Article Text

Abstract
Background Immune-checkpoint inhibitor (ICI)-pneumonitis that does not improve or resolve with corticosteroids and requires additional immunosuppression is termed steroid-refractory ICI-pneumonitis. Herein, we report the clinical features, management and outcomes for patients treated with intravenous immunoglobulin (IVIG), infliximab, or the combination of IVIG and infliximab for steroid-refractory ICI-pneumonitis.
Methods Patients with steroid-refractory ICI-pneumonitis were identified between January 2011 and January 2020 at a tertiary academic center. ICI-pneumonitis was defined as clinical or radiographic lung inflammation without an alternative diagnosis, confirmed by a multidisciplinary team. Steroid-refractory ICI-pneumonitis was defined as lack of clinical improvement after high-dose corticosteroids for 48 hours, necessitating additional immunosuppression. Serial clinical, radiologic (CT imaging), and functional features (level-of-care, oxygen requirement) were collected preadditional and postadditional immunosuppression.
Results Of 65 patients with ICI-pneumonitis, 18.5% (12/65) had steroid-refractory ICI-pneumonitis. Mean age at diagnosis of ICI-pneumonitis was 66.8 years (range: 35–85), 50% patients were male, and the majority had lung carcinoma (75%). Steroid-refractory ICI-pneumonitis occurred after a mean of 5 ICI doses from PD-(L)1 start (range: 3–12 doses). The most common radiologic pattern was diffuse alveolar damage (DAD: 50%, 6/12). After corticosteroid failure, patients were treated with: IVIG (n=7), infliximab (n=2), or combination IVIG and infliximab (n=3); 11/12 (91.7%) required ICU-level care and 8/12 (75%) died of steroid-refractory ICI-pneumonitis or infectious complications (IVIG alone=3/7, 42.9%; infliximab alone=2/2, 100%; IVIG + infliximab=3/3, 100%). All five patients treated with infliximab (5/5; 100%) died from steroid-refractory ICI-pneumonitis or infectious complications. Mechanical ventilation was required in 53% of patients treated with infliximab alone, 80% of those treated with IVIG + infliximab, and 25.5% of those treated with IVIG alone.
Conclusions Steroid-refractory ICI-pneumonitis constituted 18.5% of referrals for multidisciplinary irAE care. Steroid-refractory ICI-pnuemonitis occurred early in patients’ treatment courses, and most commonly exhibited a DAD radiographic pattern. Patients treated with IVIG alone demonstrated an improvement in both level-of-care and oxygenation requirements and had fewer fatalities (43%) from steroid-refractory ICI-pneumonitis when compared to treatment with infliximab (100% mortality).
- immunotherapy
- inflammation
- programmed cell death 1 receptor
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Highlights
Steroid-refractory immune-checkpoint inhibitor (ICI)-pneumonitis constitutes 18.5% of patients referred for multidisciplinary care of immune-related toxicity.
Steroid-refractory ICI-pneumonitis most commonly presents as diffuse alveolar damage on chest CT.
Patients treated with intravenous immunoglobulin had fewer fatalities (43%), improvements in patient oxygenation, and level-of-care.
Introduction
Immune-checkpoint inhibitor pneumonitis (ICI-pneumonitis) is the most frequently fatal toxicity from PD-(L)1 (PD-(L)1: programmed cell death protein-1/programmed death ligand-1) monotherapies.1 ICI-pneumonitis typically develops within the first 3 months (range: 9 days to 19 months) of ICI initiation, clinically improve with corticosteroids therapy within 48–72 hours, and require a median of 12 weeks to taper off corticosteroids completely.2–5 However, a subset of patients with ICI-pneumonitis do not clinically improve with corticosteroids alone and require further immunosuppression. This phenomenon, termed steroid-refractory ICI-pneumonitis, is defined as a lack of clinical improvement in ICI-pneumonitis after 48 hours to 2 weeks of corticosteroid treatment.6–9 However, the clinical and radiographic features of steroid-refractory ICI-pneumonitis are poorly understood and limited to individual cases and small case series.10–13 Additionally, patients who develop steroid-refractory ICI-pneumonitis almost universally succumb to this toxicity or the infectious complications of immunosuppressive management.2 14
Published guidelines recommend a variety of potential treatments for steroid-refractory ICI-pneumonitis including infliximab, intravenous immunoglobulin (IVIG), cyclophosphamide, or mycophenolate mofetil.4 15 16 However, the data supporting these choices are based largely on their use in other steroid-refractory irAEs.4 15 16 Infliximab, a TNF (Tumor-necrosis factor)-alpha inhibitor, has been used successfully to treat steroid-refractory ICI-colitis.17 18 IVIG is an admixture of antibodies from human sera that produces an immunomodulatory effect19 and has resulted in clinical improvements for patients with ICI-myasthenia gravis and ICI-thrombocytopenia.20 21 Thus, the optimum choice of immunosuppressive therapy for patients who develop steroid-refractory ICI-pneumonitis has yet to be established.
Given these gaps in our knowledge, we provide the first comprehensive report of the incidence, features, management, and outcomes of patients with steroid-refractory ICI-pneumonitis at a single, high-volume academic institution.
Methods
Study approval
Collection of clinical, radiographic, and pathological data was approved by the local IRB at Johns Hopkins Hospital.
Patient selection
We retrospectively identified patients who developed steroid-refractory ICI-pneumonitis after referral to an institutional immune-related multidisciplinary team or a dedicated pulmonary outpatient clinic for ICI-pneumonitis at the Johns Hopkins Hospital between January 2011 and January 2020. Patients may have been given ICIs either as part of a clinical trial or standard-of-care.
Incidence
Incidence of steroid-refractory ICI-pneumonitis was calculated by dividing the total number of steroid-refractory ICI-pneumonitis cases by the total ICI-pneumonitis cases referred internally for multidisciplinary input (inpatient and outpatient) between January 2011 and January 2020 at the Johns Hopkins Hospital.
Steroid-refractory ICI-pneumonitis definition and diagnosis
The diagnosis of ICI-pneumonitis was made by the treating medical oncologist and confirmed by a multidisciplinary team comprised of a pulmonologist, radiologist, second medical oncologist, and pathologist.22 ICI-pneumonitis was defined as clinical and radiographic lung inflammation either during or after anti-PD-(L)1 therapy. Patients with confirmed alternative diagnoses, such as cancer progression, radiation pneumonitis,23 or lung infection, were excluded with appropriate laboratory testing, diagnostic imaging and pathological evaluation. Steroid-refractory ICI-pneumonitis was defined as a failure of clinical improvement of ICI-pneumonitis after a minimum of 48 hours of high-dose corticosteroids (prednisone 1–2 mg/kg/day or more) to up to 14 days of corticosteroids.4 15 16 Clinical improvement in steroid-refractory ICI-pneumonitis was defined a reduction in either level-of-care or oxygen supplementation for ICI-pneumonitis. Death from steroid-refractory ICI-pneumonitis was defined as death attributed to ICI-pneumonitis or its management. Laboratory testing, radiologic imaging, and diagnostic bronchoscopy with bronchoalveolar lavage were performed at the discretion of the treating physician.
Radiology
Serial radiologic imaging including chest CT for steroid-refractory ICI-pneumonitis was captured and tumor radiologic response was assessed by RECIST (Response evaluation criteria in solid tumors) V.1.1 (v. 4.03) guidelines. Infiltrate types of steroid-refractory ICI-pneumonitis were categorized as diffuse alveolar damage (DAD), organizing pneumonia (OP), or non-specific by a board-certified thoracic radiologist (CTL), blinded to the clinical course of each patient. Radiologic DAD pattern of ICI-pneumonitis was defined as findings of ground glass opacities (GGOs) with or without intralobular lines (“crazy-paving”),24–26 traction bronchiectasis, and perilobular sparing; while the OP pattern was defined as lung parenchymal consolidation (occasionally with “reverse halo sign”) with traction bronchiectasis, and perilobular sparing.27 Non-specific findings included those that did not clearly demonstrate DAD or OP; including extensive nodularity with associated GGOs (pneumonitis not otherwise specified)2 and bronchial wall thickening with centrilobular tree-in-bud nodularity and consolidation (pneumonitis not-otherwise-specified).2
Level-of-care
The level-of-care received by each patient from the day of diagnosis of steroid-refractory ICI-pneumonitis was recorded and categorized as oncology floor/intermediate care, intensive care unit (ICU) without mechanical ventilation, or ICU with mechanical ventilation.28
Oxygen supplementation
The highest level of oxygen supplementation required for each patient, from the day of diagnosis of steroid-refractory ICI-pneumonitis, was recorded. The categories of oxygen supplementation required included: (1) no oxygen supplementation, (2) oxygen supplementation with nasal cannula, (3) high-flow nasal cannula (HFNC) or non-rebreather mask (NRB), (4) non-invasive positive-pressure ventilation (NIPPV; including bi-level positive airway pressure or continuous positive airway pressure), or (5) intubation with mechanical ventilation. A numerical value for the highest level of oxygen supplementation required per patient per hospitalization day was assigned. The percent time spent within each level of oxygen supplementation was calculated by aggregating individual patient data by immunosuppressive treatment group (IVIG alone, infliximab alone, combination of IVIG and infliximab (“combination”)). Additionally, the hospitalization time was subdivided into three categories: preimmunosuppression, during immunosuppression, or postimmunosuppression. Differences in percent hospitalization time by oxygen level were compared within immunosuppressive treatment groups by preimmunosuppression and postimmunosuppression hospitalization days, with the days of administration of immunosuppression (“during immunosuppression”) not included. Baseline supplemental oxygen requirement by patients and recorded increased oxygen use was calculated as a change from baseline.28 29
For patients who were readmitted to the hospital for steroid-refractory ICI-pneumonitis after an initial hospitalization for ICI-pneumonitis, time before reinitiation of immunosuppression during the second hospitalization was classified as preimmunosuppression. Patients who received more than one course of immunosuppressive therapy during the same hospitalization were classified as “postimmunosuppression” after the first immunosuppressive agent was administered if the half-life of the first dose of immunosuppressive therapy given overlapped the second (half-life IVIG: 21 days, half-life infliximab: 9.5 days).30 31
Statistical analysis
Study data were summarized using descriptive statistics using Stata V.16.1 (StataCorp). Results are reported with means with ranges, as appropriate. Categorical and ordinal variables were summarized as percentages.
Results
Incidence
The incidence of steroid-refractory ICI-pneumonitis in patients referred to a multidisciplinary immune-related toxicity team or pulmonary outpatient clinic for ICI-pneumonitis after multidisciplinary referral was 18.5% (12/65). Twenty-three patients (35.4%) were referred while receiving inpatient care and 42 (64.6%) were referred in the outpatient setting. The majority of referred patients with steroid-refractory ICI-pneumonitis had high grade toxicity at initial presentation of ICI-pneumonitis (grade 3+: 50.8%, n=33/65) while a minority had grade 2 (43.1%) and grade 1 toxicity (6.2%).
In the 12 patients who developed steroid-refractory ICI-pneumonitis, ICI-pneumonitis eventually resolved in four patients, while eight patients died either from steroid-refractory ICI-pneumonitis or its complications.
Study population
Baseline characteristics of patients who developed steroid-refractory ICI-pneumonitis, including subgroup characteristics based on immunosuppressive treatment received (IVIG only=7, infliximab only=2, combination=3), are depicted in table 1. Complete patient-level details are shown in online supplemental table 1.
Supplemental material
Baseline characteristics of patients with steroid-refractory ICI-pneumonitis by immunosuppressive treatment
We identified 12 patients with steroid-refractory ICI-pneumonitis. The mean age at diagnosis of ICI-pneumonitis was 66.8 years (range: 35–85 years), 50.0% (6/12) patients were male, 83.3% were Caucasian, 75.0% were current/former smokers. The majority of patients had lung carcinoma (75%, 9/12), predominantly non-small cell lung carcinoma (8/9). Nearly all patients had received prior chemotherapy (91.6%). Seven patients (58.3%) had a distant history of chest radiotherapy (range: 8–66 Gy) administered 276–739 days prior to onset of ICI-pneumonitis. Antitumor response to ICI assessed at 3 months post ICI-start demonstrated that 25.0% of patients had a partial response (PR) to therapy, 33.3% had stable disease (SD), and 41.7% had progressive disease (PD) by RECIST V.1.1.
Clinical features
The clinical features of patients who developed steroid-refractory ICI-pneumonitis are outlined in table 2. All patients were symptomatic (grade 2+) at initial diagnosis of ICI-pneumonitis (grade 2, 25%, n=3/12; grade 3, 75%, n=9/12) and developed ICI-pneumonitis early in their treatment course (mean number of ICI doses: 5, range: 3–12). Steroid-refractory ICI-pneumonitis developed between 40 and 127 days (median: 85 days) after the first dose of ICI and resulted in a hospitalization of between 6 and 35 total days (median: 14 days) All patients were treated with high-dose corticosteroids (median dose of prednisone equivalents: 75 mg/day (range: 50–237.5 mg/day) prior to receiving additional immunosuppressive therapy. Pulmonary medicine specialists were consulted in all cases, and infectious disease specialists in 58.3% (7/12) of cases.
Clinical features and management of steroid-refractory ICI-pneumonitis by immunosuppressive treatment
Patients were treated with either IVIG alone, infliximab alone, or a combination of IVIG and infliximab. Patients given IVIG generally had concerns for a superimposed infectious process due to immunosuppression from long-term corticosteroid use.
Steroid-refractory ICI-pneumonitis-related deaths were most frequent in those with PD at 3 months post-ICI (n=4/5, 80%), compared with SD (n=2/4, 50%) or PR (n=1/3, 33%). Following a similar pattern, fewer patients who had PD demonstrated clinical improvement after immunosuppression (n=1/5, 20%) than those who had PR (n=3/3, 100%) or SD (n=3/4, 75%).
Radiographic features
We examined serial CT imaging of patients who developed steroid-refractory ICI-pneumonitis at four timepoints: pre-ICI, at initial ICI-pneumonitis diagnosis, postcorticosteroids, and postadditional immunosuppression (up to 4 weeks). Representative CT images of patients within each treatment group (IVIG, infliximab, and combination), stratified by clinical improvement or lack thereof are shown in figure 1. Specific CT findings of our cohort are described in online supplemental figure 1. Radiographic features at the time of ICI-pneumonitis diagnosis consisted predominantly of a DAD pattern across all immunosuppressive treatments received (50%, 6/12), with OP (33.3%, 4/12) and other (16.7%, 2/12) patterns identified in a minority of cases. Most cases of steroid-refractory ICI-pneumonitis demonstrated disease in bilateral lung fields (75%, 9/12).
Supplemental material

Serial radiologic imaging in patients with steroid-refractory ICI-pneumonitis. Illustrative images from six cases, each representing one patient treated with IVIG, infliximab, or combination immunosuppression and either demonstrated improvement with immunosuppression or did not have improvement with immunosuppression. Images are taken at 1: Pre-ICI: before immune checkpoint inhibitor therapy start, 2: Initial dx ICI-pneumonitis scan: CT scan at the time of diagnosis of ICI-pneumonitis, 3: Poststeroids: postcorticosteroids, prior to additional immunosuppression, 4: Postadditional IS: within 4 weeks of administration of additional immunosuppression as outlined in top panel. Red circles in panel (2) show diagnostic features of ICI-pneumonitis. Blue circles in panel (4) show areas of worsening ICI-pneumonitis in patients whose steroid-refractory ICI-pneumonitis. Corresponding patient labels are noted in the bottom right hand corner of each image. IVIG, intravenous immunoglobulin; ICI, immune-checkpoint inhibitor; dx, diagnosis; IS, immunosuppression. The infiltrate classification is depicted in online supplemental figure 1.
Immunosuppressive management and outcomes
Intravenous immunoglobulin
After lack of clinical improvement with high-dose corticosteroids, seven patients were treated with IVIG (0.4 g/kg/day) over 5 days in accordance with institutional practices. IVIG was administered a mean of 17 days after corticosteroid initiation (range: 1–96 days). Once completing IVIG therapy, two patients (29%, n=2/7) sustained an improvement in ICI-pneumonitis grade (grade 3 to grade 2), while two patients (29%) had their ICI-pneumonitis clinically stabilize (grade 2=1; grade 3=1), and three patients worsened to grade 5 (43%, n=3/7).
Patient level details are depicted in figure 2. All patients, excluding one, required ICU-level care. Patient 2 did not require ICU-level care as oxygen levels were maintained with HFNC. Shortly after discharge, he was admitted to a palliative care service. Most patients (5/7, 71.4%) received one course of IVIG during their hospitalization. Patient 6 received two doses of IVIG during a prolonged hospital stay, but only had an improvement in level-of-care after the first dose only. Patient 3 received IVIG during each of three separate hospitalizations and sustained a clinical benefit (reduced oxygen requirements) after each administration of IVIG.
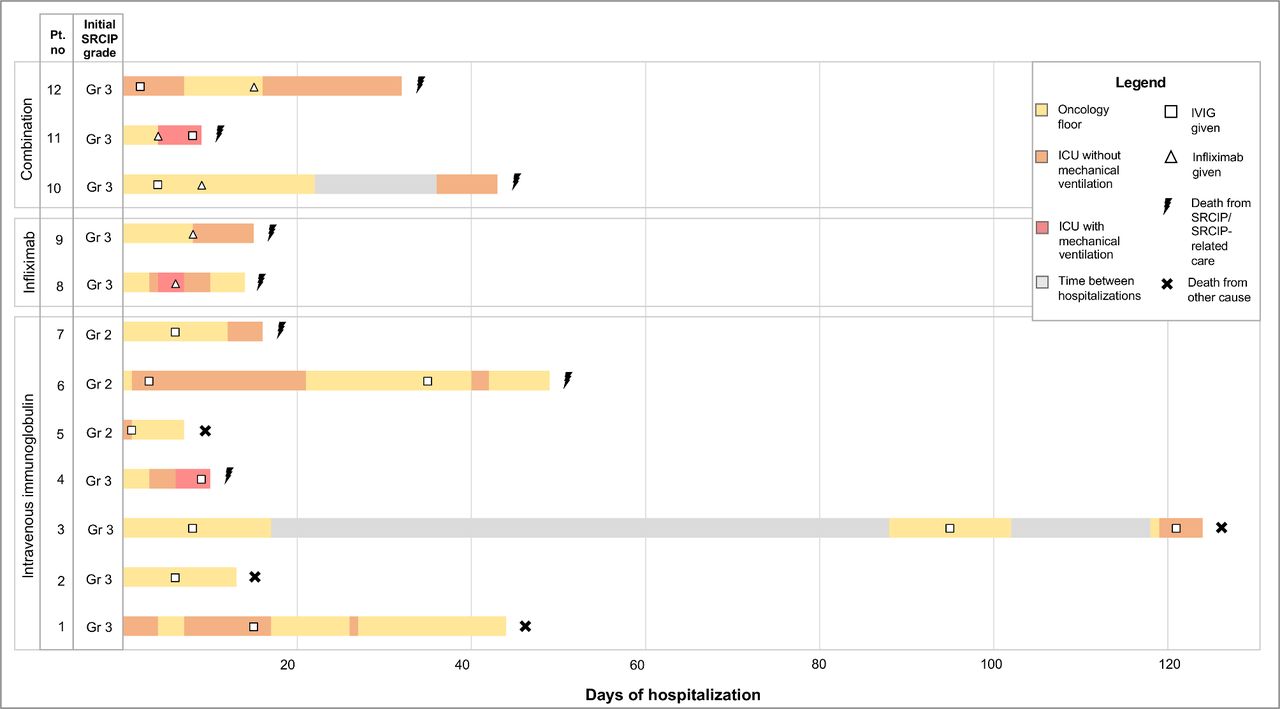
Clinical course of steroid-refractory immune-checkpoint inhibitor pneumonitis (ICI- pneumonitis) stratified by additional immunosuppressive treatment received after corticosteroids. CTCAE ICI-pneumonitis grade, immunosuppressive therapy, level-of-care, and clinical ICI-pneumonitis outcome are shown over time during days of hospitalization. Yellow shaded areas indicate admission to the oncology unit, orange shaded areas represent admission to the ICU without the need for mechanical ventilation, red shaded areas show admission to the ICU with mechanical ventilation, and gray areas represent time between hospitalizations if a patient was discharged then readmitted for further treatment. White squares within each hospitalization bar represent when IVIG was given and white triangles show when infliximab was given. The lightning bolt following hospitalization bars indicate death from SRCIP/SRCIP-related care. Pt., patient; no., number; Gr, grade; ICU, intensive care unit; ICI, immune checkpoint inhibitor; IVIG, intravenous immunoglobulin; SRCIP, steroid-refractory ICI-pneumonitis.
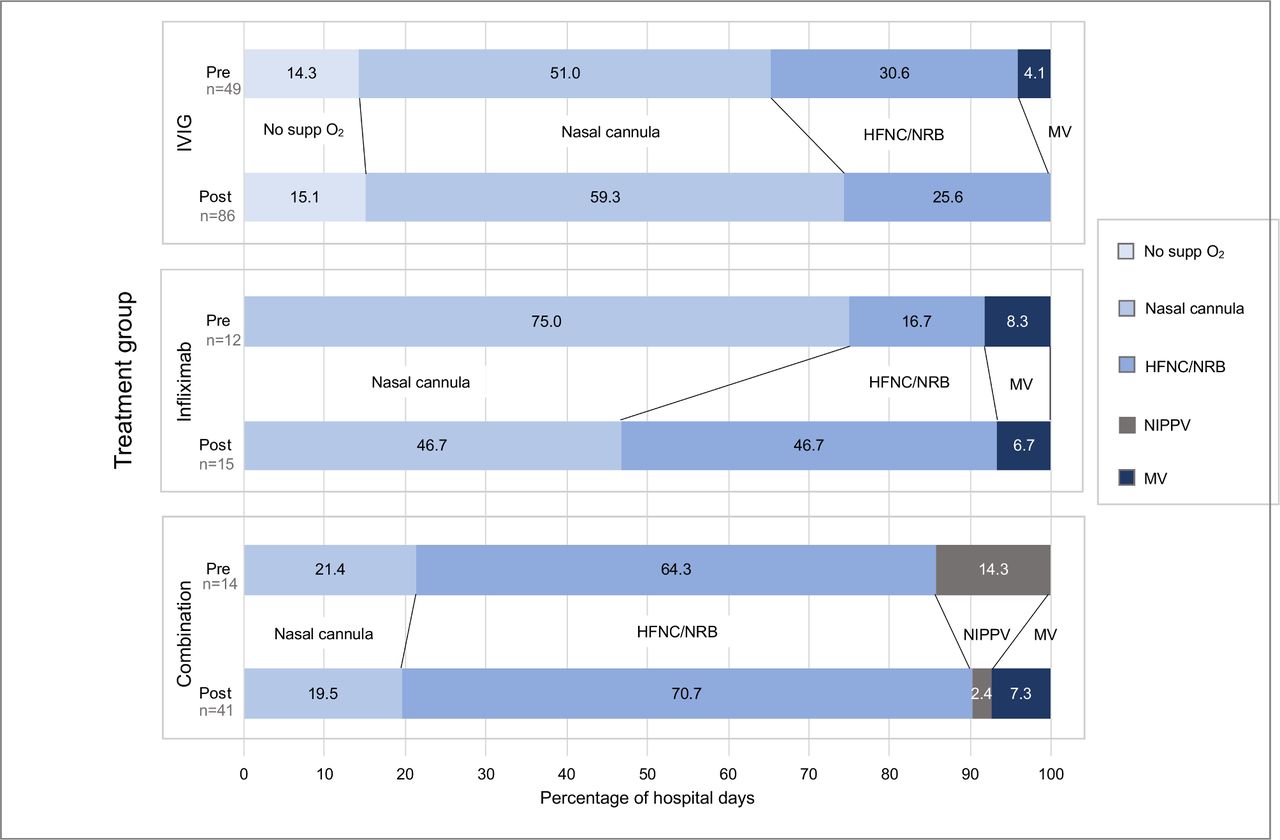
Oxygen supplementation requirements for patients treated with IVIG alone are depicted in figure 3. As a group, patients were hospitalized for 49 days total (n=7 patients) prior to IVIG administration and no patients required oxygen supplementation at baseline. During the majority of hospitalization time, patients treated with IVIG required oxygen supplementation via nasal cannula (51%, n=25/49 days), HFNC/NRB (30.6%, n=15/49 days), no oxygen supplementation (14.3%, n=7/49 days), or mechanical ventilation (4.1%, n=2/49 days). After administration, patients receiving IVIG were hospitalized for 86 days total. After IVIG was administered, we observed that no patients required mechanical ventilation, fewer patients required HFNC/NRB (25.6%), and some required no oxygen supplementation (15.1%).

{kind=link}
{kind=link}
{kind=link}
Oxygen supplementation required preimmunosuppression and postimmunosuppression as a percentage of hospitalization days. Groups were separated by additional immunosuppression given (IVIG, infliximab, or combination). Excluded 41 hospitalization days from the IVIG group, 2 hospitalization days from the infliximab group, and 15 hospitalization days from the combination group from the calculation. supp, supplemental; O2, oxygen; HFNC, high-flow nasal cannula; IVIG, intravenous immunoglobulin; NRB, non-rebreather mask; NIPPV, non-invasive positive pressure ventilation; MV, mechanical ventilation.
In terms of clinical irAE outcome, two patients (29%, n=2/7) clinically improved and were discharged from the hospital and two patients whose ICI-pneumonitis stabilized (29%, n=2/7) subsequently died from progression of cancer (n=3). For three patients whose ICI-pneumonitis worsened (43%), steroid-refractory ICI-pneumonitis was the cause of death. Patient 3 developed infectious complications after receiving IVIG (Herpes zoster shingles), however, ultimately died from cancer progression.
Infliximab
Two patients received infliximab 8 days (range: 7–8 days) after commencement of high-dose corticosteroids. All patients in our series receiving infliximab were given one dose (5 mg/kg), which is in accordance with current published literature describing successful use of infliximab for steroid-refractory ICI-pneumonitis in selected cases.10 13 After receiving infliximab, steroid-refractory ICI-pneumonitis worsened in one patient (grade 3 to grade 4) and improved in the other (grade 4 to grade 3).
Both patients in the cohort received infliximab only receiving ICU-level care, one of which (patient 8) required mechanical ventilation (figure 2). This patient was weaned off the ventilator after infliximab administration and transitioned to the oncology floor. Patient 9 required escalation to ICU-level care after receiving infliximab and was transitioned to palliative care shortly thereafter.
Neither patient required oxygen supplementation prior to the diagnosis of ICI-pneumonitis. Prior to infliximab administration, both patients contributed 12 total days of hospitalization. Of this time, the majority was spent with a requirement for oxygen supplementation by nasal cannula (75%, n=9/12 days), followed by HFNC/NRB (16.7%, n=2/12 days), and mechanical ventilation (8.3%, n=1/12 days). After infliximab administration, the proportion of time spent requiring nasal cannula and mechanical ventilation decreased, while time spent requiring HFNC/NRB increased by 30% (nasal cannula: 46.7%; HFNC/NRB: 46.7%; mechanical ventilation: 7%). Patient 9 had a new oxygen supplementation requirement on discharge.
Both patients died from complications of steroid-refractory ICI-pneumonitis. After discharge, Patient 9 passed from respiratory failure secondary to steroid-refractory ICI-pneumonitis in hospice. Patient 8 developed parainfluenza pneumonia related to infliximab therapy and died from respiratory complications.
Combination immunosuppression
Three patients were treated with sequential IVIG and infliximab. Once hospitalized, patients were administered IVIG (0.5 g/kg/day) a mean of 2 days and infliximab (5 mg/kg) a mean of 9 days after commencing high-dose corticosteroids. Two patients received IVIG first in their hospital course (patient 10=day 4, patient 12=day 2), followed by infliximab (patient 10=day 9, patient 12=day 15), while patient 11 received infliximab first (day 4), followed by IVIG (day 8). All three patients had a worsening in ICI-pneumonitis grade (grade 3 to grade 5) after administration of both immunosuppressive therapies and died from the complications of steroid-refractory ICI-pneumonitis.
All three patients required ICU-level care (figure 2). Initially, patient 10 improved clinically after receiving combination immunosuppression and was discharged for 14 days with a new oxygen requirement. However, this patient developed worsening symptoms (increasing shortness of breath) warranting readmission. Patient 11 received both immunosuppressive agents sequentially while mechanically ventilated, but was not able to be weaned off ventilation, transitioned to palliative care, and died from steroid-refractory ICI-pneumonitis. Patient 12 had early clinical benefit (downgrade from ICU to oncology floor) after administration of IVIG, however, this patient’s ICI-pneumonitis subsequently worsened. The patient was administered infliximab before a return transfer to the ICU but died from steroid-refractory ICI-pneumonitis 16 days after infliximab administration.
In terms of oxygen requirement (figure 3), only patient 12 had a baseline oxygen requirement prior to hospitalization. In total, patients contributed 14 hospitalization days before administration of their first immunosuppressive agent. The majority of this time was spent requiring HFNC/NRB (64.3%, n=9/14 days). A minority of time was spent requiring nasal cannula (21.4%) and NIPPV (14.2%). After administration of immunosuppressive therapy, the group contributed 41 hospitalization days and required more invasive methods of oxygen supplementation. The percentage of hospitalization days requiring nasal cannula (21.4% to 19.5%) and NIPPV (14.3% to 2.4%) decreased after administration of immunosuppressive therapy, while the time spent requiring HFNC/NRB increased (by 6.4%) and time spent requiring mechanical ventilation (0% to 7.3%) increased.
Taken together, all patients treated with infliximab, either alone (n=2) on as part of combination immunosuppressive therapy (n=3), died due to steroid-refractory ICI-pneumonitis or infectious complications of infliximab therapy.
Discussion
In this, the first comprehensive cohort study of patients with steroid-refractory ICI-pneumonitis, we identify several clinically relevant findings. First, the incidence of steroid-refractory ICI-pneumonitis in those referred for multidisciplinary care was 18.5%. Second, we observe that steroid-refractory ICI-pneumonitis tends to occur early in a patient’s treatment course, and exhibits a radiographic pattern of bilateral DAD. Third, we identify that when treated with IVIG, infliximab, or the combination—patients with steroid-refractory ICI-pneumonitis exhibit very different clinical courses. Patients treated with IVIG generally demonstrated improvements in level-of-care and a reduced oxygen requirement, while those treated with infliximab monotherapy or the combination had an increased level-of-care and oxygen requirement. Finally, we observed a higher rate of fatality from steroid-refractory ICI-pneumonitis or its complications, in those treated with an infliximab-containing approach.
Steroid-refractory ICI-pneumonitis is a fatal clinical phenomenon, and its incidence is poorly understood.10 11 A recent abstract by Beattie et al estimated that 0.5% of all patients with irAEs received additional immunosuppression.12 In our study, we estimate the incidence of steroid-refractory ICI-pneumonitis among patients referred for multidisciplinary care, at a surprisingly high 18.5%. Prior studies have described the radiographic features of steroid-refractory ICI-pneumonitis in individual patient cases,13 and we provide the largest experience to date, of 12 patients. Our study is the first to demonstrate that IVIG may be used successfully to treat steroid-refractory ICI-pneumonitis in multiple patients; with only one prior study in which a single case of steroid-refractory ICI-pneumonitis demonstrated improvement with IVIG.11
Importantly, our study is the first to objectively quantify the clinical outcomes of treatment of steroid-refractory ICI-pneumonitis, by assessing patient level-of-care and oxygen supplementation preimmunosuppressive and postimmunosuppressive treatment. Wiertz et al recently depicted clinical improvements in steroid-refractory hypersensitivity pneumonitis after cyclophosphamide therapy, using pulmonary function test metrics (forced vital capacity).32 More recently, a randomized control trial comparing normobaric versus hyperbaric oxygen therapy for COVID-19 utilized oxygen supplementation levels as metric of clinical improvement.33 Building on this experience, our analysis demonstrates that patients treated with IVIG alone had improved oxygenation. This was aligned with an overall improvement in level-of-care, ICI-pneumonitis grade, and fewer deaths from steroid-refractory ICI-pneumonitis in these patients.
While our study has several strengths, there were also important limitations. First, the retrospective nature of this study may limit its generalizability to other centers and clinical situations. Second, there is no standard definition for steroid-refractory ICI-pneumonitis, therefore, our study may have included patients whose ICI-pneumonitis was either steroid-dependent or steroid-resistant. This highlights the need to elucidate clearer definitions for these terms. Our estimate of the incidence of steroid-refractory ICI-pneumonitis is derived from those referred for multidisciplinary care, who likely represent more complex cases of ICI-pneumonitis, and thus may be an overestimation of the true incidence of this phenomenon. Improvement in steroid-refractory ICI-pneumonitis was assessed clinically, and in some cases, without imaging, therefore, some patients did not have CT imaging after receiving steroid therapy. Importantly, the conclusions of this study are limited by small patient numbers and the clinical status of patients at the time of immunosuppressive treatment. That is, patients treated with IVIG may have had less severe steroid-refractory ICI-pneumonitis at baseline (having less need for invasive oxygen supplementation), which may have contributed to the overall improved clinical findings for this group. Finally, since there are multiple guideline-based treatment options for this phenomenon, there was a lack of an established paradigm for patients being treated with either IVIG, infliximab, or the combination. This limits our ability to identify an immunosuppressive treatment that is truly preferable. The poorer outcomes faced by those who received infliximab (either as monotherapy or combination) may thus be due to confounding by indication and reflect timing of therapy or severity of steroid-refractory ICI-pneumonitis rather than a lack of efficacy of infliximab itself. We attempt to address some of these limitations by assessing the functional impact of ICI-pneumonitis through evaluation of oxygen requirement and level-of-care across all cases. A prospective trial is currently underway in order to evaluate these therapies for steroid-refractory ICI-pneumonitis (NCT04438382).
In conclusion, we report the incidence, clinical, radiologic features, management and outcomes of a cohort of patients with steroid-refractory ICI-pneumonitis. Steroid-refractory cases occurred in 18.5% among patients diagnosed with ICI-pneumonitis referred to a multidisciplinary team. The development of steroid-refractory ICI-pneumonitis occurred early in patients’ treatment course and demonstrated radiologic patterns of bilateral DAD. Importantly, patients treated with IVIG both demonstrated improvement in their oxygen requirements and level-of-care and also had reduced fatalities from steroid-refractory ICI-pneumonitis, while those treated with an infliximab-containing regimen had poorer outcomes. Prospective data from clinical trials in this area are needed to identify the optimum immunosuppressive approach for steroid-refractory ICI-pneumonitis.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Collection of clinical, radiographic, and pathological data was approved by the local IRB at Johns Hopkins Hospital.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @AanikaBalaji, @DrJNaidoo
AB and MH contributed equally.
KS and JN contributed equally.
Correction notice This article has been corrected since it was first published online. The dosage unit g/kg has been amended to mg/kg for infliximab.
Contributors AB, MH, CTL, JF, KM, JRB, PMF, CH, LZ, VL, PBI, SKD, KS, JN: identification, analysis, and interpretation of patient data. CTL: radiological data analysis and interpretation. AB, MH, JN, KS: study design, conceptualization, and manuscript writing. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.