Article Text

Abstract
Background Immune checkpoint inhibitors (ICIs) benefit patients with multiple cancer types, however, additional predictive biomarkers of response are needed. CD274 (programmed cell death ligand-1, PD-L1) gene rearrangements are positively associated with PD-L1 expression and may confer benefit to ICI, thus a pan-cancer characterization of these alterations is needed.
Methods We analyzed 283,050 patient samples across multiple tumor types that underwent comprehensive genomic profiling for activating CD274 rearrangements and other alterations. The DAKO 22C3 Tumor Proportion Scoring (TPS) method was used for PD-L1 immunohistochemistry (IHC) testing in a small subset with available data (n=55,423). A retrospective deidentified real-world clinico-genomic database (CGDB) was examined for ICI treatment outcomes. We also report a detailed case of CD274-rearranged metastatic rectal adenocarcinoma.
Results We identified 145 samples with functional rearrangements in CD274. There were significant enrichments for PIK3CA, JAK2, PDCD1LG2, CREBBP, and PBRM1 co-mutations (ORs=2.1, 16.7, 17.8, 3.6, and 3.4, respectively, p<0.01). Genomic human papillomavirus (HPV)-16, Epstein-Barr virus, and mismatch repair genes also co-occurred (OR=6.2, 8.4, and 4.3, respectively, p<0.05). Median tumor mutational burden (TMB) was higher compared with CD274 wild-type samples (7.0 vs 3.5 mutations/Mb, p=1.7e-11), with disease-specific TMB enrichment in non-small cell lung, colorectal, unknown primary, and stomach cancers. PD-L1 IHC skewed toward positivity (N=39/43 samples with ≥1% positivity). Of eight patients from the CGDB, three remained on ICI treatment after 6 months. Separately, one patient with metastatic rectal adenocarcinoma experienced a pathologic complete response on chemoimmunotherapy.
Conclusions CD274 gene rearrangements are associated with increased PD-L1 IHC scores, higher TMB, and potential clinical benefit in ICI-treated patients with cancer.
- immunotherapy
- biomarkers
- tumor
- immune tolerance
- programmed cell death 1 receptor
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. All data relevant to the study are included in the article or uploaded as supplementary information. The data generated by the research that support our article will be provided in the supplements.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Immune surveillance is an important mechanism by which malignant cells are eliminated before overt cancer can emerge, and therefore, applies a selective pressure for developing tumors to maintain an immune-suppressed microenvironment.1 Over the past decade, immune checkpoint inhibitors (ICIs) have transformed cancer care, with anti-programmed cell death 1 (PD-1) and antiprogrammed cell death ligand 1 (PD-L1) therapies showing strong efficacy2–4 and subsequent US Food and Drug Administration (US-FDA) approvals for clinical use in multiple tumor types.5 6
Expression of PD-L1 as detected by immunohistochemistry (IHC) has identified a subset of tumors that may be susceptible to ICI,3 however, the landscape of PD-L1 IHC testing is complex6 and it remains insufficient to consistently predict response to ICI.7–9 Many studies have also shown that high tumor mutational burden (TMB) is associated with a high neo-antigen burden and a subsequent presence of activated effector T cells that results in enhanced responsiveness to ICI.10 11 Accordingly, single agent pembrolizumab was approved by the FDA for metastatic solid tumors with TMB of at least 10 mutations per megabase.12 Despite this, ICI benefits remain restricted to a subset of patients,13 warranting research into additional predictive biomarkers of checkpoint blockade response. Tumors exhibiting focal amplification of CD274 (gene encoding PD-L1) have shown durable responses to ICI9 14–16 but little is known about the association of CD274 rearrangements and PD-1/PD-L1 checkpoint blockade. Previously, it has been reported that PD-L1 structural variants are associated with aberrant expression in T-cell leukemia, and a rare number of other solid tumors in The Cancer Genome Atlas.17
In this study, we describe a pan-cancer analysis of CD274 rearrangements identified through comprehensive genomic profiling (CGP) assessed on more than 400 tumor types comprised of more than 250 000 tumor samples sequenced during routine clinical care, and its association with ICI biomarkers. In addition, we also report on a CD274 rearranged rectal adenocarcinoma patient with complete response to FOLFOXIRI with nivolumab, and on multiple CD274 rearranged patients with sustained clinical benefit to ICI from a deidentified real-world clinico genomic database (CGDB).
Methods
Comprehensive genomic profiling
A total of 283,050 clinically advanced cases of cancer underwent CGP18 in a Clinical Laboratory Improvement Amendments (CLIA)-certified, College of American Pathologists (CAP) accredited laboratory (Foundation Medicine, Cambridge, Massachusetts, USA). CGP on 0.8–1.1 Mb of the coding genome was performed on hybridization-captured, adapter-ligation based libraries, to identify genomic alterations (GA) (base substitutions, small insertions/deletions, copy number alterations and rearrangements) in exons and select introns in up to 404 genes, TMB and microsatellite instability status (MSI).
The median sequencing depth of coverage was 830x. Functional rearrangements were defined as chromosomal translocation, deletion, duplication or inversion events with one breakpoint in CD274 (NM_014143) intron 5 to 3’-UTR and a second breakpoint outside of CD274. Such rearrangements are projected to incur loss of inhibitory microRNA binding site while leaving the Ig-like domains intact, causing PD-L1 overexpression.19 TMB was calculated as the number of non-driver somatic coding mutations per megabase of genome sequenced.20 MSI status was determined by analyzing 114 intronic homopolymer repeat loci for length variability and MSI high was defined as described previously.21 All patient data were analyzed retrospectively in a de-identified manner and all GA prevalence reported in this study only include alterations described as functional/pathogenic in literature and seen in the Catalog of Somatic Mutations in Cancer repository22 or had a likely functional status (frameshift/truncation events in tumor suppressor genes). Variants of unknown significance (VUS) were not studied.
PD-L1 IHC testing was run and interpreted by experienced board-certified pathologists according to the manufacturer instructions in a CLIA-certified and CAP-accredited laboratory (Foundation Medicine, Morrisville, North Carolina, USA) for a subset of specimens (n=55,423/283,050) in this cohort.23 24 DAKO’s Tumor Proportion Scoring (TPS) method was used to score these cases where TPS=proportion of PD-L1 positive tumor cells.
Genomic viral calling
Presence of oncogenic viruses in tumor specimens was determined by the identification of DNA sequences consistent with genomic viral DNA. Sequencing reads left unmapped to the human reference genome (hg19) were de novo assembled by Velvet25 26 and the assembled contigs were competitively aligned by BLASTn27 to the NCBI database of over 3 million known viral nucleotide sequences. A positive viral status was determined by contigs at least 80 nucleotides in length and with at least 97% identity to the Basic Local Alignment Search Tool (BLAST) sequence,28 however, because this is a research use only finding, viral nucleic acid content is not found on commercial Foundation Medicine (FMI) reports.
Statistical analysis
All statistical analyses were performed using R software (R Foundation for Statistical Computing, V.3.6.0).29 Proportions of categorical variables were compared using the Fisher’s exact test while continuous variables were compared using the Wilcoxon rank sum test. All p values are two sided and multiple hypothesis testing correction was performed using the Benjamini-Hochberg procedure to calculate the false discovery rate (FDR) of interactions between CD274 rearrangements and genomic alterations. Genomic coordinates were identified using hg19 on the University of California Santa Cruz Genome Browser.30
Clinico-genomic cohort
This study used the nationwide (US-based) deidentified Flatiron Health-FMI CGDB (FH-FMI CGDB). The deidentified data originated from approximately 280 US cancer clinics (~800 sites of care). Retrospective longitudinal clinical data (collected through September 30, 2020) were derived from electronic health record data, comprising patient-level structured and unstructured data, curated via technology-enabled abstraction, and were linked to genomic data derived from FMI CGP tests in the FH-FMI CGDB by deidentified, deterministic matching.31
Genomic alterations were identified via CGP as described above. For CD274 rearranged patients treated with ICI therapy (Monotherapy or combination therapy; N=8), duration of line of therapy (real-world time at risk of treatment discontinuation) was calculated as the time between the earliest and last recorded instance of drug regimen administration/scheduled drug regimen administration. Treatment was considered discontinued due to change in line of therapy or death of the patient, all others were censored. Real-world response data (available for N=1 patient) was defined as the clinician assessment of change in disease burden following radiographic imaging during a line of therapy32
Results
Characteristics of CD274 rearranged tumors in a large pan-cancer cohort
We assessed the genomic landscape of CD274 rearrangements across 419 different tumor types that comprised 283 050 patient samples. In total, we identified 145 samples (0.05%) with a functional rearrangement in CD274 (see methods section for definition of functional rearrangement). This cohort was 52.4% female, with a median age of 64.5 years (range 16.0–89+), and 44.2% specimens were metastatic tumor biopsies (online supplemental table 1). Interestingly, when compared with the CD274 wild type cohort, the CD274 rearranged cohort was significantly enriched for the admixed American genomic ancestry (8.6% in the wild-type cohort vs 14.5% in the rearranged cohort, p=0.02; online supplemental table 1, this association remained significant when adjusted for tumor type in a multivariate logistic regression analysis, p=0.05, online supplemental table 2).
Supplemental material
We found that nearly all of these samples harbored rearrangements that affected the 3’-UTR within 135 base pairs of the wild-type stop codon (138/145 with breakpoint within 5% of exon 7; figure 1A). Of the types of genomic events identified, most were rearrangements, with a small number of focal duplication, deletion, and truncation events (online supplemental figure 1). Importantly, CD274 amplifications occurred in 25% of the CD274 rearranged cohort (odds ratio (OR)=4.6, p=5.3e–44).
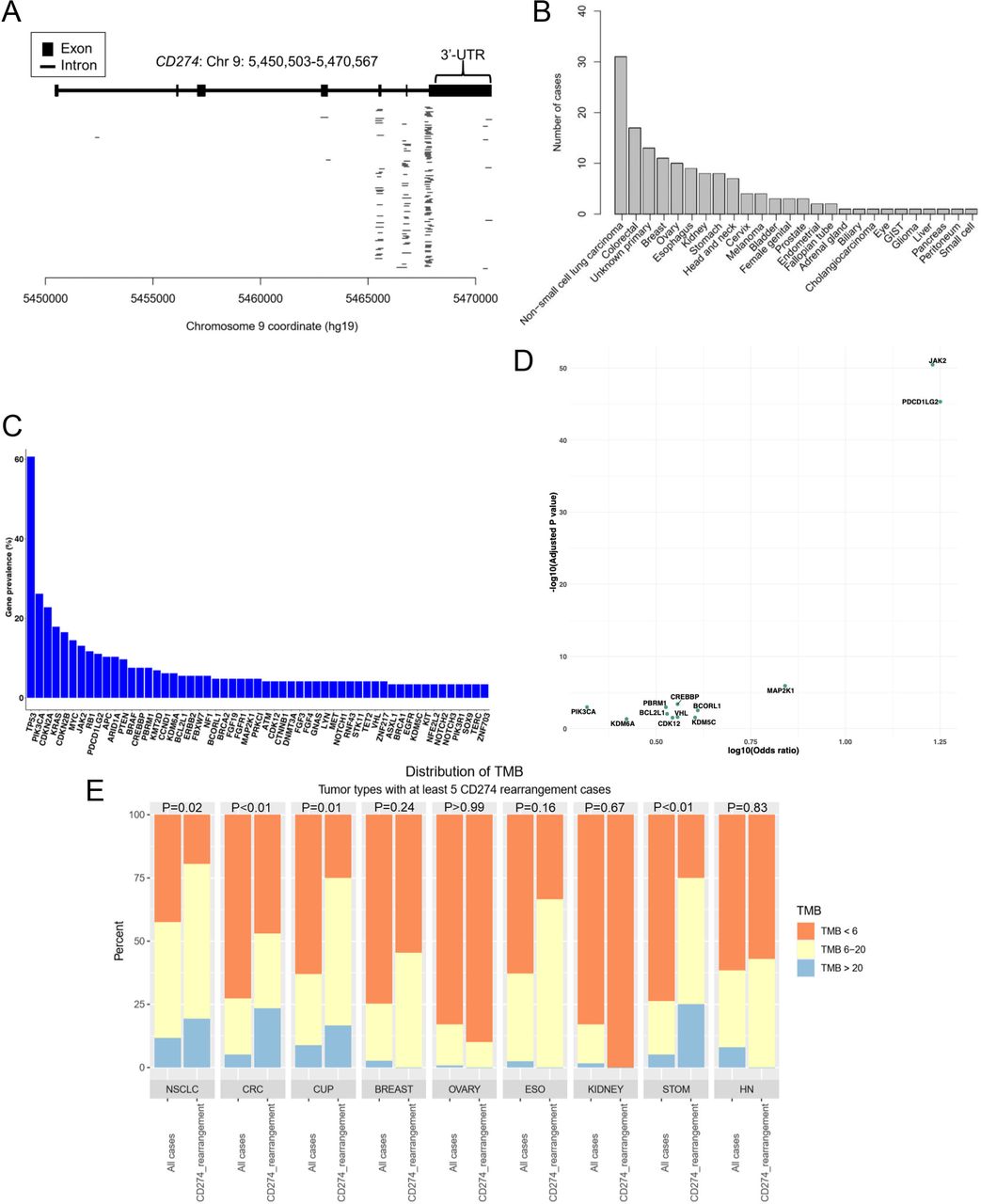
Characteristics of CD274 rearrangement positive tumors in FMI research dataset. (A) Gene diagram of CD274 with 3’-UTR annotated demonstrating that the majority of cases in this study harbor alterations that impact the native exon 7 sequence very near to the wild-type stop codon. (B) Distribution of disease groups harboring CD274 rearrangements ranked by prevalence. (C) Distribution of co-occurring gene mutations among CD274 rearranged cases. (D) Volcano plot of co-occurring gene alterations with CD274 rearrangements. The two-tailed Fisher’s exact test was used to estimate the p values and odds ratios of associations between gene alterations and CD274 rearrangements. The Benjamini-Hochberg procedure was used estimate the adjusted p values. Only genes with a pan-cancer prevalence ≥0.5% and an adjusted p value≤0.05 were labeled (E) Distribution of TMB in CD274 rearrangement positive tumors compared with respective overall tumor type population. Two-tailed Fisher’s exact tests were used to estimate the p values of the relative distribution of TMB status in the CD274 rearranged cohort versus molecularly unselected tumor type matched cases (unselected N=19,794-NSCLC; 12,642-CRC; 2727-ESO; 1597-STOM; 5595-CUP; 6512-OVARY; 1711-KIDNEY). 3'-UTR, 3' untranslated region; CRC, colorectal carcinoma; CUP, carcinoma of unknown primary; ESO, esophageal carcinoma; KIDNEY, kidney carcinoma; NSCLC, non-small cell lung carcinoma; OVARY, ovarian carcinoma; STOM, stomach carcinoma; TMB, tumor mutational burden.
The most common tumor type harboring CD274 rearrangements was non-small cell lung cancer (figure 1B), followed by colorectal cancer and cancer of unknown primary. Within the CD274-rearranged cohort, GA in TP53 were the most common (60.7%) followed by GA in PIK3CA (26.2%), CDKN2A (22.8%), KRAS (17.9%), CDKN2B (16.6%), and MYC (14.5%; figure 1C). Multiple genes were enriched with CD274 rearrangements (figure 1D) including PIK3CA (OR=2.1, FDR adjusted p=0.001), JAK2 (16.7, 3.6e–52), PDCD1LG2 (17.8, 4.8e-46), CREBBP (3.6, 4.2e-4) and PBRM1 (3.4, 0.001), though, only 13% and 11% of the CD274 rearranged cohort harbored alterations in JAK2 and PDCD1LG2, respectively, despite their adjacent chromosomal localization. Interestingly, genomic human papillomavirus (HPV)-16 (6.2, 1.1e-10), genomic Epstein-Barr virus (EBV) (8.4, 0.003) and genes involved in mismatch repair such as MLH1 (4.3, 0.052) were also enriched among CD274 rearrangements.
Importantly, within the CD274 rearranged cohort, there was an enrichment for tumor types harboring relatively high TMB, (figure 1E), but 92.4% (N=133/144; MSI was unavailable for one case) of the cohort was microsatellite stable. Subsequently, while investigating this propensity for high TMB, we observed the median TMB across the cases harboring CD274 rearrangements (7.0 muts/Mb, N=145) to be significantly greater than that observed in the CD274 wild-type cohort (3.5 muts/Mb, N=2 82 643, p=1.7e–11; TMB was unavailable for 262 cases). Compared with the subset of the CD274 wild-type cohort harboring any genomic rearrangement (of any pathogenicity status, N=96 365), the median TMB was still significantly higher in the CD274 rearranged cohort, suggesting this observation is not reflective of generalized genomic instability, but is specific to CD274 (7.0 muts/Mb, N=145 vs 4.4 muts/Mb, N=96 365, p=0.0003; online supplemental figure 2A). In addition, multivariate logistic regression found the association between CD274 rearrangements and TMB-high statistically significant, with effect size comparable to that of CD274 amplification (model was adjusted for microsatellite status, mismatch repair mutations, DNA damage response gene mutations, other pathogenic gene fusions, other CD274 alterations and patient age, with samples weighted to match the tumor type distribution in the CD274 rearranged cohort; online supplemental figure 2B). When examined within disease groups, this relationship held true only in some disease types, including non-small cell lung, colorectal, unknown primary, and gastric carcinomas (figure 1E).
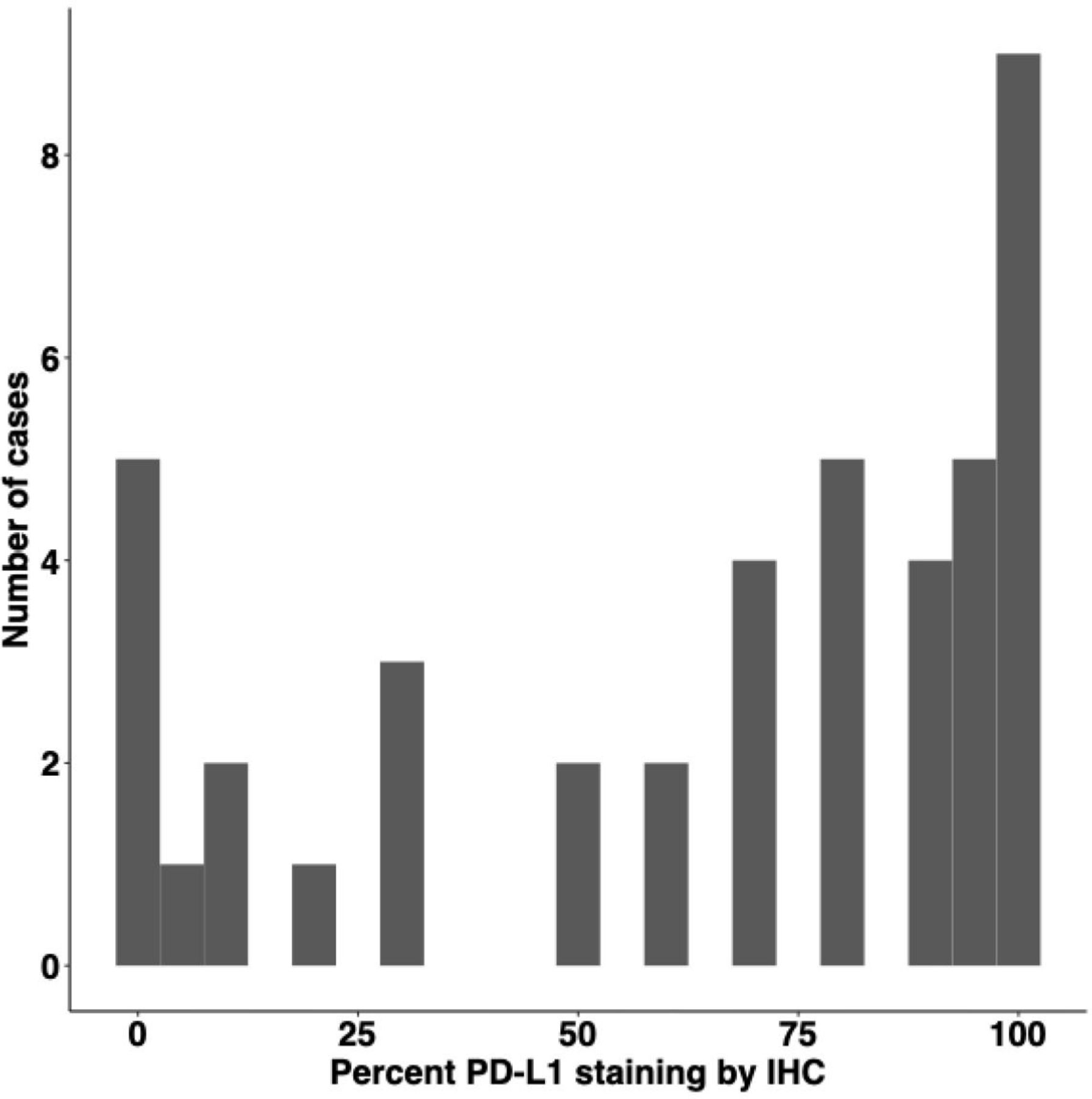
We next identified a cohort of CD274 rearranged patients for whom both CGP and PD-L1 IHC data were available n=43/145. Within this subgroup, PD-L1 staining scores (DAKO TPS) were highly skewed towards positivity with 90.7% (39/43) samples exhibiting a score ≥1% and 72.1% (31/43) samples exhibiting a score of ≥50% (figure 2, online supplemental table 3). In contrast, among the CD274 wild-type population (N=2 82 905), n=55 380 were scored for PD-L1 staining and 38.7% (21,410/55,380) had a TPS ≥1% while 15.0% (8280/55 380) had a TPS ≥50%.

Distribution of PD-L1 staining by IHC in cases with available data (n=43/145). IHC, immunohistochemistry; PD-L1, programmed cell death ligand-1.
Notably, CD274 rearranged samples with TPS <50% were found to have significantly lower numbers of paired CD274 arrangement reads (p=0.009), in contrast to their total number of reads mapped to CD274 at a comparable level to that of TPS ≥50% samples (online supplemental figure 3). From this observation, we inferred that subclonal rearrangements and genotype heterogeneity may have contributed to low TPS in these samples. Although the association between number of read pairs and rearrangement sub-clonality was not validated in the assay used, an ROC analysis indicated that number of read pairs was indeed a non-trivial predictor of TPS ≥50% in these 43 samples (area under curve (AUC)=0.80, online supplemental figure 3).
Time on ICI therapy in CD274 rearranged patients from a de-identified real world CGDB
Given the association of PD-L1 expression with CD274 rearrangements, we sought to understand whether the presence of CD274 rearrangements would be associated with clinical benefit from ICI. To this end, we observed eight CD274 rearranged cases across multiple tumor types in the CGDB treated with ICI, including two gastric adenocarcinomas, two triple negative breast cancers (TNBC), one colon adenocarcinoma, one lung squamous cell carcinoma, one lung non-squamous cell adenocarcinoma and one serous ovarian carcinoma (online supplemental table 4).
Fifty per cent (4/8) of the cases were on ICI treatment for at least 3 months and 3/4 were on ICI treatment for over 6 months (figure 3A). Sustained clinical benefit of over 2 years (778 days as of last follow-up) was observed in one gastric adenocarcinoma case (MSS, TMB of 1.25 muts/Mb, positive for genomic EBV) treated with second line pembrolizumab monotherapy. Two TNBC cases, one with a TMB of 0 muts/Mb, MSS but PD-L1 positive and another with no data on TMB, MSI and PD-L1 status were on a combination of atezolizumab and paclitaxel for 183 days and 106 days respectively, as of last follow-up. The lung adenocarcinoma case was observed to be PD-L1 high and was on first line combination therapy of carboplatin, pemetrexed, and pembrolizumab for 219 days, with a real-world partial response to treatment 3 months after start of therapy and observed real-world stable disease as of last follow-up. Given the limitations of this retrospective analysis (eg, availability of progression-free and overall survival data, length of follow-up), a comprehensive evaluation of outcomes in CD274-rearranged tumors is beyond the scope of this study. However, patient #1 with a sustained benefit of 778 days at last follow-up, is longer than the median duration of response for gastric adenocarcinoma treated with pembrolizumab monotherapy based on data from the Keynote-062 trial.33 The other patients from the CGDB cohort were censored with follow-up times comparable to, or shorter than those reported in immunotherapy trials for each respective disease type.34–38 Therefore, it is difficult to conclude whether their duration of benefit would exceed that expected for ICI in an unselected disease-matched cohort.

{kind=link}
{kind=link}
{kind=link}
Real-world clinical data in CD274 rearranged tumors. (A) Swimmer plot of duration of line of therapy for 8 CGDB patients with CD274 rearrangements treated with ICI regimen. Specific chemotherapy regimens are described in the supplement. Patient five discontinued treatment due to a change in line of therapy (B) H&E of rectum adenocarcinoma (top). PD-L1 immunohistochemistry demonstrating membranous staining of tumor cells (middle). Tumor Proportion Score was 90% via DAKO 22C3 immunohistochemistry platform. PD-L1 immunostaining of adjacent benign colonic epithelium from same patient as control with negative PD-L1 immunostaining (bottom). CGDB, clinico-genomic database; ICI, immune checkpoint inhibitor; PD-L1, programmed cell death ligand-1.
Case report and genomic characterization of CD274-rearranged metastatic rectal adenocarcinoma
A 31-year-old pregnant woman with a family history of glioblastoma in her father (age 50) presented with colonic perforation in the 37th week of pregnancy. Colonoscopy revealed an ulcerating vegetating mass 12 cm from the anal verge. Biopsy was consistent with adenocarcinoma. She underwent a Hartman procedure and Cesarean section with whole body CT showing a solitary 4 cm liver metastasis and no other sites of distant spread. She was initiated on 5-fluorouracil, oxaliplatin, and irinotecan (FOLFOXIRI) and biopsy tissue was sent to FMI for CGP.
Based on IHC, the TPS for PD-L1 expression was 90% (figure 3B). CGP results demonstrated that the tumor was microsatellite stable, with a TMB of 16 mutations per megabase. The sample was also found to harbor likely pathogenic mutations in KRAS at G12C, FBXW7 at D600Y and E332*, TP53 at C176F, truncating APC mutations at E443* and E1547*, a SMAD2 truncating mutation at S460*, a deletion in MUTYH at E466, a CTNNA1 rearrangement, and an exon 7 rearrangement of CD274 (online supplemental table 5). Based on the high PD-L1 staining and TMB, nivolumab was added to first-line FOLFOXIRI. After four cycles on the combination regimen, objective partial response was demonstrated. Because of grade 3 thrombocytopenia, FOLFOXIRI was discontinued and nivolumab was administered for two more cycles. Primary site radiation therapy was performed before low anterior resection, liver metastasectomy and ileostomy. Pathology was consistent with pathologic complete response both in liver and rectal lesions. Postoperative FOLFOX was administered to complete 6 months of perioperative treatment.
Discussion
Despite tumor site agnostic approvals for ICI, the actual clinical benefit is limited to a relatively small fraction of patients. TMB, MSI status, and PD-L1 expression measured by IHC have been used as predictive biomarkers in many clinical trials. To date, however, the mechanisms of response and/or resistance remain incompletely described.
A subset of T-cell leukemia patients with PD-L1 rearrangements have recently been shown to harbor increased PD-L1 cell surface expression,17 thought to be caused by disruption of microRNA binding sites within the 3’-UTR, and supported by in vitro experiments demonstrating that miR-34a and miR-200 can both influence PD-L1 expression at the mRNA level.39 40 These findings point to a mechanism of immune evasion that gives cancer cells a selective growth advantage and which could be exploited using ICI.
In this study we report on a case of rectal adenocarcinoma harboring a CD274 rearrangement that was associated with high tumor protein expression by IHC. This patient experienced a dramatic pathologic complete response to combined chemoimmunotherapy with surgical resection. This response was observed despite recent evidence suggesting that FBXW7 inactivating mutations may confer resistance to ICI via decreased expression of double-stranded RNA sensor proteins, diminished type I interferon response and lower MHC-I expression.41 We performed a molecular characterization of CD274 rearranged tumors in a large pan-cancer analysis along with observations of sustained clinical benefit from ICI in a small subset of patients. We observed that CD274 rearrangements, although very rare events, can occur across multiple cancer types, and have several properties suggestive of immune evasive potential.
First, the enrichment for elevated IHC staining suggests a homogeneous population of cells with respect to PD-L1 expression as the majority of cases in our analysis displayed TPS over 50%. This observation is also consistent with a mechanism of mRNA stabilization induced by 3’-untranslated region (UTR) disruption. Second, the number of CD274 rearrangement reads is shown to be a non-trivial binary predictor of TPS over 50%, with the accuracy robust to the chosen cut-off of number of reads. This observation indicates tumor heterogeneity reflected in CD274 rearrangement reads is likely to affect tumor IHC score, although a fine-tuned predictive model is beyond the scope of this study. Third, the higher-than-expected TMB among samples harboring CD274 rearrangements would be predicted to lead to a higher neoantigen burden, and therefore require means of immune evasion. It is plausible that this relationship appeared insignificant in some disease types due to small sample size, but it is also possible that there are immunological differences between the tissue types in which CD274 rearrangement was associated with high TMB. These observations are consistent with the existing literature and suggest that genomic events affecting the 3’-UTR of CD274 confer a selective advantage to cancer cells, perhaps via immunologic clonal elimination of CD274 wild-type tumor cells. Importantly, T- cell evasion driven by PD-L1 expression controlled by the interplay between miRNA and 3’ UTR of the CD274 gene is of importance in EBV positive gastric cancer.42 Here, we observe CD274 rearrangements to be enriched in EBV +ve tumors, along with durable ICI response in two CD274 rearranged stomach adenocarcinomas (one of which was also EBV +ve). Therefore, we propose that CD274 rearrangements be clinically investigated as a potential biomarker for ICI in EBV +ve gastric cancers.
These observations collectively imply that CD274 rearrangement positive cancers may respond to ICI, potentially in the presence of other genomic alterations thought to confer resistance like FBXW7. Prior to our case report, we were aware of one other clinical case of CD274 rearranged cancer treated with ICI, which was in a patient with ovarian cancer who achieved an objective response.43 The case we present here adds to the literature another example of a patient with a CD274 rearrangement who responded to ICI. In this particular example, the patient had both a high TMB, and elevated PD-L1 expression associated with CD274 rearrangement. Importantly, multiple studies suggest these two features (TMB and PD-L1 expression) have an additive effect in predicting ICI benefit.9 44–46 This alludes to the utility of a combined biomarker approach for ICI containing regimens. Another important clinical implication of our study is the use of liquid biopsy to detect CD274 rearrangements. In clinical scenarios where tissue biopsy is impossible the presence of a CD274 rearrangement in blood-derived circulating tumor DNA (ctDNA) sequencing may potentially be suggestive of ICI sensitivity with further prospective studies. To this point, we have identified three examples of CD274 rearrangements found in ctDNA sequencing, with two patients remaining on treatment as of last follow-up. Future studies with larger clinically annotated CD274 rearranged cohorts will be needed to demonstrate statistical independence from other ICI biomarkers, but our data highlight that clinical benefit is possible through blocking this rare mechanism of immune evasion.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. All data relevant to the study are included in the article or uploaded as supplementary information. The data generated by the research that support our article will be provided in the supplements.
Ethics statements
Patient consent for publication
Ethics approval
This study was conducted in accordance with the Western Institutional Review Board (WIRB) approved Protocol No. 20152817. For the Flatiron Health-Foundation Medicine. Clinicogenomic Database, Institutional Review Board approval of the study protocol was obtained prior to study conduct and included a waiver of informed consent.
Acknowledgments
We would like to thank Sunandini Chopra and Ebru Karakoc for their collaboration in facilitating the real-world data and case report included in this manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
ADK and KM contributed equally.
Contributors Author contributions are outlined below. ADK and KM are equal contributors. Conceptualization: ADK, KM, and UD. Data curation: ADK, KM, ZK, RSPH, and DIL. ormal analysis: ADK, KM, ZK, and RSPH. Investigation: ADK, KM, ZK, and RSPH. Methodology: ADK, KM, ZK, and RSPH. Resources: DIL, and UD. Writing-original draft: ADK, KM, and ZK. Writing-review and editing: ADK, KM, ZK, MM, JSR, LAA, RSPH, DIL, UD, and JC. Guarantor and author responsible for overall content: ADK.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests ADK, KM, ZK, MM, JSR, LAA, RSPH, DIL, and JC are employees of Foundation Medicine, a wholly owned subsidiary of Roche Holdings and Roche Finance, and these employees have equity interest in an affiliate of these Roche entities.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.