Article Text

Abstract
Background Immune checkpoint inhibitors (ICIs) often lead to immune-related adverse events (irAEs) with effects ranging from treatment interruption to mortality.1 2 Most irAEs are treated with corticosteroids despite mounting evidence to suggest that corticosteroid treatment may blunt antitumor efficacy.3–5 There is a paucity of data on biomarkers that predict irAEs or characterize inflammatory changes during irAEs or steroid use. We sought to identify changes in cytokines that correlate with irAEs and may suggest inflammatory mechanisms that enable rational therapies. We also aimed to study the impact of steroid treatment on cytokine levels to better understand their immunomodulatory effect.
Methods We analyzed longitudinal levels of 34 cytokines in 52 melanoma patients receiving ICIs who developed irAEs. Luminex assay was performed on serum at baseline, 1, 2, and 3 months after starting ICI. Baseline cytokine levels were compared with incidence and grade of irAEs. Cytokine fold-change was compared between patients who did not develop irAEs, patients who developed irAEs without receiving steroids, and patients who developed irAEs who received steroids during the longitudinal profiling period.
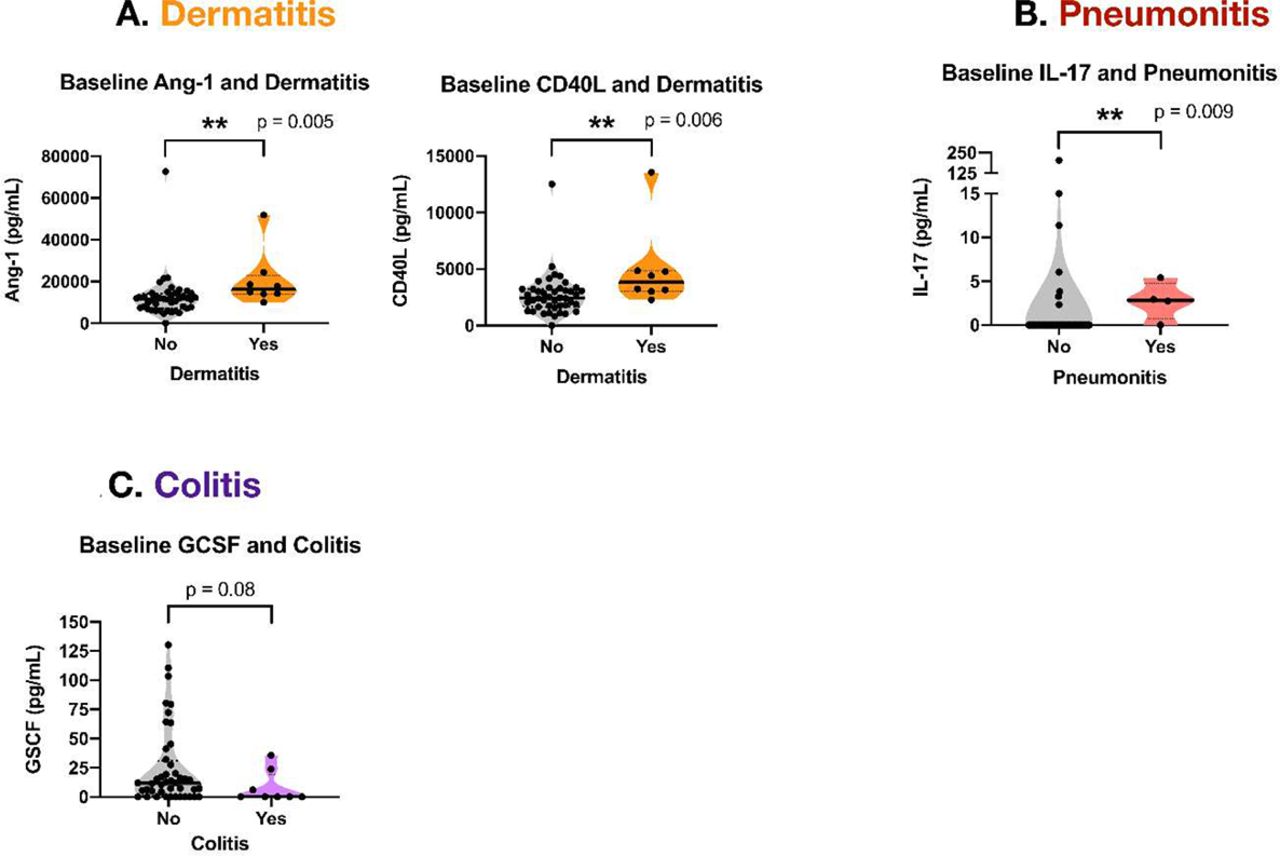
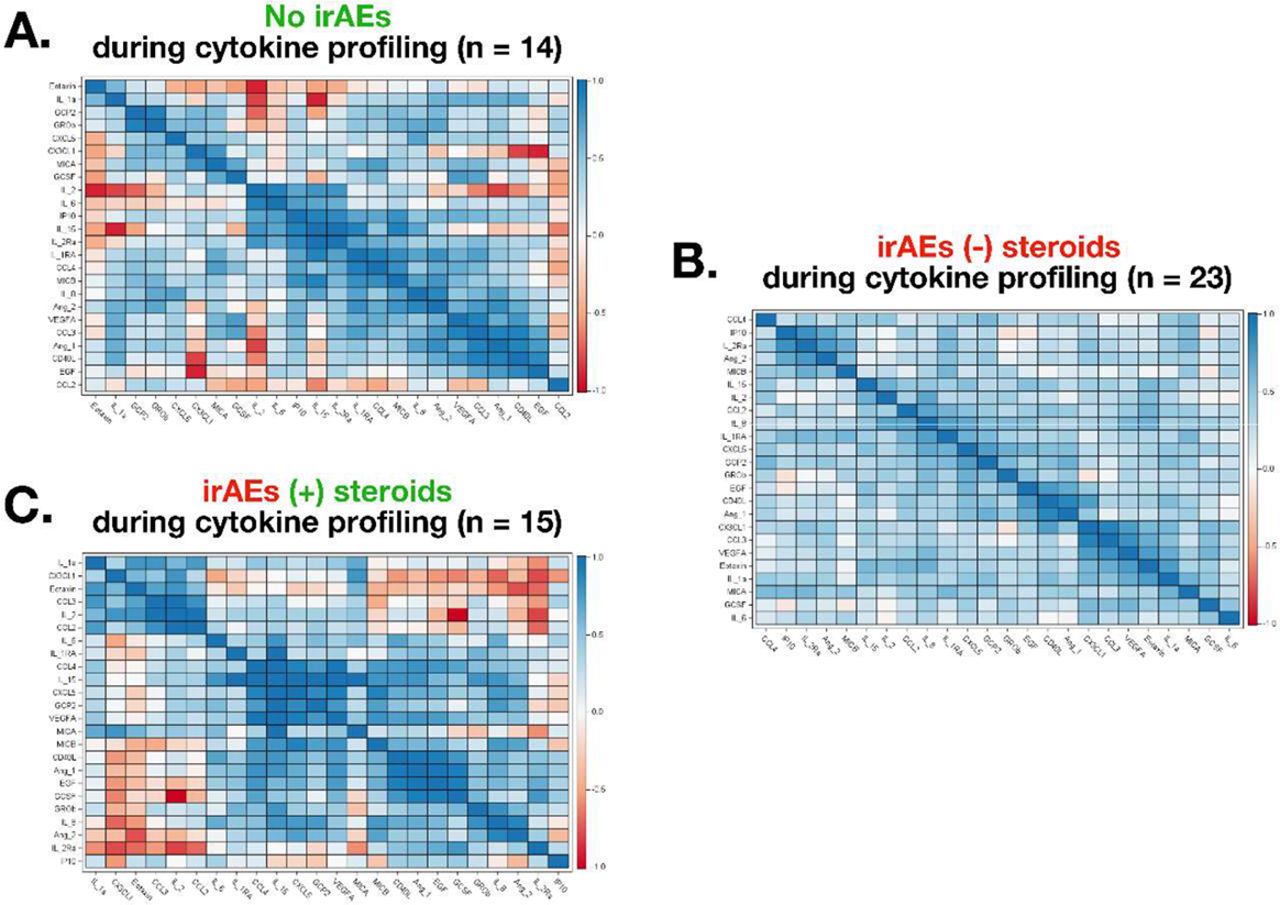
Results 33/52 (63.5%) patients were male and median age was 70.5 years. 47 patients (90.4%) received anti-PD1 monotherapy, 4 patients (7.7%) received anti-CTLA-4 monotherapy and one patient received combination therapy (1.9%). Twenty-eight patients (53.8%) developed grade 1–2 irAEs and 24 patients (46.2%) developed grade 3-4 irAEs. There were no differences in cytokine levels between patients with grade 1-2 vs. grade 3-4 irAEs. Patients with dermatitis (N = 8) had significantly higher baseline Ang-1 (p = 0.006) and CD40L (p = 0.005, figure 1A). Patients with pneumonitis (N = 4) had significantly higher baseline IL-17 (p = 0.009, figure 1B). There was a trend towards lower GCSF levels in patients developing colitis (N = 8, p = 0.08, figure 1C). We observed a harmonization of cytokine fold-change in patients who developed irAEs without receiving steroids: 269/276 (97.5%) of pairwise comparisons exhibited fold-change in the same upwards or downwards direction (figure 2). In contrast, corticosteroid treatment in patients with irAEs appeared to alter cytokine fold-change to a discordant pattern (214/276, 77.5%) mirroring patients who did not develop irAEs during the longitudinal profiling period (213/276, 77.2%). Example patient timelines are shown in figure 3.

Baseline cytokine level differences in patients with irAEs(A) Baseline levels of Ang-1 (median 16,375 vs. 11,604 pg/mL, p = 0.005) and CD40L (median 3,840.2 vs. 2433.8 pg/mL, p = 0.006) was higher in patients who developed dermatitis during ICI treatment. (B) Baseline levels of IL-17 was higher (median 2.8 vs. 0.0 pg/mL, p = 0.009) in patients who developed pneumonitis during ICI treatment. (C) There was a trend towards lower baseline levels of GSCF (median 0.0 vs. 11.9 pg/mL, p = 0.08) in patients who developed colitis during ICI treatment.P-values for baseline comparisons were obtained through Wilcoxon rank-sum test. The solid black line indicates median. Violins show range and kernel density estimate distributions of each group. (*) p < 0.05, (**) p < 0.01.
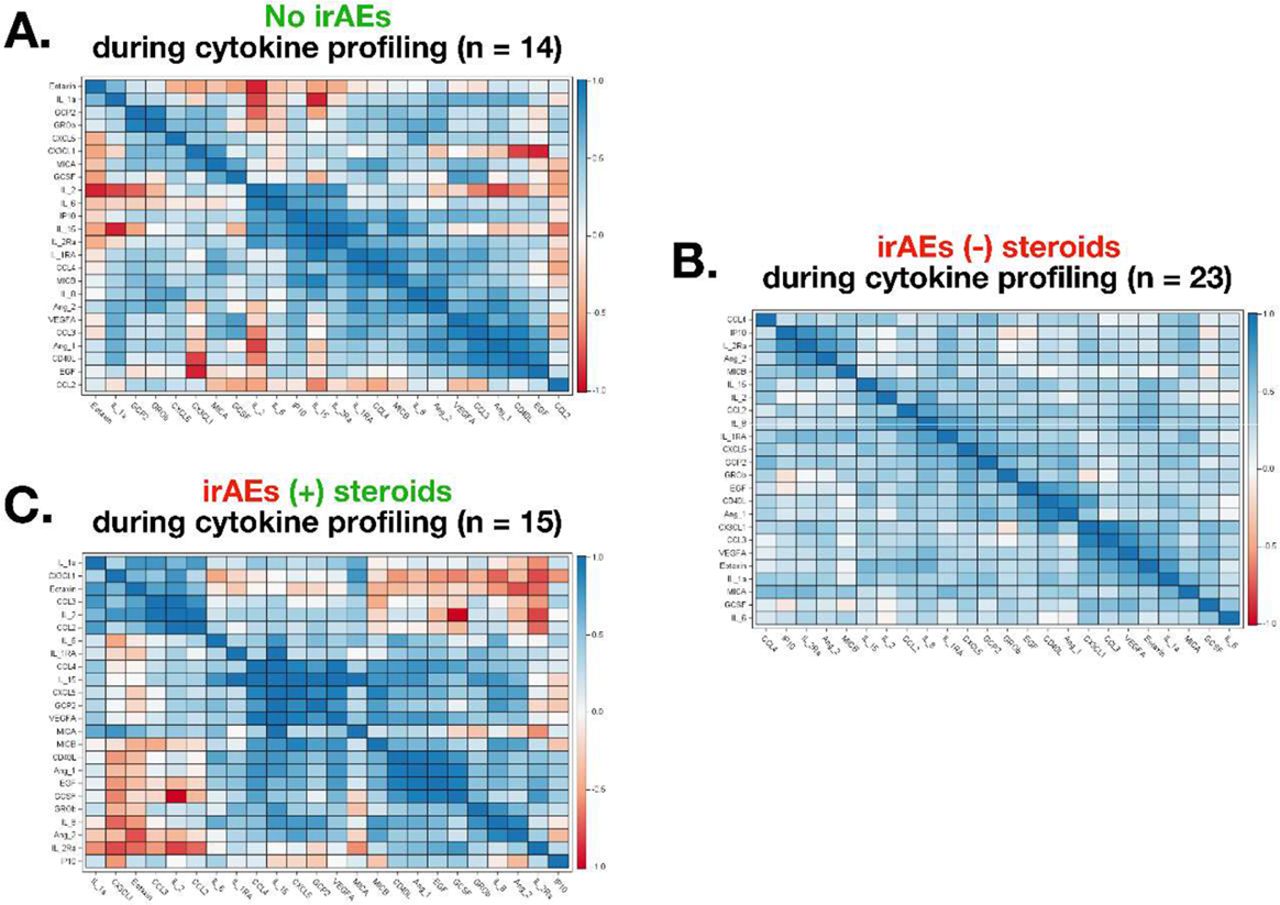
Spearman’s correlation analysis of cytokine changesSpearman’s correlation analysis of cytokine changes in patients who did not develop irAEs (A), developed irAEs without steroid treatment (B), and developed irAEs with steroid treatment (C) during the cytokine profiling period. Spearman’s correlation heatmap show changes in cytokine fold-change relative to each another. Blue indicates fold-change of two cytokines in the same direction, red indicates fold-change of two cytokines moving in opposite directions. Cytokine fold-change is based on changes in serum levels between baseline and the event of interest (irAE onset or irAE onset with steroid treatment).(A) Patients who did not develop irAEs during the cytokine profiling period had a discordant pattern of cytokine fold-change, with 213/276 (77.2%) pairwise comparisons changing in the same direction. (B) Patients who developed irAEs without receiving steroid treatment demonstrated a harmonized pattern of cytokine fold-change, with 269/276 (97.5%) pairwise comparisons showing concordant direction of fold-change. (C) Patients who developed irAEs and received steroid treatment exhibited a discordant pattern of cytokine fold-change similar to patients without irAEs, with 214/276 (77.5%) pairwise comparison changing in the same direction.

{kind=link}
{kind=link}
{kind=link}
Example patient timelinesThe log2 fold-change of all cytokines over time were graphed for each patient. Timelines below each graph indicate ICI regimen (blue), irAEs (red), steroid treatment for irAEs (green), and RECIST response status (yellow). Black arrows indicate each ICI dosage cycle. A representative timeline is shown for a patient (#1) who did not develop irAEs during the Luminex profiling period, a patient (#29) who developed grade 1 dermatitis without receiving steroid treatment, and a patient (#44) who developed grade 2 arthralgia and received prednisone and methylprednisolone.
Conclusions Baseline cytokine levels correlate with specific irAEs in melanoma patients receiving ICIs. irAEs appear to drive a concordant pattern of cytokine fold-change, which is disrupted by corticosteroid administration. These findings should be validated in larger cohorts.
Ethics Approval Patients were identified from DFCI’s melanoma bio-specimen banking protocol (DFCI protocol 05-042)
References
Rahma OE, Ott PA. General Principles of Immune-Related Toxicities. In: Enrstoff M, Puzanov I, Robert C, Diab A, Hersey P, ed. SITC’s Guide to Managing Immunotherapy Toxicity. Society for Immunotherapy of Cancer; 2018: Chapter 5.
Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med 2010;363:711–723.
Faje AT, Lawrence D, Flaherty K, et al. High-dose glucocorticoids for the treatment of ipilimumab-induced hypophysitis is associated with reduced survival in patients with melanoma. Cancer 2018;124(18):3706–3714.
Arbour KC, Mezquita L, Long N, et al. Impact of baseline steroids on efficacy of programmed cell death-1 and programmed death-ligand 1 blockade in patients with non-small-cell lung cancer. J Clin Oncol 2018;36(28):2872–2878.
Libert C, Dejager L. How Steroids Steer T Cells. Cell Reports 2014;7(4):938–939.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.