroke was identified in 489 (5.14%) patients. Mean age (±standard deviation, SD) was 60 (±12), male 62%, mean (±SD) NCI comorbidity index 2.3 (±2.12), median time to stroke was 168 days. 51.3% patients received anti-PD1 monotherapy, 37.6% received anti-CTLA4, 3.3.% anti-PD-L1 and 7.8% received combination therapy (anti-PD1 plus anti-CTLA4). One-year cumulative incidence (CI) in the matched ICI vs. targeted and ICI vs. cytotoxic chemotherapy were 6.3% vs. 5.7% (p=0.07) and 4.95% vs. 4.08% (p=0.90) respectively (table 1). Within the ICI cohort, CI of stroke events with anti-CTLA4 monotherapy vs. anti-PD1/PD-L1 and anti-CTLA-4 plus anti-PD-1 combination vs. PD1/PD-L1 monotherapy were 9.89% vs. 4.54% and 6.69% vs. 3.73%, respectively (table 2). On multivariable regression analyses, patients with malignant melanoma, and those receiving anti-CTLA-4 monotherapy were associated with higher risk of stroke events, while the risk was lower in patients with head and neck cancer and those who received anti-PD-1 monotherapy (table 3 and 4).
{kind=link}
Study design
Cumulative Incidence of Stroke in ICI cohort vs. non-ICI cohort
Cumulative incidence of stroke across ICI type
Risk factors associated with stroke events (Univariate analysis)
Risk factors associated with stroke events (Multivariate analysis)
Conclusions To the best of our knowledge, this is the largest and comprehensive real-world longitudinal study for stroke events in advanced cancer patients treated with ICI. Cumulative incidence of stroke was significantly higher in patients on anti-CTLA-4 monotherapy and anti-CTLA-4 plus anti-PD-1 combination therapy in comparison to anti-PD-1/PD-L1 monotherapy. Malignant melanoma and anti CTLA-4 therapy were independent risk factors for stroke.
Acknowledgements This work was funded by pilot award in Big Data/Cancer Informatics to Prantesh Jain, MD from University Hospitals Research & Education Institute
Ethics Approval The IBM MarketScan national database contains de-identified linked inpatient, outpatient, and pharmacy claims data. University Hospitals’ Institutional Review Board determined this study to be exempt from review and requirement of an informed consent.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.